
Abstract
Traditional medical care accounts for 10% of health outcomes, whereas SDOH account for over 60%. Optimal care of older adults with chronic illnesses requires integration of medical and social service providers. Such partnerships remain uncommon. The authors describe a successful health system/Area Agency on Aging (AAA) integrated team model that meets weekly to discuss challenging community-dwelling older adults and generate care recommendations back to the primary care providers. As part of a quality improvement project, outcomes measured over 6 months during 1 year show a statistically significant decline in the number of important threats to independent living related to the 4Ms (ie, lower fall risk, fewer high-risk medication issues, less behavioral health concerns, and less frequent health care utilization). AAA care managers expressed high satisfaction with the team process and indicated that it helped them address important issues. This model is easily replicated and modifiable to differing local needs. If replicable in rigorously designed research studies, these results would argue for changes in Medicare and Medicaid reimbursement policies to support this interagency integrated model of collaborative care.
As the number of older adults rapidly increases, health care systems must prepare for the accompanying increase in health care utilization. Chronic illness care will be a dominant issue because 80% of those ≥65 years of age have at least 1 chronic condition and 65% have at least 2. 1 Despite being the highest utilizers of health care, the vast majority of those over the age of 65 express dissatisfaction with the current US health care system. 2 These concerns are validated by objective data as the United States ranks 46th in lifespan and 72nd in health span, despite spending significantly more per capita on health care delivery than other developed countries. 3
Health systems, focusing on disease treatment, often fail to incorporate evaluations by social service providers, even though SDOH account for more than 60% of health care outcomes. 4 Because SDOH play an outsized role in health outcomes, achieving optimal chronic illness care for older adults can only occur using models of care that support interdisciplinary practice that integrates community-based social service providers and health care providers. 5 Despite this well-known link between physical and SDOH, most health systems fail to achieve such integration, with highly fragmented systems remaining the dominant model in the United States. The literature is lacking in theoretically grounded models that effectively integrate clinical and community-based social services.
Purpose
The purpose of this report is to describe the theoretical basis for the Care Management Interdisciplinary Team (CMIT), a successful collaborative partnership between providers from a health care system and community-based long-term services and supports, whose mutual goal is to optimize care of community-dwelling older adults by integrating these providers in holistic care planning. The methods and data presented are part of a leadership quality improvement (QI) project to improve outcomes captured for the CMIT intervention.
Theoretical Framework
Wagner et al6,7 theorized that optimal care for consumers with chronic illness is not possible in health care systems that heavily emphasize disease treatment. According to Wagner’s theoretical framework, improvement in the care of consumers with chronic conditions can occur only by changing organizational structures, establishing community linkages, providing effective self-management support, implementing delivery system redesign, using evidence-based decision support, and improving information systems. According to this theory, implementation of these changes should result in more productive interactions between consumers and providers who assure the delivery of services that promote optimal outcomes. Wagner’s framework has guided the development of numerous chronic illness management programs over the years, but models that integrate community-based and health care providers are still lacking.
The CMIT intervention described herein incorporates the elements of Wagner’s theoretical framework to create a care model that is integrated into the consumer’s total health care and is responsive to consumer and family needs. The core of the CMIT model involves regular interdisciplinary team consumer care meetings comprised geriatricians, nurses, social workers, and pharmacists from both the Health System and the local Area Agency on Aging (AAA). This allows for effective communication across disciplines and agencies and provides support for care managers (CMs) implementing the intervention. With this interprofessional team model, CMIT is able to integrate health care and community-based providers and cut across traditional silos created by Medicare and Medicaid payment policies. (Note that CMS CMIT is a similar acronym, but it stands for CMS Measures Inventory Tool).
Setting
CMIT is a collaboration between Summa Health System in Akron, Ohio, and Direction Home Akron Canton Area Agency on Aging and Disabilities (Ohio AAA 10B). Summa is an integrated health delivery system with 750 inpatient beds on 6 campuses, a multispecialty medical group and a health plan. AAA 10B is an independent, private, nonprofit corporation that serves over 7000 older adult consumers in NE Ohio. AAA 10B is designated by the Ohio Department of Aging to develop a network of services to assist older adults and their families. Its mission is to provide older adults and their caregivers with long-term care choices, consumer protection, and education, so they can achieve the highest quality of life and live independently for as long as possible. The population served by the AAA extends across 4 counties and several not-for-profit health systems/hospitals including Summa. CMIT emerged from a previous collaborative project between these entities called SAGE 7 (the SAGE reference included below provides an in-depth description of the process undertaken to build the foundational working relationship between the health system and the AAA). 8 CMIT was a product of intentional direct communication between health-system leadership and the local AAA and their agreement that a partnership was optimal to benefit consumers and providers to reduce avoidable health care utilization and promote independent living for their shared consumers. Formal contracts were executed between these entities to ensure institutional commitments for providers’ time, and eventually, there was reciprocal representation on each entity’s board of directors. In this model, the AAA reimburses the health system for the CMIT team meeting time of the geriatrician. AAA has always compiled an annual summary of CMIT outcomes, but starting in 2024, the AAA created a dashboard to track and trend outcomes. The AAA Quality Committee reviewed the data quarterly for ongoing QI. The data reported here is part of the QI process to improve capture of the most common outcomes that threaten independent living to quantify the impact of CMIT.
