
Abstract
Atrial fibrillation (AF) is a highly prevalent comorbidity in patients with cardiomyopathy (CM), associated with worse cardiovascular outcomes. This study aims to provide a comprehensive, national-level analysis of AF and CM-related mortality in the United States. The Centers for Disease Control and Prevention Wide-Ranging Online Data for Epidemiologic Research database was utilized, using death certificates from 1999 to 2024. The study included patients aged ≥15 years with CM and AF. Statistical analyses were conducted to calculate age-adjusted mortality rates (AAMRs) per 100,000 individuals and annual percent changes with 95% confidence intervals (CIs). Between 1999 and 2024, CM with concomitant AF accounted for 134,470 deaths among individuals aged 15 years or older. The overall AAMR rose from 1.5 per 100,000 in 1999 to 2.3 in 2024. From 1999 to 2016, the AAMR rose modestly (1.5–1.8), followed by a pronounced rise from 2016 to 2022 (1.8–2.5), and a relative decline by 2024 (2.5–2.3). Compared with 2019, mortality in 2020 demonstrated a 15% relative increase (incidence rate ratio = 1.15; 95% CI: 1.11–1.19). Males had disproportionately higher AAMRs compared to females. By race, the highest AAMRs were observed in non-Hispanic (NH) Black and White populations (1.8 each). Regionally, the West and Midwest exhibited the highest AAMRs (1.9 each). Urban–rural stratification revealed higher AAMRs among rural areas (2.2) when compared with urban (1.8) areas. Targeted public-health interventions and resource allocation to address this growing cardiovascular mortality burden, particularly in high-risk demographic groups, are needed.
Atrial fibrillation (AF) is the most common sustained cardiac arrhythmia and a growing public-health burden in the United States and worldwide, driven by population aging, cardiometabolic comorbidities, and improved survival from structural heart disease.1,2 Contemporary estimates suggest that ∼6–8 million US adults are living with AF, and projections indicate ≈12.1 million US adults will have AF by 2030, reflecting a steady rise in age-adjusted incidence and prevalence over the past two decades. 1 Globally, AF affected ∼33 million people circa 2010, with persistent upward trajectories in both incidence and years lived with disability, underscoring its contribution to stroke, heart failure (HF), and excess mortality. 3
Cardiomyopathies (CMs), including hypertrophic cardiomyopathy (HCM), dilated cardiomyopathy (DCM), restrictive cardiomyopathy, and other phenotypes, provide major substrates for AF through atrial stretch, myocyte disarray, and fibrotic remodeling; in HCM alone, AF prevalence exceeds 25% across the lifespan and is tightly linked to thromboembolism and decompensated HF.4–6 In HCM cohorts, AF is the most frequent sustained arrhythmia, often symptomatic, and consistently associated with higher risks of embolic stroke, HF admissions, and reduced functional capacity, even as disease-specific treatment has advanced.5,6 Across multi-phenotype cohorts, AF is common in CM and portends worse outcomes: in a Nationwide Electronic Health Record Study, AF prevalence reached 23.6% in HCM, 42.5% in restrictive CM, and 44.4% in DCM, and concomitant AF was associated with higher odds of mortality and hospitalization irrespective of subtype. 7 DCM-focused analyses similarly show that persistent or permanent AF, although variably prevalent, confers adverse “hard-outcome” risk (death/heart transplant) over long-term follow-up, highlighting AF as an independent marker of severity in systolic CM. 8
Observed changes in AF-related mortality in CM—particularly inflection points after 2010—likely reflect the interplay of patient-level biology, health-system adaptation, therapeutic diffusion, and surveillance/coding practices, which together determine the “marginal adaptation” of population mortality at the edges of clinical and public-health capacity.1,2 Mechanistically, AF shortens diastolic filling, impairs relaxation, increases myocardial stiffness, and—when persistent with rapid ventricular rates—can precipitate tachycardia-mediated CM characterized by left-ventricular dilatation, reduced systolic function, and elevated filling pressures.9,10 Demographically, an aging US population increases exposure time to AF triggers and cardiomyopathic progression, raising both incidence and competing-risk mortality even as age adjustment mitigates some compositional bias.1,11 Comorbidity clustering (hypertension, diabetes, obesity, chronic kidney disease) intensifies atrial substrate remodeling and HF vulnerability, augmenting AF-mediated hemodynamic derangements in CM.1,2 Disease-specific substrate matters: HCM and restrictive physiology are particularly intolerant of loss of atrial systole and rapid ventricular response, whereas DCM may more readily manifest tachycardia-mediated systolic dysfunction; these pathophysiologic distinctions can shape short-term decompensation patterns and the longer-term patterns captured on death certificates.4,5,8
