
Abstract
Heat-related illness (HRI) is the progression of symptoms toward hyperthermia resulting directly from one’s physiological response to excess heat. HRI, though preventable, is a serious health problem advancing from heat rash, heat cramps, heat syncope, and heat exhaustion to the most severe disorder, heat stroke. 1 Excess environmental heat, manifesting as the body’s inability to thermoregulate, is a precursor to HRI. Excess heat occurs in the presence of high ambient temperatures or in environments that produce but do not allow the Earth to release heat into the atmosphere. 2
A key factor in the body’s response to heat is acclimatization, the physiological adaptation to repeated or sustained exposure to heat. Acclimatization can increase an individual’s tolerance to heat stress by enhancing sweating efficiency, stabilizing circulation, and reducing core body temperature. 3 However, the benefits of acclimatization require time, consistent exposure, and appropriate hydration and rest periods. 4 When ambient temperatures rise suddenly, or when individuals are exposed to extreme heat without sufficient time or conditions for acclimatization, the risk of HRI increases dramatically. This is especially relevant in areas experiencing novel or more intense heatwaves due to climate change, where populations may not be physiologically or environmentally prepared.
Physiological responses to excess heat are further complicated by social determinants of health (SDoH).5,6 The U.S. Department of Health and Human Services Healthy People 2030 identifies SDoH as the conditions in which people are born, live, work, and age, including income, education, housing, and employment, that affect a wide range of health outcomes and risks. 7 SDoH have been shown to exert a greater influence on health than genetics or even access to medical care, though the latter still plays a meaningful role.8,9 The relationship between poor SDoH and HRI, specifically one’s capacity to adequately acclimate to or respond to rising temperatures, remains underexplored.
In the context of climate change, ambient temperatures are expected to rise and contribute to more frequent and intense heatwaves, placing vulnerable populations at greater risk of HRI. Populations of color and low-income communities, who are more likely to live in urban heat islands (UHIs), often lack the environmental and infrastructural conditions necessary for acclimatization or protection from heat.10,11Although there is an established association between socioeconomic status and exposure to extreme heat, the literature is limited in identifying which specific SDoH, alone or in combination, amplify HRI risk.12,13
The purpose of this scoping review is to understand the scope of available literature demonstrating the effects of SDoH on HRI and to identify the extent of evidence supporting specific SDoH as contributors to HRI in the United States. The findings may clarify which factors, such as inadequate access to cooling, unsafe neighborhoods, or inability to physiologically adapt due to health or occupational constraints, disproportionately increase individuals’ vulnerability to HRI. This scoping review addresses the following research question: What are the SDoH that contribute to HRI?
METHODS
This review followed the PRISMA-ScR guidelines and utilized a search strategy developed in consultation with an academic librarian (LN). 14 The databases searched included MEDLINE via PubMed, CINAHL Complete via EBSCOhost, and PsycINFO. Scopus, Web of Science, and Google Scholar were excluded due to limitations in systematic searching.15,16
Search terms focused on HRI and SDoH, with relevant MeSH terms and synonyms compiled in a term log (Supplementary Data). Searches were conducted in September 2023 and limited to English-language articles published between 2018 and 2023.
The search yielded 1647 articles. After removing duplicates and non-U.S. studies, 579 abstracts were screened. Two reviewers conducted the screening and eligibility assessment, resolving disagreements with a third reviewer. Articles were included if they explicitly mentioned high temperatures or heat exposure and defined HRI using recognizable symptoms (e.g., cramps, exhaustion, heat stroke). The final selection included 48 articles (Fig. 1).
