
Abstract
Health systems worldwide are challenged by the need to prioritize and fund rapidly evolving health technologies. The methodology of health technology assessment (HTA) incorporates benefits, costs, and social implications, supporting prioritization of public coverage regarding national health policy. The aim of this study is to identify, analyze, and compare key considerations in the adoption of medical technologies reflecting the national health policies in Israel and England. All Israeli pharmaceuticals approved for public funding during 2020–2022 (287) were analyzed and compared with England recommendations concerned clinical effectiveness, economic considerations, and social values. Both health systems demonstrated 49% agreement regarding approval of funding recommendations policy, while in oncology, diabetes, and hematology, this reached 60%–65%. In both health systems, adoption was determined by clinical impact considering the disease burden and regarding the added value of the innovative technology compared with existing treatments, followed by social considerations. Budget considerations prevail in England. This relatively high resemblance in adoption decisions between England and Israel may emerge from similar principles of accountability for public coverage of medical care. In addition, it may also be driven by the forefront of innovative technological research worldwide and global interest. Nevertheless, economic considerations differ between the 2 health systems, introducing policy discrepancies or tactical diversity.
Keywords
Health technologies evolve rapidly worldwide, constantly challenging governments to try to balance the provision of innovative treatments within limited resources. 1 The need to prioritize beneficial costly technologies 2 incorporating clinical, ethical, and cost-effectiveness considerations is an ever-growing difficulty.1,2 Health technology assessment (HTA) is a widely accepted methodological approach for decision making,1,3–5 integrating evidence-based information regarding safety, effectiveness, and cumulative health benefits.1,6,7 Although HTA methodology is based on universal principles, responding to similar global trends,6,8 indisputable differences among health systems exist. Health systems are designed to meet specific needs and local circumstances, dictated by national strategies and policy guidelines. Beyond clinical principles and economic considerations, ethical and moral philosophies play a role in each health system, as societal values and beliefs are culture-dependent and a unique social perception influences judgments during deliberations.1,7,9 Notwithstanding, mutual assessment and cooperation among health assessors may promote wise recommendations, and sharing of insights and broadly applicable solutions.
Naturally, the assessment initiates by examining technological parameters, including safety, efficacy, and effectiveness. 10 The epidemiological perspective must be taken into consideration: to meet the need and address the patients according to the level of disease severity. Occasionally, only partial reimbursement is considered, targeting a specific subgroup that will benefit the most from the technology, to enable access to affordable care to a larger number of individuals. 11 Shortage of resources may be emphasized under specific circumstances such as a pandemic, war, or unexpected shifting of national priorities.
A survey of the research literature indeed shows that, despite local consideration, comparisons of technology assessments to obtain methodological milestones have been made. In a review of 11 countries, including Oregon and New York (United States), 3 categorized parameters comprising 3 main axes were used: the clinical perspective, the practical operational implication, and the socioethical viewpoint. The first axis is a bundle of clinical benefits that meet the level of impaired health (need).2,12 Several health systems describe outcomes in terms of improved health impact: lifesaving, life extension, and improving quality of life (Sweden, Norway, Australia, the United States [Oregon], and Israel). Others focus on the added clinical advantages compared with the current treatment (Canada, Norway, Israel, and the United States [Oregon and New York]). 2 The length of illness may also play a role in assessing benefit by cost (Norway, Sweden, and the United States [Oregon]). Amplifying benefit from a specific technology, when lacking existing available and suitable therapeutic alternatives, emphasizes its prioritization (Canada, France, New Zealand, and Israel).2,12 Several assessors consider appropriateness and adherence to guidelines as leading parameters in the decision (the United States [Oregon] 2 and the European Union [EU] 12 ). Some refer to a combination of effectiveness and safety (England and France), patient preferences, 13 and social values, 14 representing patient-centeredness as a core principle guiding health policy.
The second axis reflects the economic burden, considering efficiency and cost-effectiveness, cost–benefit, and related economic impacts.2,10,15 From the system/organizational viewpoint, implementation of new technologies requires operational feasibility and budget allocation. The patient perspective, however, is applied to evaluation of the willingness of users to pay for a technology based on the perceived need in the absence of public allocation.16,17
The third axis reflects the cultural perception–social values, the ethical perspective, and national morality principles such as equality and solidarity, 2 accessibility to health services, 10 and the affordability vis-à-vis the individual patient (Israel, New Zealand, and the Netherlands). 2 As expected, these axes vary across different societies and health care systems.