Target Population
The CMIT provides a forum for the AAA CMs to discuss community-dwelling consumers with complex physical, mental, spiritual, and/or psychosocial needs with an interprofessional team. CMs are registered nurses or licensed social workers who present consumers to the team comprised geriatricians, pharmacists, and peer nurses and social workers. Consumers who are presented to the team are generally Medicare/Medicaid dual eligible, medically complex, and/or have complicated social issues. CMs follow a rotation and facilitate case discussions 3 times a year and can bring additional cases to the team as concerns are identified. CMs communicate with primary care physician (PCP) prior to the CMIT meeting and at initial and yearly assessments. CMs review their case load of approximately 70 consumers to identify cases that meet 1 or more of the following criteria to discuss with the team:
Polypharmacy and medication optimization, drug interactions, or concerning side effects Frequent health care utilization (2 or more hospitalizations in the last 6 months) Uncontrolled chronic illnesses and/or multiple comorbidities Frequent falls, falls with injury, or need for medical attention Significant health changes or uncontrolled symptoms (eg, weight loss, depression, pain, shortness of breath, change in functional status, failure to thrive) Permanent nursing home placement risk CM seeking input after exhausting their known resources
Overview of the Care Management Process
AAA provides care management services to consumers who meet the intermediate level of care and state-established poverty levels. Most consumers are seen every 90 days, but CMs will visit consumers more frequently after significant events such as hospitalizations or facility admissions. As part of standard workflows, CMs obtain assessment information through consumer reports, insurance notifications, ED visits and hospitalizations, communication with health care providers, and direct observation. CMs note current and past diagnoses, medications, and assess for fall risk, mobility issues, equipment, and health