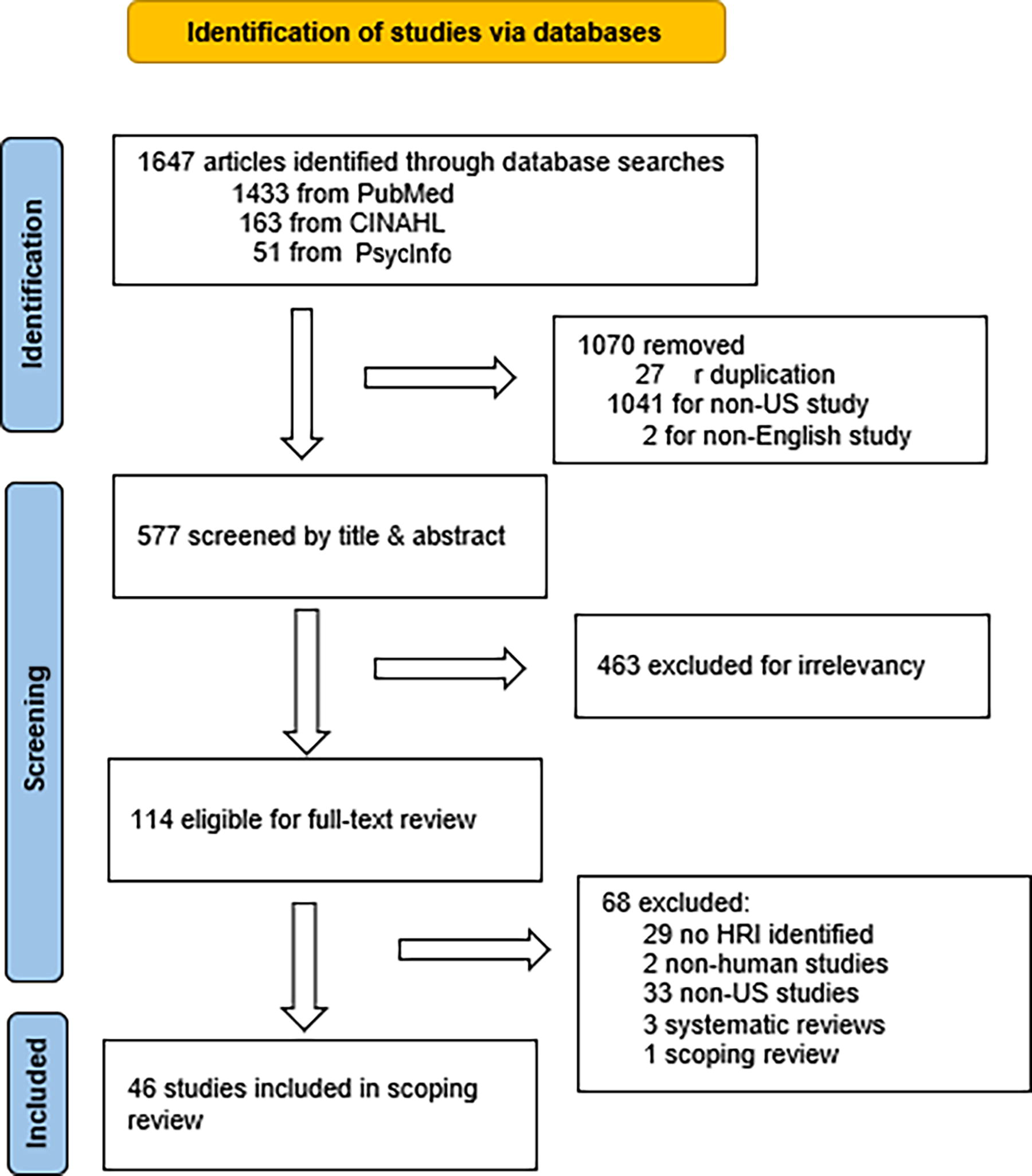
PRISMA flow diagram of study selection.
The authors organized the themes according to the levels of the socio-ecological model, individual, interpersonal, community, and societal to capture the layered nature of vulnerability to HRI.17,18,19 Two independent reviewers reached consensus on the categorization of themes. This study did not require institutional review board approval, as it involved a review of published literature and did not include human subjects.
RESULTS
This scoping review included 48 articles examining HRI and its intersection with SDoH. Most studies were observational in design (n = 42), including cohort (n = 22), case-control (n = 13), and case series (n = 7). Only two studies were experimental, and one was a clinical guideline representing the highest level of evidence according to Polit and Beck.
