
Abstract
The association between pediatric care coordination (PCC) and the prevalence of oral health problems (OHP) among children and youths in the United States was investigated. Using data from the 2022 to 23 National Survey of Children’s Health for participants ≤17 years, multivariable Poisson regression models were employed to estimate the association between effective PCC and OHP (the presence of ≥1 parent-reported case of dental caries, gum bleeding, or dental pain). The study estimated the population attributable risk (PAR) to quantify the proportion of potentially avoidable OHP with effective PCC. All models were weighted to account for the complex survey design and adjusted for sociodemographic, health insurance, and geographic covariates. The analytical sample comprised 56,287 participants, representing an estimated target population of 34 million children ≤17 years of age who needed PCC. After controlling for covariates, the difference in the prevalence of OHP between children who received effective PCC (13.1%) and those who did not (17.5%) was statistically significant (adjusted prevalence ratio: 1.33, 95% CI:1.22, 1.44). The PAR was 9.9%, indicating OHP was 9.9% more prevalent among children who lacked effective PCC. Not receiving needed effective PCC was associated with a greater burden of OHP among U.S. children and adolescents. This finding highlights the importance of intentional organization of health services among relevant stakeholders to support optimal oral health.
Keywords
Pediatric care coordination (PCC) has generated huge interest because of the burden of chronic conditions, the need for complex treatments, and the escalation of health care expenditure. 1 Chronic conditions among children have risen to an unprecedented level. About one in three children has a chronic condition, and conditions such as asthma and mental health disorders are among the leading chronic conditions before the age of 18. 2 Furthermore, oral health conditions, though often overlooked, are five times more common in children than asthma.3,4 When implemented in primary care, PCC can enhance access to oral health care and improve oral health for patients. 5 PCC across systems of care and care providers is crucial to keeping them healthy and pain-free. Additionally, when PCC is well-designed and delivered to a target population, outcomes for patients, providers, and payers improve. 6
PCC is a deliberate organization of children’s care across providers and settings to improve outcomes and efficiency. 6 The researchers conceptualize effective PCC in this study as ensuring that a child receives health services that are effectively organized and managed across health care providers, educational systems, and support services, characterized by timely communication between the involved stakeholders in delivering care. A multisystem perspective in PCC recognizes independent work among different groups, as well as the behaviors and mechanisms that carry it out.7,8 Ultimately, the goal is to improve the quality of care received. Chang and Tung (2024) reported that the value of care could be improved by enhancing health care coordination, and their study among an adult population showed that high care coordination was associated with decreased 30-day readmission, mortality rates, and the costs of heart failure. 9
Weaver and colleagues 7 adopted a multisystem perspective to develop a framework that maps the association among care coordination mechanisms, the coordination process, integrating conditions, and patient outcomes. The researchers described a multilevel framework and identified information sharing as the most pertinent indicator of successful care coordination, based on a review of 33 studies on care coordination. The framework comprised context—study characteristics and study population; coordinating mechanisms—use of a designated care coordinator; emergent integrating conditions—integrating conditions between groups; coordinating actions—information sharing; outcomes—process or clinical outcomes. The framework thus provides a conceptual model in this study, considering information sharing between health care providers, between health care providers and schools and obtaining help in coordinating care as crucial elements of PCC, which could impact oral health.
Studies have linked oral diseases with chronic diseases, supporting the calls for more integrated delivery of health services, 10 and this is reinforced given the greater oral health needs among children with special health care needs. 11 While the impact of care coordination on chronic diseases, by improving biological and psychological outcomes, has been demonstrated, 12 research examining its effect specifically on oral health among children in the United States is scarce. The researchers, therefore, investigated the association between effective PCC and oral health problems (OHPs) in the United States. The researchers hypothesize that the lack of effective PCC would significantly increase the prevalence of OHPs.
