
Abstract
This study examines the relationship between continuity of care with a family doctor and the usual place of care for minor health problems among Canadian seniors, with a focus on differences between immigrants and the native-born. Data come from the Canadian Health Survey on Seniors (n = 40,848). The outcome identifies respondents’ usual source of immediate care for minor problems: a doctor’s office, hospital outpatient/community clinic/walk-in clinic, emergency department (ED), or another location. Multinomial logistic regression models estimate associations between continuity of care—measured as duration of attachment to a family doctor—and place of care, with and without interaction terms between continuity and immigrant status, adjusting for demographic, socioeconomic, health, and access-related factors. Seniors attached to a regular family doctor for more than 2 years are significantly less likely to rely on the ED as their usual source of care (OR = 0.89, P < 0.05). Immigrants are also less likely than native-born seniors to use the ED (OR = 0.69, P < 0.001). However, interaction models show that immigrants with short-term attachment (less than 1 year) have higher odds of ED use than native-born seniors with similar attachment (OR = 2.33, P = 0.031). Poor self-rated health, lower income, and access barriers are associated with greater ED reliance. These findings highlight the importance of sustained primary care relationships, particularly for newly attached and immigrant seniors, to reduce avoidable ED use and promote equitable access to community-based care in Canada.
Older adults often use emergency departments (EDs) or their family physicians for nonurgent medical conditions, creating inefficiencies in the health care system and highlighting opportunities for targeted interventions. Empirical evidence suggests that attachment to a family physician provides multiple benefits through continuity of care. Such attachment has been associated with improved health outcomes and quality of life,1–3 reduced overuse of medical procedures,4,5 lower specialty care utilization,6,7 and decreased health system costs.8,9 Moreover, continuity of care has been shown to reduce hospitalization and ED visits for less-urgent conditions.10–12
Despite these benefits, older adults continue to have disproportionately high rates of ED use for nonurgent issues, often reflecting gaps in access to primary care. A 2022 position statement by the Canadian Association of Emergency Physicians reported that adults aged 65 and over accounted for between 20% and 40% of all ED visits, depending on location, and this proportion is expected to rise in the coming years. 13 Among older adults, immigrant seniors are particularly likely to depend on EDs for primary care–appropriate concerns, due to challenges such as language barriers, cultural differences in health beliefs, unfamiliarity with the health care system, and difficulty securing a regular family physician.14–16 These barriers can hinder the development of ongoing primary care relationships, resulting in fragmented care, delayed management of chronic conditions, and poorer health outcomes.
The economic implications of unnecessary ED visits are substantial. A 2024 report by the Montreal Economic Institute estimated that Canadian EDs handled more than 960,000 visits in 2022/2023 that could have been managed in primary care settings, adding approximately $145 million in avoidable costs nationwide. 17 Beyond financial pressures, excessive ED demand strains staff, increases wait times, and reduces the efficiency of emergency care delivery. 18 Strengthening access to continuous, person-centered primary care—particularly for older immigrants—thus represents a key strategy to improve outcomes while alleviating system pressures.
However, persistent linguistic, cultural, and systemic barriers may prevent older immigrants from establishing long-term relationships with family physicians, limiting their ability to benefit from the continuity of care observed among Canadian-born seniors. Few studies have explored whether the advantages of continuous primary care differ by immigrant status, leaving an important gap in understanding equity in health care utilization. Using nationally representative data, this study examines whether immigrant status modifies the association between long-term attachment to a family physician and the place of care for minor health problems among adults aged 65 and older. By integrating immigrant status and continuity of care within a single analytical framework, this study aims to provide evidence to inform health system planning and promote equitable access to primary care while reducing unnecessary ED use.
Methods
The analysis uses the 2019/2020 Canadian Health Survey on Seniors (CHSS) combined file, which pools two annual cross-sectional samples to represent the average population aged 65 and older over the 2-year period. The CHSS is a focus content survey conducted as a supplement to the Canadian Community Health Survey (CCHS). Administered by Statistics Canada, the CHSS collects information on health status, health care use, and social determinants of health among Canadians aged 65 and older. Data collection for the 2020 cycle was disrupted by the COVID-19 pandemic, with a pause in March 2020 and resumption in September 2020 using telephone-only interviews and shortened collection periods. Survey weights were adjusted by Statistics Canada to account for nonresponse and potential bias.