20
(Fig. 2
21
) The majority of publications were recent, with the highest number published in 2021 (n = 13).
Frequency of quality of evidence from least to most robust.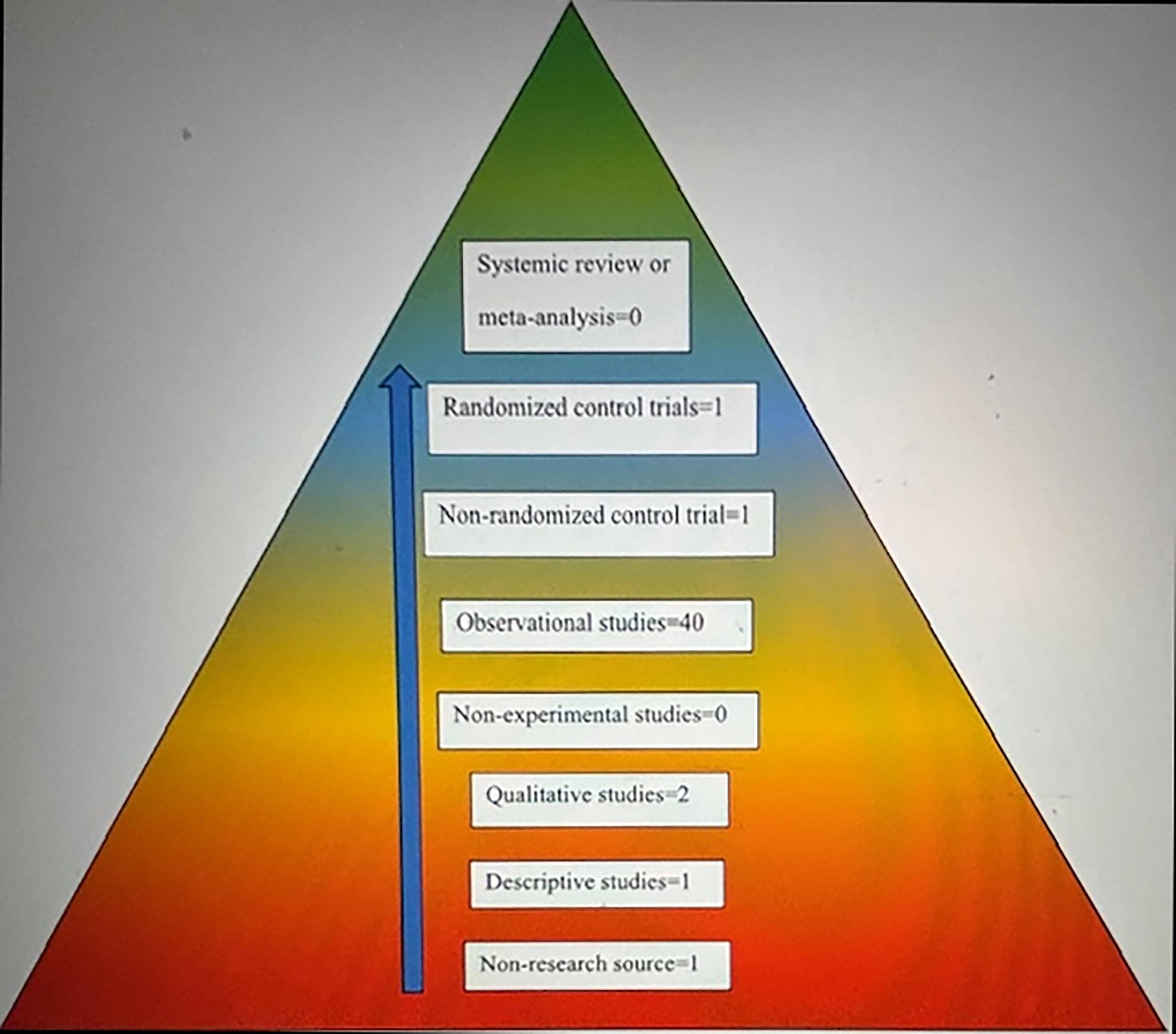
Half of the articles (n = 27) indicated the age of the study population participants. Half of those included all age groups. In seven studies, people over 65 years old were the identified population. Five studies identified participants by sex or gender, three by race, and four by ethnicity. Those studies that indicated a location were conducted in the southwest United States (n = 7). Only seven articles included references to chronic or mental health conditions. Four involved health care settings. Occupational work was the focus of nine studies; five of which were about agricultural workers. Athletes were the subject of five studies about outdoor activities. One article involved undocumented border crossers. Air cooling, such as air conditioning, fans, and window ventilation, was discussed in 21 articles.