Methods
Data source
Data for this research were obtained from the 2022 to 2023 National Survey of Children’s Health (NSCH) accessed through the Child and Adolescent Health Measurement Initiative. 13 The survey conducted by the Maternal and Child Health Bureau within the Health Resources and Services Administration HRSA sampled children and adolescents aged 0–17 years across all 50 states and the District of Columbia. 14 One child was randomly selected per household, with interviews conducted online and via mail. The NSCH provides detailed information about children’s physical and mental health, health care access and quality, and broader social environments; the full methodology is reported elsewhere. 15
Conceptual framework
The study’s conceptual framework is adapted from Weaver and colleagues’ multilevel care coordination framework. 7 The context represents [the] need for care coordination (children needing care coordination was defined here by their need to see more than one health care provider 15 ); the coordination mechanisms in this study represent the receipt of needed help in care coordination; coordinating actions are the sharing of information among health care providers and between schools and health care providers; while the outcome is the presence or absence of at least one OHP. Given the limitations of the study’s data set, a variable measuring emergent integrating conditions (representing coordination between health care providers and dental providers) was not recorded; however, the researchers included the variable “dental visit” in the regression model to highlight the independent association between effective PCC and OHP. Refer to Figure 1.

Conceptual framework as adapted from Weaver and colleagues’ multilevel care coordination framework.
Dependent variable (outcome variable)
The dependent variable was the presence of ≥1 parent-reported OHP (dental cavities, gum bleeding, and toothaches) in response to the survey questions: “whether the child had bleeding gums in the past 12 months”; “whether the child had decayed teeth/cavities in the past 12 months,” and “whether the child had toothaches in the past 12 months.”
Independent variable (exposure variable)
The exposure variable was effective PCC, which was assessed among children who had visited a health provider within the last 12 months. The parents were asked: (1) “How satisfied were you with the communication between this child’s doctors and other health care providers?” (2) “Did anyone help you arrange or coordinate this child’s care among different doctors or services that this child uses?” and (3) “How satisfied were you with the health care provider’s communication with the school, childcare provider, or special education program?” Children were reported to have effective PCC if the parents reported that they were “Satisfied,” “Yes” and “Very satisfied” in response to these questions. Individuals who did not see multiple providers were considered not to need care coordination and were excluded.15–17 The survey questions are contained in the full-length NSCH survey instruments, which are part of the publicly available files used in this study and are also included in Supplementary Data. 18
Covariates
Demographic characteristics were collected via a questionnaire, encompassing the child’s age (0–5, 6–11, 12–17 years), biological sex (male or female), race/ethnicity, household education, insurance, region (Northeast, Midwest, South, and West), and family income. Race was categorized as Hispanic; non-Hispanic (NH) White; NH Black, and NH Other (including Asian, American Indian or Alaska Native, Native Hawaiian and other Pacific Islander, and multi-race) (The Child & Adolescent Measurement Initiative, 2025). Household education was categorized < high school, high school/GED, some college/technical school, or college degree or higher. Insurance was classified in this study as either adequate (if it met the child’s health care needs, allowed access to needed providers, and incurred no unreasonable out-of-pocket costs) or inadequate. Family income was expressed as a percentage of the U.S. Census Bureau’s family poverty threshold (<100%, 100%–199%, 200%–399%, and >400%). 19 Children with Special Health Care Needs (CSHCN) were identified based on the CSHCN screener- a five-item parent-reported tool established by the Federal Maternal and Child Health Bureau. 20 This screener identified children with at least one of five health consequences, including physical, mental, behavioral, or health conditions lasting 12 months or more. It flags conditions needing prescription, more-than-usual service utilization, specialized care, mental health counseling, and functional limitations. The presence of ≥1 other medical conditions was determined from a yes/no question to a list of 24 conditions, including allergies, autoimmune, cystic fibrosis, diabetes, Down syndrome, fetal alcohol spectrum disorder, heart conditions, frequent or severe headaches, frequent or severe headaches including migraines, Tourette syndrome, anxiety syndrome, depression, behavioral conduct problems, developmental delay, intellectual disability, speech or other language disorder, learning disability, autism spectrum disorder, ADHD, hearing problems, and vision problems.
Statistical analysis
The study’s final analytical sample (n = 56,287) was determined using listwise deletion; a case was dropped if it had a missing value in at least one variable (9%). Demographics, OHP, ≥1 medical conditions, and effective PCC among the participants were summarized using descriptive statistics.