The CHSS employed a stratified multistage sampling design based on the CCHS dwelling frame, ensuring representativeness by province, age, and sex. Within each selected household, one eligible senior was randomly chosen. Of the 45,863 individuals identified as eligible for the CHSS, 41,635 completed the survey, yielding a response rate of 90.8%. Statistics Canada’s follow-up procedures (e.g., reminder letters and phone calls) minimized nonresponse bias. The analysis used deidentified, publicly available CHSS data. As there was no direct contact with participants, the study met institutional requirements for research using secondary data and did not require additional ethics review.
The dependent variable, usual place of care for minor or immediate health problems, was categorized as (1) doctor’s office, (2) hospital-based outpatient setting (including community health centers and walk-in clinics), (3) hospital ED, and (4) not stated (retained for data completeness but not interpreted due to heterogeneity). Minor or nonurgent health problems were defined as non-life-threatening issues such as fever, vomiting, headaches, sprains, minor burns, rashes, or similar conditions resulting from accidents or injuries. The dependent variable is based on a CHSS question that asks where individuals would typically seek care in such situations. The question is framed hypothetically and includes examples of minor conditions to guide interpretation (see Appendix A for all variables used in the analysis).
A multinomial logistic regression model was used to assess the association between continuity of care with a family physician and the reported place of care for minor problems among immigrants and native-born individuals. The primary variables of interest are (1) whether a respondent is an immigrant (reference: being native-born) and (2) the length of continuity of care with a family doctor, grouped into the following categories: (a) less than 1 year; (b) 1 to less than 2 years; (c) 2 years or more; and (d) not stated. The reference group comprised respondents without a regular family doctor. Finally, the model also includes interaction terms between the immigrant dummy and the length of duration of care dummies. These interaction terms indicate whether the association between length of attachment to a family physician and the likelihood of choosing each place of care differs between immigrants and nonimmigrants.
Additional covariates included demographic, socioeconomic, and health-related factors. These include sex (male, with female as the reference), marital status (single/widowed/divorced/separated/never married, with married/common-law as the reference), education (less than postsecondary, with postsecondary or higher as the reference), household income (≥$60,000, with <$60,000 as the reference), and province (with Ontario as the reference).
Health-related variables included self-perceived health (categorized as excellent/very good or good/fair, with poor as the reference) and reported barriers to accessing care (including lack of provider availability in the area, no providers accepting new patients, or provider retirement/departure). These variables are included as covariates in the regression model to account for individual differences in health status and access to care. The final sample comprised 40,848 respondents, and all statistical analyses were conducted using Stata.