The integration of all aspects is crucial to create a comprehensive policy. Technology assessors initially insist on relying on evidence-based reports in scholarly literature (proof of medicine). 15 Nevertheless, the prompt changes in clinical practice, initiated by accelerated technology development, force technology assessors to rely on reports from users, either clinicians or the industry, termed real-world evidence (RWE).18–20
Still, sometimes the enthusiasm to adopt innovation meets uncertainty and lack of or only minor evidence. Decision-makers often postpone decisions until enough evidence is available.20,21 Mechanisms such as conditional coverage are offered to provide temporary funding that can fill the gap period until essential data are accumulated to support/invalidate the implementation decision. The mechanism of coverage with evidence development (CED) enables public provision of a new technology while ongoing reassessment provides sufficient evidence to maintain further utilization.11,21,22 To enhance proper decisions balancing costs and benefits, the National Institute for Health and Care Excellence (NICE) in England uses the incremental cost–utility ratio, based on additional spending for additional benefit expressed by the number of quality-adjusted life years gained (QALYs).15,23
In the Israeli health system, the decision whether to adopt and publicly fund a new technology is conducted by the “Public Committee for the Expansion of the Health Services Basket” determined by and following the principles of the National Health Insurance Law: equity, solidarity, and justice distribution.24–26 These publicly funded technologies are detailed in a “positive list” supplementary to the law,27,28 expanded each year secondary to the allocated budget, following the deliberations and recommendations of the Public Committee.27,29 More than 500 proposed technologies are evaluated annually in this unique process, which requires balancing the interests and incentives of many stakeholders. Clinical, epidemiological, economic, and social aspects are integrated to achieve a consensus vis-à-vis a prioritized list of technologies.24,26,30,31
Unlike Israel, using an internal governmental team, in England, technology assessment is conducted by NICE, which also delivers clinical guidelines32,33 based on information provided by commercial entities.18,22 An independent committee including health professionals, economists, statisticians, and experts 33 provides recommendations for delivering optimal care within the National Health Services’ (NHS) budget.32,33
Given policy-oriented budget allocation and cross-country differences, and although hesitance toward similar adoption of health technologies may exist, technology assessors worldwide are motivated to embrace considerations that propelled their peers. An analysis of 199 drugs conducted in 10 European countries shows a correlation between the HTA outcomes for acceptance and reimbursement/rejection and a previous NICE recommendation. A 5-country comparative analysis covering England, Scotland, Sweden, Canada, and Australia regarding 287 cancer, orphan, and neurological drug indications (2007–2009) revealed a 54.0% similarity in using clinical and/or cost-effectiveness considerations by at least 2 agencies. 34 An HTA comparative assessment based on Italian requests and focusing on added therapeutic value (2017–2022), comparing recommendations in Italy, France, and Germany, regarding 189 innovative orphan, oncology, and autoimmune drug indications, showed 82% agreement between Germany and France, but only 52% agreement between Italy and France, and 57% agreement between Italy and Germany. 35
The aim of this study was to evaluate the similarity and discrepancies of the Israeli leading principles and considerations compared with England, toward their decisions to approve public funding of new technologies.
Our research focused only on budget-approved technologies, as these decisions reflect the accountability to and solidarity with patients in need. A supplementary examination would have included technologies that were underprioritized and rejected; however, our goal was to get insight into the prioritization mechanism and underlying strategy, and avoid bias toward decisions related to scarce resources per se.
Methods
All 287 health technologies and their indications that were approved for public funding in Israel between 2020 and 2022 were analyzed according to the main considerations of adoption used by the Public Committee, listed by the technology’s generic name, indication, and clinical field. We compared the listed technologies to the same technology recommendations published by NICE until February 2022. The research focused on medications only.