product needs. Behavioral health and emotional status are assessed using standardized tools such as those for depression and social isolation. CMs schedule in-home visits and meet the consumers to observe their daily environment and assess unmet activities of daily living (ADL) and Instrumental ADL are assessed, noting gaps or barriers in self-care. Many of these individuals lack social supports such as family or caregivers and live in subsidized housing. When gaps are identified, the CMs will coordinate services to meet these needs, such as personal care aides, homemaking and chore, transportation, emergency response system, and home-delivered meals services. They can also arrange for minor home modifications or vehicle modifications to improve accessibility. CM also assess for caregiver availability and stability. Considering all areas, the CM and consumer develop a plan of care with goals and services available and monitor and update these continuously.
The CMIT Team
CMIT meets weekly (previously in-person, now virtually since 2020) for 1 hour to discuss complex consumers. The CM identifies a consumer on their caseload that meets 1 or more of the criteria listed above and prepares a case summary outlining the consumer’s demographics, diagnoses, payor, medications, living situation, services, overview of function, mental health, safety, areas of concern, and consumer goals of care (see Fig. 1 for the summary content). Recommendations to assist with and resolve the issues are discussed as a team. An overview of the discussion and recommendations are summarized on a Team Communication Form (Fig. 2), and a copy is faxed to the PCP who was made aware of the CMIT meeting prior to occurring. A copy of the recommendations is also given to the CM who shares them with the consumer and implements those aspects within their scope of practice.
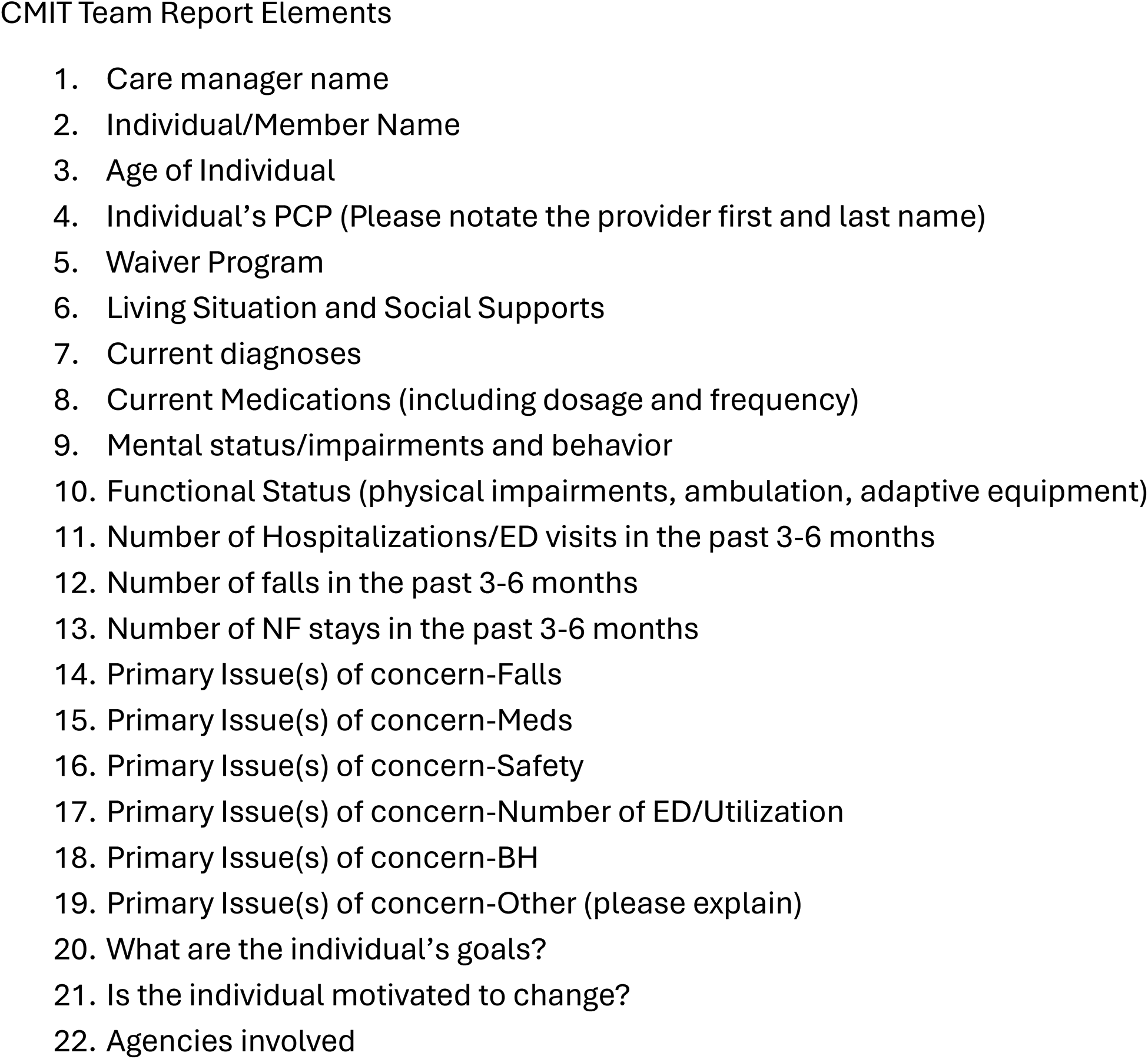
CMIT team report elements. BH, behavioral health; CMIT, Care Management Interdisciplinary Team; ED, emergency department; NF, nursing facility.
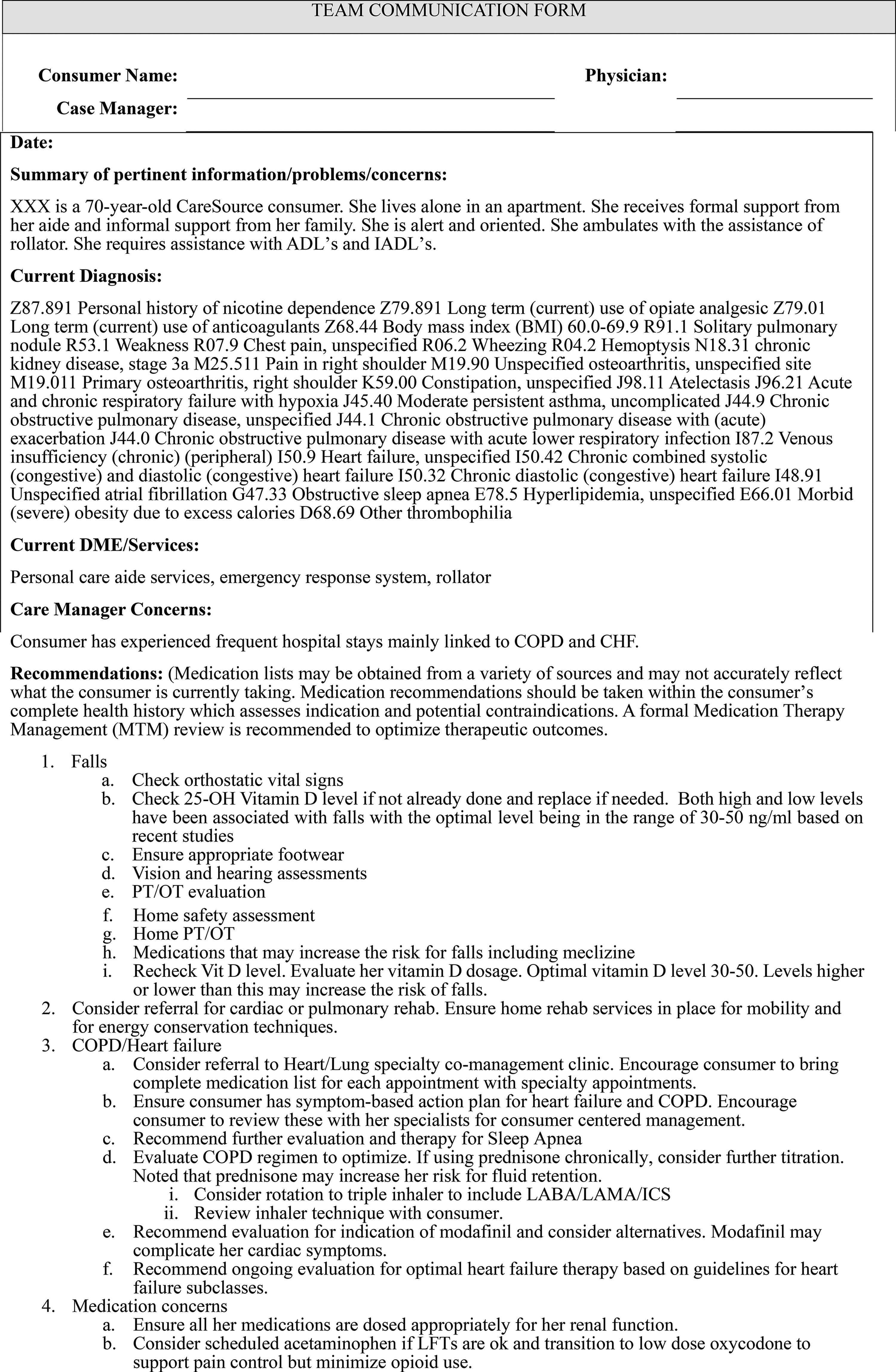
Team communication form.
