
Abstract
Background:
Asthma is characterized by variable airway obstruction, and proper inhaler choice and use are critical for effective treatment. This study aimed to identify factors influencing treatment response in newly diagnosed patients started on dry powder inhalers (DPIs) or metered-dose inhalers (MDIs).
Methods:
Between March and September 2025, 177 newly diagnosed asthma patients were screened. Eighty patients with at least high-school education, correct inhaler use, and good adherence were included (40 DPI, 40 MDI). Pulmonary function, respiratory muscle strength, Asthma Control Test (ACT), and handgrip strength (HGS) were assessed at baseline and after one month.
Results:
After one month, improvements in forced expiratory volume in 1 second (FEV1) (% predicted), maximum inspiratory pressure (MIP) and MIP (%), and maximum expiratory pressure (MEP) (%) were significantly greater in the DPI group compared with the MDI group (p = 0.03, 0.04, 0.02 respectively). In multivariate regression, among MDI users, MIP (kPa) (B = −11.305, p = 0.001), MIP (%) (B = −0.902, p = 0.003), ACT (B = 1.277, p = 0.014), and HGS (B = 0.103, p = 0.039) were independent predictors of ΔFEV1 (%). Among DPI users, MIP (kPa) (B = 11.987, p = 0.015), MIP (%) (B = 1.041, p = 0.009), MEP (kPa) (B = −6.554, p = 0.014), MEP (%) (B = −0.816, p < 0.001), and HGS (B = 0.201, p = 0.005) were significant determinants of ΔFEV1.
Conclusion:
DPIs may be preferable for patients with higher inspiratory muscle strength, whereas MDIs may be better for those with lower MIP. HGS appears to be an important factor for both inhaler control and treatment efficacy.
Introduction
Asthma is a common respiratory disease marked by chronic airway inflammation and fluctuating airway obstruction, often accompanied by flare-ups. It can affect people of all ages, from children onward, and can greatly diminish quality of life. Proper medication management and consistent patient monitoring are essential strategies to control the condition, ease symptoms, and prevent flare-ups. 1
Inhaled medications are crucial in asthma management, providing symptom control through their anti-inflammatory and bronchodilator effects. Metered-dose inhalers (MDIs) and dry powder inhalers (DPIs) are the most commonly used forms in clinical practice. 2 When used correctly, inhaled treatments offer benefits such as minimal systemic side effects, quick onset of action, and direct delivery to the lungs. However, patient response to treatment can vary based on factors like the inhaler device type, the patient’s inspiratory capacity, inhaler technique, associated clinical features, and adherence to the treatment plan. 3
Recent studies have thoroughly explored the physiological and clinical factors that influence inhaler treatment effectiveness. Many studies have demonstrated that success with DPI treatment depends on having an adequate inspiratory flow rate and inspiratory muscle strength, and that in patients with low values, forced expiratory volume in 1 second (FEV1) increases are significantly limited. 4 Mahler et al. reported that the bronchodilator response to DPIs is notably reduced in individuals with low MIP and Peak Inspiratory Flow Rate (PIFR). In MDI users, inhalation–activation coordination is crucial for treatment effectiveness, and it has been observed that high inspiratory pressures can sometimes cause paradoxical effects. 5 It has been demonstrated that higher Asthma Control Test (ACT) scores lead to better clinical responses, whereas lower scores limit treatment success. Although significant links have been reported between handgrip strength (HGS), respiratory function, and inspiratory flow capacity, no research has explored how HGS influences inhaler treatment response. 6 This indicates that the effectiveness of inhaler treatment depends not only on the pharmacological agent but also on the patient’s specific physiological capacity.
This study aimed to compare the factors influencing the effectiveness of MDI and DPI treatments in patients with asthma who used their inhaler correctly and consistently, and had the same level of education. This was intended to better demonstrate the relationship between physiological and clinical factors that affect treatment response across different inhaler types and changes in lung function.
Materials and Methods
Study design
This prospective randomized study included patients who presented to our hospital’s Pulmonology outpatient clinic between March 2025 and September 2025 with complaints of shortness of breath, cough, exertional dyspnea, and chest pain, and who were diagnosed with asthma based on clinical, functional, and/or laboratory criteria. Patients were diagnosed according to current guidelines (GINA criteria). Eligible patients were started on either MDI or DPI and were randomly assigned to two groups.
All patients received standardized training on the correct use of inhalers at the start of treatment, and device usage techniques were demonstrated and practiced. Patients were regularly monitored for proper inhaler use throughout the study. Patients were re-evaluated before treatment and one month afterward, with clinical data and pulmonary function tests prospectively recorded.
The study was approved by the Atatürk University Faculty of Medicine Clinical Research Ethics Committee and was conducted in accordance with the principles of the Declaration of Helsinki. All participants received detailed information about the study and provided written informed consent. Participation was voluntary, and patients were informed that they could withdraw at any time.