Excess heat affects outdoor pursuits, such as occupational activities (n = 41) and behaviors requiring physical exertion (n = 23), as well as indoor work (n = 2). Environmental circumstances, in addition to the presence of excess heat, included air pollution (n = 16) and UHI (n = 15). Socioeconomic factors were characterized in 32 other articles related to education level (n = 1), income status (n = 17), lack of available resources (n = 9), and living in unsafe neighborhoods (n = 4). Components related to physical aspects consisted of comorbidities (n = 36) and taking medications (n = 2). Cardiovascular disease (n = 2), diabetes (n = 3), hypertension (n = 2), mental health disorders (n = 3), and pregnancy (n = 2) were the most frequently identified health conditions. The risk of suicide was noted in one study. Also, consumption of alcohol (n = 2) and energy drinks (n = 1) was cited. Acclimatization was discussed in 19 articles, as an ineffective outcome because there was no adequate time for thermoregulation, and others as a mitigation strategy where physiological adaptation permitted optimal performance or reduced the deleterious effects of excess heat (See Figure 3).
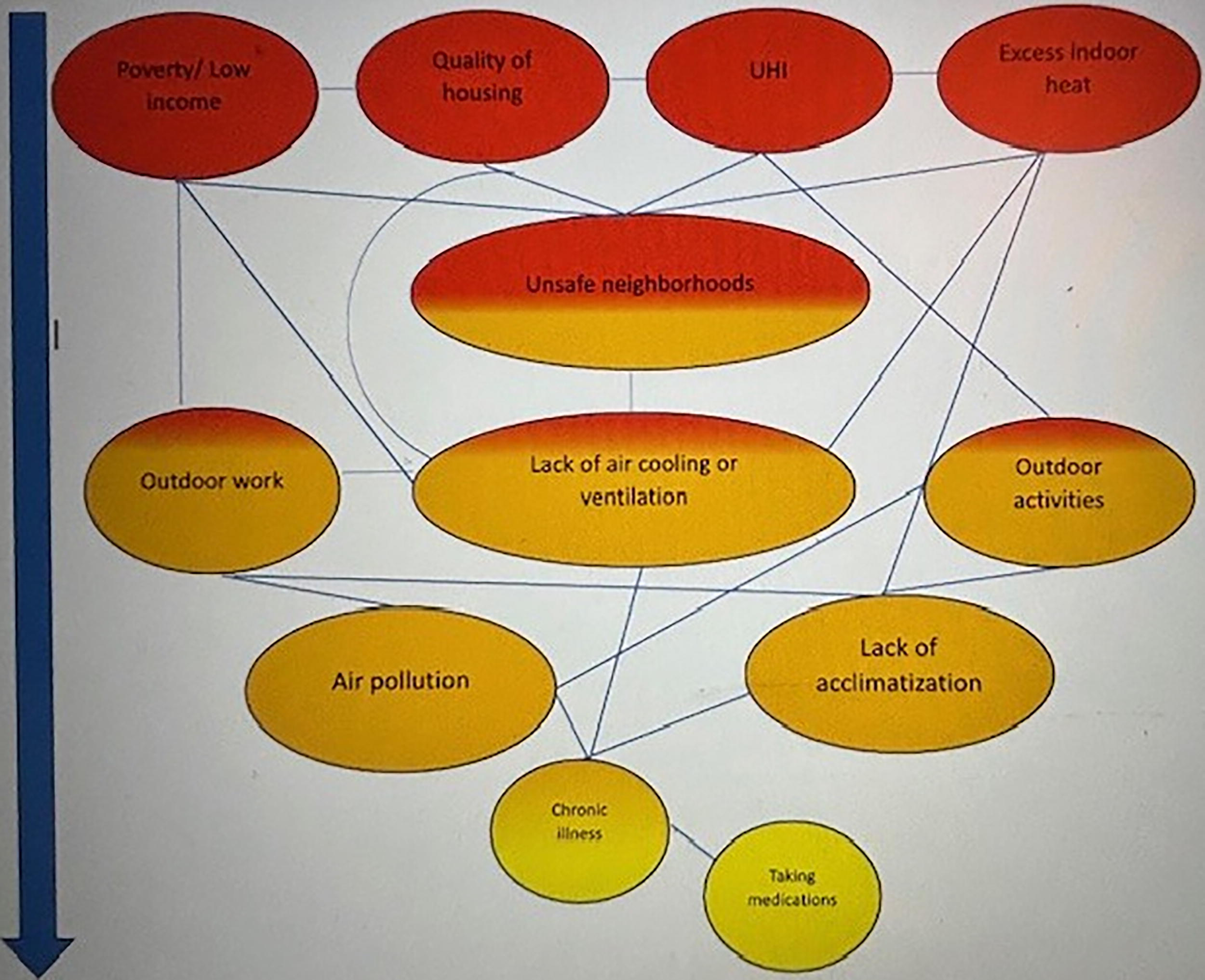
Heatmap representation of thematic frequency (most in red to least in yellow) and their relationships.
Interventions included clinical (n = 17), policy (n = 18), and educational (n = 2) strategies. SDoH concepts most frequently identified were:
Socioeconomic status (n = 32), including income (n = 21), resource access (n = 9), education (n = 1), and neighborhood safety (n = 4) Housing quality (n = 13) UHIs (n = 15) Occupational exposure (n = 18), including agriculture and indoor work Outdoor activities (n = 27), including athletes and undocumented border crossers Preexisting medical conditions (n = 25)