Bivariate analyses (chi-square tests) examined the associations between effective PCC, covariates, and the outcome variables (at least one OHP). Multivariable Poisson regression models estimated the unadjusted and adjusted prevalence ratios for associations with effective PCC. Subgroup analyses were also performed based on whether the children received both medical and dental care in the past 12 months, using the same covariates. The researchers then calculated the population attributable risk (PAR) to determine the proportion of oral problems that could potentially be averted through the receipt of the needed care coordination.
21
Where PAF, population attributable fraction; PR, population ratio (adjusted for covariates), and Pe, proportion of total population exposed (i.e., proportion of the entire population not receiving the needed effective PCC).
All analyses conducted in this study incorporated sampling weights derived from the survey design, thus providing nationally representative estimates. The weighting accounted for the complex survey design and included a base weight with adjustments for factors such as households having multiple telephone numbers and survey nonresponse. The significance level was set at P < 0.05, and all analyses were conducted using Stata version 18.0 (StataCorp, College Station, TX).
Results
Characteristics of the study population
The study comprised 56,734 participants, representing an estimated 34,654,917 children aged 0–17 years. Notably, 14.8% (95% CI:14.2,15.4) of the children had OHP, while an assessment of receipt of effective PCC revealed that 33.4% (95% CI: 32.6, 34.2) did not receive the needed effective PCC. Having OHP was greater among children who lacked effective PCC (P < 0.001), ≥1 medical condition (P < 0.001), belonged to households with income <99% Federal Poverty Level (FPL) versus >400%FPL, (P < 0.001), from households with educational level less than high school degrees versus college or higher degrees (P < 0.001), CSHCN compared to non-CSHCN (P < 0.001) (Refer to Tables 1 and 2 for more details of the results of the descriptive analyses).
Characteristics of Children Who Needed Care Coordination Aged 0–17 Years in the United States, National Survey of Child Health 2022–2023
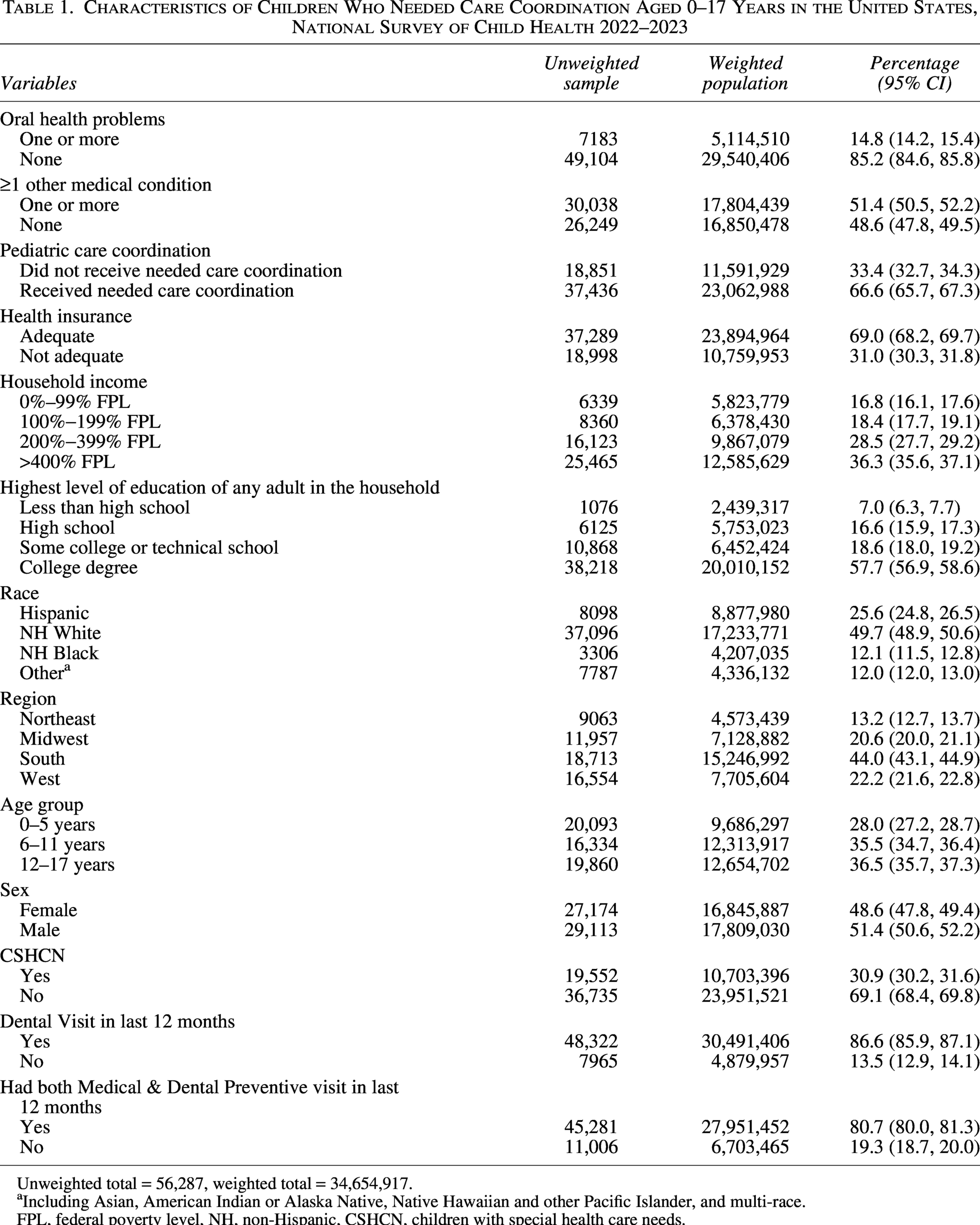
Unweighted total = 56,287, weighted total = 34,654,917.
Including Asian, American Indian or Alaska Native, Native Hawaiian and other Pacific Islander, and multi-race.
FPL, federal poverty level, NH, non-Hispanic, CSHCN, children with special health care needs.
Bivariate Analysis of the Association Between Independent Variables and Covariates and ≥1 Oral Health Problem, National Survey of Child Health 2022–2023
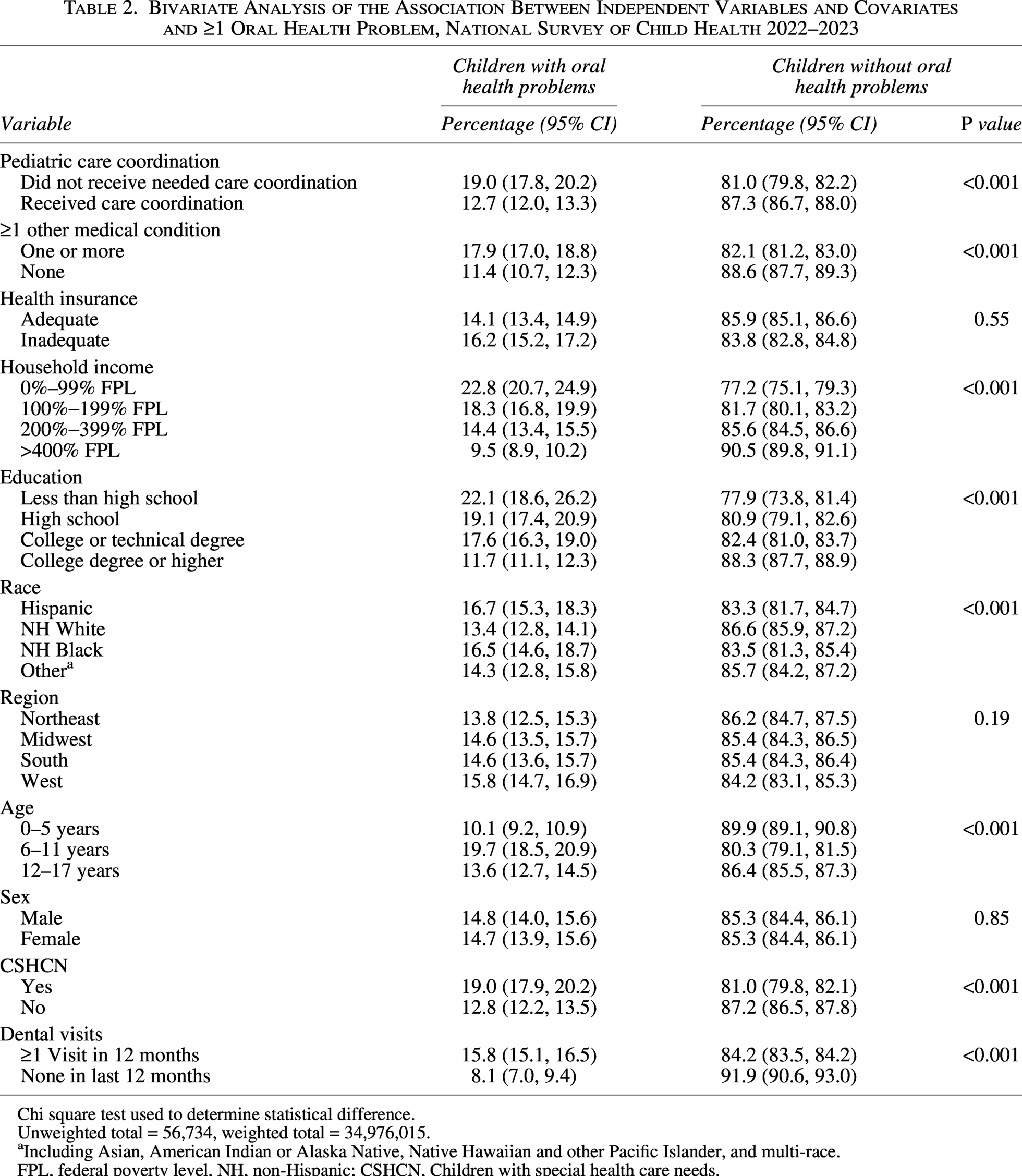
