
Abstract
Terminal patients and their families face severe psychological distress—including anxiety, depression, caregiving stress, and grief—that exceeds the capacity of routine hospice care. While narrative nursing and psychological resilience training have shown individual efficacy, the synergistic effects of their combination remain unexamined. This study aimed to unravel the effects of narrative nursing combined with psychological resilience training in enhancing the psychological adaptation of patients and their families in hospice care. Seventy-four patients and their families receiving hospice care were allocated into an observation group (received an 8-week intervention of narrative nursing combined with psychological resilience training on top of routine hospice care) and a control group (received routine hospice care). Hospital Anxiety and Depression Scale (HADS) scores and Connor-Davidson Resilience Scale-10 (CD-RISC-10) scores of patients and their families before and after nursing were compared between the 2 groups. Psychological Distress Thermometer (PDT) and Pittsburgh Sleep Quality Index (PSQI) scores of patients before and after nursing were also compared. The modified hospice care satisfaction scale (based on the FAMCARE-2 scale) was applied to compare the nursing satisfaction of patients and their families after nursing. After nursing, the observation group demonstrated significantly greater reductions in HADS-A and HADS-D scores, more pronounced improvements in CD-RISC-10, PDT, and PSQI scores, as well as higher nursing satisfaction scores compared to the control group (all P < 0.05). The integration of narrative nursing with psychological resilience training in hospice care enhances the psychological adaptability of both patients and their families, while also contributing to improved sleep quality and greater satisfaction with care delivery.
Keywords
Terminal cancer represents an advanced stage where curative treatment is no longer viable, making a dignified end-of-life experience the primary goal. Hospice care plays a crucial role by offering individualized support based on disease severity, promoting the concept of a “good death.” This approach not only improves patient quality of life but also advances patient-centered medical practice. 1 Hospice care constitutes a specialized component of palliative care designed for individuals with a terminal prognosis, generally defined as a life expectancy of 6 months or fewer. Unlike general palliative care, hospice care emphasizes symptom relief and psychosocial support for patients and families, foregoing interventions aimed at curing the underlying condition. 2 As a multidimensional care model, hospice care aims to fulfill the biopsychosocial and spiritual needs of patients with life-limiting illnesses and their relatives. 3 Family caregivers with limited training or readiness are routinely required to observe and address these acute symptom exacerbations. This responsibility may exacerbate caregiver distress and perceived burden. 4
Narrative nursing is a patient-centered approach with the core objective of improving emotional distress and psychological isolation caused by patients’ inability to effectively express and integrate their inner pain and concerns by guiding them to narrate and reconstruct their disease experiences.5–10 Health care professionals with narrative competence actively listen to and interpret patients’ disease stories, aiding them in clearly expressing their emotions and traumatic experiences. 8 This process not only helps patients express their emotions, alleviate inner pain, and cultivate positive emotions 10 but also promotes the reconstruction of meaning in their life and disease experiences.6,7 Based on this in-depth understanding, nurses can identify key needs and implement tailored psychological interventions, thereby enhancing the specificity and clinical efficacy of nursing care. 9
The cultivation of psychological resilience aims to address issues of psychological maladjustment and health depletion that individuals (such as family caregivers) may face when confronted with persistent stress and adversity. It is a dynamic capability that enables individuals to effectively adapt to and recover from challenging life circumstances, thereby maintaining mental health amidst difficulties. Among family caregivers, high resilience has been demonstrated to enhance psychological adaptation levels, reduce perceived caregiving burden, and thus improve their overall quality of life.11,12 This capability is shaped by both intrinsic traits and external support, with social support from health care professionals, family, and social networks playing a crucial role in enhancing resilience, 13 and collectively promoting positive health outcomes. 14
However, there is a lack of empirical research exploring whether the combined application of narrative nursing and psychological resilience training can produce synergistic effects. Given this, the present study aims to investigate the effects of narrative nursing combined with psychological resilience training in hospice patients and their families.