Themes that emerged from the literature on HRI resulting from excess heat are framed using a social-ecological model to better illustrate the complex nature of vulnerability. 22 The reviewed literature reveals that vulnerability to HRI is shaped by a complex interplay of individual, interpersonal, community, and societal-level factors. At the individual level, physiological susceptibility, such as pre-existing health conditions (e.g., diabetes, cardiovascular disease, pregnancy), emerges as a central risk factor. This is compounded by behavioral and physical limitations, including use of medications, alcohol consumption, and limited acclimatization to heat. Financial barriers to operating or acquiring air cooling also directly influence individual capacity to mitigate heat exposure.
At the interpersonal level, caregiving responsibilities and social isolation, particularly among the older adults, can limit an individual’s ability to seek or relocate to cooler environments. Shared household practices and family dynamics, while less frequently studied, play a role in decisions around heat mitigation and resource use.
The community and environmental context further constrain or support resilience. Outdoor labor and physical exertion, particularly in occupations such as agriculture, kitchen work, and welding, expose workers to intense and prolonged heat. The UHI effect and substandard housing amplify exposure, especially when compounded by neighborhood safety concerns that prevent residents from accessing public cooling spaces. Community infrastructure and housing quality thus shape both exposure and opportunities for relief.
Finally, at the societal level, structural determinants such as income inequality, employment in low-wage or informal sectors, and lack of transportation or public resources underscore systemic barriers to adaptation. Educational disparities, though underrepresented in this body of literature, may influence awareness and utilization of heat safety strategies. Broader policy gaps, such as lack of mandated workplace protections or cooling standards in housing, represent missed opportunities for structural mitigation of HRI risk.
