
Abstract
Background:
Intranasal corticosteroids (INCSs) are widely prescribed for allergic and nonallergic rhinitis and chronic rhinosinusitis, frequent causes of upper airway cough syndrome (UACS). In UACS, adherence is strongly influenced not only on pharmacological efficacy but also on device performance and sensory tolerability. Despite this, few studies have linked in vitro spray characteristics with patient-reported outcomes.
Objective:
To evaluate the technological characteristics and clinical acceptability of mometasone furoate administered via the liquid VP3 nasal spray device by integrating in vitro performance testing and in vivo patient-reported outcomes in individuals with chronic cough and UACS.
Methods:
In vitro experiments assessed deposition patterns in a silicone nasal cast, dripping behavior on inclined gel surfaces, viscosity, and spray plume geometry. An observational study enrolled 10 patients (80% female, mean age 56 ± 8.4 years) referred to a tertiary cough clinic for chronic cough (mean duration 3.5 years) associated with postnasal drip. Patients switched from conventional mometasone sprays to the device and completed Anchored Best–Worst Scaling evaluations of 11 sensory and treatment-related attributes. Global satisfaction was rated using a visual analog scale (VAS) and Treatment Satisfaction Index (TSI).
Results:
Deposition was reproducible (27.9 ± 1.7% of cast surface) with distribution into middle and lower turbinates. Moderate viscosity (14.4 ± 3.2 mPa·s) and stable plume geometry supported retention. In vivo, overall satisfaction scores remained stable following switching (TSI: 64.3 ± 3.4 vs 63.8 ± 4.6; VAS: 6.8 ± 3.2 vs 6.1 ± 1.6). However, patients reported significantly greater satisfaction in two sensory domains and rated three domains as more important (p < 0.05). No deterioration in any attribute was observed.
Conclusion:
The liquid VP3 nasal spray device delivering mometasone furoate demonstrated reliable in vitro performance and favorable patient acceptability in UACS. The correspondence between deposition behavior and patient-reported tolerability supports its suitability for INCS delivery and warrants further evaluation in larger, longer-term studies.
Introduction
Intranasal corticosteroids (INCSs) are the standard first-line therapy for inflammatory conditions of the nasal mucosa, including allergic and nonallergic rhinitis and chronic rhinosinusitis with or without nasal polyps.1,2 Their clinical utility extends beyond nasal obstruction and rhinorrhea, as they also modulate mucosal inflammation and sensory irritation in the upper airways.1,2 These mechanisms are relevant in patients with chronic cough attributed to upper airway cough syndrome (UACS), a frequent etiology encountered in specialist cough clinics. 3 In UACS, persistent cough may arise through mechanical stimulation of oropharyngeal receptors by secretions or through a neuroinflammatory mechanism leading to sensitization of the cough reflex. 3 Accordingly, controlling rhinological symptoms is considered fundamental in UACS management.
Although INCSs are broadly similar in pharmacological potency, patients often report meaningful differences in tolerability and usability between spray devices.4,5 Sensory attributes such as aftertaste, nasal irritation, dripping anteriorly or posteriorly, dryness, and perceived onset of action may influence adherence more strongly than small pharmacodynamic differences. 6 This has practical implications in chronic, symptom-driven conditions such as UACS, in which sensory feedback strongly modulates treatment acceptability.
Spray formulation and device geometry jointly determine droplet size, plume spread, and mucosal adhesion, which, in turn, shape the sensory experience of administration.4,5 Most marketed INCSs are delivered via pump-actuated sprays, but the deposition profile and user-perceived tolerability can vary substantially across devices. 7 Despite this, relatively few studies have linked objective in vitro performance with patient-reported outcomes, particularly in groups of patients with chronic cough associated with UACS rather than classical allergic rhinitis cohorts.
This translational study was designed to integrate laboratory characterization of a mometasone furoate nasal spray (BrusonexTM, Bruschettini s.r.l., Genoa, Italy) delivered via the liquid multidose nasal spray VP3 device (Aptar Pharma, Le Vaudreuil, France) with in vivo patient-reported outcomes in individuals with chronic cough attributed to UACS. By examining both mechanistic performance and user experience, this study aims to provide a more comprehensive understanding of how device engineering translates into real-world acceptability. This approach responds to the growing recognition that tolerability and usability are central determinants of persistence with INCS therapy, particularly in symptomatic conditions such as UACS, where sensory burden is a dominant driver of health-seeking behavior.
Methods
Study design overview
This translational study comprised two complementary components: (1) laboratory characterization of a mometasone furoate aqueous nasal spray delivered via the VP3 device and (2) a prospective observational switch study evaluating patient-reported satisfaction in individuals with chronic cough attributed to UACS. The rationale was to relate measurable spray performance properties to real-world usability and tolerability. The in vitro experiments assessed deposition profile, dripping/retention, spray plume geometry, and viscosity. The in vivo component evaluated satisfaction before and after switching from a conventional INCS to the same molecule delivered by the VP3 device.
In vitro characterization
Materials and device
All in vitro measurements were performed using the marketed pump–actuator combination supplied with the commercial product (VP3 pump fitted with its corresponding nasal actuator/nozzle tip and protective cap), with no actuator substitutions or modifications introduced for the experimental program. The mometasone furoate nasal spray is delivered via the VP3 multidose, premetered mechanical pump, which incorporates a reproducible metering chamber and piston mechanism to support dose uniformity across actuations and to generate a consistent plume geometry. Within this system, the actuator–nozzle assembly regulates droplet formation and spray angle, whereas the suspension’s viscosity supports mucosal adhesion without impairing atomization.