Results
Results from Table 1 suggest that among seniors aged 65 and older, longer continuity with a family doctor is associated with greater reliance on primary care for minor problems. Those with two or more years of attachment are more likely to use a doctor’s office (65.7%) compared with those with shorter attachment (<1 year: 57.5%; 1–2 years: 57.6%) or no regular doctor (59.3%). Also, immigrant seniors are more likely than native-born seniors to report a doctor’s office as their usual place of care (67.8% vs. 59.6%) and less likely to use hospital outpatient clinics (17.4% vs. 22.1%) or the ED (5.9% vs. 8.8%), suggesting that immigrants either maintain stronger primary care engagement or face barriers to hospital-based services.
Usual Care Source for Minor Problems Among Seniors: Sample Characteristics
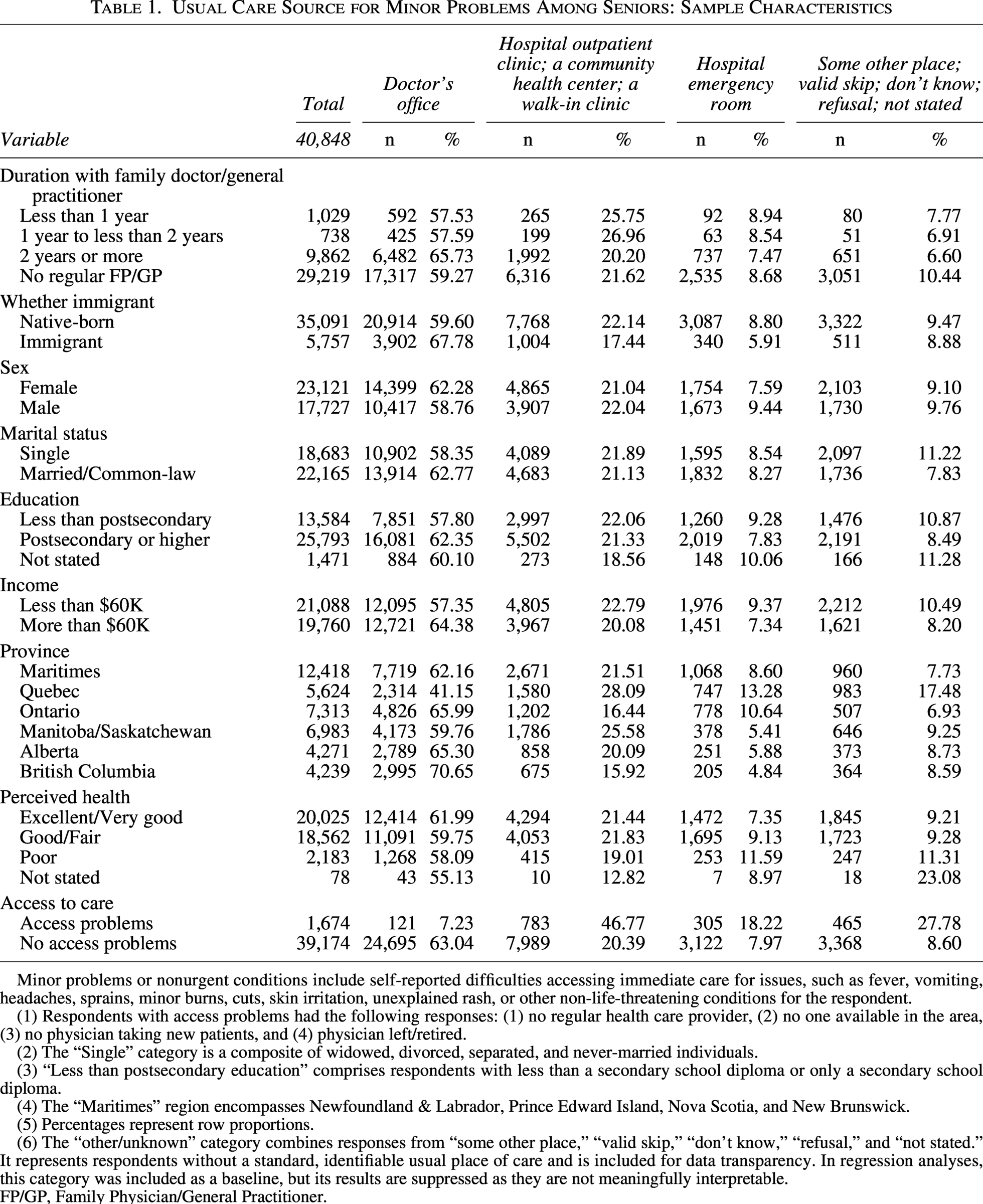
Minor problems or nonurgent conditions include self-reported difficulties accessing immediate care for issues, such as fever, vomiting, headaches, sprains, minor burns, cuts, skin irritation, unexplained rash, or other non-life-threatening conditions for the respondent.
(1) Respondents with access problems had the following responses: (1) no regular health care provider, (2) no one available in the area, (3) no physician taking new patients, and (4) physician left/retired.
(2) The “Single” category is a composite of widowed, divorced, separated, and never-married individuals.
(3) “Less than postsecondary education” comprises respondents with less than a secondary school diploma or only a secondary school diploma.
(4) The “Maritimes” region encompasses Newfoundland & Labrador, Prince Edward Island, Nova Scotia, and New Brunswick.
(5) Percentages represent row proportions.
(6) The “other/unknown” category combines responses from “some other place,” “valid skip,” “don’t know,” “refusal,” and “not stated.” It represents respondents without a standard, identifiable usual place of care and is included for data transparency. In regression analyses, this category was included as a baseline, but its results are suppressed as they are not meaningfully interpretable.
FP/GP, Family Physician/General Practitioner.
Primary care utilization varies by sex, marital status, education, and income. Females and married/common-law seniors are more likely to use a doctor’s office, whereas males and single seniors have higher ED use. Higher education and higher income are similarly associated with a greater reliance on primary care and lower use of hospital-based services, consistent with differences in health literacy, access to resources, and health care navigation.
In addition, the table suggests that seniors reporting excellent or very good health are more likely to use a doctor’s office and less likely to use emergency services, whereas poorer health is associated with higher ED use. Individuals experiencing access problems are significantly less likely to utilize primary care and more likely to rely on hospital outpatient clinics or other non-primary care settings. Regional variations are also notable, with Quebec seniors exhibiting higher hospital-based use and lower use of doctors’ offices, while British Columbia and Ontario seniors predominantly use primary care offices, highlighting differences in health care system structure and accessibility across provinces.