Materials and Methods
Ethics statement
The research was approved by the Ethics Committee of Jinzhou Medical University. The participants involved in the study signed the written informed consent forms.
Subjects
This study enrolled 74 patients and their families treated with hospice care in Jinzhou Medical University from January 2022 to October 2024 (with each patient corresponding to 1 family member, totaling 74 pairs). Patients met the following inclusion criteria: (1) clinically diagnosed with a terminal illness and eligible for hospice care; (2) age ≥18 years; (3) conscious and able to communicate effectively; (4) willing to participate in the study and signed an informed consent form; (5) no history of severe cognitive impairment or mental illness. Inclusion criteria for family members were (1) primary caregiver of the patient with a close relationship (such as spouse, children, parents, etc.); (2) age ≥18 years; (3) accompanied the patient for ≥3 days per week; (4) willing to participate in the study and signed an informed consent form; (5) no history of severe cognitive impairment or mental illness.
Exclusion criteria for patients included (1) severe cognitive impairment or mental illness, unable to cooperate with the study; (2) critically ill with an expected survival of less than 1 month; (3) refusal to participate in the study or withdrawal midway. Exclusion criteria for family members were (1) severe cognitive impairment or mental illness, unable to cooperate with the study; (2) non-primary caregiver or estranged from the patient; (3) refusal to participate in the study or withdrawal midway.
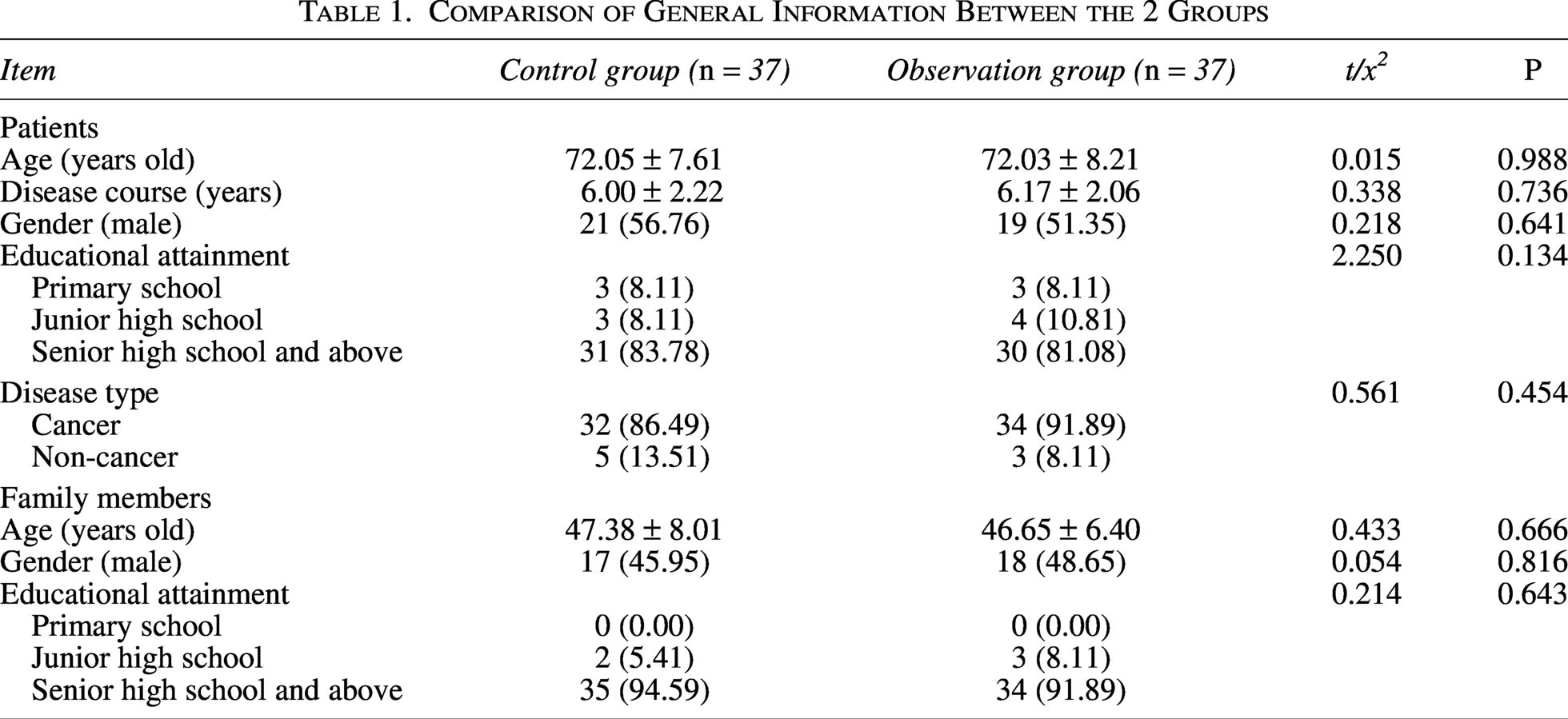
The 74 patients and their families were randomly classified into the observation group and the control group, with 37 pairs in each group. There were no statistical differences in general information such as age, gender, education level, disease type, and duration of illness between the 2 groups of patients and their families (P > 0.05), making them comparable (Table 1).
Comparison of General Information Between the 2 Groups
Methods
Patients and their families in the control group were treated with routine hospice care, including pain management, symptom control, psychological support, and basic nursing. Pain management was conducted through a combination of medications (such as opioids, nonsteroidal anti-inflammatory drugs, etc.) and non-pharmacological methods (such as physical therapy, relaxation training, etc.) based on the patient’s pain level. Symptom control involved adopting corresponding medical and nursing measures for specific symptoms of patients (such as dyspnea, nausea, vomiting, etc.) to alleviate discomfort. Psychological support meant that emotional support was provided to patients and their families through means such as listening, empathy, and comfort to help them cope with the psychological pressure brought by the illness. Basic nursing consisted of daily life nursing, nutritional support, and skin care to ensure that patients’ physiological needs were met.