Nasal cast deposition
Each condition was tested in triplicate. Deposition was evaluated using a standardized three-dimensional silicone nasal cast (Fig. 1) replicating human nasal anatomy (Model LM-005, Koken Ltd., Tokyo, Japan); only the left nasal cavity was considered for analysis. 8 To visualize spray deposition, the entire cast surface was coated with a thin layer of water-indicating paste (Sargel®, Arkema, Exton, PA, USA), which undergoes a rapid color change from white to purple upon contact with aqueous solutions, enabling clear visualization of the deposition footprint. The device was inserted to a depth of 1 cm into the left nostril and actuated manually once at a 45° angle (defined as the pitch angle between the nozzle centerline/spray axis and the horizontal plane of the cast base). The device was maintained within the sagittal plane of the left nostril (yaw = 0°) and without axial rotation (roll = 0°), such that only the pitch angle was set to 45°. This angle was selected because it represents typical patient use as clinically recommended for nasal spray administration. 9 Three different VP3 units were tested to account for device-to-device variability. One minute after actuation, digital images of the cast interior were obtained using a high-resolution Sony α5100 camera (24.3 megapixels APS-C sensor) under standardized lighting and exposure parameters. Images were analyzed using ImageJ software (NIH, Bethesda, MD, USA). The nasal cavity was divided into three anatomical regions of interest (ROIs): vestibule, middle–upper turbinate, and lower turbinate. The threshold for pixel recognition was standardized across all images (0–73) to minimize variability. Deposition was quantified as the percentage of surface area covered relative to the total available area, both overall and within each ROI. 10 This coverage-based endpoint is commonly used in Sar-Gel®-coated nasal cast models to capture spatial distribution and surface wetting, rather than absolute deposited drug mass. 11 Deposition in the anterior vestibule and deeper turbinate regions was assessed descriptively.
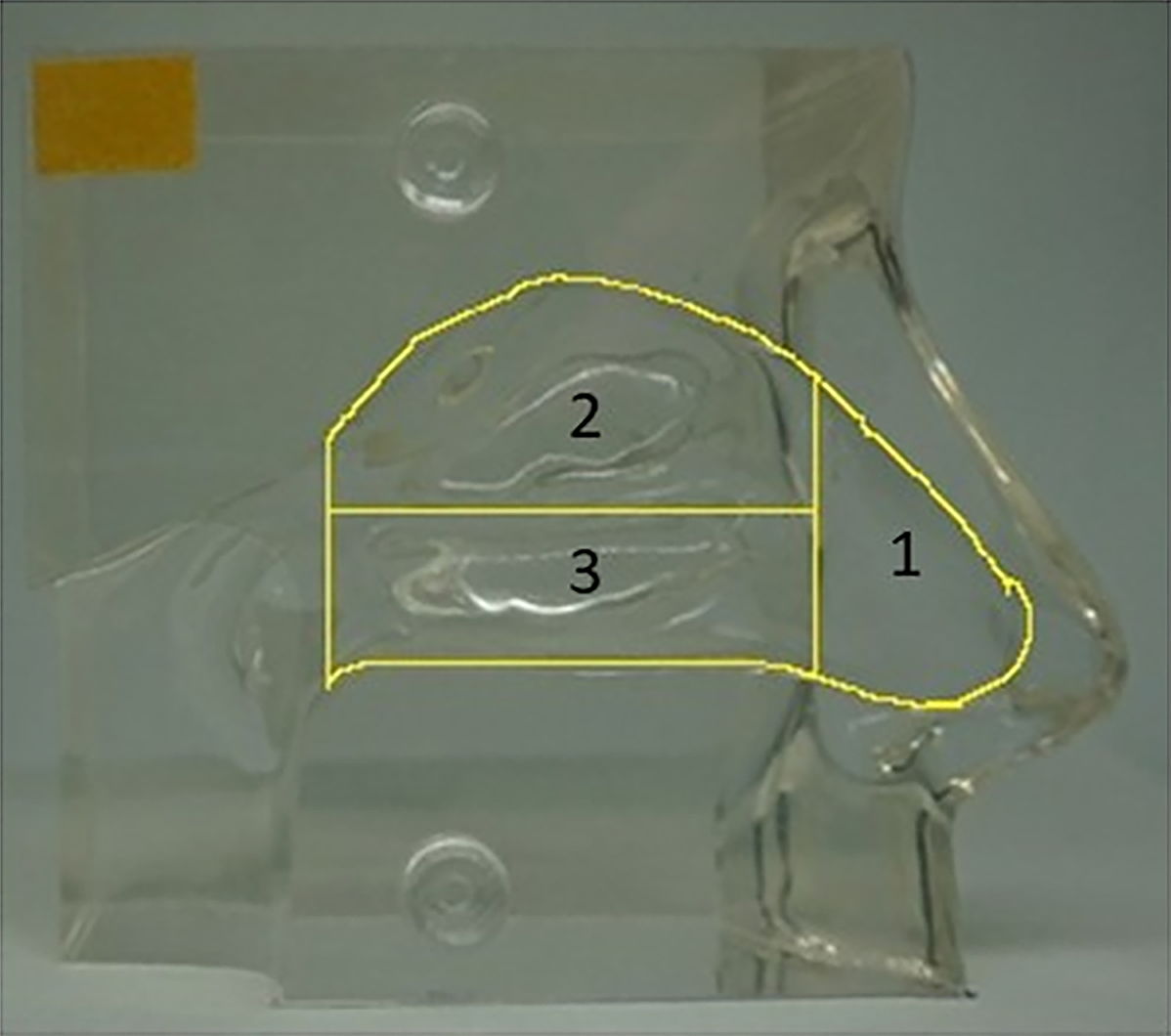
Standardized silicone nasal cast (Koken® model) used for deposition analysis, divided into three anatomical regions of interest: vestibule (1), middle–upper turbinate (2), and lower turbinate (3).