Chi square test used to determine statistical difference.
Unweighted total = 56,734, weighted total = 34,976,015.
Including Asian, American Indian or Alaska Native, Native Hawaiian and other Pacific Islander, and multi-race.
FPL, federal poverty level, NH, non-Hispanic; CSHCN, Children with special health care needs.
Multivariable regression
The unadjusted prevalence of OHP was higher among children who lacked the needed effective PCC (18.9% vs. 12.6%; prevalence ratio 1.49; 95% CI, 1.38–1.62). After controlling for the covariates, the difference in the prevalence of OHP among children lacking the needed effective PCC (17.5%) compared with those who reported receiving effective PCC (13.1%) was attenuated but remained statistically significant (adjusted prevalence ratio [aPR], 1.33, 95% CI, 1.22–1.44). Subgroup analyses revealed significant (aPR, 1.28, 95% CI, 1.17, 1.40) when children had both preventive medical and dental visits, and when participants had no preventive medical and dental visit in the past year ([aPR], 1.59, 95% CI, 1.28, 1.96).
Covariates significantly associated with an increased prevalence of OHP were the presence of ≥1 other medical condition, age groups, dental visits, household income (>400% FPL vs. 0%–99% FPL), and the highest education level in the household (having a college or higher degree vs less than high school education) (P < 0.001) (Refer to Tables 3 and 4).
