
Abstract
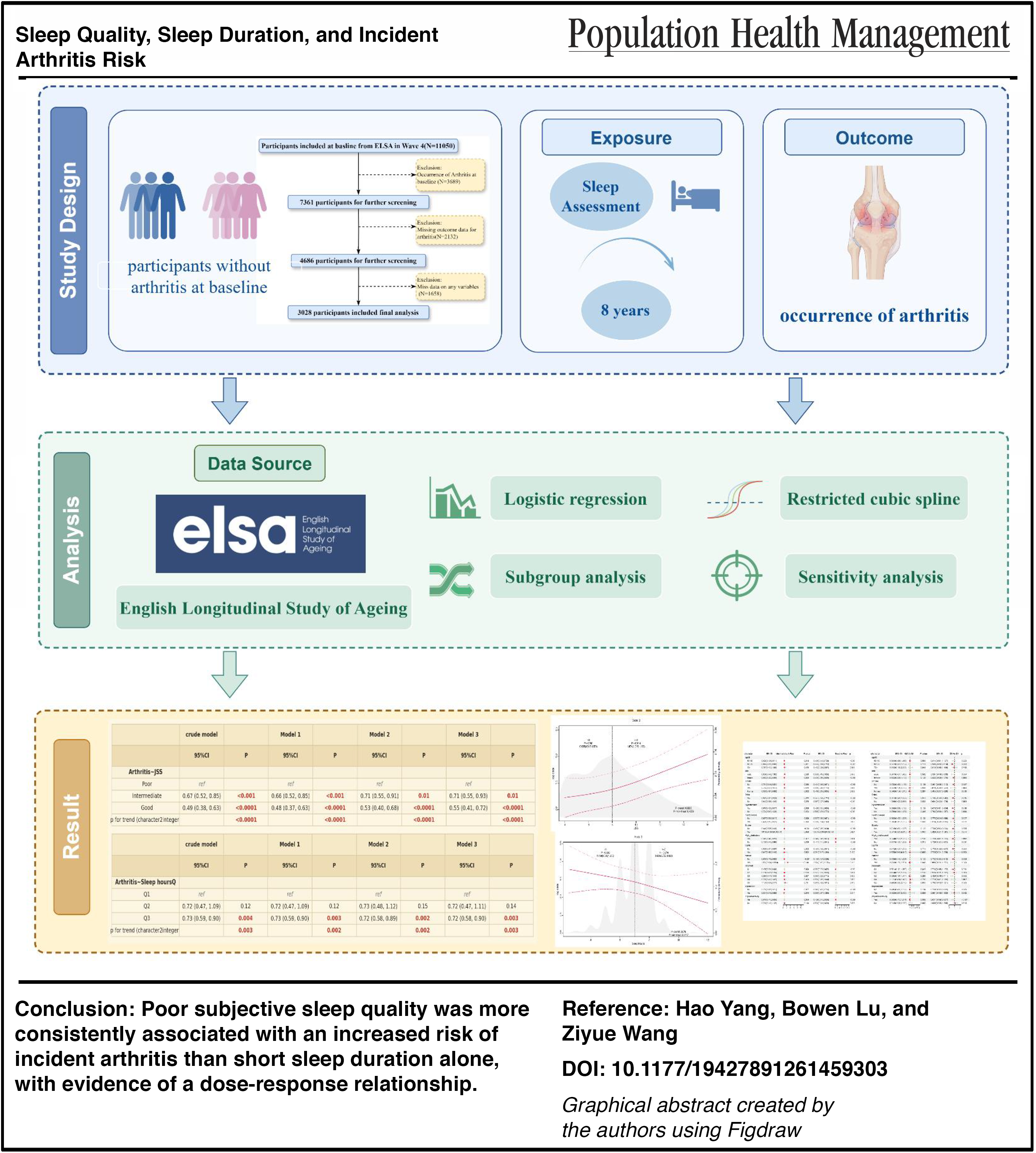
To examine the associations of sleep quality, sleep duration, and their trajectories with the risk of incident arthritis in middle-aged and older adults in the United Kingdom. Data from waves 4 to 8 of the English Longitudinal Study of Aging were used. We included 3028 participants aged ≥50 years without arthritis at baseline, followed for ∼8 years. Sleep quality was assessed using the Jenkins Sleep Scale (JSS), categorized as good, intermediate, or poor. Sleep duration was divided into tertiles. Incident arthritis was self-reported and physician-diagnosed. Associations were estimated using multivariable logistic regression and stratified analyses, including restricted cubic spline (RCS) models to explore dose–response relationships. Overall, 559 cases of incident arthritis were identified. Both intermediate and good sleep quality were associated with a lower risk of arthritis compared to poor sleep (odds ratio [OR] intermediate = 0.71, OR good = 0.55, P for trend < 0.001). The longest sleep tertile (Q3) showed a modest protective effect (OR = 0.72). RCS analysis revealed a significant linear dose–response relationship between JSS scores and arthritis risk. Sensitivity analyses of sleep-quality trajectories showed lower arthritis risk in all but the stable poor pattern, with the lowest risk in the stable good group (OR = 0.44). Poor subjective sleep quality is a more consistent predictor of arthritis than short-sleep duration alone, with a clear dose–response gradient. Improving poor sleep quality may be key to reducing arthritis risk.