Current Issues Identified Through the QI Process
Data were collected as part of the team’s QI process to estimate the team’s impact for purposes of institutional support of the model, rather than relying on anecdotal reports from CMs. Although it lacks rigorous scientific design, the data here are meant to serve as pilot data to guide the design of future rigorous studies and to facilitate sample size calculations. Data include process measures and consumer-centered outcomes measures. Data were collected via a nonmandatory questionnaire where responses were dichotomous and kept to yes/no in order to reduce respondent burden and encourage completion. Process measures asked whether team recommendations were implemented at follow-up and whether they felt the CMIT team intervention was helpful to the particular consumer discussed. Consumer-centered outcomes reflect the most common issues encountered by the team as well as those most likely to diminish the consumer’s ability to live at home. These outcomes reflect goals for providers across the care spectrum as well as goals that support the 4Ms.
CMs identify a consumer on their caseload with concerns that threaten independent living. The case summary serves as the baseline data. To obtain follow-up data, the AAA supervisor contacts all CMs who present consumer cases via e-mail at 3- and 6-month postteam meeting as part of their internal QI process. CMs are asked whether each of the following consumer-centered key variables is a current issue of concern at the initial team review and at follow-up based on their knowledge of the consumer:
Falls Medications Safety (environmental, medication, mental health) Health care utilization per insurance notifications to the CM Mental health
A QI committee at AAA meets monthly to review these data in their rapid cycle QI process where they look for trends requiring intervention adjustments.
Statistics
Data presented here were collected over 1 year from January 2023 to December 2023 as part of a QI leadership project with the goal to improve outcomes captured for the CMIT intervention. Outcomes were evaluated using descriptive statistics, and chi-square test was performed for differences in percentages of consumers exhibiting each issue pre and post CMIT.
QI Results
Baseline data were available for 81 consumers presented during the 1-hour CMIT meetings in 2023. The small number indicates missed meetings due to holidays and vacations, as well as transitions in staffing. Three-month follow-up data were available for 64 of these, and 6-month follow-up data were available for just 26. Overall, the number of key issues being experienced by consumers declined from baseline to 6 months (Table 1). Recall that the key issues being examined are falls, medications, safety, health care utilization, and mental health issues. CMs responded yes if a variable that was present at baseline remains an area of concern at follow-up.
Consumer Baseline and Follow Up Key Issues

At 3 months, CMs indicated that in 32% of cases, the CMIT team recommendations were implemented; in 23% of cases, the recommendations were not implemented yet; and in 44% of cases, they were unsure of whether recommendations were implemented. Many of the “unsure” responses were due to missing data at 3 and 6 months. Note also that CMs may not have conducted a follow-up visit at the time of the 3- or 6-month outcome measure and therefore would be unsure of whether recommendations were implemented. Furthermore, the PCP does not report back to the CM, so recommendations may have been implemented without the CM’s knowledge. Seventy percent of CMs indicated that the CMIT intervention was useful in this specific case, with 26% indicating it was not useful, and 3% unsure.
Data were paired pre/post intervention. Due to missing data at 6 months, a chi-square test was performed to compare baseline and 3-month outcome data only. Consumers with missing follow-up data were excluded from the analysis. This analysis showed that 33% of those who listed falls as an issue at baseline indicated it was not an issue at 3 months (P < 0.0001) (Table 2). Fifty-two percent of those who listed medication issues at baseline indicated that medications were not an issue at 3 months (P = 0.03). Forty-five percent of those who said safety was an issue at baseline said it was not an issue at 3 months (P < 0.0001). Thirty-six percent of those for whom ED use/hospitalizations were an issue at baseline indicated it was not an issue at 3 months (P < 0.0001). Finally, 29% of those for whom there was a behavioral health issue at baseline indicated that it was not an issue at 3 months (P = 0.006 Table 3).