In Israel, the entire assessment is based on the internal governmental team members who are well-aware of policy principles as well as the existing list of technologies available to the public. Moreover, the assessors personally participate in the experts’ discussion, provide information, and specify dilemmas in allocation. 31 This allows a more flexible insight into prioritizations and balancing needs and opportunities to clinical subgroups and socioeconomic gaps. In England, a different perspective is taken: first, the consultants are external experts, conscious of clinical guidelines and the medical environment, not necessarily related to policy, while comprehensive policy considerations and adoptions are engaged in the final steps of the decision. Moreover, the economic framework in England limits the number of technologies that can be added to the list of funding; therefore, economic considerations are significant determinants in the decision-making mechanism.32,33
The indications/recommendations were analyzed, categorized, and coded according to clinical, technological, social, and economic considerations as follows:
Clinical considerations refer to disease severity, considering specific targeted and personalized medicine (including genetic detection). 19
Technological considerations refer to perceived added value recognition compared with the current/existing technology being used, lack of available alternatives, and sustainability of guidelines for care delivery, lack of clinical alternatives, 36 and declaration of innovation per se, meaning, particularly, the familiarity versus hesitation toward utilization (adherence), based on experts’ opinions.
Social considerations refer to specific vulnerable populations, such as explicit age groups (children or the elderly), and considering patient preferences as mentioned in the decision-making process. 8
Economic considerations include using risk sharing mechanisms, such as conditional coverage or CED,11,21 cost-effectiveness analysis to assess feasibility, 2 and value for money/worthwhileness. 16
Statistics
A Z-test for the difference in population proportions was conducted. The test examined the percentage of use of considerations for public funding of medical technologies in Israel and England, with a significance level of α = 0.05. The null hypothesis was that there is no difference between the 2 population proportions, H0: p1 = p2; the alternative hypothesis was that there is a difference, p1 ≠ p2.
Results
Our findings reveal that during a 3-year period, 148 technologies were documented in the NICE database compared with 287 technologies accepted in Israel. The analysis shows a 52% resemblance in decisions regarding discussed similar indications and 49% consent to reimburse (8 pharmaceuticals out of 148 discussed by NICE rejected, mainly due to cost–benefit considerations). Among the remaining 139 technologies (48%), 91 technologies (66%) were not discussed in England, 35 technologies (25%) were approved with different indications, and 13 technologies (9%) had combined, yet unsimilar, indications. These technologies (139) were excluded from our consideration analysis.
Considerations analysis