Arthritis (AR) refers to inflammation or swelling of one or more joints and encompasses a group of inflammatory diseases caused by inflammation, infection, degeneration, trauma, or other factors. The main types include osteoarthritis, rheumatoid arthritis, and psoriatic arthritis, among others. 1 Clinically, AR is characterized by joint pain, swelling, stiffness, and restricted mobility, and is a leading cause of disability and economic burden worldwide. 2 Globally, ∼500 million people are affected by osteoarthritis, and its prevalence continues to rise with population aging and the obesity epidemic. 3 Moreover, the precise etiology of AR remains unclear, and no curative treatment is currently available. 4
The impact of arthritis on sleep has been extensively investigated. The core clinical manifestations of arthritis—pain and restricted joint mobility—are closely associated with insomnia. 5 Surveys have shown that up to 81% of patients with arthritis experience insomnia. In addition, a study from the United States reported that nearly one-third of adults with arthritis had various sleep disturbances. 6 Sleep is also an important psychosocial factor in patients, and its association with osteoarthritis has gained increasing recognition, encompassing both sleep quality and sleep duration. 7 Several studies have shown that patients with better sleep quality tend to report less severe knee pain, whereas restless or poor sleep is associated with more pronounced knee osteoarthritis symptoms.8,9 Other studies have indicated that individuals with knee osteoarthritis are more prone to sleep disturbances.10,11
However, a nationwide cross-sectional study found that only sleep deprivation was associated with a higher prevalence of osteoarthritis. 12 Consistently, a recent Mendelian randomization study reported that sleep duration exerted a similar effect on the risk of overall osteoarthritis but had no significant impact on knee osteoarthritis specifically. 13 These discrepant findings highlight the need for further investigations into diverse populations. Longitudinal evidence on the impact of sleep duration on the incidence of knee osteoarthritis in UK populations remains scarce.
Therefore, the present study aimed to use data from the English Longitudinal Study of Aging (ELSA) to conduct a longitudinal cohort analysis to examine the associations of sleep duration and sleep quality with the risk of knee osteoarthritis among middle-aged and older adults.
Methods
Study population
Data for this study were derived from the ELSA. ELSA is an ongoing prospective population-based cohort designed to investigate the aging process in adults aged ≥50 years living in England across social, psychological, and health domains. To maintain national representativeness, the cohort is periodically refreshed with new participants, and detailed information has been collected every 2 years since baseline through computer-assisted personal interviews combined with self-completed questionnaires. The design and implementation of ELSA have been comprehensively described elsewhere. 14
In the present study, wave 4 (2008–2009) was defined as baseline because this was the first wave to systematically assess self-reported sleep quality. Participants were followed from waves 5 to 8, yielding an approximate follow-up duration of 8 years (2008–2017). A total of 11,050 core sample members completed the wave 4 survey. After exclusions based on the study aim and data completeness, 3028 participants who were free of arthritis at baseline and had complete information on exposure variables, outcome, and covariates were included in the final analyses (Fig. 1).
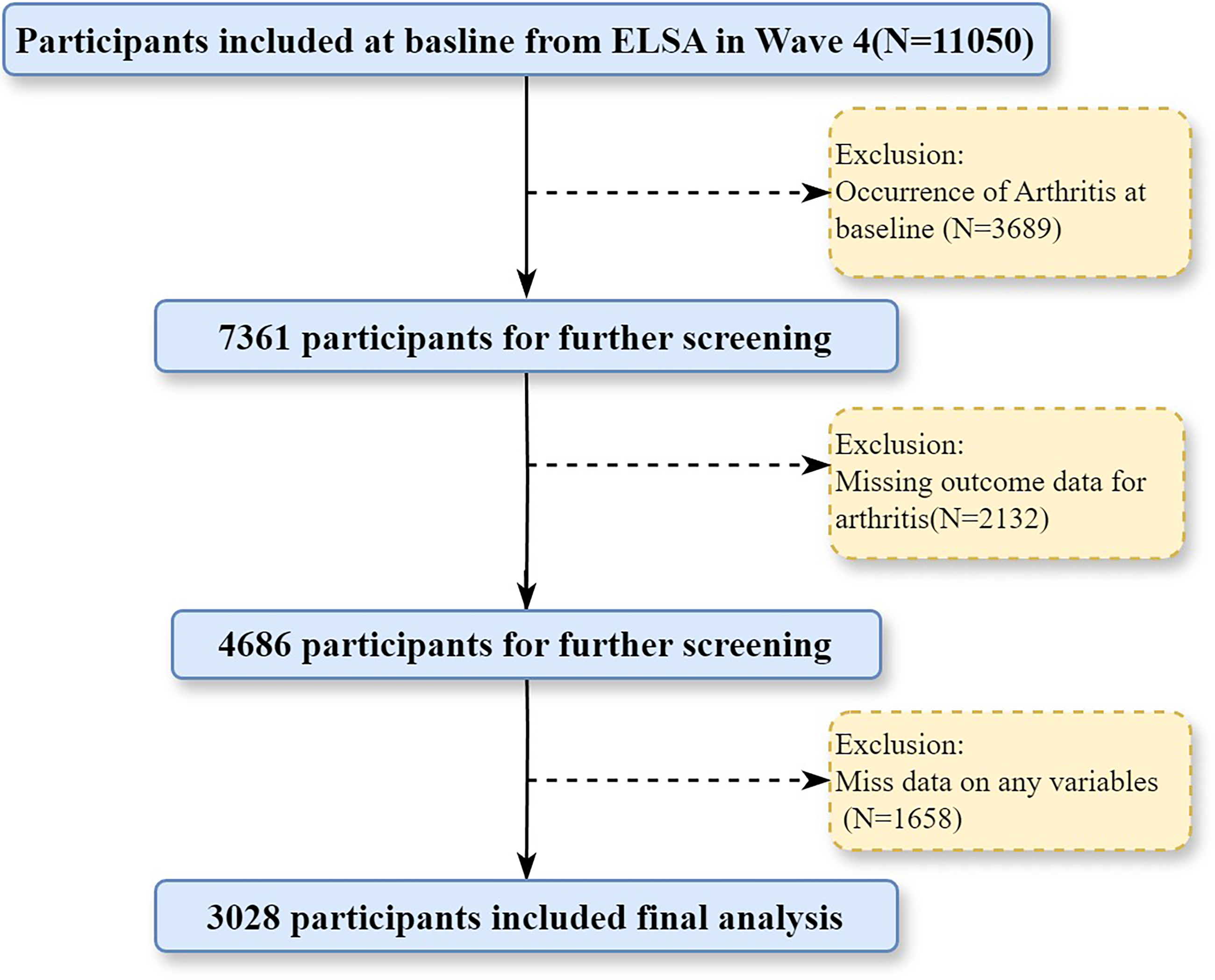
Flowchart of participant inclusion.