Number of Key Issues Identified Over Time by Consumer

Resolution of Issues
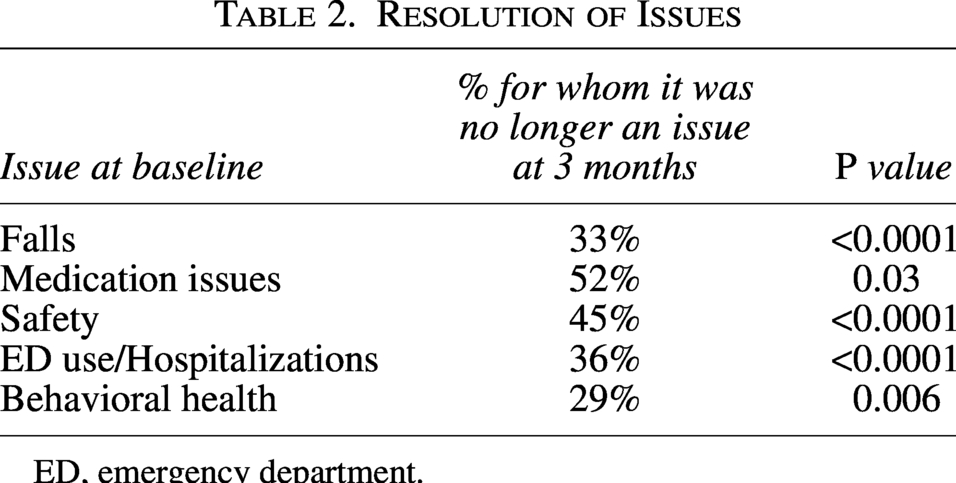
ED, emergency department.
How CMIT Is Consistent with Wagner’s Chronic Illness Care Model
Delivery system redesign
The redesign implemented in CMIT is the integration of the medical and social models of care by creating an interprofessional and interagency collaborative care management team that meets together in real time, utilizes community-based social worker and nurse CMs, as well as health system geriatric medicine and pharmacy experts. The team communicates care recommendations with the consumer and the PCP. The ability of these typically siloed providers to meet together and discuss cases in real time is not characteristic of most health systems. The involvement of the CM helps ensure coordination of care across all providers and settings in a way that is generally not possible for a single primary care provider. CMIT CMs highlight consumer-centered goals and concerns with the team to keep the consumer’s voice at the forefront of recommendations. It is normal for clinicians to tend to focus on diagnosis and symptoms while being unaware of the struggles at home for their consumers to remain compliant with the treatment plan. Consumers may not disclose or may not realize the impact of their home environment. CMs see this firsthand during their home assessments.
Establishing community linkages
In the CMIT model, a health care system and an AAA are acting as full partners. Optimal care for complex chronic conditions requires such integration of medical and social service providers. 9 AAA personnel ensure that psychosocial needs are addressed and assist with gaining access to those services, whereas members of the medical team help assure optimal medical and geriatric syndrome management. An example of the benefit of this collaborative relationship is demonstrated through medication management. Polypharmacy is a major issue in this population, potentially contributing to excess morbidity, avoidable hospitalizations, and suboptimal outcomes.10,11 In addition, medical providers are often unaware of the realities of the consumers’ medication management practices and/or adherence. 12 AAA CMs have firsthand knowledge of medication adherence through their in-home assessments. Without CMIT, medical providers would assume medications are being used as prescribed, and the AAA CM would not generally know about dangerous drug interactions or recognize new symptoms as potential drug side effects. In an integrated team, all sides of an issue emerge in real time, so every provider has a clearer picture from which they can make more meaningful recommendations.
Providing effective self-management support
The first step in effective self-management support is having the consumer state their values and goals of care. As can be seen in Figure 1, all CMIT cases include consumer-stated goals. CMIT assessments also include a question regarding the consumer’s motivation to change. Armed with this knowledge, more appropriate care plans can be devised to meet consumers where they are in their readiness to change to help them achieve their goals. The CM promotes self-directed care by providing the consumer with a written summary of the care plans devised by the team, as well as with educational resources. CMIT consumers often have low health literacy and inadequate knowledge of their conditions or prognosis. 13 CMs can provide education, assistance, skills training, coaching, and help with problem-solving. The CM also maximizes consumers’ psychosocial support to optimize their ability to self-manage. Advance care planning is also incorporated into the intervention to ensure that clients maintain as much control over their care as they desire to ensure care parallels what matters most.
Organizational structure, leadership, incentives, and resources
The CMIT intervention would not be possible without the cooperation between the health system’s leadership and high-level administrators at the AAA. The health system and AAA have a shared goal: for their consumers to remain healthy and live independently for as long as possible, which also coincides with what matters most to many older adults. Leadership from both organizations realized that optimal outcomes for consumers with chronic conditions could not be obtained if professional silos were not breached. 8 They agreed that only through a collaborative team process using professionals representing the complete biopsychosocial sphere could the goals of both health care and social service providers be met. Despite leadership changes at both organizations since the CMIT team intervention began in 2004, CMIT remains a priority across institutions. Furthermore, additional iterations and expansion of the CMIT team have occurred over time.