Dripping and retention behavior
Retention was assessed under inclined-surface conditions to approximate gravitational run-off as reported previously.11,12 Dripping studies were designed to evaluate the retention of the formulation on inclined mucosal surrogate surfaces. A glass slab was covered with a fluorinated liner (3M, USA) and coated with a uniform 0.03 mm layer of Sargel® paste using a casting knife (BYK, Germany). The prepared surface was positioned at a 45° incline. Two experimental conditions were assessed: (1) deposition of 50 µL of formulation by pipette, simulating static liquid placement, and (2) deposition by spray actuation from a distance of 3 cm at a 45° actuation angle, simulating dynamic delivery. Images were captured 1 minute after deposition, and the distance of liquid run-off was measured (in cm) using ImageJ with a graduated scale as reference. Each condition was repeated in triplicate. Dripping length served as a proxy for retention: shorter run-off suggested greater adhesion and reduced tendency for anterior or posterior dripping in vivo.
Spray pattern analysis
Spray plume geometry was evaluated under standardized laboratory conditions.4,13,14 Fluorinated glass plates were coated with a 0.03 mm layer of Sargel® paste, like in the dripping study. The plates were positioned horizontally at distances of 3 and 6 cm above the nozzle tip. The device was actuated once per measurement, and experiments were performed in triplicate. Spray deposition was visualized as a circular plume on the coated surface. Image analysis (ImageJ) was used to calculate plume diameter, area, and perimeter. These parameters were used to characterize atomization quality and reproducibility. Symmetrical, stable plumes were considered favorable for achieving reliable deposition within the nasal cavity.
Viscosity analysis
The apparent viscosity of the formulation was measured under controlled temperature and shear conditions using a controlled-stress rheometer (Thermo Scientific HAAKE Series 1 Rheometer, Karlsruhe, Germany). The term “apparent viscosity” is used because suspensions may exhibit non-Newtonian behavior, and viscosity depends on the applied shear conditions. A C35/2° Ti cone geometry was used, and experiments were performed at 25°C. For each measurement, 1 mL of formulation was applied to the rheometer plate. Shear was applied at a rotational speed of 1.5 rpm (rheometer cone–plate) for 300 seconds, and viscosity was recorded at 1-minute intervals. Each measurement was performed in triplicate, and results were expressed as mean ± standard deviation (SD). Viscosity was selected as a parameter of interest because excessively low viscosity increases dripping and clearance, whereas excessive viscosity may impair atomization.
In vivo clinical study
Participants
The clinical arm was conducted at the Florence Cough Clinic, a specialist center for chronic cough. Ten adult patients (≥18 years) with chronic cough attributed to UACS 3 were enrolled. The clinical diagnosis of UACS was based on persistent postnasal drip symptoms and absence of active lower airway disease, confirmed by specialist evaluation. Exclusion criteria comprised current smoking or smoking history >10 pack-years, uncontrolled asthma or chronic obstructive pulmonary disease, recent systemic corticosteroid use (<4 weeks), respiratory tract infection within 4 weeks, or documented intolerance to INCSs. The study was approved by the local Institutional Review Board (Comitato Etico Regione Toscana—Area vasta Centro, OSS-14131), and written informed consent was provided by all participants.
Study procedures
This was a prospective switch study in which each participant served as their own control. At baseline (visit 1), patients evaluated their existing conventional INCS. They were then switched to mometasone furoate delivered via the liquid VP3 nasal spray device at an equivalent daily dose. After a minimum of 2 weeks of treatment, patients returned for reassessment (visit 2). The 2-week interval was selected to allow stable exposure sufficient for preference assessment while minimizing the risk of symptom fluctuation due to seasonal or environmental variability.
Patient-reported outcomes
Patient satisfaction and attribute importance were evaluated using Anchored Best–Worst Scaling (ABWS).7,15 This method requires individuals to repeatedly select the most and least satisfactory (or important) attributes from subsets of options. A Best–Worst score (BWS) was calculated as BWS = (Most chosen – Least chosen)/Total appearances, yielding a score ranging from –1 (least favorable) to +1 (most favorable). Participants subsequently rated the attributes they selected as most and least satisfactory on a 0–10 verbal rating scale. These anchor ratings were used to rescale BWS to a 0–100 Treatment Satisfaction Index (TSI), improving interpretability.7,15 Eleven attributes were assessed: seven sensory (immediate taste, aftertaste, smell, irritation, urge to sneeze, dripping, and dryness) and four treatment-related (convenience, perceived onset of effect/fast acting, duration of effect, and symptom control). Each patient completed the ABWS questionnaire at baseline (on their prior INCS) and after switching to mometasone furoate delivered via VP3; evaluations were separated by a minimum of 2 weeks to allow acclimatization to the new spray. Additional details on the questionnaire (choice task format and anchoring items) are provided in the Supplementary Data. In addition to ABWS, patients rated overall satisfaction with each device using a 0–10 cm visual analog scale (VAS).