Urban–rural health care capacity further conditions outcomes: rural counties experience higher cardiovascular death rates and slower improvements. 12 End-of-life care patterns, including hospice penetration and shifting preferences for home death, also modulate place-of-death distributions for CM and may influence multiple-cause coding of AF on death certificates. 13 Despite extensive international literature, nationally representative US data characterizing mortality trends and regional disparities for CM with coexisting AF remain limited. Using mortality data from the Centers for Disease Control and Prevention Wide-Ranging Online Data for Epidemiological Research (CDC WONDER) database, this study addresses that gap by quantifying national and regional trends in AF-associated CM deaths and describing demographic patterns relevant to resource allocation and public-health planning. 14
Methods
Study setting and population
In this retrospective, population-based study, death certificate data from the CDC WONDER database were analyzed from 1999 to 2024 to evaluate trends in CM with AF-related mortality among US adults aged 15 and older. The CDC WONDER database compiles annual death certificate data from all 50 states and the District of Columbia, reporting both underlying and contributing causes of death along with demographic variables. 14 The study population included individuals aged 15 years and older. The authors used the International Classification of Diseases, 10th Revision (ICD-10) codes I42.0–I42.9 to identify CM-related deaths and code I48 to capture deaths associated with AF and atrial flutter, as previously used in administrative databases. 15 All deaths were included if these conditions were listed in the multiple cause-of-death field, regardless of whether they were identified as the primary or a secondary cause of death. As the study involved only publicly available, de-identified data, Institutional Review Board approval was not required. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology guidelines. 16
Data abstraction
Data were collected and categorized based on gender, racial and ethnic background, age bracket, geographic region, degree of urbanization, and US state. Gender was identified as either male or female. Racial and ethnic classifications included non-Hispanic (NH) White, NH Black or African American, Hispanic or Latino, NH American Indian or Alaskan Native, and NH Asian or Pacific Islander. The United States was divided into four census-defined regions: Northeast, Midwest, South, and West. Urban–rural status was determined using the 2013 Urban–Rural Classification Scheme for Counties developed by the National Center for Health Statistics. 17 Counties were grouped into urban areas (large central metro, large fringe metro, medium metro, and small metro) and rural areas (micropolitan and noncore). Age was grouped in 10-year intervals, beginning at 15 years of age and older. Additional details on variable definitions, category classifications, and ICD-10 codes used to define CM and AF are provided in Supplementary Table S1.
Statistical analysis
Trends in CM and AF-related mortality were analyzed using the Joinpoint Regression Program (V5.3.0, National Cancer Institute). 18 Age-adjusted mortality rates (AAMRs) per 100,000 individuals from 1999 to 2024 were calculated, standardizing to the year 2000 US population as the baseline, to account for differences in age distribution over time. 19 Monte Carlo permutation testing was applied to describe data with the fewest segments necessary, while preserving statistical significance. Significant trend changes were detected by fitting log-linear regression models, with potential joinpoints identified using a grid-search algorithm. The analysis began with a minimum of 0 joinpoints and evaluated up to a maximum of 4 joinpoints. Annual per cent change (APC) and its 95% confidence intervals (CIs) were estimated for each identified segment using the permutation test, and the weighted average of these APCs were reported as the average APC (AAPC) with corresponding 95% CIs to summarize trends across the study period. APCs were classified as increasing or decreasing if the slope representing the change in mortality was found to be significantly different from zero using 2-tailed t-testing. A zero slope indicated no change in mortality over time, while a positive slope signified an increase in annual CM and AF-related mortality trends. A P value of <0.05 was considered statistically significant. Year-to-year comparison of AAMRs between 2019 and 2020 was performed by calculating incidence rate ratios (IRRs) with 95% CIs using Poisson regression, accounting for annual death counts and corresponding population denominators.
Results
Between 1999 and 2024, CM with concomitant AF accounted for 134,470 deaths among individuals aged 15 years or older (Supplementary Table S2). Among cases with a documented location of death, 56,767 occurred in medical facilities, 42,331 at home, 23,734 in nursing homes or long-term care facilities, and 6072 in hospice (Supplementary Table S3).
Overall trends in mortality
The overall AAMR per 100,000 increased significantly from 1.5 in 1999 to 2.3 in 2024. From 1999 to 2016, the AAMR rose modestly (1.5–1.8; APC: 1.27; 95% CI: 0.87–1.66), followed by a more pronounced increase from 2016 to 2022 (1.8–2.5; APC: 5.56; 95% CI: 2.97–8.23), and a relative decline by 2024 (2.5–2.3; APC: −4.65; 95% CI: −14.70 to 6.59) (Fig. 1, Supplementary Tables S4 and S5). Between 2019 and 2020, the AAMR increased from 2.0 to 2.3, corresponding to an IRR of 1.15 (95% CI: 1.11–1.19) (Supplementary Table S6).