In addition to routine hospice care, the observation group was exposed to narrative nursing combined with psychological resilience training intervention, specifically encompassing the following: (1) Training: To ensure the quality of the study, all nursing staff participating in the study received professional training in narrative nursing and psychological resilience training before the intervention to ensure they mastered relevant skills. After each nursing session, nursing staff needed to record in detail the nursing content, reactions of patients and their families, and nursing effects for subsequent analysis and adjustment. During the nursing process, the psychological status of patients and their families was regularly assessed, and the nursing plan was adjusted in a timely manner to ensure nursing effectiveness; (2) Narrative nursing intervention: By guiding patients and their families to tell their personal life stories, it helped them reexamine the meaning of life and enhance psychological adaptation ability. Specific steps comprised: ① Storytelling: Nursing staff guided patients and their families to narrate their disease experiences, family life, and important life events, and helped them sort out the storyline through listening and questioning; ② Reconstruction of the meaning of life: Nursing staff discussed the meaning and value of life with patients and their families based on their storytelling, helping them reexamine the impact of the illness on their lives and enhance their understanding and acceptance of life; ③ Emotional expression and release: Narrative nursing encouraged patients and their families to express their inner emotions (such as fear, sadness, anger, etc.) and facilitated emotional release under the guidance of nursing staff to relieve psychological pressure; (3) Psychological resilience training: Psychological resilience training intervention improved the psychological resilience levels of patients and their families through psychological education, cognitive-behavioral intervention, and emotion regulation training. Specific content covered: ① Psychological education: The concept and importance of psychological resilience were popularized to patients and their families, helping them understand the role of psychological resilience in coping with illness and stress; ② Cognitive-behavioral intervention: Cognitive restructuring techniques were utilized to help patients and their families identify and correct negative thinking patterns and establish a positive cognitive framework. For example, they were guided to focus on the positive aspects of the illness and cultivate an optimistic attitude; ③ Emotion regulation training: Patients and their families were taught emotion regulation techniques, such as deep breathing, mindfulness meditation, relaxation training, etc., to help them better manage negative emotions; ④ Strengthening social support: Patients and their families were encouraged to actively seek and utilize social support resources (such as relatives, friends, support groups, etc.) to enhance their ability to cope with difficulties; ⑤ Goal setting and achievement: Patients and their families were assisted to set short-term and long-term goals and formulate specific action plans to enhance their sense of control and accomplishment in life.