Statistical analysis
In vitro outcomes (percentage nasal cast surface covered, drip length, plume metrics, and viscosity) were summarized as mean ± SD of three independent replicates for each condition. Reproducibility was quantified descriptively by examining the variability across replicates and calculating coefficients of variation. Because only a single formulation–device combination was tested, in vitro differences (e.g., between test distances) were interpreted descriptively, and no formal hypothesis testing was performed. For the clinical arm, paired analyses were used throughout, as each participant contributed data under both conditions (before and after switching). Differences in TSI and domain-level BWSs were evaluated using paired t-tests. A p-value <0.05 was considered statistically significant. Statistical analysis was performed using GraphPrism (version) and SAS (SAS Institute, Cary, NC, USA; version 9.4).
Results
In vitro findings
The mometasone furoate nasal spray delivered via the VP3 device demonstrated reproducible deposition patterns in the nasal cast model (Fig. 1B). Following a single actuation at a 45° angle, the formulation covered 27.91 ± 1.69% of the available nasal surface area (Fig. 2). Analysis of regional distribution revealed that deposition was not restricted to the anterior vestibule but extended into deeper turbinate regions (Fig. 2). Specifically, measurable deposition was observed in both the middle–upper turbinate region and the lower turbinate region. Importantly, deposition was consistent across replicates, with low variability between devices, underscoring the reproducibility of the formulation–device combination.
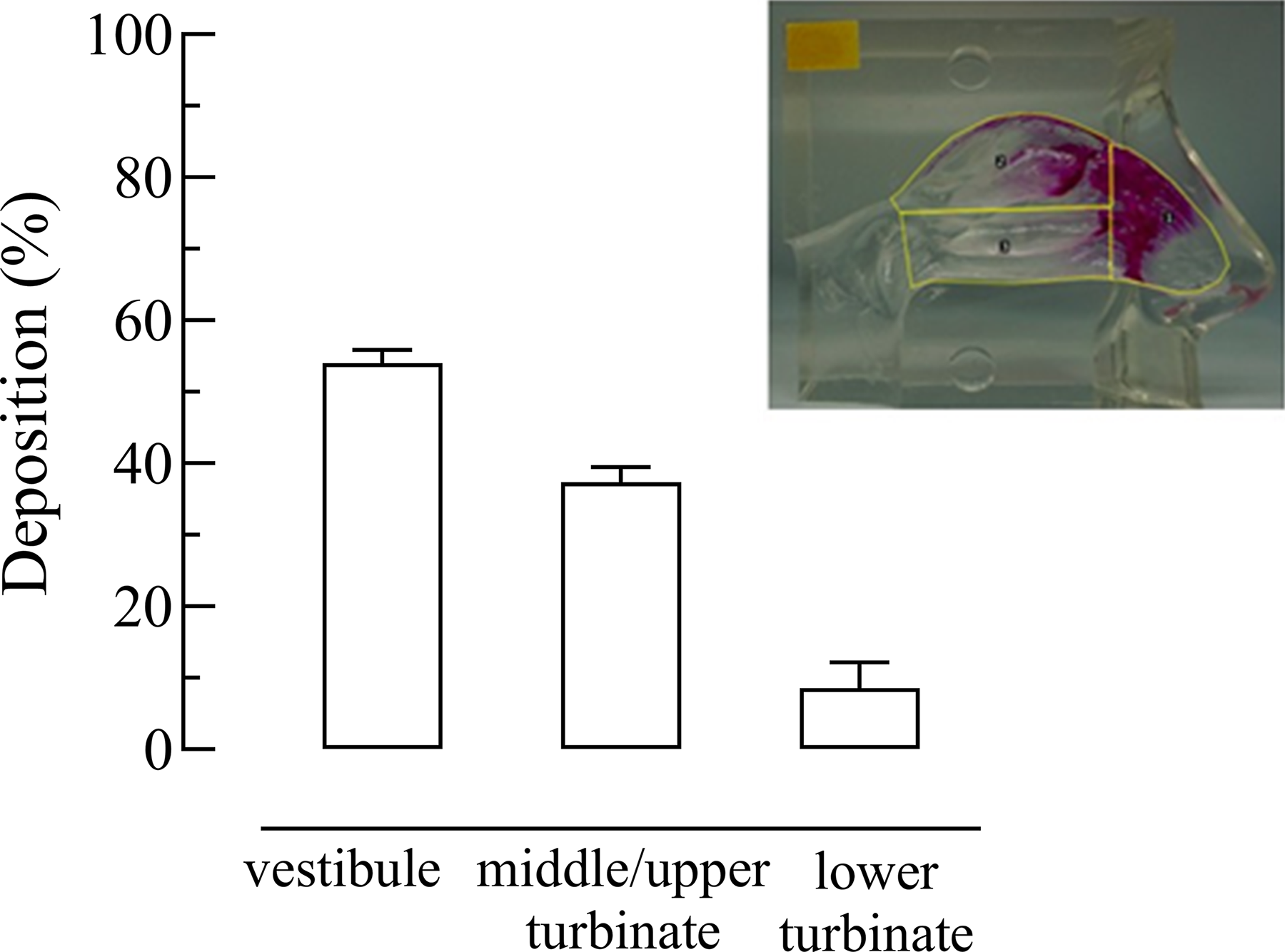
Mean (±standard deviation) percentage of mometasone furoate deposition in the vestibule, middle–upper turbinate, and lower turbinate. The inset shows a representative image of deposition pattern after a single actuation of the VP3 device at a 45° angle in the Koken® nasal cast.