As shown in Table 1, in Israel, the gained clinical benefit was the leading element in approving public funding (up to 78%), followed by technological considerations (up to 55%). Social determinants are less influential (up to 7%), and economic aspects were not mentioned at all in the Israeli deliberations. Among the clinical considerations, disease severity was the significant justification (78%), followed by personalized medicine (31%). Among the technological considerations, perceived added value compared with the current treatment had the most impact (55%), and lack of alternatives was mentioned in 9% of the considerations. Declaration of innovation per se was mentioned in 37% of the technologies discussed. Social considerations included indication for adults (6%), children (7%), and the elderly and/or postmenopausal women (1%).
Distribution of Mechanisms and Considerations Used for Adopting Technologies and Indications, Comparing Israel and England
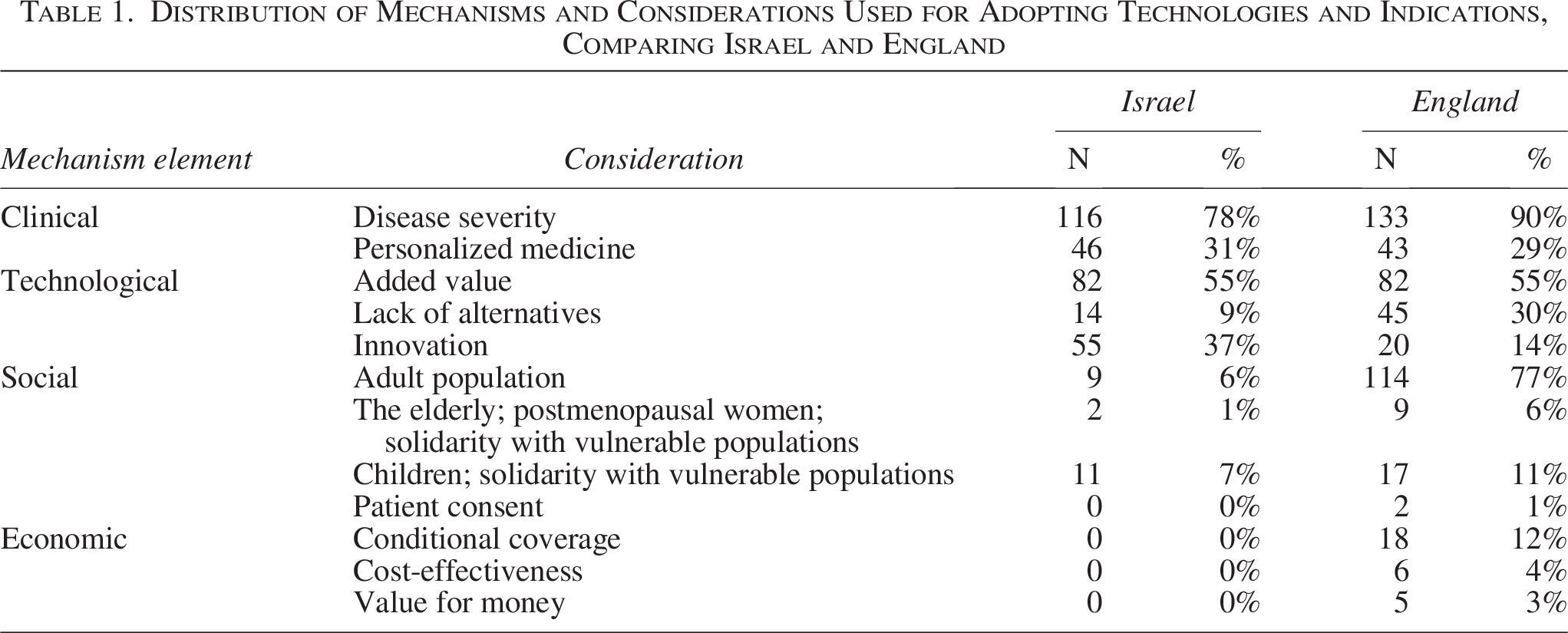
In England, the clinical aspect, especially disease severity, was the main factor in most decisions (90%). Personalized medicine was mentioned in 29% of the technologies. The most prominent technological consideration was added value (55%), followed by lack of alternatives (30%), and innovation (14%).
Among the social considerations, 77% were related to specific adult populations, 11% related to children, and 6% to the elderly and/or postmenopausal women. 1% of the social considerations concerned the need to get patient consent.
Economic considerations focused on the mechanism of conditional coverage (12%) in particular, followed by cost-effectiveness (4%) and calculating value for money (3%).
When comparing the 2 health systems, as expected, the clinical argument was dominant both in Israel and England (78% and 90%, respectively), as was added value (55% in both countries). Personalized medicine as a marker of additional benefit and innovation was mentioned in 31% of the technologies in Israel compared with 29% in England. Innovation per se was mentioned in 37% of the technologies in Israel compared with 14% in England.
The statistical analysis revealed significant differences between the 2 health systems regarding social parameters. Considerations such as specific attention to adults and the elderly, alongside a lack of alternatives and, in particular, severe morbidity, were more prominent in England. While in England, these social elements are enhanced, in Israel, innovation plays a major role. Equality between the 2 countries regarding personalized medicine, added value, and children’s solidarity consideration cannot be rejected. Other issues, such as patient consent and economic considerations, did not yield enough evidence to perform and observe statistical results.
Analysis of specific clinical fields
Out of 287 pharmaceuticals approved for public funding in Israel and the 140 approved in England, 216 (75%) and 114 (81%), respectively, were classified within 6 major clinical fields: oncology (27%, 34%), hemato-oncology (10%, 11%), neurology (16%, 14%), pulmonary (8%, 5%), and diabetes and hematology (7%, 9%) (see Table 2).
Distribution of Technologies Prioritized for Public Funding in Israel and England by Clinical Field

All the clinical fields are listed in Appendix 1.
The distribution of indications among all clinical fields is presented in Appendix 1.
Discussion
Distribution of topic prioritized clinical fields
A comparison of funding recommendations per clinical field revealed that during the 3 years of the study period, among the 287 technologies that were recommended for public funding in Israel, 75% were classified into the 6 aforementioned leading clinical fields (oncology, hemato-oncology, neurology, and, to a lesser degree, diabetes, hematology, and pulmonology), while in England their relative share reached 81%.