Table 2 presents the results from a multinomial logistic regression model examining the association between continuity of care and the usual place of immediate care for minor health problems. The reference category for the usual place of care for minor problems is at the doctor’s office. In this model without interaction terms, immigrants are significantly less likely than native-born respondents to report the ED as their usual place of care for minor problems [odds ratio (OR) = exp (−0.368) = 0.69, P < 0.001], indicating lower reliance on hospital-based services overall. Among all respondents, only those with long-term continuity of care—being attached to a regular family doctor for more than 2 years—had significantly lower odds of using the ED (OR = 0.89, P = 0.018) compared with those without a regular doctor. In contrast, respondents with shorter durations of attachment (less than 1 year or 1 to 2 years) did not differ significantly from those without a regular doctor. These results suggest that the benefits of continuity of care in reducing ED use become evident only after a stable relationship with a primary care provider has been established. The findings also indicate that, on average and regardless of continuity length, immigrants are less likely to substitute emergency care for primary care than the native-born population, which may reflect differences in health-seeking behavior, familiarity with the health care system, or access barriers.
Regression Results Between Place of Care of Minor Problems and Duration of Care with Family Physician, Immigrants, and Native-Born (No Interaction Terms)
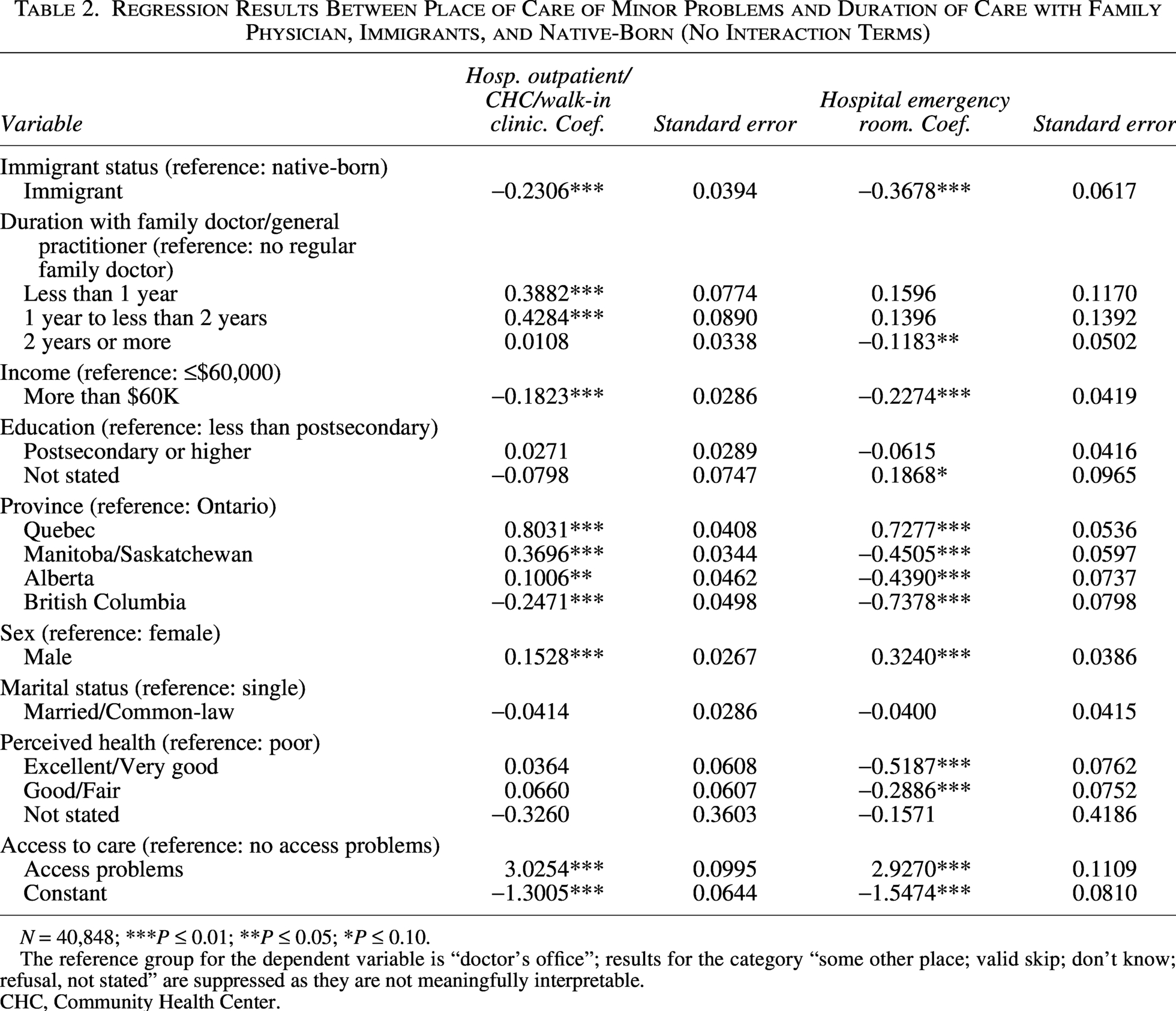
N = 40,848; ***P ≤ 0.01; **P ≤ 0.05; *P ≤ 0.10.