Dripping studies demonstrated that the formulation exhibited adequate adhesion to inclined surfaces, with limited run-off. When 50 µL of formulation was pipetted onto the inclined surface, the mean drip length after 1 minute was 5.22 ± 0.01 cm. Under dynamic conditions, when the spray was actuated from 3 cm distance, the mean drip length was 8.32 ± 0.01 cm. Rheological analysis showed that the formulation had a mean viscosity of 14.36 ± 3.23 mPa·s. Repeated measurements across three replicates confirmed stability and reproducibility of viscosity values.
Spray plume evaluation at 3 and 6 cm distances showed symmetrical and reproducible deposition patterns (Fig. 3). At 3 cm, the plume was compact with a defined circular shape, while, at 6 cm, it expanded predictably, maintaining overall symmetry. Image analysis confirmed that diameters, areas, and perimeters were consistent across replicates, with minimal variability.
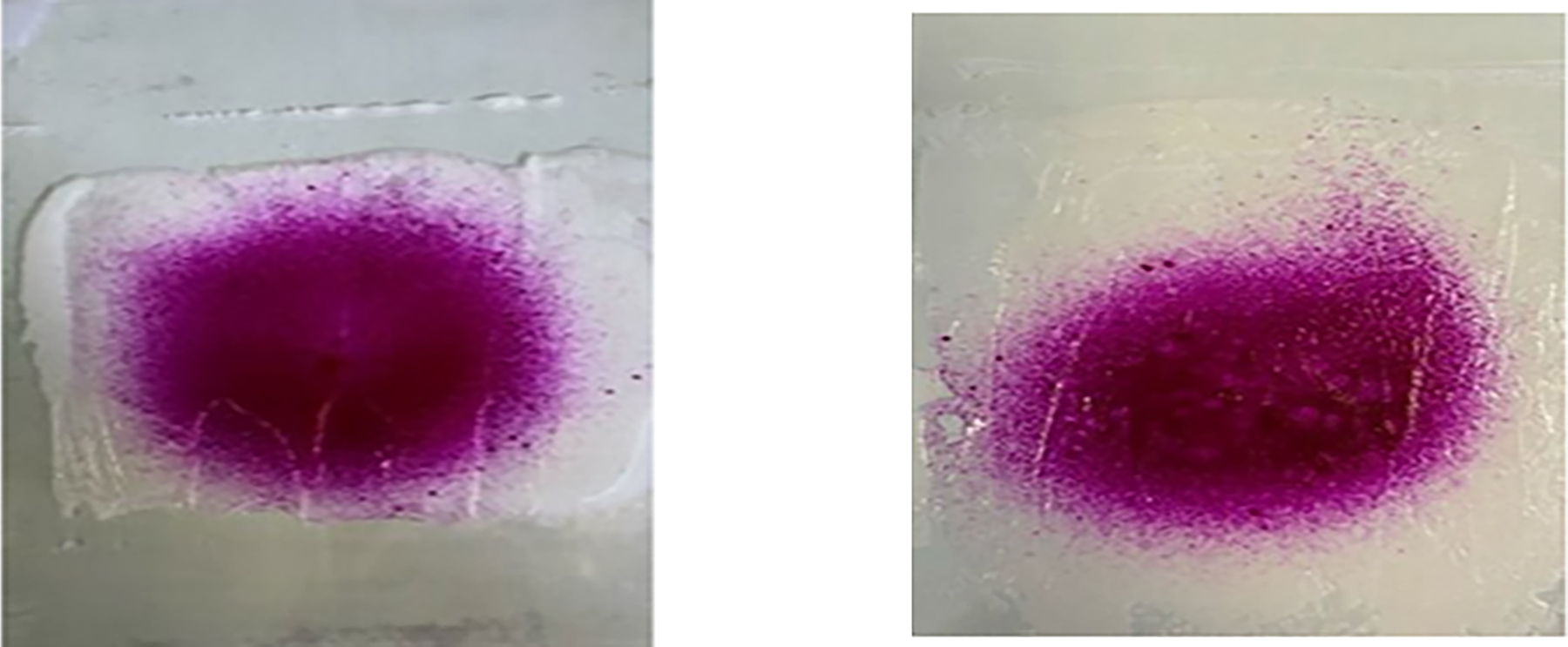
Representative spray plume geometry after a single actuation of the VP3 nasal spray device at distances of 3 cm (left) and 6 cm (right) from the nozzle tip obtained on a Sargel®-coated surface.
In vivo findings
Ten patients were enrolled (8 females, mean age 56.0 ± 8.4 years), as summarized in Table 1. The most frequent diagnostic category was allergic rhinitis (n = 7), followed by nonallergic rhinitis (n = 2) and chronic rhinosinusitis with nasal polyps (n = 1). All patients reported chronic cough associated with postnasal drip and nasal obstruction. Baseline intranasal therapy consisted of mometasone monotherapy (n = 2), mometasone combined with nasal lavage (n = 6), azelastine (n = 1), or fluticasone dipropionate (n = 1). None had recent respiratory infections at the time of enrollment. No withdrawals occurred, and adherence to the switch protocol was complete.