Predictors of ≥1 Oral Health Problem, National Survey of Child Health 2022–2023
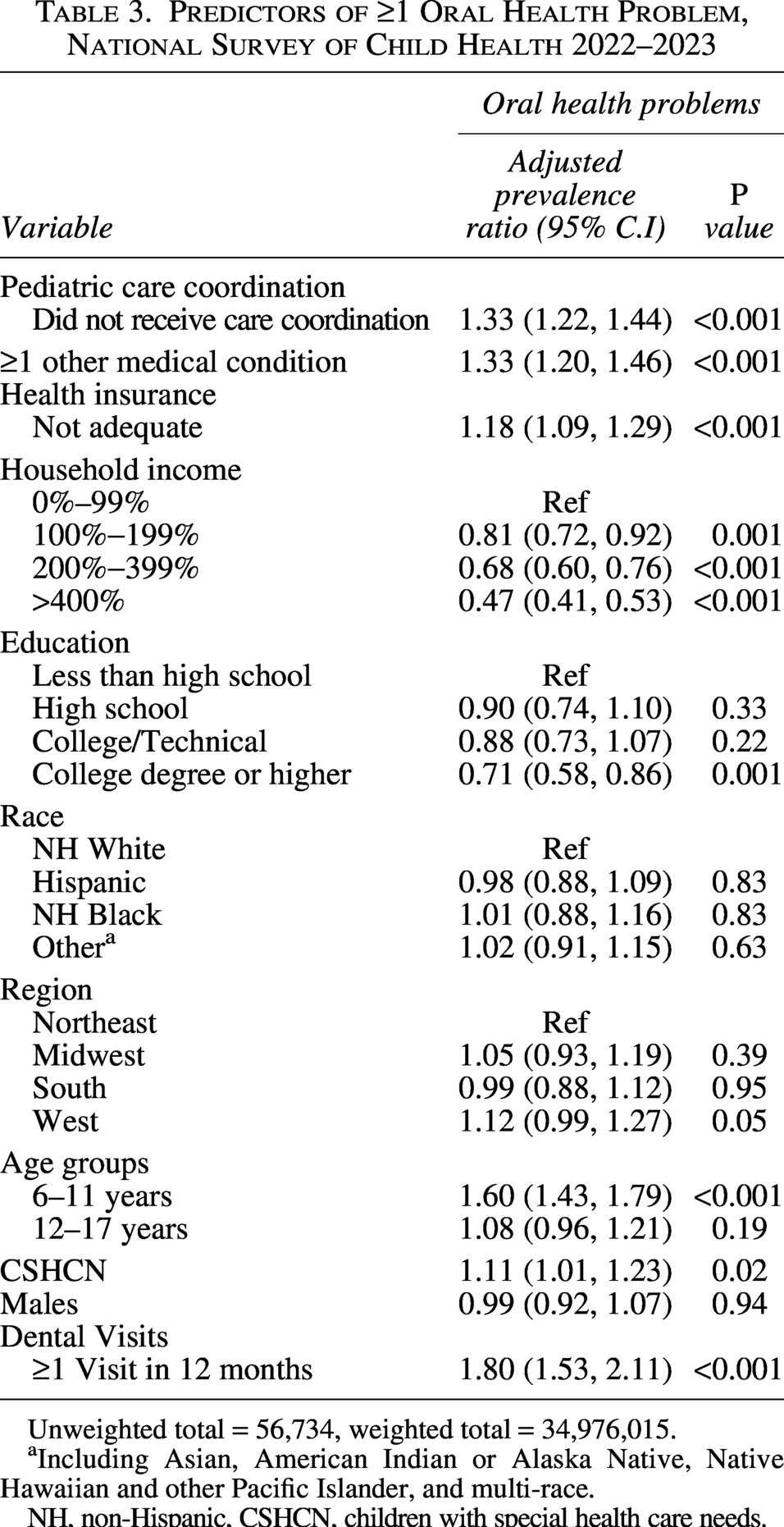
Unweighted total = 56,734, weighted total = 34,976,015.
Including Asian, American Indian or Alaska Native, Native Hawaiian and other Pacific Islander, and multi-race.
NH, non-Hispanic, CSHCN, children with special health care needs.