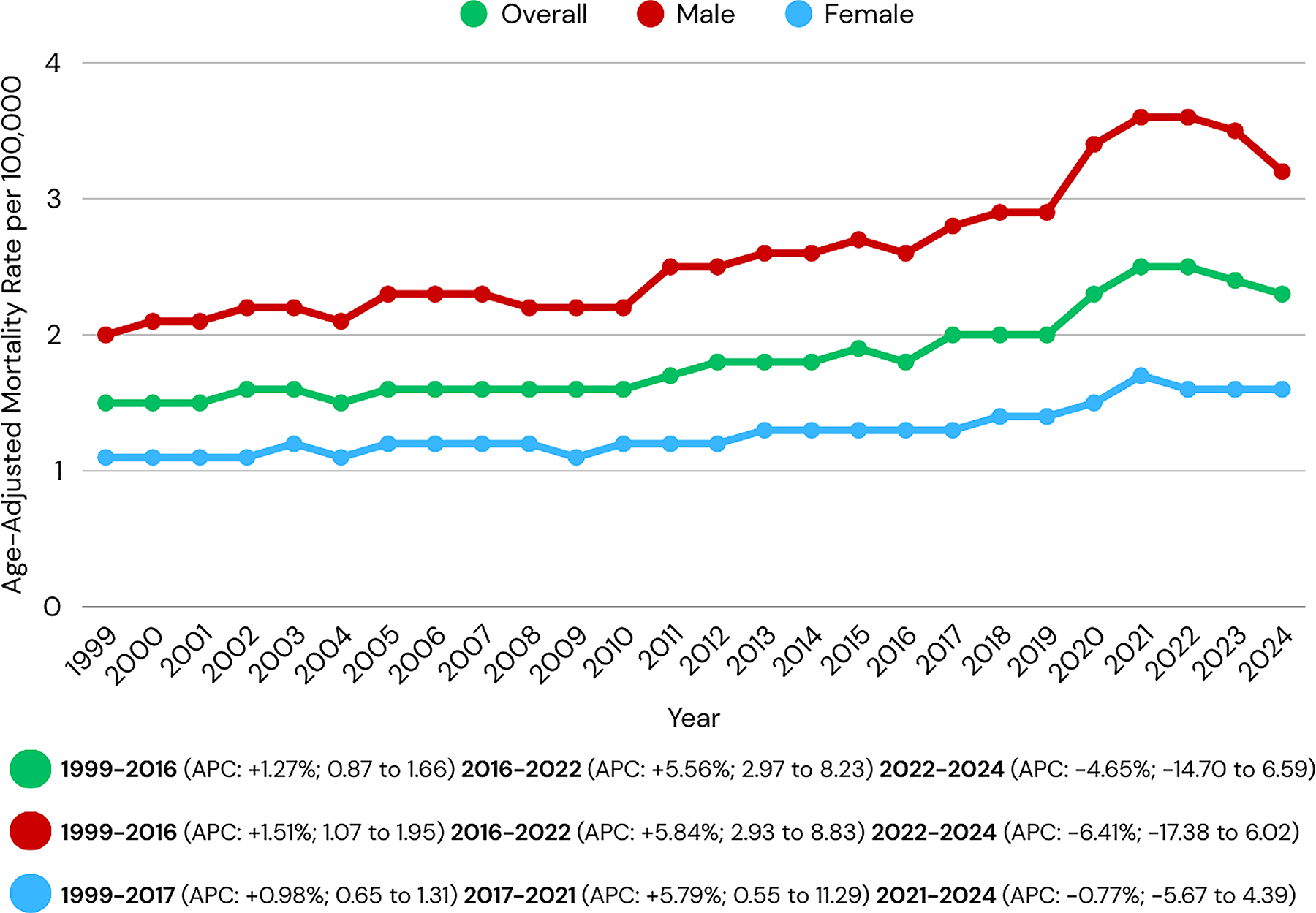
Overall and sex-stratified cardiomyopathy and atrial fibrillation-related age-adjusted mortality rates per 100,000 in adults in the United States, 1999–2024. APC, annual percent change.
CM with AF-related mortality stratified by sex
Sex-stratified analysis showed disproportionately higher AAMRs in males compared with females (Fig. 1; Supplementary Tables S4 and S5). Among males, AAMR rose gradually from 2.0 in 1999 to 2.6 in 2016 (APC: 1.51; 95% CI: 1.07–1.95), followed by a steeper increase to 3.6 by 2022 (APC: 5.84; 95% CI: 2.93–8.83), and ultimately a relative decline to 3.2 by 2024 (APC: −6.41; 95% CI: −17.38 to 6.02). In females, the AAMR increased from 1.1 in 1999 to 1.3 in 2017 (APC: 0.98; 95% CI: 0.65–1.31), followed by a rise to 1.7 in 2021 (APC: 5.79; 95% CI: 0.55–11.29), and a period of relative stability till 2024 (1.7–1.6; APC: −0.77; 95% CI: −5.67 to 4.39).