The reference group for the dependent variable is “doctor’s office”; results for the category “some other place; valid skip; don’t know; refusal, not stated” are suppressed as they are not meaningfully interpretable.
CHC, Community Health Center.
When interaction terms between immigrant status and continuity of care are included in Table 3, the main negative effect for immigrant status remains (OR = 0.65, P < 0.001), confirming that immigrants are overall less likely to use the ED than native-born respondents. However, a significant positive interaction between immigrant status and short-term continuity (<1 year) (OR = 2.33, P = 0.031) indicates that immigrants who are newly attached to a family doctor are more likely to report the ED as their usual place of care than native-born respondents with similar attachment. This suggests that, among immigrants, recent attachment to a doctor may initially coincide with continued reliance on emergency services, possibly reflecting transitional barriers, limited familiarity with primary care pathways, or unmet expectations of accessibility. No significant interactions are observed for longer durations of continuity, implying that the positive effect of long-term attachment operates similarly across groups. Overall, adding the interaction terms reveals important within-group variation among immigrants that is masked in Table 2, highlighting that while immigrants generally use EDs less often, the moderating role of continuity of care depends on how long they have been integrated into the primary care system.
Regression Results Between Place of Care of Minor Problems and Duration of Care with Family Physician, Immigrants, and Native-Born (With Interaction Terms)
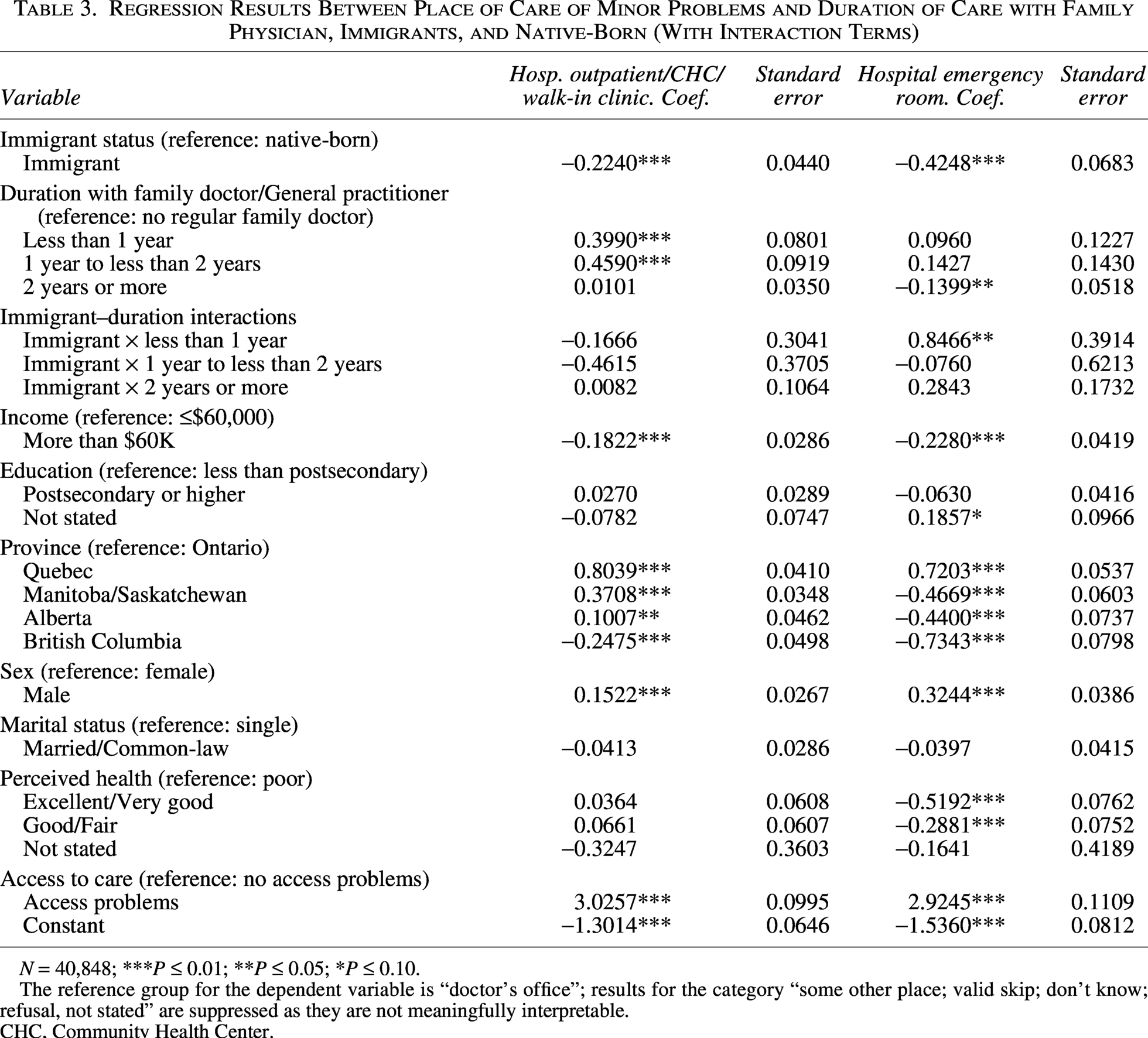
N = 40,848; ***P ≤ 0.01; **P ≤ 0.05; *P ≤ 0.10.
The reference group for the dependent variable is “doctor’s office”; results for the category “some other place; valid skip; don’t know; refusal, not stated” are suppressed as they are not meaningfully interpretable.
CHC, Community Health Center.
Other variables in Table 3 provide some interesting insights. Seniors reporting poorer self-rated health have higher odds of identifying the ED as their usual source of care, underscoring the link between declining health and reliance on hospital-based services for minor problems. Those who experience access problems—such as difficulty obtaining appointments or reaching a doctor—are substantially more likely to use the ED rather than a physician’s office, suggesting that perceived barriers in primary care directly contribute to emergency service utilization. Furthermore, seniors with lower household income are more likely to report using nonoffice settings (such as EDs, hospital outpatient, or walk-in clinics), while marital status is not a significant predictor after adjusting for other factors.