Study population
A total of 177 patients started inhaler therapy during the study period. Two main criteria guided the selection of participants: Their ability to use inhalers correctly and accurately and an education level with a minimum of high school education or higher. This was to ensure that participants could properly understand and perform inhaler techniques. Patients were then randomized into two groups. Patients included in the study were assigned to study groups using a simple randomization method with Microsoft Excel®. Group 1 consisted of patients using MDIs (n = 97), and group 2 consisted of patients using DPIs (n = 80). Patients were expected to have a timely first-month follow-up, consistent medication use, and grade A MDI and DPI use according to the scoring performed by Lenney et al. 7 A total of 80 patients were recruited, with 40 in each group, meeting the specified criteria (Fig. 1). Based on the study by Vázquez-González et al., the sample size was calculated beforehand using G*Power, assuming a medium effect size (Cohen’s d = 0.63), α = 0.05, and a statistical power = 0.80 for changes in lung function between two independent groups; a target of 40 patients per group (80 in total) was achieved. 8
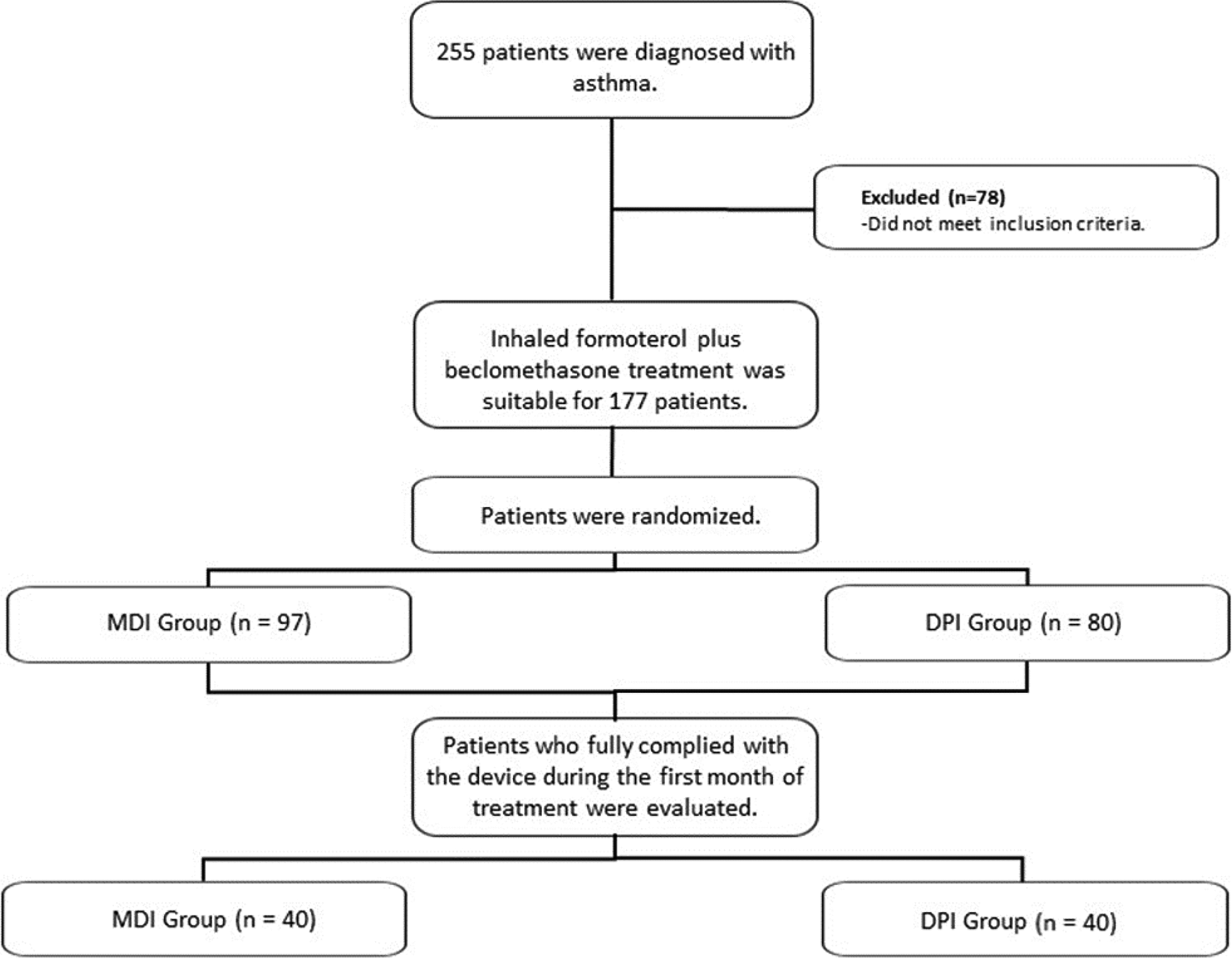
CONSORT diagram.
Our study included newly diagnosed, treatment-naive asthma patients aged 18 years and older who met the criteria outlined above, volunteered to participate, and signed informed consent. All participants were completely inhaler-naive and had not received any prior inhaled therapy before enrollment. Active tobacco smokers at the time of enrollment were excluded. Patients with other chronic lung diseases such as Chronic Obstructive Pulmonary Disease PFT: Pulmonary Function Test (COPD) or interstitial lung disease, those experiencing acute exacerbations, individuals who made significant technical errors while using their inhalers, those with advanced neurological or cognitive impairments, pregnant or breastfeeding women, and those who did not provide consent were excluded.
Medical treatment
All patients included in the study were started on standard inhaler combination therapy. Patients in the MDI group received two doses twice daily of a Foster® metered-dose inhaler (ODI) (beclometasone dipropionate 100 µg + formoterol fumarate 6 µg/puff), whereas patients in the DPI group received two doses twice daily of a Foster Nexthaler (beclometasone dipropionate 100 µg + formoterol fumarate 6 µg/inhalation). The treatment lasted one month. All patients received standardized training on the proper use of inhaler devices before beginning the treatment, and their techniques were evaluated in practice. Patients were monitored regularly throughout the treatment period to detect device usage errors. No additional inhaler controllers or systemic steroids were given to patients during the study.