Assessment of sleep quality
At baseline, sleep quality was assessed using four standardized items from the Jenkins Sleep Questionnaire, which has been used in previous studies of older populations. Participants were asked to report the frequency of the following problems during the past month: (1) difficulty falling asleep; (2) waking up several times during the night; (3) waking up too early and being unable to fall asleep again; and (4) dissatisfaction with overall sleep.15,16 Participants were asked to report the frequency of the following problems during the past month: (1) difficulty falling asleep; (2) waking up several times during the night; (3) waking up too early and being unable to fall asleep again; and (4) dissatisfaction with overall sleep. Each item was rated on a 4-point Likert scale, where 1 = “not at all in the past month” and 4 = “three or more times per week.” Following the conventional scoring approach used in previous studies applying the Jenkins Sleep Scale (JSS), scores for the four items were summed to generate a total sleep quality score ranging from 4 to 16, with higher scores indicating more severe sleep disturbances and poorer overall sleep quality. This raw summed score was used as the primary measure of subjective sleep quality, and the score was further categorized into good, intermediate, and poor sleep quality according to previously used cutoffs. Participants were required to have completed at least three of the four items to be included in the analysis. Following previous work in ELSA and similar cohorts, the total sleep quality score was categorized into three levels: good (4–7 points), intermediate (8–11 points), and poor (12–16 points). 17
Sleep duration was assessed based on participants’ self-reported average nighttime sleep on a typical weekday. To further explore the association between trajectories of sleep quality and incident arthritis, we constructed five sleep-quality trajectory patterns using sleep-quality categories at waves 4 and 6: (1) persistently good: good sleep quality at both waves; (2) improved: sleep quality improving from poor to intermediate, or from poor/intermediate to good; (3) worsened: sleep quality deteriorating from good to intermediate/poor, or from intermediate to poor; (4) persistently intermediate: intermediate sleep quality at both waves; and (5) persistently poor: poor sleep quality at both waves.
Assessment of arthritis
The outcome of interest was incident, self-reported, physician-diagnosed arthritis during follow-up. At each wave, participants were presented with a standardized list of doctor-diagnosed conditions and asked whether they had ever been told by a doctor that they had any of these diseases. Incident arthritis was defined as a new report of physician-diagnosed arthritis at wave 8 among participants who were free of arthritis at baseline wave 4. Baseline sleep quality and sleep duration were measured at wave 4 and therefore preceded the ascertainment of incident arthritis. Because the exact date of arthritis onset was unavailable, incident arthritis was analyzed as a binary outcome over follow-up.
Assessment of covariates
A comprehensive set of potential covariates was included. Sociodemographic characteristics comprised: age (measured in years and categorized as 50–59, 60–69, 70–79, and ≥80 years in descriptive analyses; see Table 1), sex (male/female), marital status (currently partnered [married/cohabiting], never partnered, previously partnered [divorced/widowed]), educational attainment (higher education, secondary education, no qualifications or low education), and household income level (equivalized household income, categorized into quintiles from lowest to highest: Q1–Q5). Employment status was classified according to self-reported occupational group as managerial and professional, intermediate, routine/manual, or currently not in paid work.
Baseline Characteristics of Study Population by Arthritis
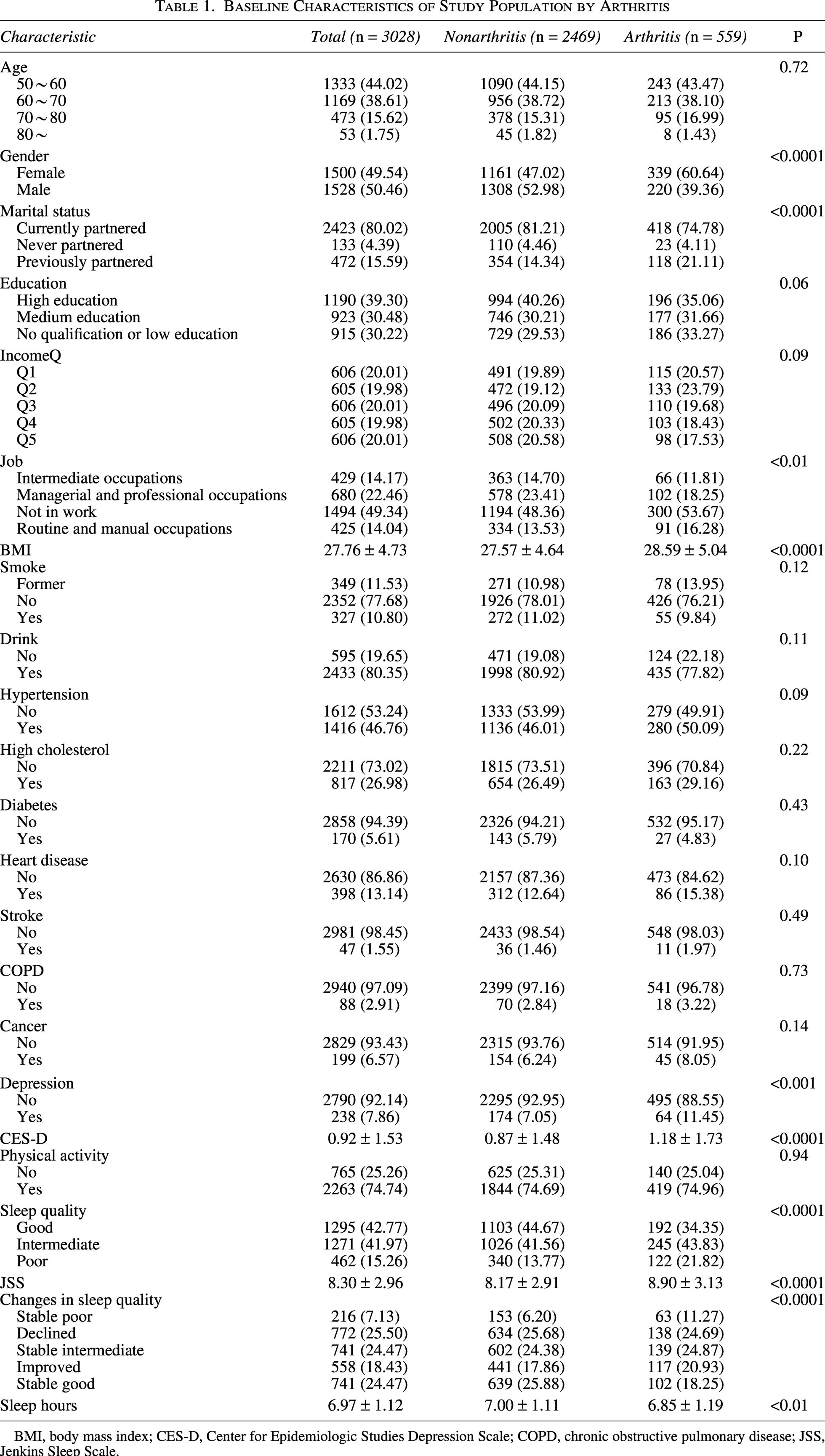
BMI, body mass index; CES-D, Center for Epidemiologic Studies Depression Scale; COPD, chronic obstructive pulmonary disease; JSS, Jenkins Sleep Scale.