Both groups received nursing for 8 weeks, with 1 to 2 sessions per week, each lasting 30–60 minutes. The nursing form involved a combination of individualized intervention and group intervention. Individualized nursing provided personalized guidance based on the specific needs of patients and their families. Group nursing promoted mutual communication and support among patients and their families by organizing group activities. The nursing team consisted of professionally trained hospice care nurses, psychological counselors, and social workers to ensure the scientific and effective nature of nursing care.
Observation indicators
Anxiety and depression: Before and after nursing care, the Hospital Anxiety and Depression Scale (HADS)
15
was applied to evaluate patients and their family members. The scale comprised 14 items, divided into the HADS-A and HADS-D, each containing 7 items. Each item was scored using a Likert 4-point scale (0–3 points), with subscale total scores ranging from 0 to 21 points. Scoring criteria were as follows: A total score ≥8 indicated the presence of anxiety or depressive symptoms, with 8–10 points classified as mild, 11–14 points as moderate, and ≥15 points as severe. Psychological resilience level: Before and after nursing care, the Connor-Davidson Resilience Scale-10 (CD-RISC-10)
16
was employed to evaluate patients and their family members. The CD-RISC-25 scale consisted of 25 items, divided into 3 dimensions: tenacity (13 items), strength (8 items), and optimism (4 items). Each item was scored using a Likert 5-point scale (0–4 points), with total scores ranging from 0 to 100 points. Higher scores indicated greater psychological resilience. Psychological distress assessment: Before and after nursing care, the Psychological Distress Thermometer (PDT)
17
was adopted to assess patients. The scale employed a single visual analog scale (0–10 points), with 0 indicating “no distress” and 10 indicating “extreme distress.” A score ≥4 means the need for professional care. Sleep quality: Before and after nursing care, the Pittsburgh Sleep Quality Index (PSQI)
18
was performed to evaluate patients. Higher scores showed poorer sleep quality. The scale contained 18 items, divided into 7 dimensions: subjective sleep quality, sleep latency, sleep duration, sleep efficiency, sleep disturbances, use of sleeping medications, and daytime dysfunction. Each dimension was scored from 0 to 3 points, with total scores ranging from 0 to 21 points. Scoring criteria were as follows: A total score > 7 implied the presence of sleep disorders. Nursing satisfaction: Before and after nursing care, a modified palliative care satisfaction scale, adapted from the Assessment Measure for Caregivers of Advanced-stage cancer patients-version 2 (FAMCARE-2),
19
was conducted to assess patient and family member satisfaction with nursing services. The scale involved 10 items, covering dimensions such as symptom control, communication quality, psychological support, information provision, and overall experience. Each item was scored using a Likert 5-point scale (1–5 points), with total scores ranging from 10 to 50 points. A score ≥40 suggested “satisfaction.”
Statistical methods
Data analysis was performed using SPSS 26.0 software. Measurement data were expressed as mean ± standard deviation, with paired t-tests applied for within-group comparisons and independent sample t-tests for between-group comparisons. Categorical data were depicted as frequencies and percentages, with χ2 tests employed for between-group comparisons. A P value < 0.05 was considered statistically significant.
Results
Anxiety and depression
Before nursing care, there were no remarkable differences in HADS-A and HADS-D scores between the 2 groups (P > 0.05). After nursing care, anxiety and depression scores decreased in both groups (P < 0.05), with greater reductions observed in the observation group (P < 0.05) (Tables 2 and 3).