Adherence to inhaler therapy was assessed through patient self-report during follow-up visits and by reviewing regular medication use based on clinical interviews. Only patients demonstrating consistent daily use and correct inhaler technique during follow-up evaluations were included in the final analysis.
Maximum inspiratory pressure and maximum expiratory pressure measurement
Maximal inspiratory pressure (MIP) and maximal expiratory pressure (MEP) measurements were performed using the RP Check MIP & MEP & SNIP device (MediTrack, Belgium), a portable and validated device specifically designed for assessing respiratory muscle strength. Measurements were conducted with participants seated upright and wearing a nose clip to prevent air leakage. For MIP, participants were instructed to exhale fully to residual volume before performing a maximal inspiratory effort against an occluded mouthpiece. For MEP, participants first inhaled fully to total lung capacity before exerting a maximal expiratory effort against the mouthpiece.
Each measurement was repeated at least three times to ensure reliability, with the highest value recorded as the final result. Rest periods of at least one minute were provided between attempts to prevent fatigue and ensure consistency. All participants received verbal encouragement during the tests to maximize effort. Calibration of the device was performed daily prior to measurements to maintain accuracy. This methodology adhered to the guidelines outlined by the American Thoracic Society (ATS) and the European Respiratory Society (ERS) for respiratory muscle strength evaluation. 9
PFT application
The rules that patients should follow before spirometry were announced to the patients in line with the ATS/ERS 2019 guideline. The movement to be performed was explained to the patient by the technician. Each patient performed three acceptable spirograms. Tests complying with the pulmonary function test reproducibility and acceptability criteria published by ATS/ERS in 2019 were included in the study. 10 The lower limits of normal parameters determined for the healthy population are presented by calculating on a spirometry device in accordance with the criteria in this declaration. Spirometry was performed by the same technician with Plusmed MIR SpiroLab III device.
Asthma Control Test
The ACT was given to all patients in the study before treatment and one month afterward. The ACT is a five-question self-evaluation that measures asthma symptom severity over the past four weeks. Each question is scored from 1 to 5, resulting in a total score ranging from 5 to 25. Patients completed the questionnaire on their own, and the scores were used in the analysis.
Hand grip strength test
A standard hydraulic hand dynamometer (Jamar®) was used to measure HGS. Measurements were obtained with patients seated upright, with the elbow flexed to 90°, the forearm in a neutral position, and the wrist slightly extended. Patients performed three maximal squeezes with each hand, with 60-second rest intervals between measurements. The highest value for each hand was recorded, and the measurement from the dominant hand was used in the analyses.
Statistical analysis
Statistical analyses of the data collected in the study were conducted using SPSS for Windows, version 27.0 (IBM Corp., Armonk, NY, USA). The distributional characteristics of continuous variables were evaluated using the Kolmogorov–Smirnov test and, if needed, the Shapiro–Wilk tests. Descriptive statistics were presented as mean ± standard deviation for normally distributed variables and as median (minimum–maximum) for variables that were not normally distributed. Categorical variables are shown as numbers (n) and percentages (%). For between-group comparisons, the independent samples t-test was used for normally distributed continuous variables, whereas the Mann–Whitney U test was applied to variables that were not normally distributed. The chi-square test or Fisher’s exact test, as appropriate, was used for comparisons of categorical variables. Spearman’s rank correlation analysis was employed to assess nonlinear relationships between variables. Multivariate regression analyses were performed to identify independent factors influencing the response to inhaler therapy; a stepwise method was applied by including significant variables in the model. The sample size was calculated beforehand using G*Power 3.1 software. A p value of <0.05 was considered statistically significant in all tests.
Results
Among the patients included in our study, the median age was 46.5 years (range 28–75) in the MDI group and 37 years (range 20–72) in the DPI group. No statistically significant difference was found between the ages of the patients (p = 0.13). There were 34 male patients (85%) in the MDI group and 24 male patients (60%) in the DPI group. Statistical analysis by gender showed a higher proportion of male patients in the MDI group (p = 0.023).
A total of 80 patients with a high school education or higher participated in our study. In the DPI group, 24 patients (60%) were high school graduates and 16 patients (40%) were university graduates; in the MDI group, 22 patients (55%) were high school graduates and 18 patients (45%) were university graduates. There was no significant difference between the two groups regarding education level (p = 0.742). Regarding smoking history, five patients (12.5%) in the MDI group and eight patients (20%) in the DPI group were former smokers, whereas the remaining participants had never smoked. There was no statistically significant difference between the groups in terms of smoking status (p = 0.36).
A comparison of the patients’ demographic data, pulmonary function tests, inspiratory and expiratory muscle strength, and ACT and HGS test levels is presented in Table 1. Accordingly, weight and body mass index (BMI) levels were higher in the MDI group (p = 0.003, 0.03, respectively). ACT and HGS levels were significantly lower in the DPI group compared to the MDI group (p = <0.001, 0.03, respectively).