Health-related behavioral covariates included body mass index (BMI, calculated from self-reported weight and height, kg/m2), smoking status (never, former, or current smoker), and current alcohol consumption (yes/no). Baseline chronic health conditions were based on self-reported doctor diagnoses and included hypertension, diabetes, heart disease, stroke, hypercholesterolemia, chronic obstructive pulmonary disease (COPD), and malignant neoplasms (cancer). Depressive symptoms were assessed with the short form of the Center for Epidemiologic Studies Depression Scale (CES-D). We recorded both the presence of depressive symptoms as a binary variable and the continuous distribution of the CES-D total score in descriptive analyses. Physical activity was evaluated according to the questionnaire used in the Health Survey for England, with participants reporting the frequency of engagement in light, moderate, and vigorous physical activities. In line with previous studies and guideline recommendations, individuals who reported engaging in moderate or vigorous physical activity at least once per week were classified as having regular physical activity, and all others were classified as having no regular physical activity.
Statistical analysis
Continuous variables were summarized as means ± standard deviations (SD), and categorical variables as percentages. Sleep quality and sleep duration were treated as the main exposure variables to examine their associations with incident arthritis. In this prospective cohort analysis, multivariable logistic regression to investigate the relationships of sleep quality and sleep duration with the risk of incident arthritis.
To estimate odds ratios (ORs) and 95% confidence intervals (CIs) for incident arthritis, four logistic regression models were fitted: Crude model: unadjusted; Model 1: adjusted for age (continuous); Model 2: additionally adjusted for socioeconomic variables based on Model 1, including educational attainment, occupational class, marital status, and equivalized household income quintiles; Model 3: further adjusted, based on Model 2, for baseline health-related factors, including smoking status (never/former/current), alcohol consumption (drinker/nondrinker), regular physical activity (yes/no, defined as moderate or vigorous physical activity at least once per week), BMI, and baseline chronic conditions and mental health status (presence of hypertension, diabetes, heart disease, stroke, hypercholesterolemia, COPD, malignant neoplasms, and depression [defined according to the CES-D scale]).
In addition, restricted cubic spline (RCS) functions were applied based on these four models to visualize the dose–response relationships of the JSS total score and sleep duration with the risk of incident arthritis. To further assess the robustness of the findings, subgroup analyses and several sensitivity analyses were performed. First, logistic regression was used to evaluate the association between sleep-quality trajectory patterns and incident arthritis. Second, the analytic sample was restricted to participants with baseline sleep duration of 6–9 hours, and the association between baseline sleep quality and incident arthritis was reexamined. All statistical analyses were conducted using R software version 4.4.2, with a two-sided significance level of α = 0.05.
Results
Characteristics of the study population
Table 1 shows baseline characteristics stratified by incident arthritis status. Among the 3,028 included participants, 559 reported incident arthritis during follow-up. Compared with those who did not develop arthritis, participants with incident arthritis were more likely to be women, to have been previously partnered (divorced/widowed), and to be engaged in routine/manual occupations or not in paid work. They also had higher BMI, a higher prevalence of depression and higher CES-D scores, higher Jenkins Sleep Scale (JSS) scores, and slightly shorter sleep duration (all P < 0.05). Other sociodemographic characteristics and most chronic conditions did not differ significantly between the two groups.
Table 2 summarizes baseline characteristics according to categories of baseline sleep quality (good, intermediate, poor). There were significant differences across sleep-quality groups in age, sex, marital status, educational attainment, income quintile, smoking and alcohol consumption, dyslipidemia, heart disease, depression and CES-D score, physical activity, JSS total score, and sleep duration (all P < 0.05). Overall, poorer sleep quality was associated with a higher proportion of women, lower education and income levels, a greater prevalence of adverse health behaviors and cardiovascular risk factors, a heavier burden of depressive symptoms, and shorter sleep duration, whereas the distributions of hypertension, diabetes, COPD, and cancer were broadly similar across groups.