Comparison of HADS-A Scores of Patients and Their Family Members Between the 2 Groups (

Compared with before nursing, *P < 0.05.
Comparison of HADS-D Scores of Patients and Their Family Members Between the 2 Groups (
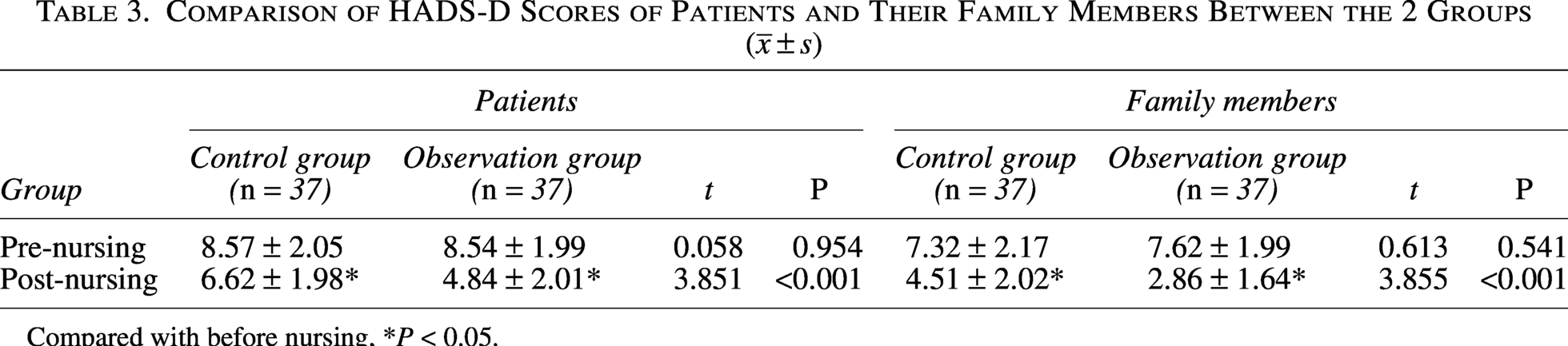
Compared with before nursing, *P < 0.05.
Psychological resilience level
Before nursing care, there were no marked differences in CD-RISC-10 scores between the 2 groups (P > 0.05). After nursing care, CD-RISC-10 scores remarkably increased in both groups (P < 0.05), with greater increases observed in the observation group (P < 0.05) (Table 4).
Comparison of Psychological Resilience Scores of Patients and Their Family Members Between the 2 Groups (
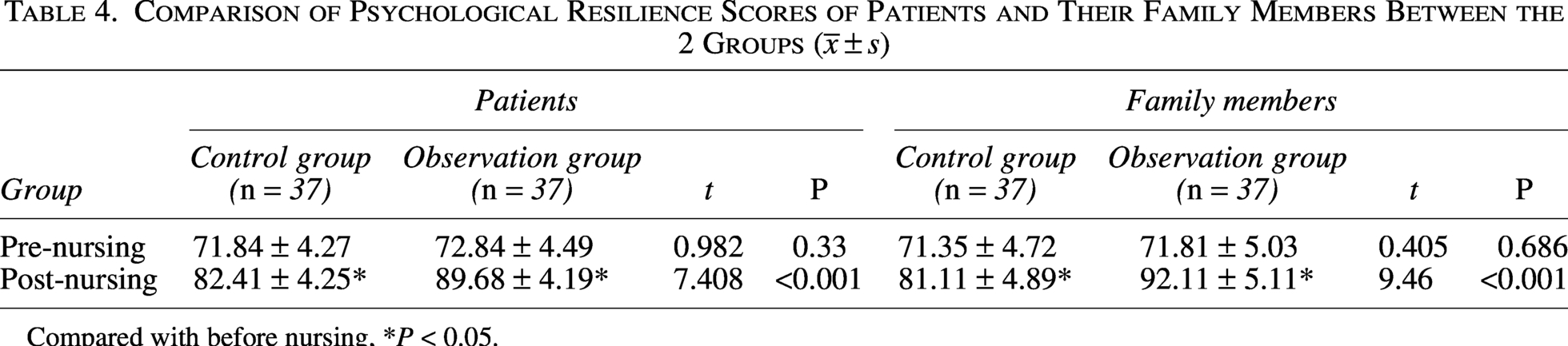
Compared with before nursing, *P < 0.05.