Together, these findings illustrate that effective interventions must move beyond individual behavior to address the layered social and structural contexts in which heat exposure and vulnerability occur.
Access to air cooling emerged as a multifaceted theme influenced by economic, behavioral, and infrastructural elements. At the individual level, studies highlighted an inability to afford the purchase or operation of air conditioning systems, often tied to low income or energy insecurity. At the interpersonal level, household norms and practices, such as limiting cooling use to conserve electricity or relying on shared decision-making, shaped how available cooling was used. At the community and societal levels, access was further constrained by limited public infrastructure, including inadequate transportation to reach cooling centers or the absence of such centers in vulnerable neighborhoods. These overlapping barriers emphasize that cooling access is not solely about physical availability but also about affordability, social dynamics, and systemic resource allocation.
DISCUSSION
This review expands the understanding of what SDoH contribute to HRI by identifying lack of air cooling as both an independent and interconnected factor influencing HRI. It highlights how air cooling is shaped by economic status, housing infrastructure, and neighborhood safety. Without air cooling, individuals face compounded health risks as ambient temperatures rise.
Low-income status restricts access to cooling technologies. 23 Poor housing may lack ventilation or insulation, and unsafe neighborhoods may discourage residents from opening windows or may necessitate outdoor time due to high indoor temperatures.24,25,26,27 UHI effects exacerbate these risks, especially where structural disparities prevent heat dissipation.28,29 Occupational exposure to heat is another critical factor, with indoor workers like kitchen staff often overlooked. 30
Although education level is a widely recognized SDoH, its presence in the reviewed literature on HRI was notably limited. Only one article in the analysis explicitly examined education as a contributing factor to HRI risk. This underrepresentation is significant, given that education level often influences other critical determinants such as health literacy, income, employment opportunities, and the ability to access and interpret information related to heat safety and mitigation strategies. The lack of focus on education in HRI research may reflect a broader gap in understanding how cognitive and informational resources affect individuals’ capacity to recognize symptoms, seek timely intervention, or implement protective behaviors during extreme heat events. Future research should explore how education level interacts with other SDoH, such as housing quality, income, and access to air cooling, to shape vulnerability and adaptive capacity in the face of rising temperatures.
While air pollution is an identified SDoH in Healthy People 2030, which addresses structural racism and its reinforcement of inequitable systems, its direct link to HRI was not well established in the reviewed literature.31,32 Similarly, occupations beyond kitchen work, like factory jobs, were underrepresented.
Residential air conditioning is recognized as a key adaptation strategy yet is unevenly distributed, reinforcing systemic disparities.33,34,35 Even in cities with widespread access, certain neighborhoods remain vulnerable. 36 Although experimental studies are sparse, the perception of elevated HRI risk among those without air cooling reinforces its role as an SDoH. More rigorous research is needed to quantify the protective effects of air cooling and inform policy.
While this review identifies lack of air cooling as a key SDoH contributing to HRI, the influence of this determinant varies significantly by geography. 37 In regions of the United States where high ambient temperatures and prolonged heatwaves are common, such as the South, Southwest, and some urban centers, air cooling is a necessary adaptation mechanism. 38 However, in temperate or cooler geographic regions, where extreme heat events are less frequent or historically uncommon, other SDoH may play a more prominent role in determining HRI risk.
In these regions, housing may not have been constructed with heat resilience in mind. 39 As a result, housing infrastructure, such as insulation, ventilation, and structural design, can strongly influence internal heat retention during atypical heat events. 40 Populations in higher elevations or mountain regions, for example, may be particularly vulnerable to rapid-onset heatwaves due to the absence of air conditioning and limited public awareness about heat-related risk. In these contexts, heat vulnerability is more closely tied to infrastructure readiness and emergency preparedness than to cooling access alone.
Social cohesion and community engagement also emerge as critical mitigating factors in areas where cooling infrastructure is less prevalent. The review also notes mental health concerns, including increased suicide risk during heatwaves, particularly among socially isolated individuals. 41 In geographically dispersed rural communities, individuals who are socially isolated or homebound may be less likely to receive timely support during extreme heat. Conversely, in communities with strong social networks, informal caregiving systems can help identify and respond to signs of HRI among vulnerable residents, particularly the elderly and chronically ill.