A one-by-one analysis revealed a 49% consent to public funding. In oncology, diabetes and hematology, however, consent exceeded 60%–65%. Most likely, this similarity emerges from shared interests within the scientific and academic community, coupled with industry investments in these areas.37,38 Unsurprisingly, a substantial share (58%) of the recommendations for public funding was allocated to cancer-related conditions (oncology and hemato-oncology) in both countries, being a substantial health threat worldwide. 39 We found that 4 out of 8 drugs rejected by NICE were cancer drugs. For 2 of them, it is noted that the reasons are related to the funding threshold set by the Health Ministry. There is a prevailing interpretation, although it is controversial, that restricted access to cancer drugs has been an important contributor to relatively poor survival. In 2010, England’s Minister of Health pledged to create a Cancer Drugs Fund specifically intended to provide access to cancer treatment drugs not yet appraised or found to be not cost-effective. 40 A generous budget was also allocated to neurological therapeutics, which presumably grapples with the increase in threat of stroke and rising neurodegenerative morbidity. 41 Diabetes, defined as an emerging “pandemic,” 42 is also of interest in Israel and England, with a relatively considerable allocation of funding.
The noticeable agreement for funding in leading clinical fields may be driven by the enthusiasm of clinicians as well as providers, insurers, technology assessors, and even patients. Low agreement for funding pulmonary technologies (29%) could be explained by the data showing higher levels of air pollution and related deaths in Israel compared with England (267.6 and 214 deaths per million residents, respectively). 43
Considerations Contributing to Prioritization of Publicly Funded Medical Technologies
Beyond clinical incentives, motivated by the impact of patient morbidity and the burden on society,2,12 the perceived added value has a large impact on more than half of the approvals in both health systems. Innovation implementation, perceived as an additional opportunity to improve health outcomes, is more dominant in Israel compared with England, second to a national strategy to encourage scientific curiosity.
Social Considerations
Both England and Israel share principles of governmental accountability for citizens’ health, distributive justice and equity, as well as solidarity and protection of the vulnerable.24–28,44,45 Historically, the principle of social welfare introduced in Beveridge’s 1942 report inspired the NHS with the vision to provide free, adequate, and equally accessible health care for all. 44 Nonetheless, in England, 93% of the considerations referred to a specific, targeted population—77% allocated to adults, 11% to children, and 6% to the elderly, compared with 6%, 7%, and 1%, respectively, in Israel. The absence of an explicit justification by the Israeli decision mechanism can be explained by the conceptual understanding that each Israeli resident is entitled to free health services by law24–28 as well as a national commitment to provide clinical treatment to all who meet the indications.25,27–28 This correlates with the fact that economic mechanisms were mentioned in England’s deliberations only. Another explanation could derive from the ethical conceptual distribution approach (equity compared with justice). Whereas English policymakers favor supporting specific vulnerable populations, Israel takes the approach of equal allocation to every individual. 2
Moreover, when cost-effectiveness analysis is uncertain, NICE may reduce risk by restricting recommendations only to certain patient subgroups until sufficient evidence regarding clinical benefit (including experts’ opinions) is accumulated. 45 Thus, “real-world evidence” may guide recommendations at an earlier stage.18–20
Clinical Considerations
A patient-centeredness strategy may correlate with specific innovative pharmaceutical mechanisms, such as cellular markers and personalized medicine, aimed to increase effectiveness by providing tailor-made medications to the individual patient, based on their genetic fingerprint. This unique setting incorporates medical need with individual characteristics that forecast the level of response to treatment. In a broader perspective, balancing the opportunity to access targeted care prioritized by maximizing benefit not only to the single patient but to the entire population in need, within the limitation of budget allocation. 46 A better understanding and utilization of genetics and epigenetics in human disease is expected to dramatically lower costs and lead to widespread implementation of personalized clinical diagnoses and treatments. 19
Technological Considerations
The combination of parameters and cumulative information regarding the weight of the estimated added value enables policymakers and decision-makers to identify beneficial technologies and allocate public funding. This methodology is widely used in England, Israel, the Netherlands, Canada, 11 and some EU countries. 36 Although the main intention is to reduce expenditure, quality of care may also be increased by detecting overuse and unnecessary use. Screening of medications in European countries revealed an evolving trend: restrictions in technology implementation by using more rigorous indications and conditions for prescriptions,11,47 encouraging generic prescriptions, monitoring doctors’ prescribing patterns, and constraining budget allocation. 11 We assume innovation per se plays a role as an incentive in the Israeli medical community. Israel is ranked sixth among OECD countries for the number of patents per capita and among the top 5 in the number of publications in journals ranked in the first quarter, per capita. 48 It may be that researchers’ and clinicians’ eagerness to adopt innovations is sometimes subordinate to the latter’s promising potential as an opportunity to increase health.