Baseline Clinical and Demographic Characteristics of the Chronic Cough Patients (n = 10)
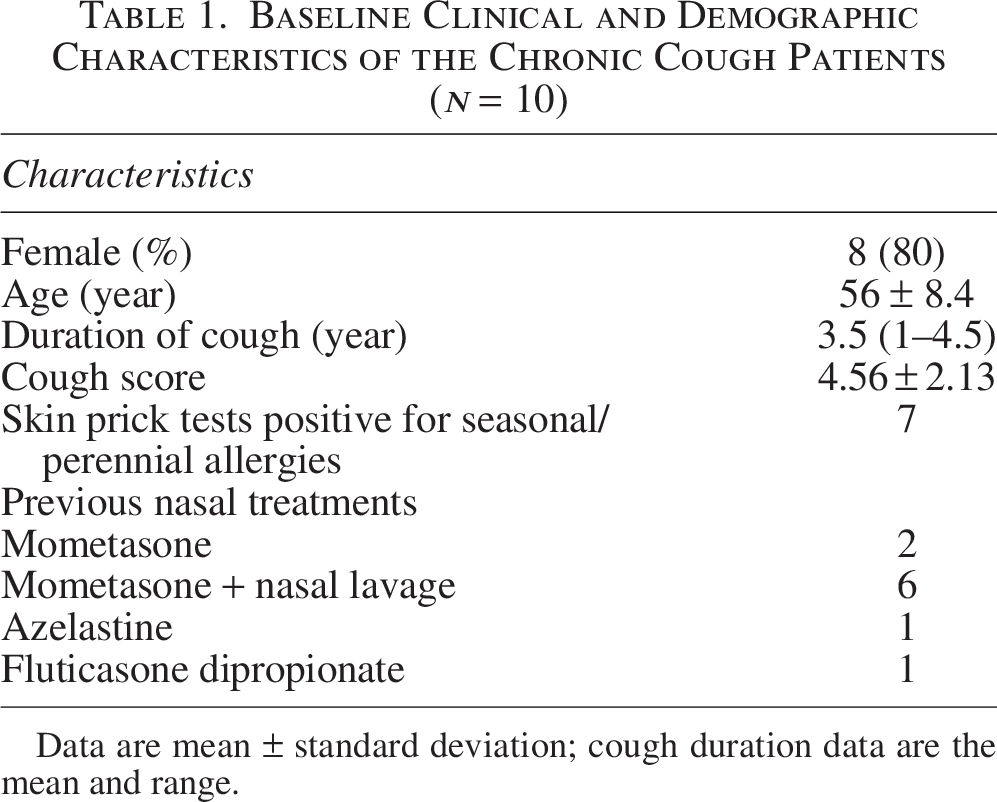
Data are mean ± standard deviation; cough duration data are the mean and range.
Global satisfaction remained stable following the switch. Mean TSI scores were 63.78 ± 4.58 with prior sprays and 64.26 ± 3.39 with the VP3 device. Overall, VAS ratings were similarly comparable (6.14 ± 1.55 cm vs 6.78 ± 3.18 cm).
At the domain level (Table 2), significant improvements were observed for convenience (p < 0.05) and for perceived duration of effect (p < 0.05). Fast-acting sensation demonstrated a nonsignificant trend toward improvement (p = 0.059). No statistically significant worsening was detected in any sensory domain. The dryness score showed a small numerical decrease after switching, but this difference was not statistically significant. Satisfaction with taste, aftertaste, smell, irritation, urge to sneeze, dripping, and symptom control remained stable. In terms of importance ratings (i.e., the relative weight of each attribute in the overall evaluation and independent of satisfaction), dripping down the nose/throat and duration of effect were rated as more important after switching (p < 0.05 for each). Importantly, this reflects a change in salience rather than increased symptom severity or frequency (e.g., more dripping or dryness). Conversely, dryness was rated as less important after switching (p < 0.05, Table 2). There were no decreases in the importance of other attributes. No new or exacerbated adverse sensory effects were reported during the study.
Satisfaction and Importance Scores
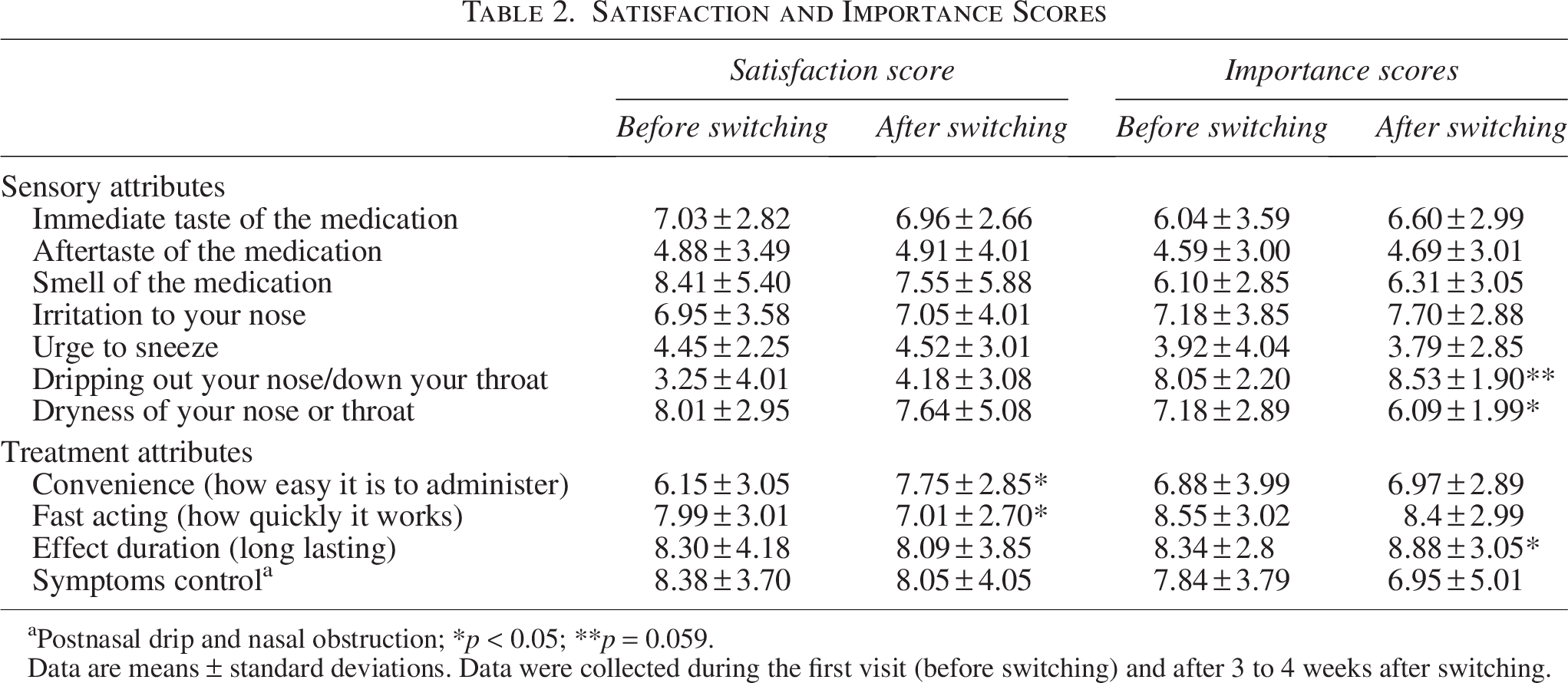
Postnasal drip and nasal obstruction; *p < 0.05; **p = 0.059.
Data are means ± standard deviations. Data were collected during the first visit (before switching) and after 3 to 4 weeks after switching.
Discussion
The in vitro and in vivo findings were complementary, demonstrating that the VP3 device delivers predictable nasal deposition together with acceptable sensory performance in clinical use. Laboratory testing showed reproducible deposition, an apparent viscosity in the tested range, and limited dripping, whereas patients reported preserved overall satisfaction and targeted improvements in usability domains. These aligned results support translational consistency between technical performance and patient-perceived tolerability. Importantly, this study was not designed to establish a quantitative in vitro/in vivo correlation; rather, the in vitro findings provide mechanistic plausibility for the sensory domains captured in the patient-reported assessments.
The extent and distribution of deposition observed in the nasal cast were consistent with previously reported values for marketed INCS devices and, importantly, extended beyond the anterior vestibule into turbinate regions. This coverage falls within the range reported for marketed intranasal sprays in similar cast models, 10 indicating effective deposition without excessive anterior loss. Most spray particles were delivered beyond the vestibule, thereby reaching the mucosal surfaces most commonly implicated in inflammatory processes such as allergic rhinitis and chronic rhinosinusitis. 