Comparison of Pretreatment Demographic Data, Pulmonary Function Tests, Inspiratory and Expiratory Muscle Strength, Asthma Control Test Scores, and Hand Grip Strength Levels in Patients Receiving Metered Dose and Dry Powder Inhaler Therapy
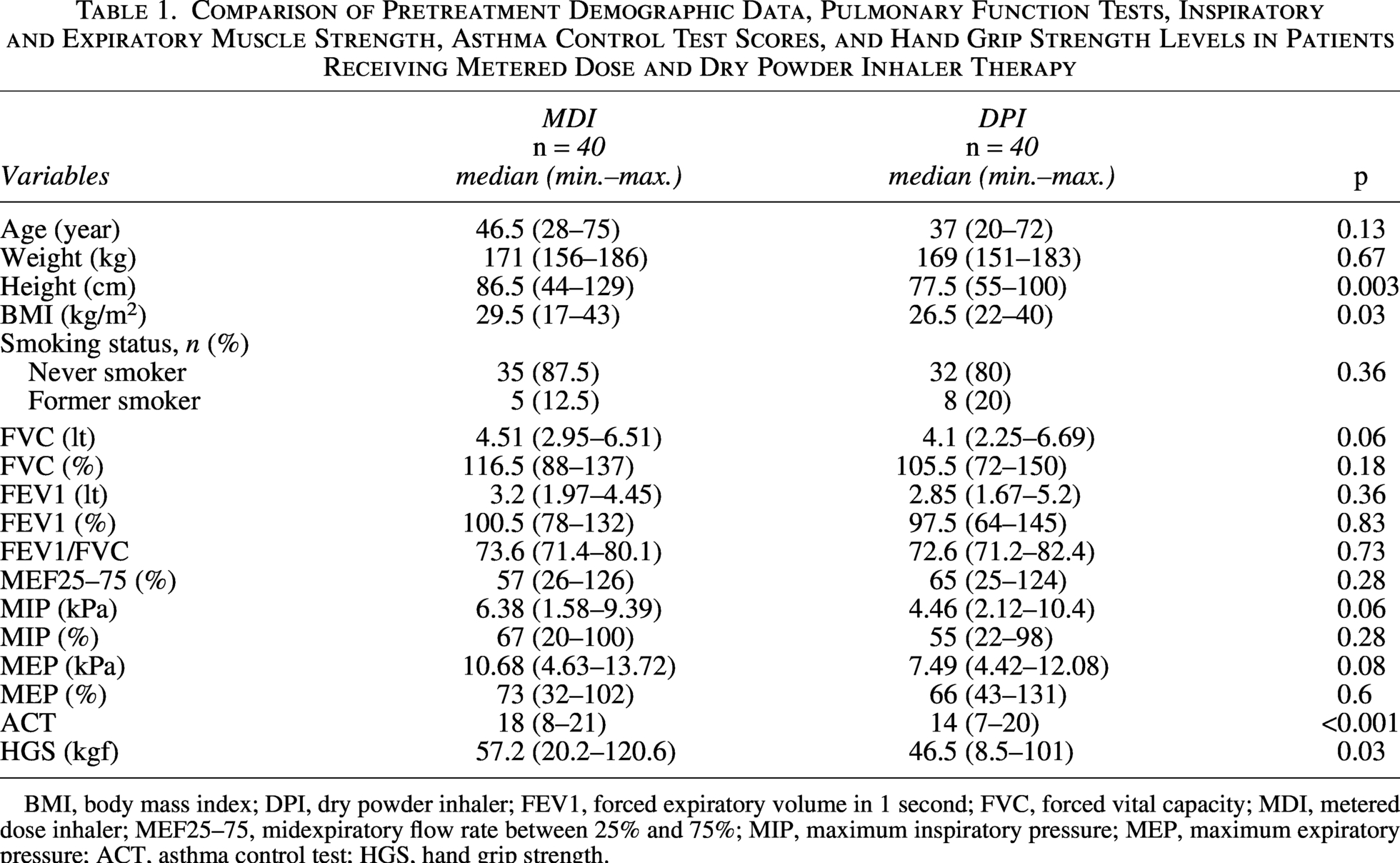
BMI, body mass index; DPI, dry powder inhaler; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; MDI, metered dose inhaler; MEF25–75, midexpiratory flow rate between 25% and 75%; MIP, maximum inspiratory pressure; MEP, maximum expiratory pressure; ACT, asthma control test; HGS, hand grip strength.
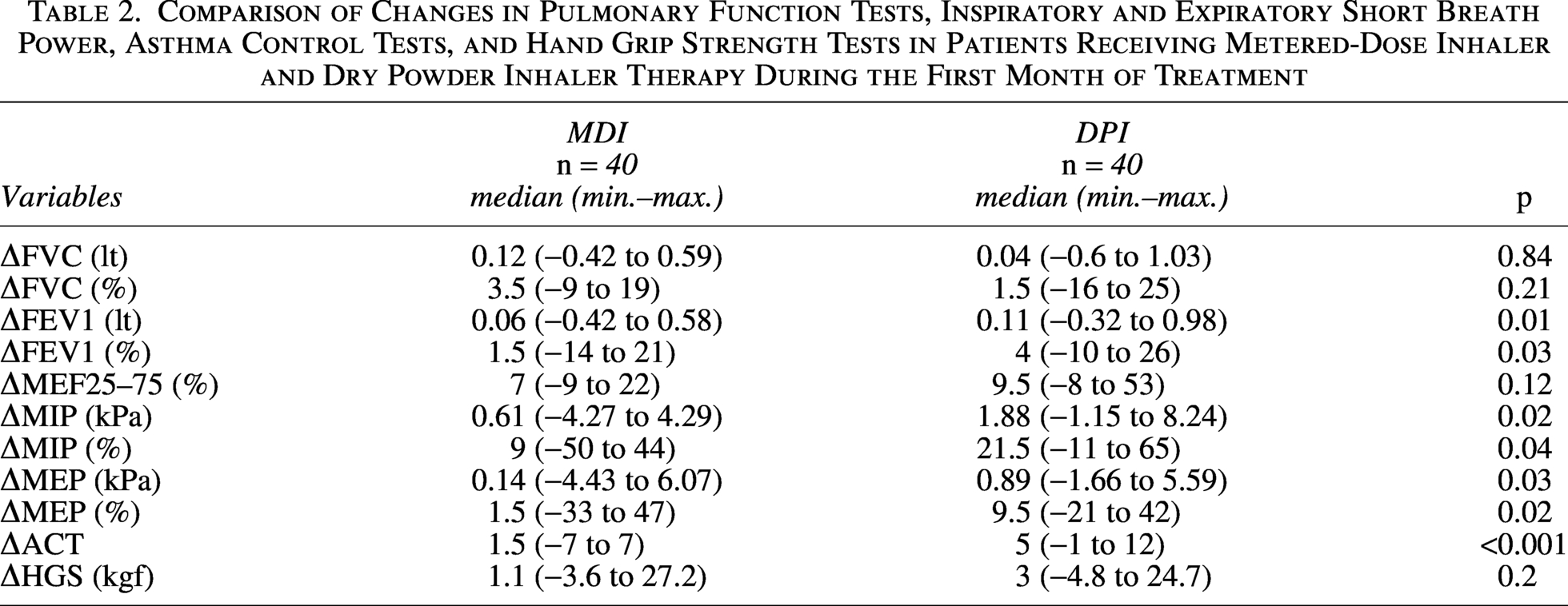
A comparison of changes in pulmonary function tests, inspiratory and expiratory muscle strength, ACT, and HGS test levels of the patients at the first month of treatment is shown in Table 2. Accordingly, it was observed that the increase in FEV1 (lt), FEV1 (%), MIP (kPa), MIP (%), MEP (kPa), MEP (%), and ACT levels increased more in DPI patients than in MDI patients (p = 0.01, 0.03, 0.02, 0.04, 0.03, 0.02, <0.001, respectively).