Psychological distress
Before nursing care, there were no notable differences in PDT scores between the 2 groups (P > 0.05). After nursing care, PDT scores of both groups dropped (P < 0.05). Reductions in the observation group were more pronounced (P < 0.05) (Table 5).
Comparison of Psychological Distress Scores of Patients Between the 2 Groups (
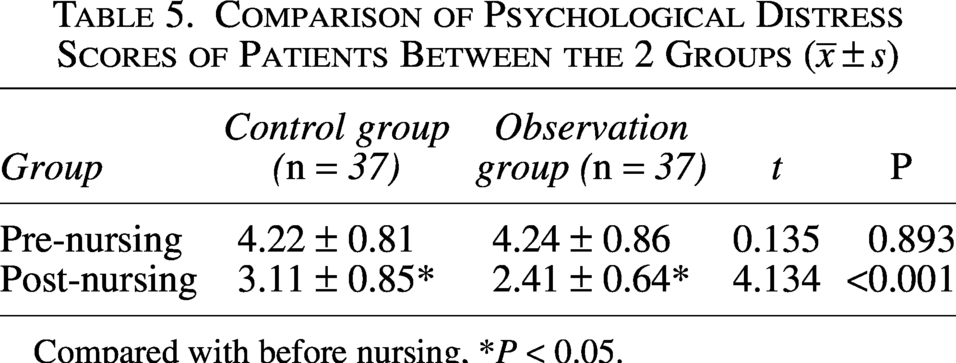
Compared with before nursing, *P < 0.05.
Sleep quality
Before nursing care, there were no noticeable differences in PSQI scores between the 2 groups (P > 0.05). After nursing care, PSQI scores decreased in both groups (P < 0.05), with a more remarkable reduction in the observation group (P < 0.05) (Table 6).
Comparison of PSQI Scores of Patients Between the 2 Groups (
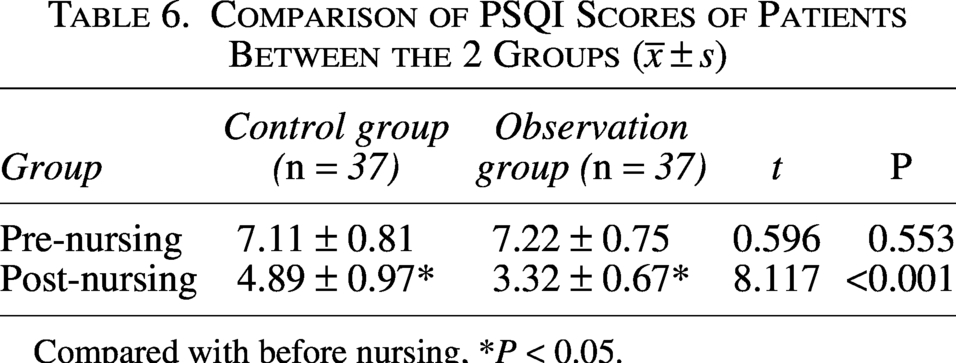
Compared with before nursing, *P < 0.05.
Nursing satisfaction
After nursing care, FAMCARE-2 scores were superior in the observation group in contrast to the control group (P < 0.05) (Table 7).