Race stratification for CM with AF-related mortality
Stratification by race revealed that the highest AAMRs were among NH Black and NH White individuals (1.8 each), followed by NH American Indian or Alaska Natives (1.2), Hispanics (1.0), and NH Asian or Pacific Islander populations (0.9). The AAMR for the NH White population showed an increase from 1999 to 2017 (APC: 1.72; 95% CI: 1.38–2.06), followed by a significant increase from 2017 to 2020 (APC: 6.01; 95% CI: 0.57–11.75). The AAMR for NH Black or African Americans increased from 1999 to 2017 (1.50; 95% CI: 0.89–2.10), followed by a pronounced rise that did not reach statistical significance (APC: 5.93; 95% CI: −3.50 to 16.28). The AAMR for NH Asian or Pacific Islanders decreased from 1999 to 2016 (APC: −1.14; 95% CI: −2.22 to −0.05), followed by a marked increase that did not reach statistical significance (APC: 5.71; 95% CI: 4.30–16.77). The AAMR for the Hispanic or Latino population remained stable from 1999 to 2010 (APC: 0.41; 95% CI: −0.90 to 1.74), followed by a prominent rise from 2010 to 2020 (APC: 2.50; 95% CI: 1.24–3.77) (Fig. 2, Supplementary Tables S4 and S5).

Cardiomyopathy and atrial fibrillation-related age-adjusted mortality rates per 100,000 stratified by race in adults in the United States, 1999–2020. APC, annual percent change; NH, non-Hispanic.
Region stratification for CM with AF-related mortality
Throughout the study period, the West and Midwest exhibited the highest regional AAMRs (1.9 each), followed by the South (1.7) and Northeast (1.6) (Fig. 3; Supplementary Table S7). At the state level, Vermont (2.9), Maryland (2.8), Hawaii (2.8), Ohio (2.4), and Washington (2.4) ranked in the top 90th percentile for CM with AF-related AAMR, reporting rates nearly double those observed in the 10th percentile states, which included New York (1.0), Nevada (1.1), New Mexico (1.1), Arkansas (1.2), Utah (1.2), Louisiana (1.2), Massachusetts (1.2), and Arizona (1.2) (Fig. 4, Supplementary Table S8).