Comparison of Changes in Pulmonary Function Tests, Inspiratory and Expiratory Short Breath Power, Asthma Control Tests, and Hand Grip Strength Tests in Patients Receiving Metered-Dose Inhaler and Dry Powder Inhaler Therapy During the First Month of Treatment
The correlation analysis between posttreatment changes in pulmonary function test results and maximum expiratory muscle strength changes with initial maximum expiratory muscle strength is shown in Figure 2. Accordingly, a weak negative correlation was observed with ΔFVC (lt), ΔFVC (%) (R = −0.28, p = 0.012, R = −0.26, p = 0.02), and a weak negative correlation was seen with ΔFEV1 (lt) and ΔFEV1 (%) (R = −0.26, p = 0.02, R = −0.28, p = 0.01). In the analysis of correlation with ΔMEP (kPa) and ΔMEP (%), a negative but moderate correlation was also found (R = 0.45, p = 0.02, R = 0.48, p = <0.001).
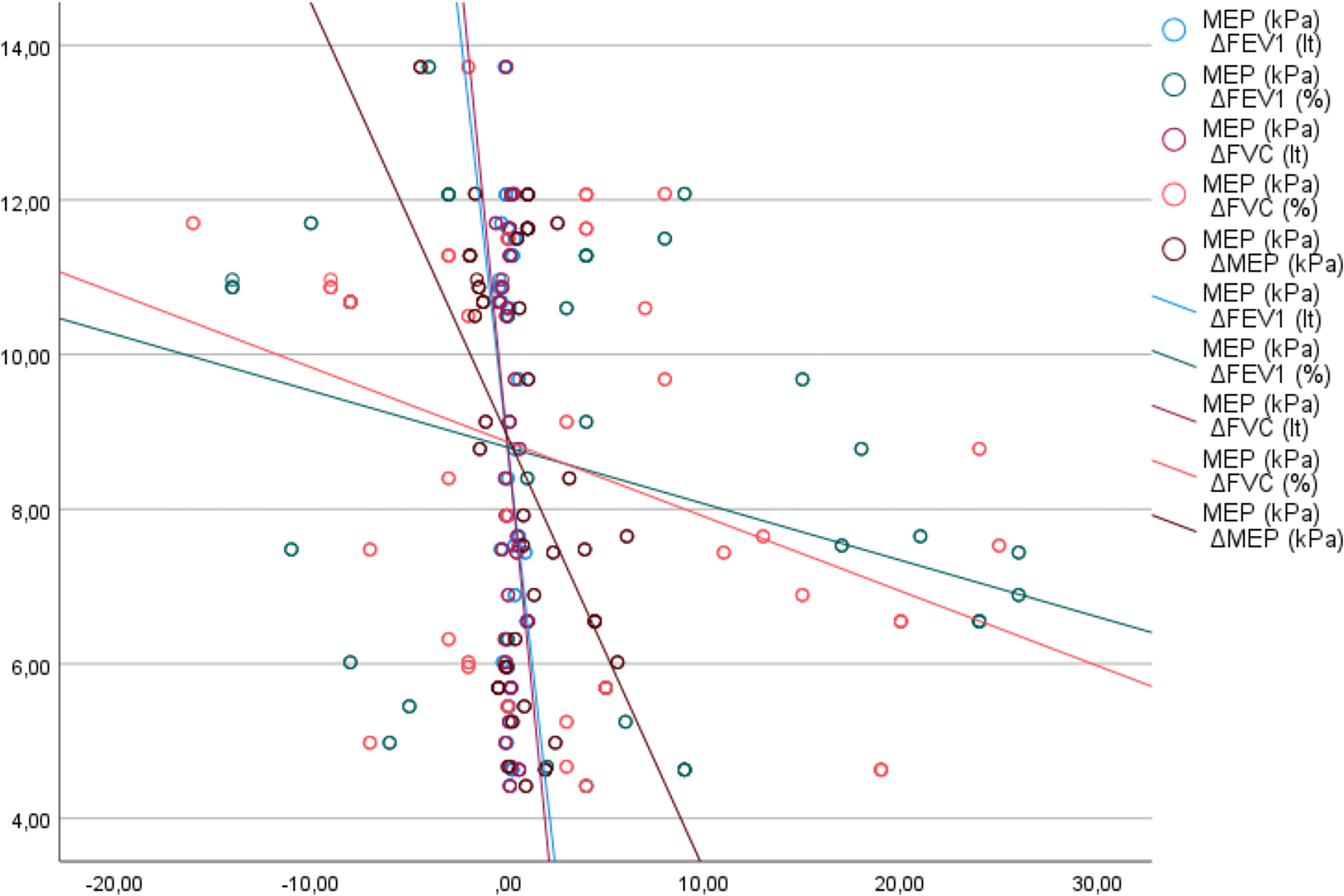
Correlation analysis of changes in posttreatment pulmonary function tests and maximum expiratory muscle strength with initial maximum expiratory muscle strength.