Evidence-based decision support
CMIT recommendations are discussed with the team and include community and agency-based connections with evidence-based programming. Consumers are often referred to community-based programming offered by the AAA including Bingocize 14 and Tai Chi 15 related to fall prevention strategies and Powerful Tools for Caregivers. 16 Team recommendations including short paragraphs containing academic detailing are provided to the consumer’s PCP and appropriate specialists. These might feature considerations for additional medical workup and medication optimization with references to pertinent evidence-based guidelines. To support consumer goals around what matters most and align with evidence-based practices, consumers may be encouraged to pursue palliative care evaluations to optimize symptom management. Nonpharmacologic interventions with known efficacy and recommendations for evidence-based community supports are also embedded in these recommendations. Examples include evidence-based guidelines for falls prevention, sleep hygiene, and management of incontinence. Recommendations also include referrals to community-based programs with known efficacy such as the Alzheimer’s Association for caregiving supports around dementia-related behaviors or home-based behavioral health supports. 16
Improved information systems
Health information sharing platforms have expanded, and community-based CMs are increasingly able to access real-time hospital records, insurance information, medication dispense reports, and other information to enhance care management strategies. This information is incorporated into team reviews. Team assessment findings and computerized care plans are communicated to the PCP by fax and/or phone. To optimize the effectiveness of this written communication, recommendations are kept brief to help ensure they are read and to minimize the burden on PCPs.
Despite advances in technology, communication between health system-based and community-based providers remains a challenge. 17 AAA leadership continues to seek opportunities to improve information sharing across electronic health records (EHRs)/platforms because cross-communication remains especially challenging.
Consumer communication remains one of the most difficult and important information challenges. CMs assess for technological barriers and offer digital literacy training. Additionally, the CMIT intervention always assesses consumer goals and wishes. This provides a means for the CM to serve as a proxy for the consumer in the team to express what matters most to the consumer in a way that does not happen in a lot of interdisciplinary teams. The communication back to the consumer, although there are still opportunities to improve, closes the loop of communication of what matters to the consumer.
Alignment of CMIT with Age Friendly
CMIT is an integrated care model that focuses on consumer goals of care and spans medical and psychosocial determinants of health. Through provider integration, CMIT eliminates duplication or gaps in services through communication across the continuum from the medical to the community setting. Although it predates them, CMIT aligns with Age-Friendly Health System goals endorsed by The Hartford Foundation and the Institute for Healthcare Improvement as a framework for organizing geriatric care to improve outcomes. 18 The Age-Friendly model focuses on the “4Ms”: what Matters most, Mentation including cognitive and behavioral health concerns, Mobility such as ambulation and falls risk along with transportation concerns, and Medications to ensure that when medications are necessary, side effects and interactions are minimized and are utilized to maintain what matters to the individual. This model reprioritizes care to become more responsive to consumer goals and preferences and emphasizes the contribution of SDOH in influencing health outcomes. CMS has endorsed this model by recently approving a quality measure that will require hospitals to report on their ability to provide Age-Friendly care, 19 and Summa is actively pursuing Age-Friendly Health System recognition. One of the key components of hospital integration is to address social vulnerability in older adults. CMIT advances the Age-Friendly model by linking health systems, AAAs, and community-based programming to directly address medical and SDOH of older adults. The community linkages associated with CMIT align with Age-Friendly 4Ms health care and community concepts by focusing on medications, aligning with what matters most to the consumer, addressing mentation, and optimizing mobility.
Discussion
Acknowledging the limitations of QI analyses in making causal inferences and the small sample size with a 3-month follow-up, results of this QI project did show significant improvement for key outcomes related to medical, social, physical, and behavioral outcomes, with issues identified at baseline decreasing over time. Moreover, an overwhelming number of CMs (70%) found CMIT to be helpful. CMIT can provide support to CMs by validating their concerns and providing psychological support. These results argue for expansion of the model to reach larger segments of the population to help both health systems and community-based providers meet the mutual goal of supporting people to live independently for as long as possible. For example, this intervention was shown to have a positive impact on falls, which is one of the biggest risk factors associated with living independently.20,21 Using written team recommendations, CMIT assists the PCP in delivering the best evidence-based care for older adults, which infuses geriatric-specific knowledge into primary care. This helps mitigate the impact of the growing shortage of trained geriatricians (ie, less than 50% of geriatric specialty fellowships are filled each year 22 ).
Another benefit of CMIT is that it supports national efforts aimed at improving geriatric education as championed by the Bureau of Health Workforce (BHW) through Health Resources and Services Administration (HRSA)’s Geriatric Workforce Enhancement Programs (GWEPs). CMIT disseminates evidence-based geriatric education to all levels of providers. As the team brainstorms to find interventions that will help consumers, all team members are educated on resources and information that can be applied to other consumers. CMIT demonstrates how real-world challenges of implementing evidence-based guidelines in older adults with complex medical and social concerns benefit from an interprofessional team approach. This education extends to the medical providers that are sent the evidence-based recommendations as well as the many health-profession students and residents who attend the CMIT meetings. It also extends to consumers and families because CMs share the team recommendations with them.