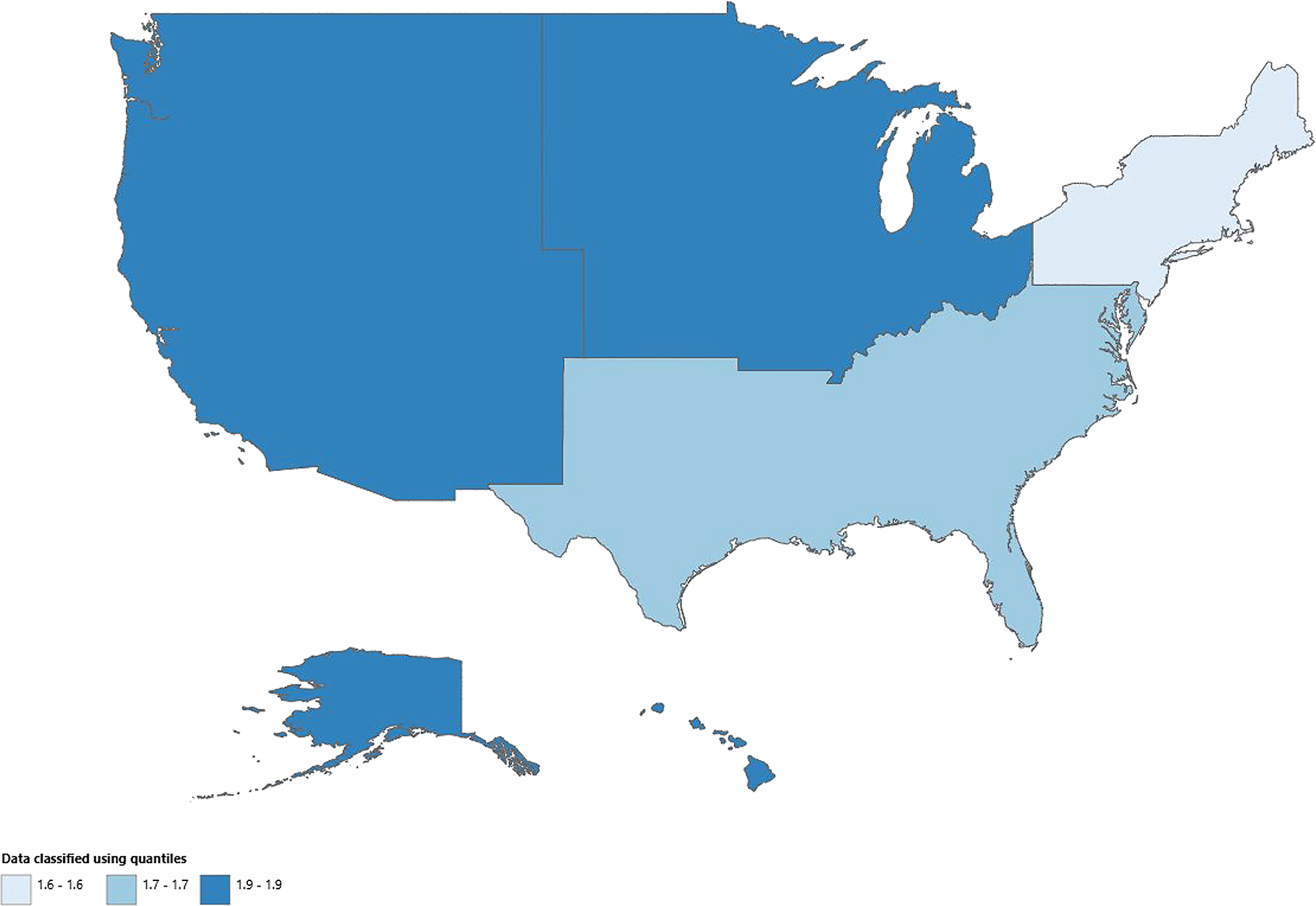
Cardiomyopathy and atrial fibrillation-related age-adjusted mortality rates per 100,000 stratified by census region in adults in the United States, 1999–2020.

Cardiomyopathy and atrial fibrillation-related age-adjusted mortality rates per 100,000 stratified by state in adults in the United States, 1999–2020.
Urban–rural stratification for CM with AF-related mortality
AAMRs for individuals with CM and AF were higher in rural areas (2.2) when compared to urban areas (1.8). In urban areas, AAMRs gradually increased from 1.5 in 1999 to 1.6 in 2010 (APC: 1.10; 95% CI: 0.57–1.64), followed by a rise to 2.0 in 2017 (APC: 1.98; 95% CI: 0.80–3.17) and further to 2.3 in 2020 (APC: 4.46; 95% CI: 1.48–7.52). In rural areas, AAMRs initially rose from 1.3 in 1999 to 1.7 in 2003 (APC: 5.36; 95% CI: 0.02–10.98), followed by a nonsignificant decline to 1.5 in 2007 (APC: −1.98; 95% CI: −8.99 to 5.57), and then increased to 2.0 in 2017 (APC: 3.04; 95% CI: 1.79–4.29) and 2.5 in 2020 (APC: 6.69; 95% CI: 1.57–12.06) (Fig. 5; Supplementary Tables S4 and S9).
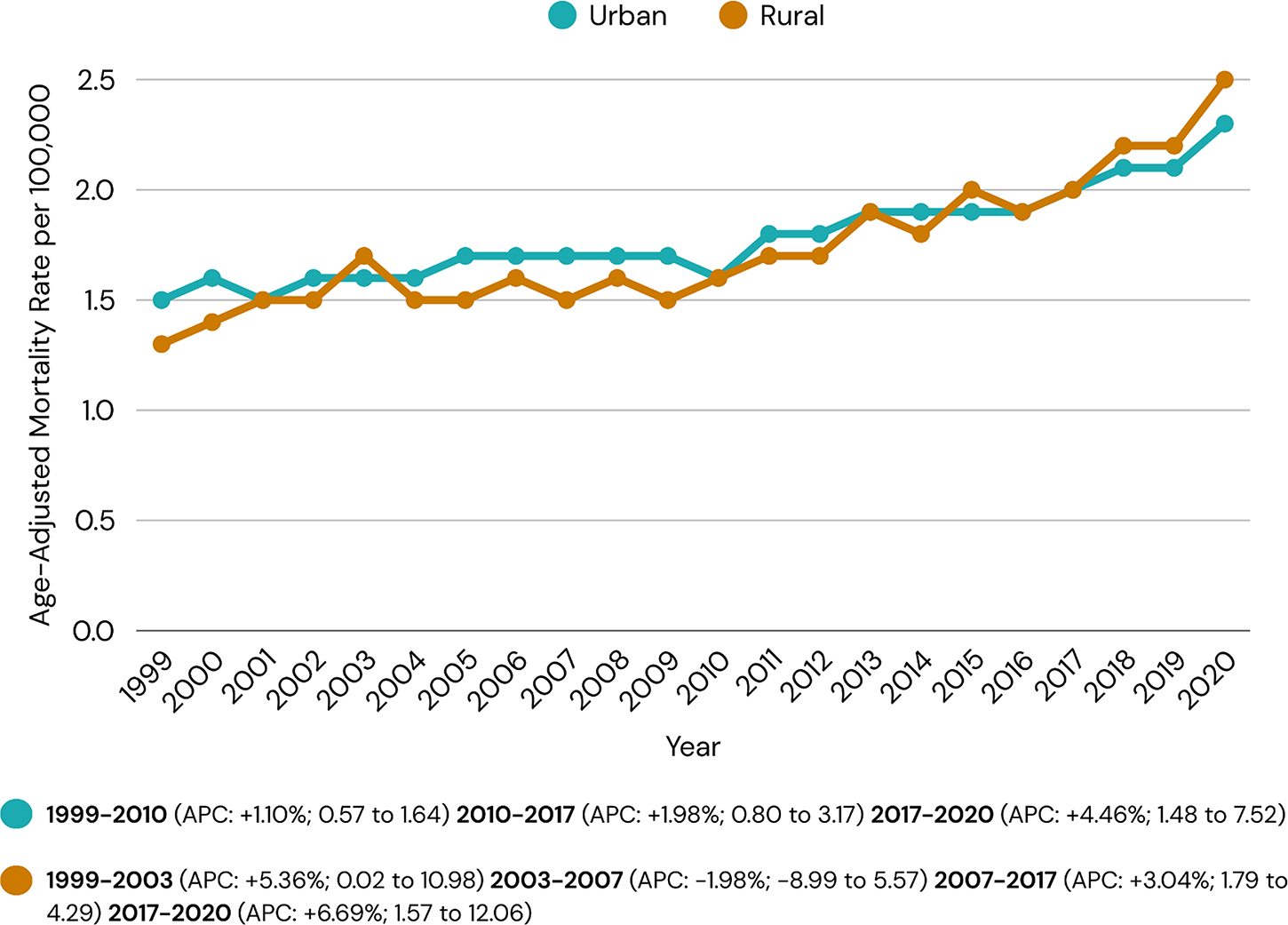
Cardiomyopathy and atrial fibrillation-related age-adjusted mortality rates per 100,000 stratified by urban–rural status in adults in the United States, 1999–2020. APC, annual percent change.
Discussion
This study demonstrated a significant rise in mortality rates among decedents with CM and AF from 1999 to 2024 (AAPC: 1.79*; 95% CI: 0.75–2.84; P < 0.05). Although both males and females showed increasing mortality over time, the trends indicated an unfavorable disparity between sexes (Fig. 6). Racial stratification