Baseline Characteristics of Study Population by Sleep Quality
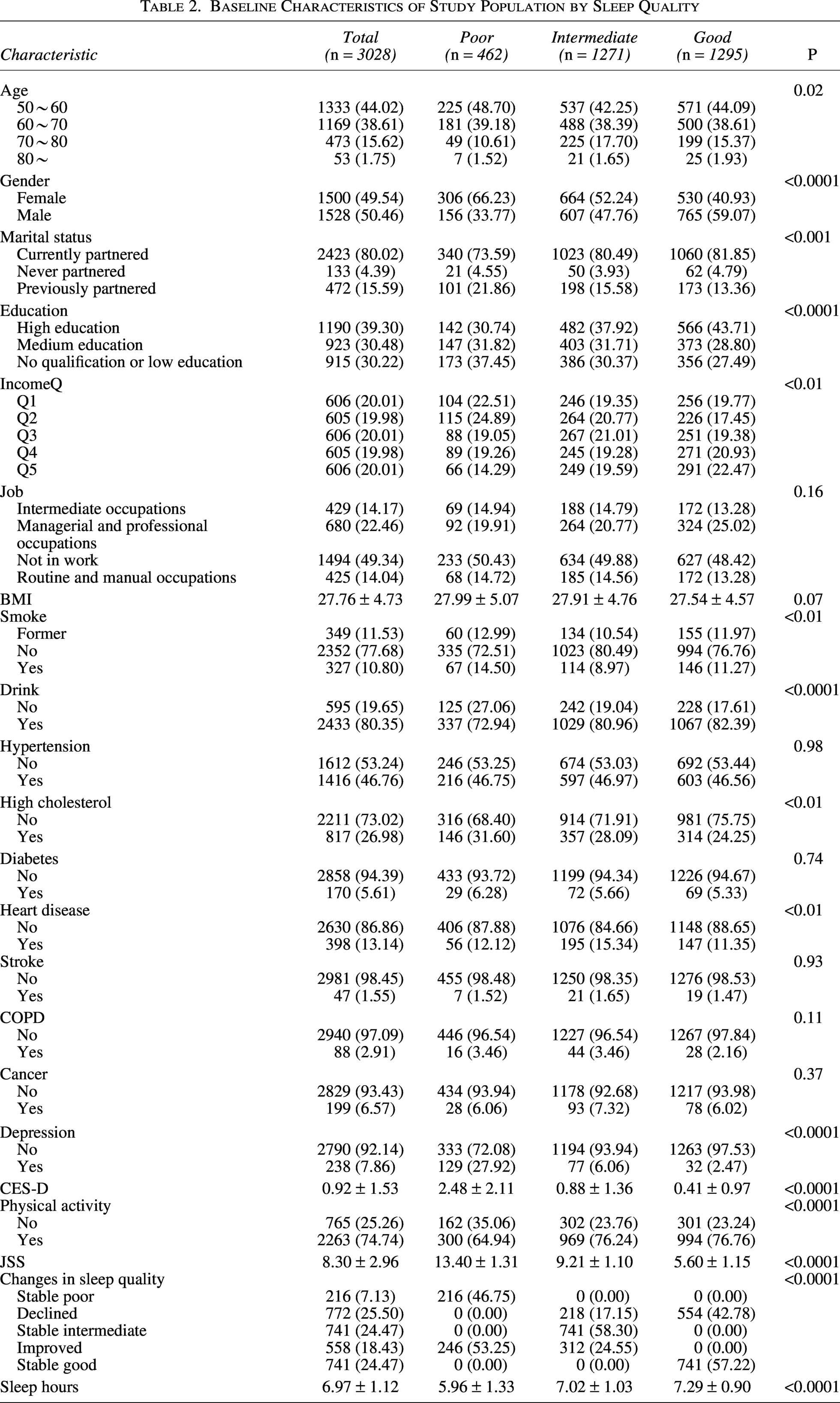
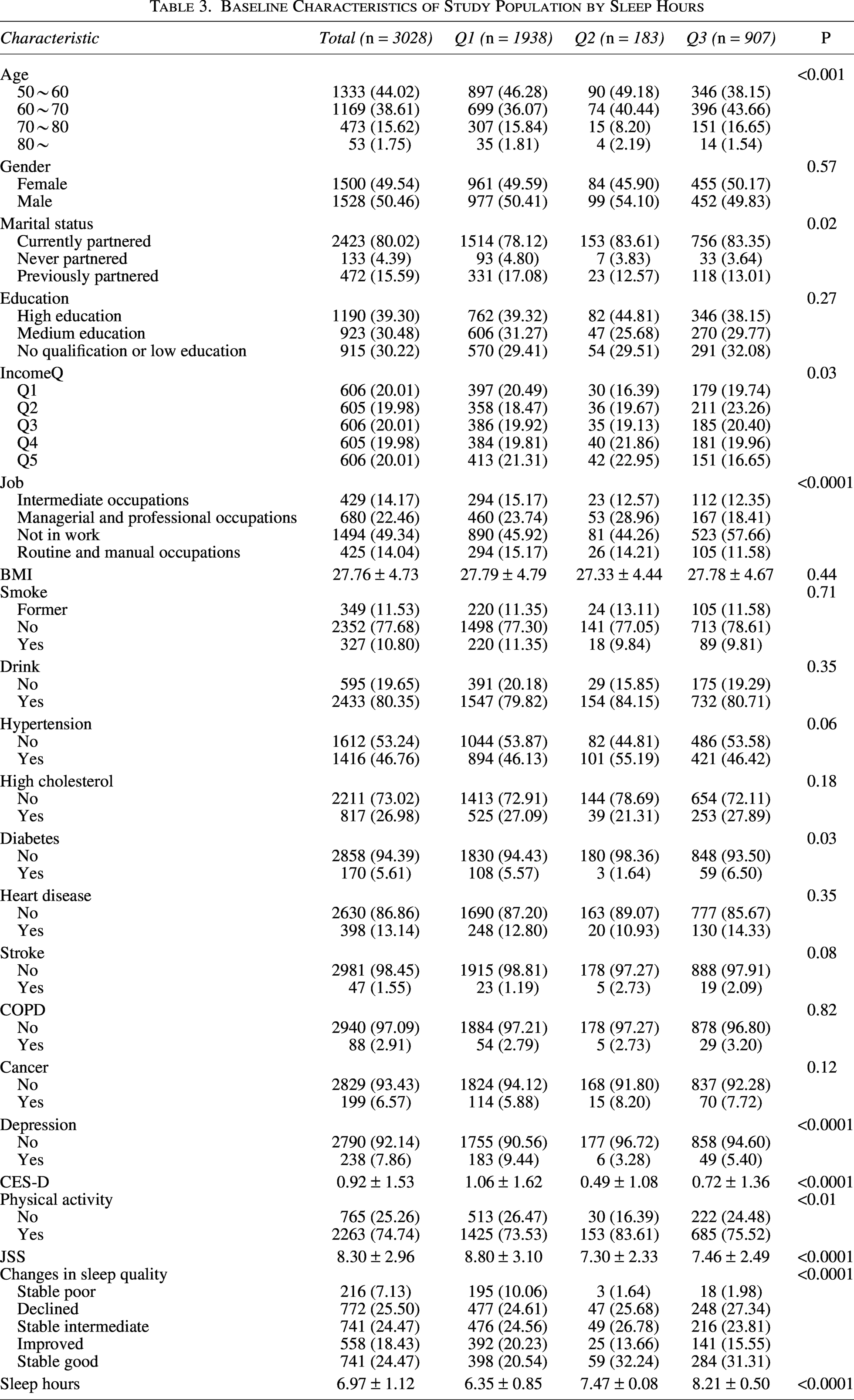
Table 3 compares baseline characteristics across tertiles of baseline sleep duration (Q1–Q3). Significant differences between sleep-duration groups were observed for age, marital status, income quintile, occupational class, diabetes, depression and CES-D score, physical activity, sleep-quality categories, JSS total score, and sleep-quality trajectory patterns (all P < 0.05). Participants in the short-sleep group were more likely to have low income, not be in paid employment, and have diabetes and depression, and tended to report poorer sleep quality and less favorable sleep-quality trajectories. By contrast, those in the long-sleep group generally had more favorable profiles on these indicators, while distributions of sex, education, smoking and alcohol consumption, hypertension, heart disease, COPD, and cancer did not differ appreciably across sleep-duration groups.
Baseline Characteristics of Study Population by Sleep Hours
To assess potential selection bias related to missing data, baseline characteristics were compared between participants included in the final complete-case analytic sample and those excluded because of missing exposure, outcome, or covariate data. Among baseline arthritis-free participants, 3028 were included in the final