As well, the results reflect substantial variation in care-seeking patterns across provinces. For example, seniors in Quebec are more likely to rely on hospital-based settings, including EDs and outpatient clinics, whereas those in provinces such as British Columbia more often report physician offices as their usual source of care. These differences likely reflect variation in the organization and accessibility of provincial health care systems, including differences in primary care attachment models, availability of walk-in clinics and community health centers, and referral pathways. More broadly, these patterns may capture underlying system-level factors such as physician supply, appointment availability, and the degree of integration within primary care, which can influence reliance on community-based versus hospital-based care. Rurality and geographic dispersion may also contribute to these differences. Overall, the findings point to persistent structural and geographic disparities in how seniors navigate care for minor health problems, even after accounting for continuity of care and immigrant status.
Discussion
This study examined the association between continuity of care with a family doctor and the usual place of care for minor health problems among seniors, with a particular focus on differences between immigrants and native-born individuals. Descriptive analyses indicated that seniors with longer attachment to a family doctor are more likely to use primary care offices and less likely to rely on hospital-based services, including EDs. Immigrants are more likely than native-born seniors to report a doctor’s office as their usual place of care, suggesting higher engagement with primary care or potential barriers to accessing hospital-based services. Regression analyses further confirm these patterns: In models without interaction terms, longer continuity of care is associated with reduced odds of ED use, and immigrants overall had lower odds of relying on the ED compared with native-born seniors.
The introduction of interaction terms between immigrant status and continuity of care reveals nuanced heterogeneity. While immigrants generally used the ED less than native-born seniors, those with only short-term attachment (<1 year) to a family doctor have higher odds of reporting the ED as their usual place of care, suggesting that the beneficial effect of continuity may accrue more slowly for this population. Longer-term attachment, by contrast, reduces ED use for both groups. These findings highlight the importance of considering not only whether seniors are attached to a primary care provider but also the duration and stability of that relationship, particularly for immigrant populations who may face additional barriers or require time to establish trust in the health care system.