showed that NH Black and NH White populations experienced the highest mortality rates, whereas NH Asian or Pacific Islander populations experienced the lowest. Clear geographic disparities were also observed across US regions, with the highest AAMRs in the West and Midwest regions and higher AAMRs in rural areas when compared with urban areas.
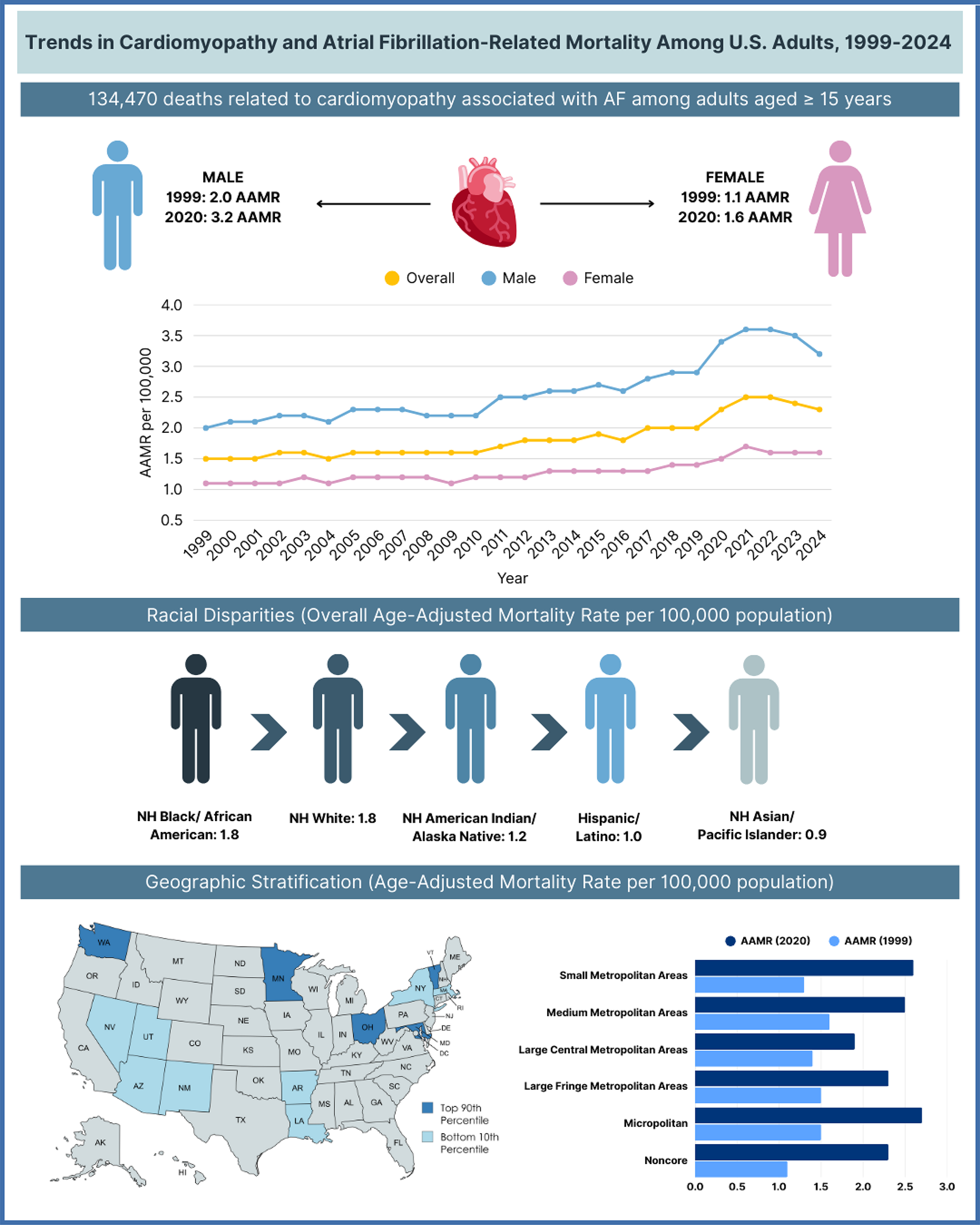
Central illustration of trends in cardiomyopathy and AF-related mortality among US adults, 1999–2024. AAMRs, age-adjusted mortality rates; AF, atrial fibrillation; NH, non-Hispanic.
The increasing mortality burden among individuals with CM and AF between 2002 and 2022 underscores the clinical significance of AF beyond thromboembolic complications. AF in the setting of CM can contribute to worsening cardiac function, increased hospitalization risk, and impaired quality of life. 10 These adverse outcomes may be related to hemodynamic compromise and impaired cardiac filling, along with neurohormonal and structural impairment. 20 From an etiologic perspective, the coexistence of AF and CM may plausibly increase mortality risk through loss of atrial contribution to ventricular filling, irregular ventricular activation, and tachycardia-related ventricular dysfunction, which can precipitate or worsen HF decompensation and recurrent hospitalization.10,20 Sustained rapid ventricular rates may also contribute to an arrhythmia-induced (AF-mediated) CM phenotype, further worsening ventricular function. 10 In parallel, the observed population-level increases may partly reflect improved recognition and identification of AF over time through expanded use of ambulatory and implantable monitoring and greater clinical awareness.