2 Excessive anterior deposition is associated with irritation and limited therapeutic penetration, whereas adequate delivery to the turbinates is linked to both treatment efficacy and improved comfort. The limited drip lengths observed in the retention tests further support the notion that the formulation maintains contact with the mucosal surface without rapid gravitational run-off. The longer path observed during active spraying is expected given the greater initial droplet momentum and higher effective deposited volume. However, both run-off distances remained modest, indicating that the formulation is sufficiently viscous to maintain mucosal adherence without causing prolonged anterior flow. Taken together, these findings suggest a favorable balance between retention and spray performance (plume formation and ease of actuation), a property likely to reduce posterior drip sensations in vivo and to influence tolerability, as both anterior leakage and posterior drip are key drivers of patient perception in routine use.
The measured apparent viscosity likely contributes to the observed balance between retention and spray performance: formulations that are too low in viscosity tend to drip or produce unwanted postnasal flow, whereas excessively viscous formulations may impede atomization and dose release. Importantly, because this product is a suspension containing viscosity-enhancing agents, it is expected to exhibit non-Newtonian, shear-thinning rheology such that the apparent viscosity decreases under the higher shear stresses encountered during actuation and atomization and increases again after deposition. This behavior is consistent with efficient spray formation during delivery while supporting mucosal adhesion and limiting gravitational run-off after application. Under shear conditions used in our rheological test, the formulation exhibited an apparent viscosity that is commonly described as intermediate for intranasal formulations, 16 suggesting adequate mucoadhesion while remaining sufficiently fluid to ensure efficient atomization and delivery. 17 The uniformity of the spray pattern further indicates that the device consistently atomizes the formulation, supporting the concept of a device–formulation synergy, in which nozzle architecture and rheological properties interact to maintain stable spray characteristics.18,19 In practice, this physicochemical profile aligns with the sensory domains that patients perceive most readily—such as dripping, coating, and comfort—providing a mechanistic basis for the favorable usability ratings observed in the switch phase.
The maintenance of global satisfaction, coupled with significant improvements in convenience and perceived duration of effect, indicates that patients recognized added functional value without experiencing new drawbacks. The nonsignificant trend toward faster perceived onset further suggests that usability-related aspects of delivery, rather than pharmacological potency, contributed to more favorable early impressions of treatment. This pattern is consistent with clinical experience, in which patients frequently evaluate INCS therapy on the basis of its immediate sensory profile rather than on its delayed anti-inflammatory effect. 10
Adherence to INCSs is often undermined by tolerability issues such as unpleasant taste, irritation, anterior or posterior dripping, or dryness. 9 Although pharmacological efficacy is broadly comparable across available corticosteroid formulations, small differences in sensory experience can influence persistence more than potency.20,21 In the present study, global satisfaction was maintained after switching to the VP3 device, but improvements were noted in domains such as convenience and perceived onset of action. These attributes are relevant in UACS, where sensory burden and symptom salience strongly influence perceived treatment adequacy. The observation that no negative trade-offs were reported in other domains supports the acceptability of the device for routine use.