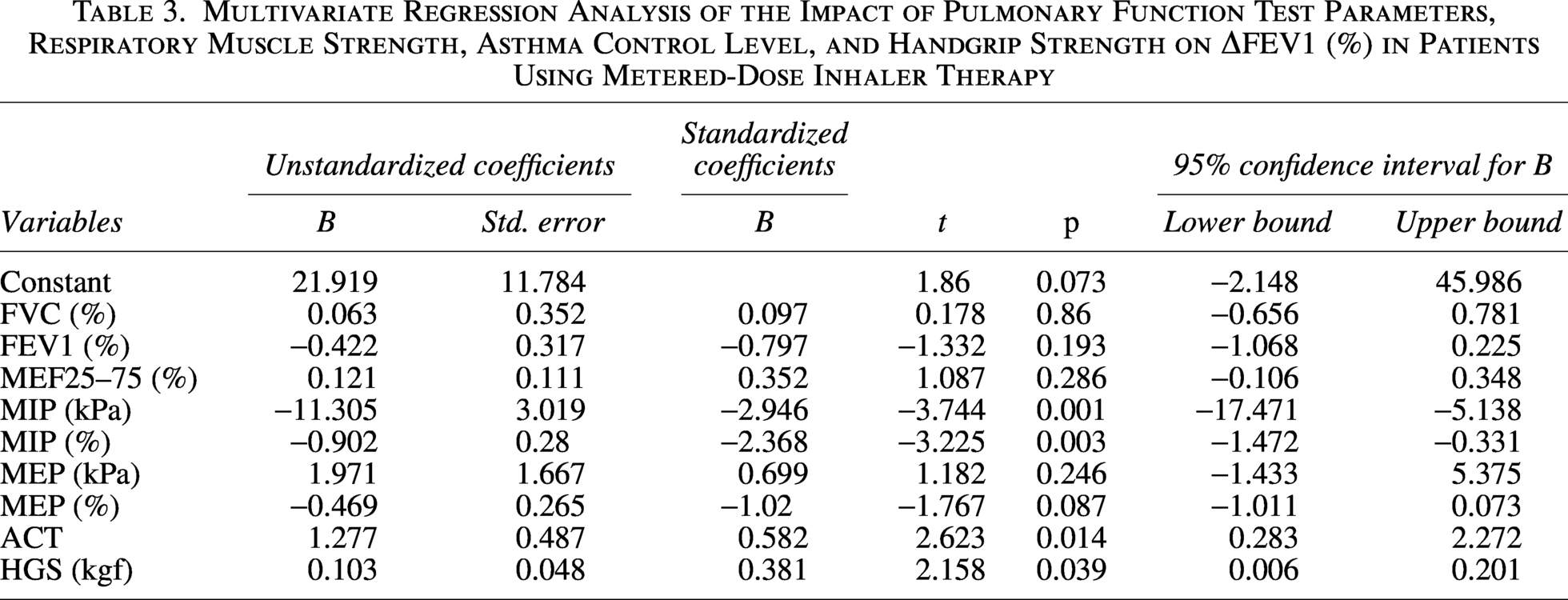
A multivariate regression analysis was performed to evaluate the factors affecting ΔFEV1 (%) in patients receiving MDI treatment, as shown in Table 3. According to the results, MIP (kPa) (B = −11.305, p = 0.001), MIP (%) (B = −0.902, p = 0.003), ACT score (B = 1.277, p = 0.014), and HGS (B = 0.103, p = 0.039) were identified as statistically significant independent predictors of change in ΔFEV1 (%).