analytic sample, and 4333 were excluded. Missingness was mainly attributable to missing wave 8 sleep-quality measures and arthritis status, followed by missing alcohol consumption and BMI. Compared with included participants, excluded participants were older, had lower income and educational attainment, were more likely to be out of paid work, and had higher prevalences of diabetes, heart disease, stroke, and COPD. Excluded participants were also less likely to report regular physical activity. However, the mean JSS score and sleep duration were broadly similar between included and excluded participants. These findings suggest that missingness was unlikely to be completely random, and potential selection bias should be considered when interpreting the results. Detailed information is provided in the Supplementary Table.
Associations of sleep quality and sleep duration with incident arthritis
Using incident arthritis as the dependent variable (arthritis = 1, no arthritis = 0), we fitted multivariable logistic regression models with sleep quality and sleep duration as the main independent variables (Tables 4 and 5). Sleep quality was categorized into three groups (poor, intermediate, good), with poor sleep quality as the reference. In the overall sample, compared with the poor group, both the intermediate and good sleep-quality groups showed significantly lower risks of incident arthritis, and the results were broadly consistent across the four progressively adjusted models. In the fully adjusted Model 3, the OR was 0.71 (95% CI: 0.55–0.93) for the intermediate group and 0.55 (95% CI: 0.41–0.72) for the good group, indicating that individuals with good sleep quality had an ∼45% lower risk of incident arthritis than those with poor sleep quality. Trend tests showed a significant graded decrease in incident arthritis risk with improving sleep quality from poor to good (P for trend < 0.001). In sex-stratified analyses, this protective gradient remained robust among women, whereas in men the ORs for the intermediate and good groups were below 1, but their CIs mostly included 1, suggesting weaker statistical evidence and a potentially more limited association between sleep quality and arthritis risk in men.
Logistic Regression Results for Sleep Quality and the Risk of Arthritis
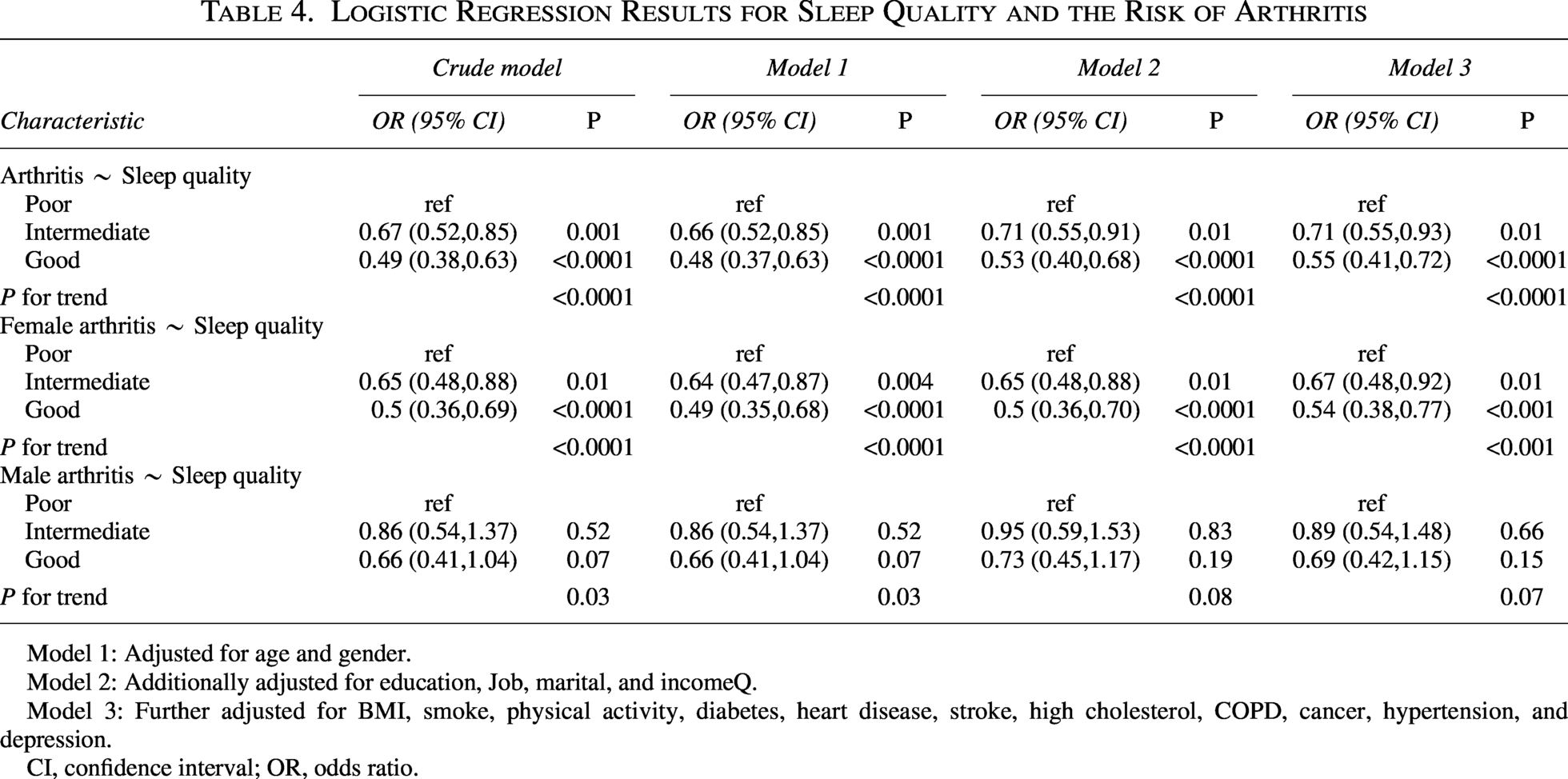
Model 1: Adjusted for age and gender.
Model 2: Additionally adjusted for education, Job, marital, and incomeQ.
Model 3: Further adjusted for BMI, smoke, physical activity, diabetes, heart disease, stroke, high cholesterol, COPD, cancer, hypertension, and depression.
CI, confidence interval; OR, odds ratio.
Logistic Regression Results for Sleep Hours and the Risk of Arthritis
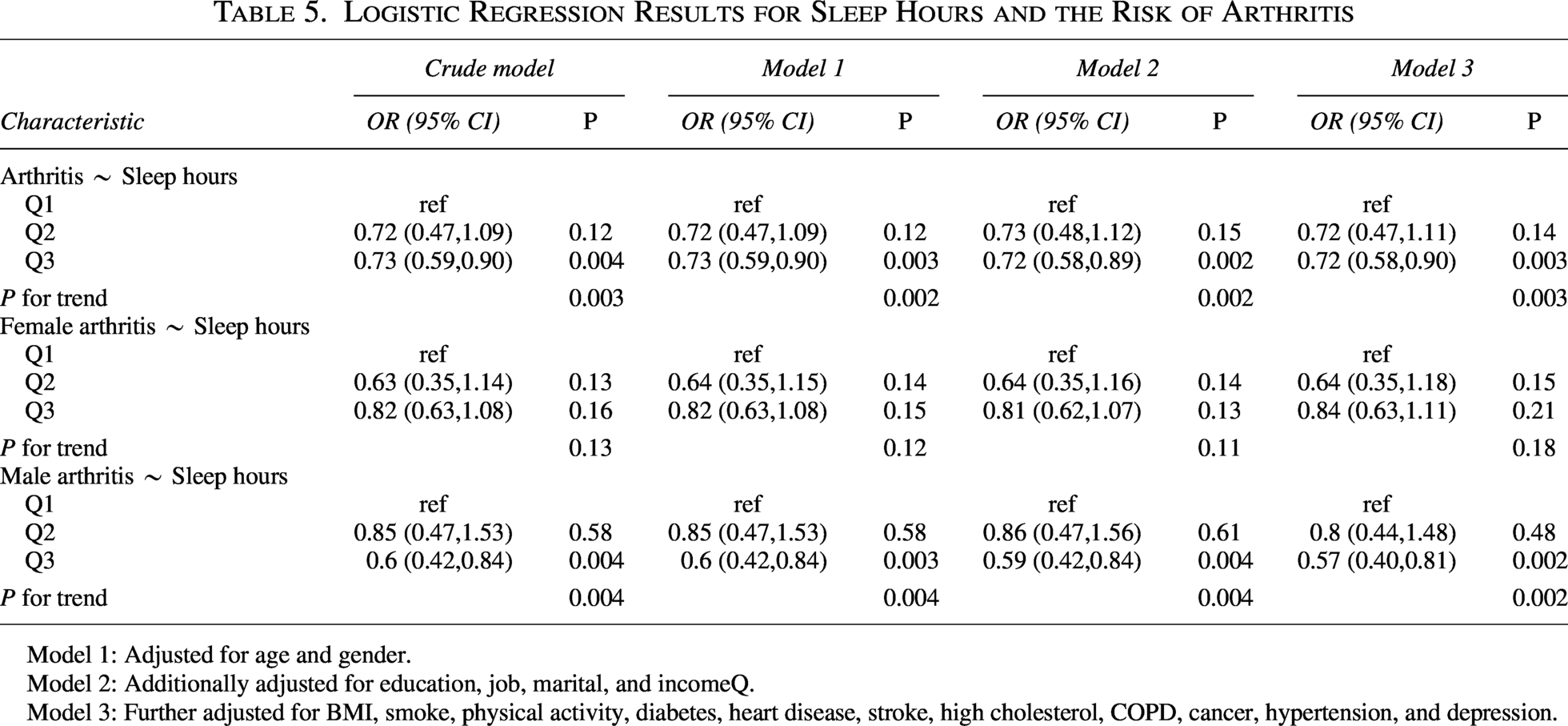
Model 1: Adjusted for age and gender.