Comparison of Nursing Satisfaction Scores of Patients and Their Family Members Between the 2 Groups (

Discussion
Rising life expectancy and rapid population aging have heightened global focus on end-of-life care quality, with China being no exception. 20 Timely transition to end-of-life care enhances the experience for patients and families by providing continuous psychosocial support, regular opportunities to express preferences and concerns, and comprehensive, multidimensional nursing that ensures holistic, patient-centered care.21,22 This study aimed to explore the effectiveness of integrating narrative nursing with psychological resilience training in improving psychological adaptability among patients and their families in the hospice care setting. The findings offer a comprehensive perspective on the impact of this combined intervention model.
In terms of emotional well-being, both the control and observation groups showed significant post-intervention reductions in anxiety and depression, as measured by HADS-A and HADS-D scores, with the observation group exhibiting significantly greater improvements. Research suggests that narrative care enhances emotional processing by allowing patients to articulate life stories, reframe illness experiences, and foster a sense of continuity and identity in the face of life-limiting disease. 9 Psychological distress scores also declined more notably in the observation group. These benefits are likely attributable to the narrative nursing component, which allowed patients and family members to share personal stories and express their emotions, thereby alleviating psychological stress. In addition, the intervention strengthened social support and encouraged meaningful goal-setting, offering emotional reinforcement. These findings align with previous research by Zhou et al, 23 reinforcing the effectiveness of this integrated approach in addressing psychological challenges in hospice care. Regarding psychological resilience, CD-RISC-10 scores increased significantly in both groups after intervention, with the observation group showing a more substantial improvement. Psychological resilience is not fixed; it fluctuates under the influence of internal and external factors such as personal cognition, emotional regulation, and perceived social support.13,24 The structured resilience training included psychoeducation to raise awareness of resilience, cognitive-behavioral strategies to reframe negative thought patterns, and emotional regulation exercises to enhance coping capacity. These methods collectively improved participants’ sense of control and ability to manage stress and adversity. This outcome supports existing evidence that psychological resilience can be cultivated through targeted interventions such as cognitive restructuring, behavioral adaptation, and emotion regulation. 25
Sleep quality, assessed by the PSQI, improved in both groups post-intervention, with the observation group again demonstrating superior gains. The reduction in negative emotions and anxiety—facilitated by narrative expression and emotional support—may have contributed to better sleep. Narrative nursing, by promoting relaxation and emotional release, likely played a direct role in this improvement. 9 Nursing satisfaction was also higher in the observation group. Patients and families reported feeling more heard and understood through narrative nursing, while the resilience training contributed to a more stable emotional state. These combined effects translated into greater overall satisfaction with nursing care. Prior studies have shown that nurses trained in narrative techniques demonstrate greater professionalism, empathy, and humanistic care, which are critical factors in patient satisfaction. 26 Moreover, interventions that address both patient and caregiver needs are known to reduce caregiver burden and improve perceptions of care quality. 4
In conclusion, narrative nursing combined with resilience training offers a holistic, evidence-based strategy to enhance psychosocial adaptation, emotional well-being, sleep quality, and care satisfaction in hospice settings. Its multidimensional benefits align with international palliative care goals and represent a meaningful advance in the pursuit of dignified, compassionate end-of-life care. These findings underscore the potential of integrating narrative nursing and psychological resilience training into hospice care frameworks. The dual approach supports not only patient-centered care but also family adaptation and overall care quality. Nevertheless, this study has certain limitations. Firstly, the single-center design and relatively limited sample size may affect the generalizability of the study findings. In addition, the potential impact of individual differences in religious beliefs on disease perception, attitudes toward death, and emotional regulation was not considered, which may introduce confounding factors in the assessment of intervention effects. Future research could validate the universality of the conclusions through multicenter, large-sample designs and explore the long-term effects of combined interventions on bereavement outcomes and caregiver mental health through longitudinal follow-up. Furthermore, incorporating psychological and cultural variables such as religious beliefs into measurement and control will contribute to enhancing the accuracy of the assessment.
Footnotes
Author Disclosure Statement
The authors declared that they have no conflicts of interest regarding this work.
Funding Information
The work was not funded by any funding.