Multivariate Regression Analysis of the Impact of Pulmonary Function Test Parameters, Respiratory Muscle Strength, Asthma Control Level, and Handgrip Strength on ΔFEV1 (%) in Patients Using Metered-Dose Inhaler Therapy
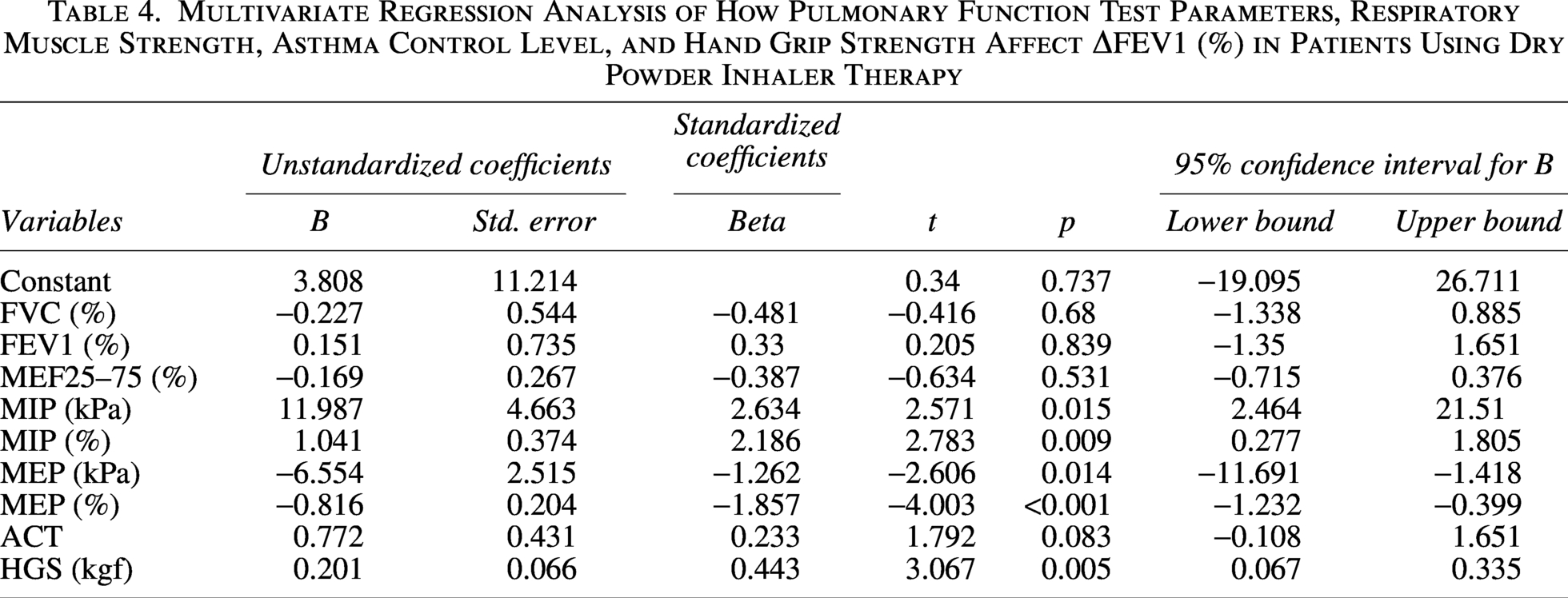
A multivariate regression analysis conducted to assess the factors influencing ΔFEV1 (%) in patients receiving DPI treatment is shown in Table 4. In this analysis, MIP (kPa) (B = 11.987, p = 0.015), MIP (%) (B = 1.041, p = 0.009), MEP (kPa) (B = −6.554, p = 0.014), MEP (%) (B = −0.816, p < 0.001), and HGS (B = 0.201, p = 0.005) were identified as statistically significant independent predictors of ΔFEV1 (%).
Multivariate Regression Analysis of How Pulmonary Function Test Parameters, Respiratory Muscle Strength, Asthma Control Level, and Hand Grip Strength Affect ΔFEV1 (%) in Patients Using Dry Powder Inhaler Therapy
Discussion
In our study, increases in FEV1, MIP, MEP, and ACT levels were observed in both patient groups at the first-month follow-up for patients using MDI and DPI, but this increase was greater in those using DPI than in the MDI group. When evaluating the relationship between changes in pulmonary function tests, muscle strength parameters, and baseline functional parameters, greater changes in FEV1, FVC, and MEP were seen in patients with lower baseline MEP levels. Multivariate regression analysis in patients using MDIs showed that lower MIP, higher ACT, and HGS levels led to a greater increase in FEV1, while in DPI patients, the increase in FEV1 was more significant with higher MIP, HGS, and lower MEP.
Inhaled medications are essential in managing asthma by controlling the condition and alleviating symptoms. Guidelines highlight that choosing the right inhaler and using it with proper technique are just as important as the medication’s effectiveness for achieving symptom control. 11 Among inhaler devices, MDIs and DPIs are the most frequently used methods of delivery. 12 Although the pharmacological components of both devices are similar, their mechanisms for delivering medication to the lungs differ. MDI devices release medication as a pressurized aerosol, making simultaneous use and inhalation critical, whereas DPI devices rely on an adequate inspiratory flow rate.12,13 Thus, choosing the right device and ensuring successful treatment depend on individual factors such as the patient’s inspiratory capacity, muscle strength, coordination skills, and adherence to treatment. Research shows that a low inspiratory flow rate can limit effectiveness in DPI users, while in MDI users, poor inhalation-activation coordination can cause inaccurate dosing.2,14,15
Current literature features numerous studies on the physiological and clinical factors that influence inhaler treatment effectiveness. It emphasizes that inspiratory flow rate and inspiratory muscle strength are crucial for treatment success, especially in DPI users. Mahler et al. showed that inhaler success depends on an optimal inspiratory flow rate, and DPI effectiveness is significantly reduced in patients with low flow rates. 16 Similarly, Weers et al. reported that failing to provide adequate flow rates in passive DPI devices disrupts particle dispersion, limiting drug delivery to the distal airways. 4 Suriyakul et al. found significant correlations between HGS and PIFR, suggesting that HGS may indirectly indicate inspiratory muscle capacity. 17 Tsuburai et al. demonstrated that HGS levels correlate with inhalation rates, particularly in individuals with mild COPD, emphasizing the importance of physical capacity in inhaler effectiveness. 6
In MDI users, treatment success depends on the correct timing of inhalation activation due to the device’s pressurized aerosol mechanism. Clark and Hollingworth have shown that technical errors in MDI devices most often arise from inadequate activation–inhalation coordination. Additionally, various studies have demonstrated that treatment success depends not only on inhaler technique but also on the level of clinical control. 18 The positive correlation between ACT scores and lung function parameters has been consistently shown in both pediatric and adult asthma populations, with higher scores linked to better functional outcomes.19,20 These findings indicate that inhaler treatment effectiveness relies heavily not only on pharmacological properties but also on individual factors like inspiratory capacity, muscle strength, coordination ability, and level of clinical control.