A strong justification for allocating public funding in England was the lack of alternatives, reflecting governmental accountability to provide care to all unmet need. Specifically, in England, age-related indications are widely used, in particular as regards the older age group. This tendency may stem from the higher proportion of the elderly in England compared with Israel (19% and 12%, respectively). 49 A significant difference regarding technological considerations was found in the statistical test, supporting our finding. We expect similar justification will be used in Israel in the future, as the elderly population is a growing burden worldwide, demanding excessive technology utilization and financial outlays 50 alongside the inability, unaffordability, or unwillingness to pay.
Cross-country comparisons
A review of the literature reveals that in most cross-country comparisons, similarity in policy regarding the reimbursement of drugs reaches 50%–82%.34–35 This may be explained by 2 reasons: the first is similar interest among the clinical academic community worldwide, showing predisposition to adopt innovations in similar morbidities.37–39 Second, smaller HTA agencies tend to rely on assessments conducted by their colleagues from stronger agencies. Notably, the leading forces are NICE England and IQWiG Germany (Germany—Institute for Quality and Efficiency in Health Care). An example of this dependency is presented in a 10-country study comparing drug reimbursement in Belgium, France, Poland, Portugal, Sweden, the Netherlands, Scotland, England, Germany, and Spain, all of which rely on NICE recommendations and adopt complex economic evaluations to comply with comprehensive assessments. 9
Focusing on the leading clinical fields, oncological drugs are of the highest interest. This may seed due to the significant clinical challenge, rapid development, highly dynamic nature of the biological innovative drugs, alongside their huge benefit contributing to prolongation of lives. Additionally, their substantial cost increasing treatment burden on both patients and health care systems.37–39 Similarly, orphan drugs are associated with extremely high costs essentially, high expenditures for few beneficiaries, presenting a socioethical dilemma in budget allocation to policy makers, beyond effectiveness considerations to clinicians.51,52
Given these complexities, extensive collaboration and mutual learning may provide valuable insights and support more informed, evidence-based decision making.
Conclusions
In the era of growing health opportunities and budget shortages, HTA is an essential tool for making wise decisions and prioritization policies while balancing multiple stakeholders (providers, insurers, payees, and patients). Notably, economic considerations dominant; nevertheless, governments’ worldwide face the challenge of embracing social values alongside offering value for money. Unexpected global events such as the COVID-19 pandemic can interfere with strategic outlines, requiring swift adoption of unique solutions, prioritized by each country. HTA has emerged as a global methodology, offering mutual learning and fostering cooperation among countries.
Similarity among national health systems, however, is only partial and should be addressed carefully. Recent publications have introduced the importance of international comparison. In our research, an almost 50% consent similarity regarding funding decisions was found, with prominent resemblance of certain medical fields that probably derives from global interests, similar technological progress, and regulatory status. This similarity has inspired a multinational model that has been evolving for about 20 years.15,53 Nevertheless, national differences may cause hesitance: the Israeli mechanism of technology adoption is based on a “positive” list of health services and lack of a delisting/disinvestment process. 54 In England, the health budget is allocated per technology per patient55–56 and may be changed annually,23,55 emphasizing economic considerations.
Since prioritization and adoption of innovative technologies decisions reflect health national strategy, it is unavoidable to ignore local guiding principles and adhere to traditional HTA mechanisms. Technology assessors and policy makers, however, are tempted to seek for unique mechanisms to cope with medical opportunities facing scare resources. For decades, mutual shared knowledge in HTA prevailed, yet recently published articles point to the need to compare considerations of funding, priority setting, and targeted solutions, particularly in the era of global transparency.