Association Between Pediatric Care Coordination, and the Prevalence of ≥1 Oral Health Problem, National Survey of Child Health 2022–2023
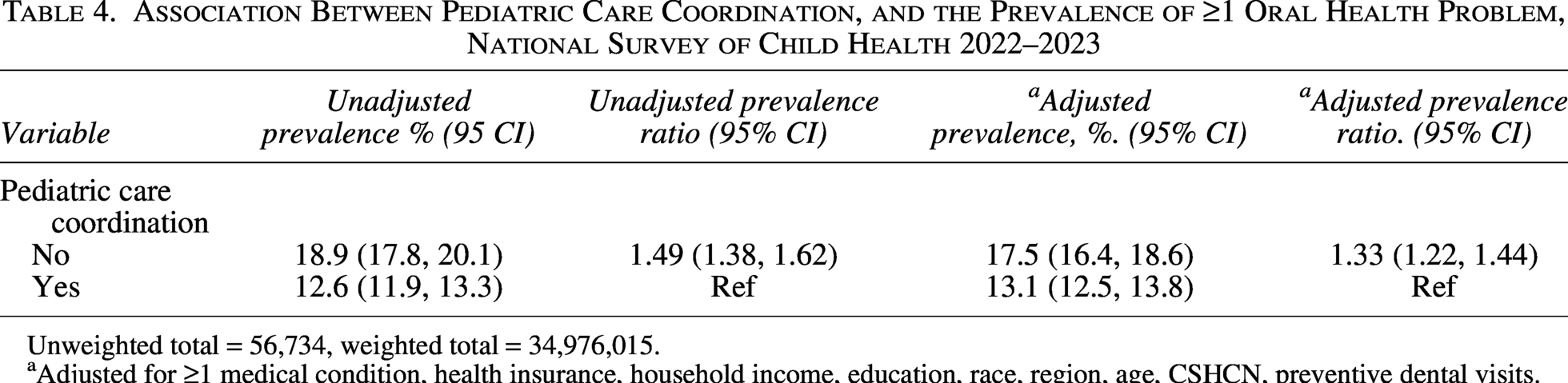
Unweighted total = 56,734, weighted total = 34,976,015.
Adjusted for ≥1 medical condition, health insurance, household income, education, race, region, age, CSHCN, preventive dental visits.
Population attributable risk
The PAR was 9.9%, representing an estimated 464,540 cases of OHP among children needing PCC that were associated with the lack of receipt of effective PCC. To estimate the potential economic impact of effective PCC, the researchers applied national data on pediatric dental expenditures from the Medical Expenditure Panel Survey. The mean annual dental expenditure among U.S. children aged 2–17 years with at least one dental visit was $721 in 2021, U.S. 22 This amount represents the average annual direct cost of dental care for children who use dental services and was selected as a conservative proxy for the cost associated with having an OHP, as defined in the NSCH. Applying this per-case cost to the estimated 464,540 cases derived from the PAR yields an estimated $334.9 million in direct dental costs associated with the lack of receipt of universally provided effective PCC to children who need it. Additionally, assuming a marginal change (e.g., 5% or 10%) in dental visits per annum owing to increased effective PCC, and applying the conservative estimate of 464,540 cases, would yield an estimated $16.7 million or $33.4 million in direct costs, which is still lower than the attributable costs associated with the lack of effective PCC.
Discussion
This study extends the evidence on the impact of not receiving effective PCC on oral health, using the NSCH 2022–2023 data, a nationwide survey conducted in the United States. The analysis shows a significant association between not receiving effective PCC and the presence of at least one OHP. Notably, the findings demonstrate the importance of optimizing patient oral health through continuity of care and increased investment in effective PCC, thereby providing a proxy indicator for other health problems that may not be adequately addressed when effective PCC is lacking. In this study, effective PCC is approached as a distinct construct that focuses on information sharing among care providers and with schools, as well as receiving assistance with coordinating care. These elements play a crucial role in delivering cohesive care, especially for persons with multiple medical conditions.6,23
The study builds on previous research that highlighted prevalent unmet needs for care coordination 24 by extending the research to the oral health implications of not receiving effective PCC. The current study’s finding that a lack of effective PCC was significantly associated with the presence of at least one OHP in children is consistent with existing literature on improving access to care through care coordination. 25 Recognizing care coordination is often embedded within the broader framework of medical home operations, the study findings align with previous studies that reported lower adjusted odds for fair or poor oral health among children in these homes after accounting for special health care needs. 26 Worse oral health has been reported among individuals with special health needs, largely due to access barriers such as the lack of a medical home. 11 While these previous studies explore broader associations between oral health and medical home (and, by extension, care coordination), the current study establishes a more direct link between oral health and effective PCC. Communication and collaboration between diverse health care providers, the patient, and the patient’s family are critical for better health outcomes. Even though it is quite ambiguous and challenging to measure, the impact of collaboration between health care organizations and non-health organizations can improve population health. Effective PCC, which includes sharing information between health care providers and organizations like schools, as measured in this study, was strongly associated with the oral health of children in the United States.