The actualization of this project’s framework has additionally produced a pipeline for future opportunities to implement best practices while caring for older adults and measuring outcomes for consumers who are not typically included in studies. In particular, the medication recommendations supplied by the team’s pharmacists have integrated evidence-based recommendations from the American Geriatrics Society and European groups into the care of each consumer by assessing complex medical scenarios and detecting probable medication adverse effects. Reviewing the totality of these recommendations creates the potential to systematically approach care at the local level; specifically, these recommendations may be tabulated and characterized with the purpose of identifying recurring patterns affecting our community. These patterns may then lead to educational opportunities for community outreach and interprofessional education regarding safe medication use. Moreover, they may be converted into evidence-based recommendations for medication management principles in support of Age-Friendly communities.
Limitations of CMIT
The most important limitation of CMIT is communication to the medical provider when they are not present at the team meeting. Currently, the recommendations are faxed to the provider. With the number of communications that most medical offices receive, it is likely that some of these do not reach the appropriate provider. The authors have trialed other versions of CMIT including a model where the CMIT CM accompanied the consumer to their PCP visit to review the recommendations of the team. This model had limited efficacy and acceptability for providers and consumers. 22 More recently, the CMIT model has been expanded to include representation from primary care (PCP or medical care management providers) who actively present the case to the team, receive recommendations directly from team members, and are able to implement recommendations in real time. Participating primary care offices find the model helpful. 23 Currently, the authors are collaborating on a HUD-funded expanded CMIT model with the local Habitat for Humanity affiliate where someone with direct primary care communication is present at the team meeting. The authors endorse a version of CMIT where someone in communication with the primary care office is present to ensure team recommendations are delivered.
Another limitation is finding the best method to relay complicated medication recommendations. Medication changes occurred in about 11% of consumers. Coordinating recommendations with an office visit or having someone from the PCP office (or who communicates directly with the PCP office) will likely help this as well. Sending a pharmacist’s written recommendations is another way to improve communication of complex information with the PCP office.
With respect to barriers that occur during the interprofessional meetings, the authors found that obtaining accurate information about each consumer’s medication list can be challenging. Although each CM obtains and submits medication lists, without an integrated EHR, these lists are often incomplete or not accurately representative of the consumer’s chronic medical conditions. Additionally, the medication lists do not capture medication adherence, may reflect outdated medication lists if consumers have had recent transitions of care or appointments, and may not capture medication organization systems. Although this can be a limitation of the current team approach, incorporating a systematic assessment of medication adherence and keeping track of each consumer’s follow-up appointments will address these concerns.
CMs often bring consumer cases to CMIT after a recent interaction, hospitalization, or transition of care. This may not coincide with the routine cadence of medical appointments. Many of the CMIT recommendations require follow-up visits with medical providers to further evaluate and treat acute or chronic illnesses. The medical complexity of many of the consumers requires close collaboration between PCP, specialists, and coordination by a CM. Although CMIT CMs support consumer activation to engage with medical providers, a higher level of coordination and follow-up is beyond the scope of the CMIT team itself without significantly increasing team members’ time commitment.
Limitations of This QI Data
The authors also faced an issue regarding missing follow-up data. Several reasons exist for the missing data including the CM did not follow up, the CM did follow up but was not able to get the information requested from the consumer, the consumer passed away, or they were discharged to a nursing facility. Furthermore, the AAA programs themselves experience high consumer turnover as consumers transition into and out of different insurance programs and become lost to follow-up. It is possible that those who were lost to follow-up represented the more severely ill, therefore skewing the data; however, absent dedicated research staff, retrieval of the data necessary to more definitively answer these questions was not within the scope of this QI project.
Outcome data were recorded simply as yes or no, as to whether the problem is still an issue at follow-up. This was meant to encourage completion of follow-up questionnaires by reducing respondent burden on CMs and to encourage at least some outcome data from nonmandatory questionnaires. The authors acknowledge the limitations of data collection in this manner, leading to incomplete follow-up and nonstandardized responses. Future projects should employ dedicated research staff to administer validated objective assessments and conduct chart reviews to improve the quality of outcome data. Expanded outcome measures should also be considered such as those in the CMS Measures Inventory Tool.
Although it is possible that CMs select cases in such a way as to distort the eventual outcomes (eg, easiest consumers, most compliant), the team’s experience is that cases are mainly selected after CMs have exhausted their known resources and thus may represent the more difficult consumers. The authors would expect such a population to be more difficult to impact positively.
Only a randomized trial would provide convincing proof of the causal benefit of CMIT. The authors continue to explore methods to gather objective data to support the model, although challenges remain. For example, CMs may not have follow-up visits before the 3- or 6-month outcome measures. Furthermore, outcomes were not always amenable to yes/no answers, which meant to decrease the reporting burden on the CMs. Ultimately, the lack of an integrated EHR places significant limitations on quantitative data collection accuracy. As part of this lack of integration, it is difficult to discern whether PCPs implemented the team recommendations. A more systematic approach to data collection by dedicated personnel would allow the required time for chart review and standardized consumer assessments to improve the ability to objectively capture outcomes.