Several limitations should be considered. First, the data collection overlaps with the COVID-19 pandemic, which may have altered health-care-seeking behavior, including reduced use of hospital-based services and disruptions to access and continuity of primary care. These changes may have differentially affected individuals based on their attachment to a family physician and familiarity with the health care system, particularly among immigrants. As a result, the estimated associations between duration with a family physician, immigrant status, and place of care should be interpreted with caution; however, to the extent that the pandemic exacerbated existing disparities in access and continuity, the observed relationships may be strengthened rather than driven by this period. Second, the data are cross-sectional, preventing causal inference; it is not possible to determine whether continuity of care reduces ED use or whether healthier or more proactive seniors are both more likely to maintain a family doctor and less likely to use the ED. Third, the study relies on self-reported measures of usual place of care, which may be subject to recall bias. Fourth, the immigrant variable does not distinguish by country of origin, length of time in Canada, or language proficiency, which may influence health-care-seeking behaviors. Finally, while the models adjust for sociodemographic and health-related factors, unmeasured confounders, such as cultural preferences, prior health care experiences, or local availability of primary care services, could influence results.
Despite these limitations, the study provides important evidence that both continuity of care and immigrant status are key determinants of health care utilization patterns among seniors and that newly attached immigrants may continue to rely on ED services until a stable primary care relationship is established. Policies aimed at facilitating early access to and sustained engagement with primary care for immigrants could help reduce unnecessary ED use and improve the efficiency of health care delivery for aging populations.
Conclusion
This study highlights the critical role of continuity of care and immigrant status in shaping where seniors seek care for minor health problems. Seniors with a long-standing relationship with a family doctor are less likely to rely on EDs, underscoring the favorable effect of stable primary care attachment. While immigrants overall are less likely than native-born seniors to report the ED as their usual place of care, those with only recent attachment to a physician remain more dependent on emergency services. These findings suggest that the benefits of continuity of care may take time to materialize for immigrant populations, emphasizing the importance of early, proactive engagement with primary care following attachment. Persistent socioeconomic and regional disparities further indicate that access to and organization of primary care continue to influence utilization patterns among older adults. Strengthening continuity of care—particularly during the early stages of patient attachment and among immigrant seniors—may help reduce unnecessary ED use and support more equitable access to appropriate, community-based care.