Transportation and access to health care further compound these challenges in rural or mountainous areas. In such geographies, limited proximity to emergency services or public cooling shelters can delay care during acute heat events. Even moderate heat exposure may lead to worse outcomes if individuals are unable to access timely intervention or treatment.
Finally, geographic features such as elevation, vegetation, and urban design alter microclimates and can either exacerbate or buffer heat exposure. For instance, residents of UHIs within otherwise moderate climates may face elevated risk due to built environments that trap heat.42,43 In these settings, lack of green space, poor air circulation, and high-density housing without ventilation or insulation intersect with SDoH such as poverty and poor housing quality to increase vulnerability.
While air cooling is a crucial SDoH in regions with frequent extreme heat, it should not be viewed in isolation. Geographic variation influences which SDoH are most salient and reveals the necessity of localized, context-specific public health interventions. Recognizing these variations allows for more precise strategies that account for regional infrastructure, social networks, environmental factors, and historical climate exposure.
Air cooling, while interrelated with SDoH, such as income, housing quality, and neighborhood safety, emerges from this review as a distinct and independent factor due to its direct and immediate role in preventing HRI. Unlike broader structural determinants, which tend to have cumulative or indirect effects on health outcomes, lack of access to air cooling exerts a proximate and acute impact during extreme heat events, often within hours or days.
What distinguishes air cooling as an SDoH is that it serves as a final, protective defense against rising temperatures. While poverty, poor housing, or unsafe neighborhoods set the stage for vulnerability, the presence or absence of air cooling determines whether a person can physiologically withstand heat stress. For example, two individuals may have identical socioeconomic status and chronic health conditions, but the one with access to functioning air cooling is significantly less likely to suffer from heat exhaustion or stroke.
Moreover, air cooling intersects with but is not fully explained by other SDoH. A person may technically afford air conditioning, but local infrastructure limitations (e.g., no central cooling, poor electrical grids, inadequate housing structures) or fear of opening windows in unsafe neighborhoods may prevent effective use of cooling technologies. These nuances show that air cooling is not merely an extension of income or housing but rather has become an environmental health determinant, affected by physical, economic, and social variables, though still functionally separate.
This distinction also has implications for advocacy and policy. While poverty alleviation and housing improvements are long-term goals, targeted interventions to increase access to air cooling, such as subsidies, cooling centers, or building codes, can offer immediate protection from HRI. In this way, air cooling operates both as a marker of systemic inequity and a point of intervention for climate adaptation.
LIMITATIONS
Limitations include the broad and sometimes imprecise definitions of HRI and SDoH, as well as potential reviewer bias. The geographic focus was on the U.S. Southwest, and temporal limitations may not reflect evolving climate conditions.
CONCLUSION
This review clarifies the relationship between SDoH and HRI, identifying lack of air cooling as a newly emergent determinant. It emphasizes the need to recognize air cooling not only as a mitigation strategy but as a critical SDoH shaped by income, housing quality, occupational exposure, and neighborhood safety. As heatwaves become more frequent and intense, equitable access to cooling resources must be prioritized to address growing health disparities linked to climate change.
Footnotes
AUTHORS’ CONTRIBUTIONS
J.M.B.: Conceptualization (lead), methodology (lead), writing original draft (lead), data collection and analysis (lead), visualization (lead), writing—review and editing (lead). L.T.-B.: Writing—original draft (equal); data collection and analysis (equal). N.D.-G.: Writing—original draft (equal); data collection and analysis (equal). L.-M.O.: Writing—original draft (equal); data collection and analysis (equal), visualization (equal). E.R.: Data collection and analysis (equal). M.S.: Writing—review and editing (equal).
AUTHOR DISCLOSURE STATEMENT
No competing financial interests exist.
FUNDING INFORMATION
No funding was received for this article.
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.