The current study’s findings align with Weaver and colleagues’ multilevel care coordination framework, 7 which explicates the coordinating mechanisms and actions in the context of care coordination needs among children, influencing oral health outcomes. Although the current study lacked information on emerging integrating conditions, because the NSCH full-length survey instruments did not gather explicit information about care coordination between the health care provider and a dental provider, notably, the regression model controlled for dental visits made by the participants. In the model, a greater number of dental visits was significantly associated with OHP. This finding may be counterintuitive; however, children with more pre-existing OHP are more likely to seek dental care, and those without problems may have fewer visits. By controlling for dental visits, the researchers have evaluated the effect of effective PCC among children with similar levels of dental service utilization. Furthermore, even among frequent dental attenders, a lack of effective PCC independently influenced OHP, and this is critical for quality care.
The study reports a substantial PAR of 9.9%, implying OHP was 9.9% more prevalent among children lacking effective PCC. Policy efforts that prioritize investment in effective PCC for children facing social risk factors and those with special health care needs and reimbursement mechanisms that support effective PCC for underserved or other at-risk populations are essential. 27 Strengthening cross-sector collaborations between medical and dental professionals, integrating oral health care into primary care and pediatric care, and enhancing communication between providers while closing referral loops through information technology will be crucial for delivering comprehensive care.25,28 Additionally, restructuring of interprofessional training to foster collaboration and continuity of care across medical and dental settings will be essential. 29
Interprofessional collaboration and integration may also be enhanced through formal referral networks, including dental professionals in a structured referral pathway. PCC may also be incentivized if payment models reward health care providers for following up on clients’ overall health outcomes across medical and dental settings.
This study is not without limitations. The researchers acknowledge that different health systems may interpret these results through entirely different implementation lenses, which may limit the generalizability of the findings. As a cross-sectional study, the current study cannot establish causality; however, given the use of a nationally representative data set with weighted estimates and robust analysis, the researchers have significantly enhanced the validity of these findings. The study utilized a risk-based measure of effect size, namely prevalence ratios, rather than odds ratios, because the outcome in this study had a prevalence greater than 10%. 30 The utilization of prevalence ratios offers a more conservative estimate of the association between effective PCC and OHP. 30 The study estimated the PAR, which may represent the proportion of cases that may be averted if effective PCC were implemented; however, the cross-sectional nature of this study limits this causal interpretation. The observed PAR, therefore, reflects an associational rather than a causal measure of the population impact of effective PCC. Self-reporting of specific measures may introduce some bias; nevertheless, studies also provide evidence of the strength and consistency of self-reported measures, especially when using multi-item questionnaires rather than single-item measures. 31 The results of this study highlight the importance of avoiding the Table 2 fallacy, as the Poisson model was designed to estimate the effect of effective PCC on OHP while adjusting for confounders. Accordingly, the coefficients of these confounders represent adjusted effects and therefore not total effects on OHP since the primary exposure variable, effective PCC, was held constant in these estimates. 32 Finally, the researchers note the possibility that missing data may create bias in the study findings, given the amount of missing data among cases in the study sample (9%), and thus ran a sensitivity analysis via multiple imputation by chained equation, assuming the data were missing at random. Multiple-imputation estimates for the regression table are provided as a Supplementary Data. Comparing the confidence intervals of the multiple-imputation estimates for the weighted Poisson models with those of the weighted Poisson models revealed overlap, indicating no statistically significant difference between the two estimates.
Conclusion
The findings of this study highlight a strong association between the lack of receipt of parent-perceived coordination support and the presence of OHP. Almost one in five children who did not receive the needed effective PCC had at least one OHP. The study findings draw attention to the importance of investing in and strengthening cross-sector collaboration to provide improved quality of care and optimal oral health among children in the United States. While other unmeasured variables may shape oral health, the study draws attention to the effect of deliberate organization and planning of health care on the oral health of children in the United States.
Authors’ Contributions
M.I.A. conceptualized and designed the study, drafted the initial article, conducted the initial analysis, and critically reviewed and revised the article. T.D. and O.A. appraised the data collection instruments, conducted initial analyses, and critically reviewed and revised the article for its important intellectual content. V.G. and M.A.A. critically reviewed and revised the article. B.W. conceptualized and designed the study, coordinated and supervised data collection, and critically reviewed and revised the article.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.