Footnotes
Author’s Contributions
The author was responsible for research, writing, and statistical analyses.
Ethics Approval
All data are encrypted and publicly available, so no ethics approval was required.
Availability of Data and Material
The data are publicly available from the Statistics Canada website.
Code Availability
The code is available upon request.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Appendix A
Variables Used for Analysis
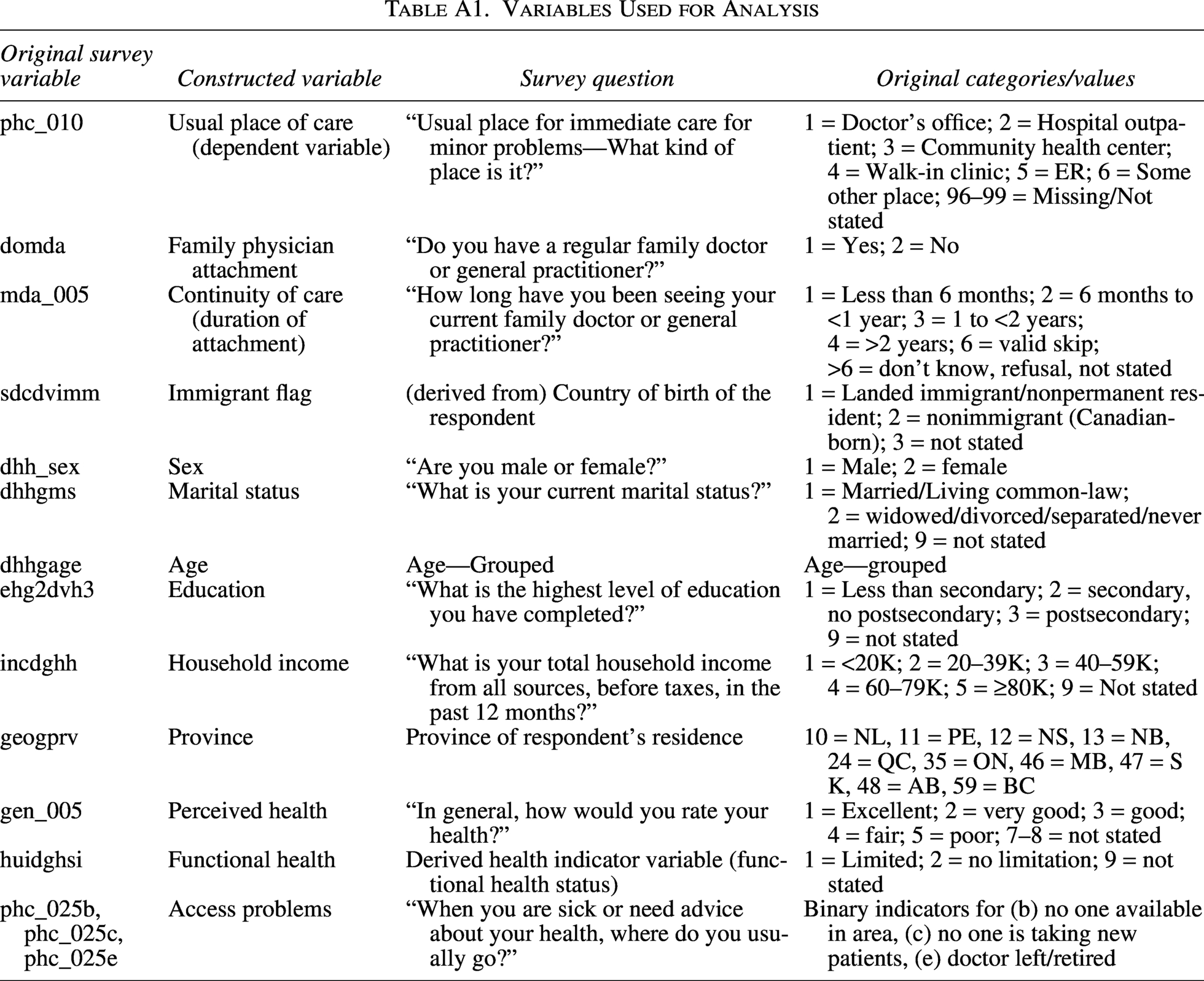
| Original survey variable | Constructed variable | Survey question | Original categories/values |
|---|---|---|---|
| phc_010 | Usual place of care (dependent variable) | “Usual place for immediate care for minor problems—What kind of place is it?” | 1 = Doctor’s office; 2 = Hospital outpatient; 3 = Community health center; 4 = Walk-in clinic; 5 = ER; 6 = Some other place; 96–99 = Missing/Not stated |
| domda | Family physician attachment | “Do you have a regular family doctor or general practitioner?” | 1 = Yes; 2 = No |
| mda_005 | Continuity of care (duration of attachment) | “How long have you been seeing your current family doctor or general practitioner?” | 1 = Less than 6 months; 2 = 6 months to <1 year; 3 = 1 to <2 years; 4 = >2 years; 6 = valid skip; >6 = don’t know, refusal, not stated |
| sdcdvimm | Immigrant flag | (derived from) Country of birth of the respondent | 1 = Landed immigrant/nonpermanent resident; 2 = nonimmigrant (Canadian-born); 3 = not stated |
| dhh_sex | Sex | “Are you male or female?” | 1 = Male; 2 = female |
| dhhgms | Marital status | “What is your current marital status?” | 1 = Married/Living common-law; 2 = widowed/divorced/separated/never married; 9 = not stated |
| dhhgage | Age | Age—Grouped | Age—grouped |
| ehg2dvh3 | Education | “What is the highest level of education you have completed?” | 1 = Less than secondary; 2 = secondary, no postsecondary; 3 = postsecondary; 9 = not stated |
| incdghh | Household income | “What is your total household income from all sources, before taxes, in the past 12 months?” | 1 = <20K; 2 = 20–39K; 3 = 40–59K; 4 = 60–79K; 5 = ≥80K; 9 = Not stated |
| geogprv | Province | Province of respondent’s residence | 10 = NL, 11 = PE, 12 = NS, 13 = NB, 24 = QC, 35 = ON, 46 = MB, 47 = SK, 48 = AB, 59 = BC |
| gen_005 | Perceived health | “In general, how would you rate your health?” | 1 = Excellent; 2 = very good; 3 = good; 4 = fair; 5 = poor; 7–8 = not stated |
| huidghsi | Functional health | Derived health indicator variable (functional health status) | 1 = Limited; 2 = no limitation; 9 = not stated |
| phc_025b, phc_025c, phc_025e | Access problems | “When you are sick or need advice about your health, where do you usually go?” | Binary indicators for (b) no one available in area, (c) no one is taking new patients, (e) doctor left/retired |