Study Limitations
The study initiated from the Israeli approved list of medical technologies and was then compared with the NICE database for the same technologies. The study focused on a 3-year period. Enlarging the time frame should provide a clearer picture of developing trends. Explicit consideration based on strategy (and legal) principles was used to analyze the results; however, distinctive policy outlines were not found in Israel and in the England’s NICE database. In our study, we focused on the top prioritized publicly funded technologies, aiming to reveal the values that shape national strategy. A complementary study of the less favored technologies could broaden our understanding. The details of the considerations under discussion, nevertheless, were not always publicly accessible and sometimes were found to have emerged from the economic restrictions rather than from socioclinical philosophy.
Study Importance
The challenges of adopting innovative health technologies are increasing as a result of the rapid development of costly technologies, the growing number of opportunities for different target populations (expanding indications), multiple actors, and the widening number and complexity of considerations. These include medical ethics, patient autonomy and engagement, family involvement, the potential of new inventions, budget limitations and decisions of fair distribution allocation, changes in politics and governments, and uncertainty regarding unexpected threats that require immediate funding (eg, COVID-19 pandemic, natural disasters, armed conflicts). Moreover, the dynamic medical environment, alongside the growing complexity of and new assessment methods, introduces a wide range of methodologies offered by discussion group, panels, consensus conferences, patient parliaments, and artificial intelligence. The limited number of technology assessors confronted with the need to make swift decisions is challenged on all fronts. As such, peer learning could be beneficial; but one must consider both the potential similarities in methodologies alongside differences in values and policies. Mutual or comparative assessment may provide insight regarding arguments leading to decision-making closing gaps in cases of scarce evidence, insufficient data, or while policy is still vague.
Future Research
Exploring and examining technologies rejected by both health systems, whether due to clinical considerations, social factors, budget constraints, or a combination of these, can expand the understanding of the degree of agreement on public health funding between 2 countries. Analyzing a country’s deliberations can provide valuable insights into how health policy is determined in the light of equity and solidarity. In addition, comparing considerations between other countries would elucidate and deepen our understanding of HTA methodology.
Authors’ Contributions
Dr. Tal: Conceptualization, methodology, supervision, and writing—review and editing. Ms. Finkelshtein-Zloof: Data curation, investigation, formal analysis, and writing—original draft preparation.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Data Availability Statement
The supporting data are publicly available in additional supporting Excel file. The file contains the data for each drug (287) that were collected, edited, and analyzed from the websites of NICE England and the Ministry of Health in Israel.
Supplemental Material
Appendix
Distribution of Technologies Prioritized for Public Funding by Clinical Field

| Israel | England | Comparison between the 2 countries | |||
|---|---|---|---|---|---|
| Clinical field | N | % | N | % | % of agreement for public funding between 2 countries |
| Oncology | 78 | 27% | 47 | 34% | 60% |
| Hemato-oncology | 28 | 10% | 15 | 11% | 54% |
| Neurology | 46 | 16% | 19 | 14% | 41% |
| Pulmonary | 24 | 8% | 7 | 5% | 29% |
| Diabetes | 20 | 7% | 13 | 9% | 65% |
| Hematology | 20 | 7% | 13 | 9% | 65% |
| Rheumatology | 9 | 3% | 3 | 2% | 33% |
| Dermatology | 9 | 3% | 3 | 2% | 33% |
| Infectious diseases | 9 | 3% | 2 | 1% | 22% |
| Cardiology | 7 | 2% | 6 | 4% | 86% |
| Mental health | 7 | 2% | 1 | 1% | 14% |
| Ophthalmology | 6 | 2% | 3 | 2% | 50% |
| Gastroenterology | 6 | 2% | 2 | 1.5% | 33% |
| Allergies and clinical immunology | 4 | 1% | 2 | 1.5% | 50% |
| Endocrinology | 4 | 1.5% | 1 | 1% | 25% |
| Metabolic diseases | 3 | 1% | 0 | 0% | 0% |
| Osteoporosis | 2 | 1% | 1 | 1% | 50% |
| Gynecology | 2 | 1% | 0 | 0% | 0% |
| Nephrology | 2 | 1% | 1 | 1% | 50% |
| Urology | 1 | 0.3% | 1 | 0.7% | 100% |
| Total technologies | 287 | 100% | 140 | 48% | |
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.