Consistent with these findings, prior national data have shown increasing AF-related hospitalizations, particularly among older adults with CM and multiple comorbidities, highlighting the growing strain this population may place on the health care sector. 19 Among patients hospitalized for HF, a common downstream consequence of CM, the prevalence of concomitant AF increased substantially between 2008 and 2017, emphasizing the increasing need for individualized treatment strategies in aging cardiac populations. 21 Collectively, these observations support the interpretation that the co-occurrence of AF and CM increasingly affects older adults and warrants vigilant monitoring and timely intervention.
Sex differences were evident, with males demonstrating consistently higher AAMRs across the study period. Men are more likely to develop AF at younger ages; however, given women’s longer life expectancy, lifetime AF risk remains similar across sexes (approximately 30%). 22 Potential contributors to higher mortality in males may include differences in modifiable risk factor burden and comorbidity profiles, such as smoking, alcohol use, and higher prevalence of chronic obstructive pulmonary disease, type 2 diabetes mellitus, and atherosclerotic cardiovascular disease. 23 Differences in health care–seeking behavior and treatment adherence may also contribute, as men have been reported to have lower adherence to recommended regimens and may delay seeking medical care. 24 In contrast, women with CM and AF may demonstrate better survival in some cohorts, consistent with prior reports showing improved long-term prognosis and lower adverse outcome rates.25,26 Nonetheless, women may experience delayed diagnosis and remain vulnerable to complications, including cerebrovascular events and cognitive decline, 27 underscoring the need for timely recognition and equitable access to appropriate AF and CM care in both sexes.