In our study, we found that weight, BMI, ACT, and HGS levels were higher at baseline in the MDI and DPI patient groups. Although patients were randomized, baseline differences in ACT and HGS levels may reflect natural variability within a relatively small sample size rather than systematic selection bias. Despite initial differences between the groups, the absence of a significant correlation between weight and BMI levels and the pulmonary function test and respiratory muscle strength parameters that changed during treatment suggests that these variables did not influence the main results of our study. Differences between ACT and HGS levels were eliminated through analysis within each group.
In assessments conducted after one month of treatment, greater increases were observed in FEV1, respiratory muscle strength, and ACT levels in the DPI group; however, given the randomized parallel design without a cross-over phase, these findings should be interpreted as between-group observations rather than definitive superiority of one device over another. The higher inspiratory pressure applied during inhalation in patients using DPI may be associated with the greater increases observed in respiratory muscle strength and lung function parameters. This could have led to effective bronchodilation, reducing air trapping and elevating both MEP and FEV1 levels. In this group, which had lower initial ACT scores, it is believed that increased respiratory muscle strength and FEV1 levels also helped improve ACT scores.
It is noteworthy that in the multivariate regression analysis conducted in the MDI group, low MIP, high HGS, and high ACT scores were significantly linked to changes in FEV1. With MDI devices, the technique of slow and deep inhalation combined with device activation is more important than quick inspiration. The tendency to breathe slower and deeper in individuals with low maximum inspiratory pressure may have increased compliance with the device technique. Higher HGS enhances device stability, improves coordination of inhalation activation, and helps achieve adequate inspiratory volume. Additionally, higher ACT scores may have contributed to better initial disease control, potentially increasing both adherence to inhaler technique and the response to treatment. The combination of these three factors may explain the physiological basis of the bronchodilator response in the MDI group.
In the DPI group, high MIP, low MEP, high HGS, and high ACT scores were significantly linked to FEV1 change, aligning with the physiological needs of the device. Effective drug release and particle dispersion in DPI devices depend on the patient’s inspiratory flow strength. Patients with high MIP levels generate enough negative pressure during inhalation, allowing more effective drug delivery to the distal airways. It is believed that low MEP levels may have contributed to slower exhalation after inhalation, allowing particles to remain in the airways longer and increasing lung deposition. Indeed, correlation analyses between baseline MEP levels and PFT and MEP changes support this conclusion. High HGS indicates greater muscle strength related to inspiratory capacity and enhances the stability of the inhalation maneuver. High ACT scores, which reflect good clinical control, help improve correct inhaler technique and treatment adherence.
This study has several limitations that should be considered. First, baseline bronchodilator reversibility testing was not performed; however, the study focused on treatment-naive patients to evaluate device-related physiological response rather than acute bronchodilator reversibility. Second, the randomized parallel design without a cross-over phase may limit direct within-subject comparison between DPI and MDI devices; nevertheless, this approach was intentionally chosen to avoid potential carry-over effects and to better reflect real-life initiation of inhaler therapy. Third, only patients with adequate education level and correct inhaler technique were included to minimize technique-related variability and to isolate physiological determinants of response, although this may reduce generalizability to broader real-world populations. Finally, the predominance of male participants and the single-center design with short-term follow-up may limit extrapolation of the findings to more diverse asthma populations.
In conclusion, for asthma patients where inhaler therapy is the primary treatment, inspiratory muscle strength may be a key factor in device selection. DPI devices were associated with greater improvement among patients with higher MIP levels, whereas MDI response appeared more favorable among those with lower MIP levels; however, these observations should be interpreted within the context of the randomized parallel design and do not indicate definitive device superiority. Additionally, HGS, an indicator of peripheral muscle strength, may represent a physiological factor associated with treatment effectiveness for both inhaler types. Higher HGS levels may lead to more precise device grasp and better activation-inhalation coordination in MDI users, as well as deeper and longer inhalations in both MDI and DPI users, thereby supporting successful treatment. These results emphasize the need to consider not just clinical parameters but also inspiratory and peripheral muscle strength when choosing an inhaler device. HGS thresholds vary according to age, sex, and population characteristics; therefore, in the present study, HGS was interpreted as a relative indicator of peripheral muscle performance rather than an absolute marker of abnormality.
Authors’ Contributions
B.K.: Conceptualization, methodology, investigation, formal analysis, writing—original draft, and supervision. A.A.: Data curation, investigation, validation, and writing—review and editing. S.M.Ç.: Resources, data curation, visualization, and writing—review and editing. E.Y.U.: Supervision, methodology, project administration, and writing—review and editing.
Footnotes
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Author Disclosure Statement
The authors declare that they have no conflict of interest to the publication of this article.
Funding Information
No funding was received for this article.