Generalizability and Sustainability
With the support of the local AAA and the health system, CMIT has operated since 2004 with only minor changes. This longevity, as well as the numerous spin-off CMIT variations, speaks to the value CMIT brings to shared consumers from all involved institutions. CMIT can be easily adapted to any organization, as it requires minimal funding since health care providers attend one 1-hour meeting per week and AAA CMs rotate presenting cases at CMIT, so that they generally present 2–3 cases per year. Time for CMIT is always a consideration for most health professionals, so strong commitment from involved leadership from both the health system and the AAA is imperative and should include a formal Business Associate Agreement and, minimally, a memorandum of understanding that (1) elucidates the roles and responsibilities of each partner, (2) establishes a time commitment for implementation of the team, and (3) establishes procedures to end the team if either party decides to do so. The AAA should have 1 staff member who coordinates the CM presentations and compiles the team recommendations (usually a supervisor), and the health system should minimally provide consultation services by a geriatrician and pharmacist. Hospitals cannot afford to allow doctors and pharmacists to participate unless the project has a direct impact on increased revenues, cost savings, and/or quality. Thus, the argument must be made to each entity that the collaborative will positively impact the bottom line by, for example, creating savings in staff time due to streamlined communications and tasks, increased referrals, or decreased readmissions/emergency department (ED) visits as shown by these results. These arguments are stronger in health systems that also provide insurance products because potential revenue lost by decreased utilization can be more than compensated by lower insurance payments. Outcome measures reported in this QI analysis demonstrate concordance with Age-Friendly Health System’s best practices and the preservation of independent living. Although the authors do support the evaluation of additional objective parameters including ED utilization, readmission rates, or nursing home placement to maximize sustainability, ultimately, these partnerships will be vital for improving accountability, quality, and cost-effectiveness.
Because CMIT brings together a broad range of individuals and organizations, many of whom did not have a history of working together, strong leadership is required. Two major factors are critical to success: commitment and communication. The team needs to build a common language and support group decision making; making sure to keep all members informed about what is going on; enabling members to learn about each other’s concerns, values, and work; and enabling them to air disagreements. It is important that participants feel free to talk about what they think is and is not working. Furthermore, the parties involved must perceive a compelling need to work together and be willing to do so. In this case, each organization had a shared goal of helping consumers remain living independently in their homes but had different problems needing to be addressed to achieve that goal. Leadership realized that only by working together could they be successful.
The logistics of assembling an in-person team from multiple organizations could limit sustainability due to the time commitment for travel alone. For many years, the CMIT team met in person to review cases. In response to COVID-19, in 2020, the team transitioned to a virtual platform, which has been maintained. The benefits of virtual meetings allow increased flexibility to meet and increase the number of people able to attend the team meeting. This allowed an expansion of the diversity of team members (ie, primary care, probate court, health department, Alzheimer’s Association), as well as allowing an increased number of learners from regional education centers and the community.
This model has demonstrated flexibility to be used for a variety of populations and settings. For example, as the population of the AAA changed to include a younger disabled population, the CMIT model continued to be applicable. This model has also been used to identify and manage palliative care needs earlier in the disease process. 24 It has been implemented by a local FQHC in a low-English-proficiency population to address cultural barriers to care.16, 25 The model has also been adopted by the local Habitat for Humanity to enhance aging in place initiatives to include home improvements aimed at falls prevention. The authors have also expanded this model to an additional AAA to reach new geographic regions in the state. Finally, as part of our HRSA-funded GWEP grant, the authors have expanded the team members as part of our experiential educational offerings to include representatives from adult protective services, probate court, the local health department, the Alzheimer’s Association, addiction services providers, and more. 25
Summary
This article describes an innovative, but long-supported, care model that addresses the complex health care and social needs of community-dwelling older adults and how this model fits the Wagner Chronic Illness Care theoretical framework. Through ongoing support from the health care system and AAA leadership, the model described here is associated with improvements in mutual goals, including fall risk reduction, medication concerns, behavioral health, and health care utilization. Future efforts should address improved data collection, EHR integration between community-based organizations and health care providers, and greater integration of the team with primary care. Using a more rigorous experimental design will help to validate the positive benefits of the CMIT model. If positive benefits are replicated, this may lead to reimbursement policies that support this model of collaborative care.
Authors’ Contributions
J.D., S.F., M.H., B.C., J.M., and M.G.: Conceptualization, methodology, and writing—reviewing. S.H.: Conceptualization, methodology, and writing—original draft. D.K.: Methodology, data curation, and writing—reviewing. K.B.: Data curation. M.S.: Writing—reviewing and supervision.
Footnotes
Author Disclosure Statement
The authors declare that they have no relevant or material financial interests related to the work described in this article.
Funding Information
This project is supported by the HRSA of the U.S. Department of Health and Human Services (HHS) under grant number U1QHP53043 entitled Geriatric Workforce Enhancement Program. This information or content and conclusions are those of the author and should not be construed as the official position or policy of, nor should any endorsements be inferred by HRSA, HHS, or the US government.