Racial disparities were pronounced, as NH Black patients with CM and concomitant AF had the highest mortality rates and a significant upward trend from 2002 to 2020. Multiple factors may contribute to these differences, including higher prevalence of cardiometabolic comorbidities such as hypertension, type 2 diabetes mellitus, and obesity, which may worsen prognosis in CM and AF. 28 Disparities in access to health care and tailored management may also play a role, including underutilization of anticoagulation and rhythm-control strategies. 29 Beyond broad differences in access, lifestyle, and adherence, potentially modifiable contributors may include inequities in timely AF detection and diagnostic evaluation (eg, access to electrocardiogram and echocardiography), initiation and persistence of appropriate anticoagulation, continuity of outpatient follow-up, and access to specialist-led management (eg, electrophysiology and CM/HF programs). Additional actionable factors may include medication affordability, barriers to longitudinal monitoring, and variability in the implementation of guideline-based therapies across health systems. These considerations should be interpreted as plausible, non-causal contributors and represent intervention targets that can be evaluated in future studies using clinical or claims-based datasets. Additionally, genetic testing remains underutilized in hereditary cardiovascular diseases such as CMs, particularly among NH Black populations. 30 Despite its importance for risk stratification, socioeconomic stressors may accelerate health deterioration in African American women through the “weathering hypothesis.” 31 Taken together, these inequities underscore the need for targeted strategies to improve care access, continuity, and evidence-based management in high-risk populations.
Geographic disparities were also evident. AAMRs were higher in rural areas when compared with urban areas, although both settings showed increasing trends over time. Despite rising AAMRs, rural populations may face delayed diagnosis, limited access to specialized health care services, and socioeconomic barriers that impede timely and high-quality care. 32 In addition, patients in rural settings are less likely to receive advanced cardiac procedures, which may contribute to adverse outcomes in CM and AF. 33 Regionally, the West and Midwest exhibited the highest mortality burden during the study period. This pattern may reflect a confluence of factors, including higher prevalence of modifiable cardiometabolic risk factors (eg, obesity and hypertension), access barriers in remote or underserved areas, delayed clinical recognition, and suboptimal implementation of evidence-based protocols.34,35 These findings support the potential value of regionally targeted interventions such as telehealth expansion, improved referral pathways, and culturally responsive patient education to reduce inequities in cardiovascular care and outcomes. 36
Several limitations should be considered. First, reliance on death certificate data introduces potential inaccuracies in identifying the underlying cause of death and capturing coexisting conditions; documentation of CM and AF may have limited sensitivity and specificity, and both conditions may be underreported or misclassified, particularly when not listed as the primary cause of death. Inconsistencies in documentation practices across states and health care institutions may further affect validity and could influence apparent temporal patterns. Second, ICD-10 coding (eg, I42.1, I42.2, and I48) restricts analyses to documented diagnoses and does not allow distinction by clinical subtype or severity (eg, persistent vs paroxysmal AF). Third, the dataset lacks individual-level clinical information (eg, treatment regimens, comorbidity burden, or complications), limiting assessment of how differences in care influence outcomes. Fourth, demographic representation may not be uniform, and SDOH were not directly measured, potentially contributing to observed disparities across racial, ethnic, and geographic groups. Fifth, listing CM and AF on a death certificate does not confirm these as primary contributors to mortality. Fifth, because data for racial groups after 2020 were formatted inconsistently, and information on urban–rural stratification was unavailable beyond 2020, these variables could not be included in the study. Last, the descriptive nature of this analysis precludes causal inference regarding associations between demographic or geographic factors and mortality outcomes in patients with CM and AF. Despite these limitations, the analysis leverages a large, nationally representative dataset via CDC WONDER and a prolonged observation period, providing valuable context for the evolving epidemiology of CM and AF in the United States.
Conclusion
AF-related mortality in patients with CM has significantly increased in the United States over the past two decades, with a sharper rise observed since 2010, peaking in 2021. The burden of mortality is disproportionately higher among males and the NH Black and White populations. Targeted public-health interventions and resource allocation to address this growing cardiovascular mortality burden, particularly in high-risk demographic and geographic groups, are needed.
Authors’ Contributions
H.M.S.: Study conceptualization, data curation, statistical analysis, and article writing. O.E.A.: Data curation, statistical analysis, article writing, review, editing. O.A.D., A.A., and A.B.: Article writing, review, and editing. M.A.: Formal validation, article writing, review, and editing. N.P.: Graphical data visualization. M.J.: Data organization, article review, and editing. A.H.: Data organization, article review, and editing. A.B.: Project supervisor.
Footnotes
Availability of Data and Materials
Author Disclosure Statement
The authors declared no potential conflicts of interest concerning the research, authorship, and/or publication of this article.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.