The shift in importance ratings for attributes such as dripping, dryness, and duration of effect likely reflects increased patient awareness of these dimensions once the delivery experience changed. This reprioritization aligns with real-world decision-making, where patients often persist with a therapy that feels more acceptable, even in the absence of substantial change in global satisfaction scores. The increase in the rated importance of these tolerability-linked attributes suggests that patients were not merely satisfied with the device but were actively reweighting which aspects of performance they considered meaningful for continued use. In clinical terms, this shift in sensory salience supports a behavioral mechanism for adherence: day-to-day comfort, reduction in postnasal drip burden, and perceived duration of effect become primary drivers of persistence once a neutral baseline of overall satisfaction has been achieved.
Previous investigations have shown that sensory differences between INCS sprays can affect both preference and adherence.4,5 Comparative studies of fluticasone, budesonide, and mometasone have demonstrated variability in aftertaste, irritation, and perceived drip, which, in turn, influenced patient continuation rates. 4 Device design has also been shown to affect deposition patterns in nasal cast and scintigraphy models,22,23 although few studies have linked these findings directly with patient-reported outcomes. The present study contributes to this gap by providing an integrated translational evaluation in which laboratory performance characteristics for a single formulation–device combination are interpreted alongside patient-reported treatment experience after switching. Given the single-device design, these findings should not be interpreted as demonstrating a quantitative convergence/correlation; rather, they provide mechanistic plausibility and hypothesis-generating alignment that should be tested in comparative studies across multiple devices/formulations. In this context, the VP3 device demonstrated consistent in vitro performance in our test conditions without compromising sensory tolerability, which is clinically relevant for long-term use and particularly important in patients with UACS, who are often sensitive to upper airway sensations.
Adherence remains a barrier to sustained benefit from INCSs. Patients frequently discontinue treatment due to perceived sensory burden rather than inadequate efficacy.9,21 A device that can maintain satisfaction while improving usability-related attributes may therefore facilitate persistence, particularly in patients with UACS given their highly sensitive upper airway sensations. The finding that satisfaction is preserved after switching suggests that the formulation–device combination can be introduced without jeopardizing engagement when device changes are required.
This study has limitations. The sample size was small, and the follow-up period was short. The nasal cast cannot fully reproduce mucociliary clearance or anatomical variability. The study was not designed or powered to assess long-term adherence or symptom outcomes. Accordingly, we could not test whether between-product differences in in vitro performance translate into between-product differences in patient-reported outcomes, nor could we formally model in vitro/in vivo associations at the individual level. Future adequately powered, head-to-head studies comparing multiple nasal spray devices/formulations should quantify in vitro differences (regional deposition and postdeposition liquid motion/retention) and evaluate whether these predict patient-reported sensory perceptions and satisfaction. Nonetheless, the integration of mechanistic and patient-reported data strengthens the validity of the findings and reduces the likelihood that the observed effects were incidental or device-independent. Deposition in the cast was quantified as surface area coverage (detectable wetting) rather than regional mass recovery; therefore, our results primarily reflect distribution/extent of surface contact and not directly the absolute dose deposited within each region. An additional limitation is that the in vitro characterization was performed only for the VP3 device after switching, whereas comparable in vitro measurements were not collected for the conventional preswitch nasal spray devices. As a result, we cannot determine which in vitro performance parameters change significantly upon switching (e.g., regional deposition patterns and postdeposition liquid motion/retention), nor can we directly attribute observed changes in patient-reported outcomes to specific between-device in vitro differences. Future prospective head-to-head studies should include standardized in vitro testing of both devices/formulations in parallel with patient-reported outcomes to enable robust between-product comparisons and formal in vitro/in vivo linkage.
In summary, the VP3 device demonstrated stable in vitro performance and favorable patient acceptability in individuals with chronic cough attributed to upper airway disease. The convergence of deposition characteristics with usability-related patient preferences supports its suitability for INCS delivery. Future research in larger cohorts with longer follow-up and direct head-to-head comparisons will help determine whether these performance attributes translate into sustained adherence and improved clinical outcomes.
Conclusions
This translational study demonstrates that a mometasone furoate nasal spray delivered through the VP3 device provides consistent in vitro performance with favorable tolerability in patients with chronic cough attributed to upper airway disease. The correspondence between deposition behavior, retention characteristics, and patient-reported usability suggests that formulation–device synergy contributes meaningfully to treatment acceptability. Larger, longer-term comparative studies are warranted to determine whether these advantages translate into sustained adherence and improved clinical outcomes.
Footnotes
Author Disclosure Statement
The authors declare no conflict of interest related to the present study.
Funding Information
This study was not funded.
Authors’ Contributors
F.L., F.B., A.S., and F.S. conceived and designed the study. F.S., F.B., and V.P. performed the in vitro experiments. A.S., G.F., G.V., and L.B. contributed to patients’ enrollment, collection, and analysis of data; A.S. conducted and supported the statistical analysis. F.L., F.B., F.S., and A.S. wrote the first draft of the article, on which all authors commented and provided intellectual input. F.L., F.B., and F.S. accessed and verified the underlying data. All authors had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Supplemental Material
Abbreviations
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.