Model 2: Additionally adjusted for education, job, marital, and incomeQ.
Model 3: Further adjusted for BMI, smoke, physical activity, diabetes, heart disease, stroke, high cholesterol, COPD, cancer, hypertension, and depression.
Sleep duration was divided into tertiles (Q1–Q3), representing increasing levels of sleep duration, with the shortest sleep group (Q1) as the reference. In the total population, the ORs for Q2 were close to 1 and not statistically significant, whereas Q3 was consistently associated with a lower risk of incident arthritis across all models. In Model 3, the OR for Q3 was 0.72 (95% CI: 0.58–0.90), indicating that, compared with short sleepers, participants in the highest tertile of sleep duration had an ∼28% lower risk of arthritis. The p for trend ranged from about 0.002 to 0.003, supporting a dose–response relationship between longer sleep duration and lower arthritis risk. Sex-stratified analyses suggested that this pattern was driven mainly by men: among men, the ORs for Q3 were stably between 0.57 and 0.60, with all tests for linear trend being statistically significant. In contrast, among women, the ORs for Q2 and Q3 were generally <1 but did not reach statistical significance, implying that the protective effect of adequate sleep duration on arthritis risk may be more pronounced in men.
Dose–response relationships between sleep quality, sleep duration, and incident arthritis
Figure 2 presents the results of the RCS analyses, with the x-axis representing the continuous distribution of sleep-related measures (JSS total score or sleep duration) and the y-axis showing the corresponding predicted ORs for incident arthritis. The dashed line indicates the median value of the exposure in the study population. In the fully adjusted model, there was a significant linear dose–response relationship between JSS score and the risk of arthritis (P_overall = 0.0003, P_nonlinear = 0.4279): as JSS scores increased (indicating worsening sleep quality), the risk of incident arthritis rose progressively. Segmented regression analyses (Table 6) further showed that when JSS < 8, JSS was not significantly associated with arthritis risk (OR = 0.935, 95% CI: 0.813–1.074, P = 0.341); however, when JSS ≥ 8, the risk of arthritis increased significantly with each unit increase in JSS (OR = 1.074, 95% CI: 1.015–1.136, P = 0.014), suggesting that more pronounced sleep impairment may represent a critical threshold for arthritis onset.
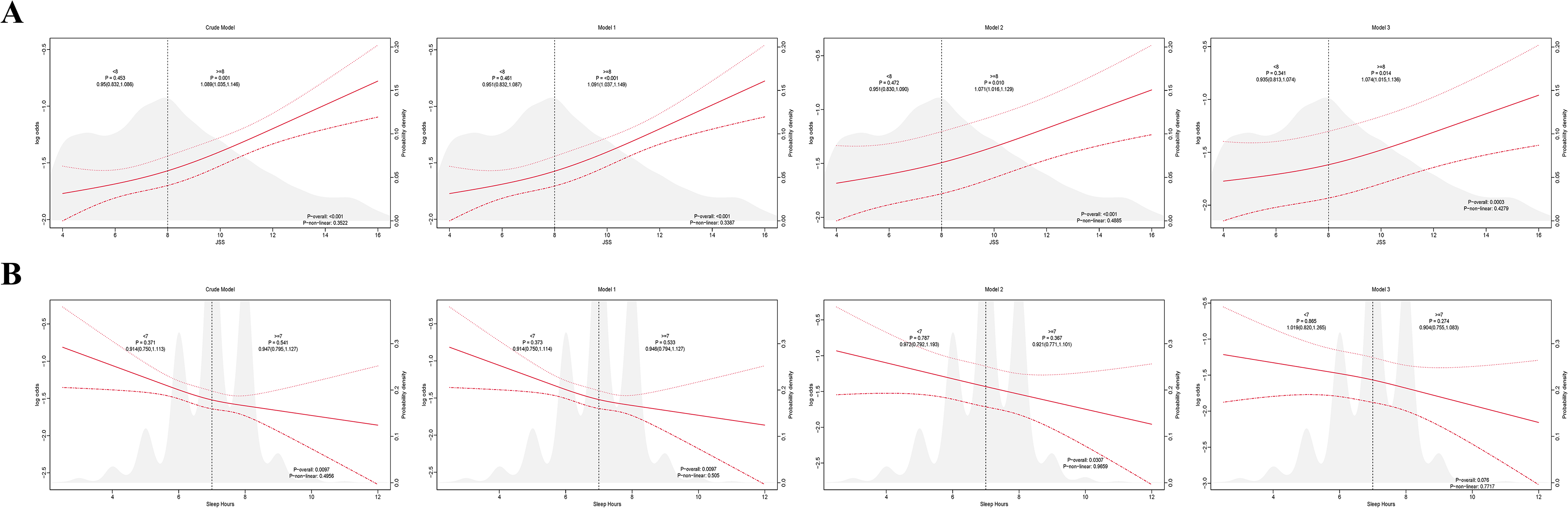
Associations of sleep quality and sleep duration with incident arthritis.
Logistic Regression Results for Changes in Sleep Quality and the Risk of Arthritis
Model 1: Adjusted for age.
Model 2: Additionally adjusted for education, job, marital, and incomeQ.
Model 3: Further adjusted for BMI, smoke, physical activity, diabetes, heart disease, stroke, high cholesterol, COPD, cancer, hypertension, and depression.
By contrast, no clear dose–response or nonlinear relationship was observed between sleep duration and arthritis risk (P_overall = 0.076, P_nonlinear = 0.7717). Segmented regression further indicated that when sleep duration was < 7 hours, the risk of incident arthritis did not change materially (OR = 1.019, 95% CI: 0.820–1.265, P = 0.865); when sleep duration was ≥7 hours, the association likewise did not reach statistical significance (OR = 0.904, 95% CI: 0.755–1.083, P = 0.274). Taken together, these findings suggest that, in this study population, sleep quality may be more closely related to the development of arthritis than sleep duration.
Subgroup analyses
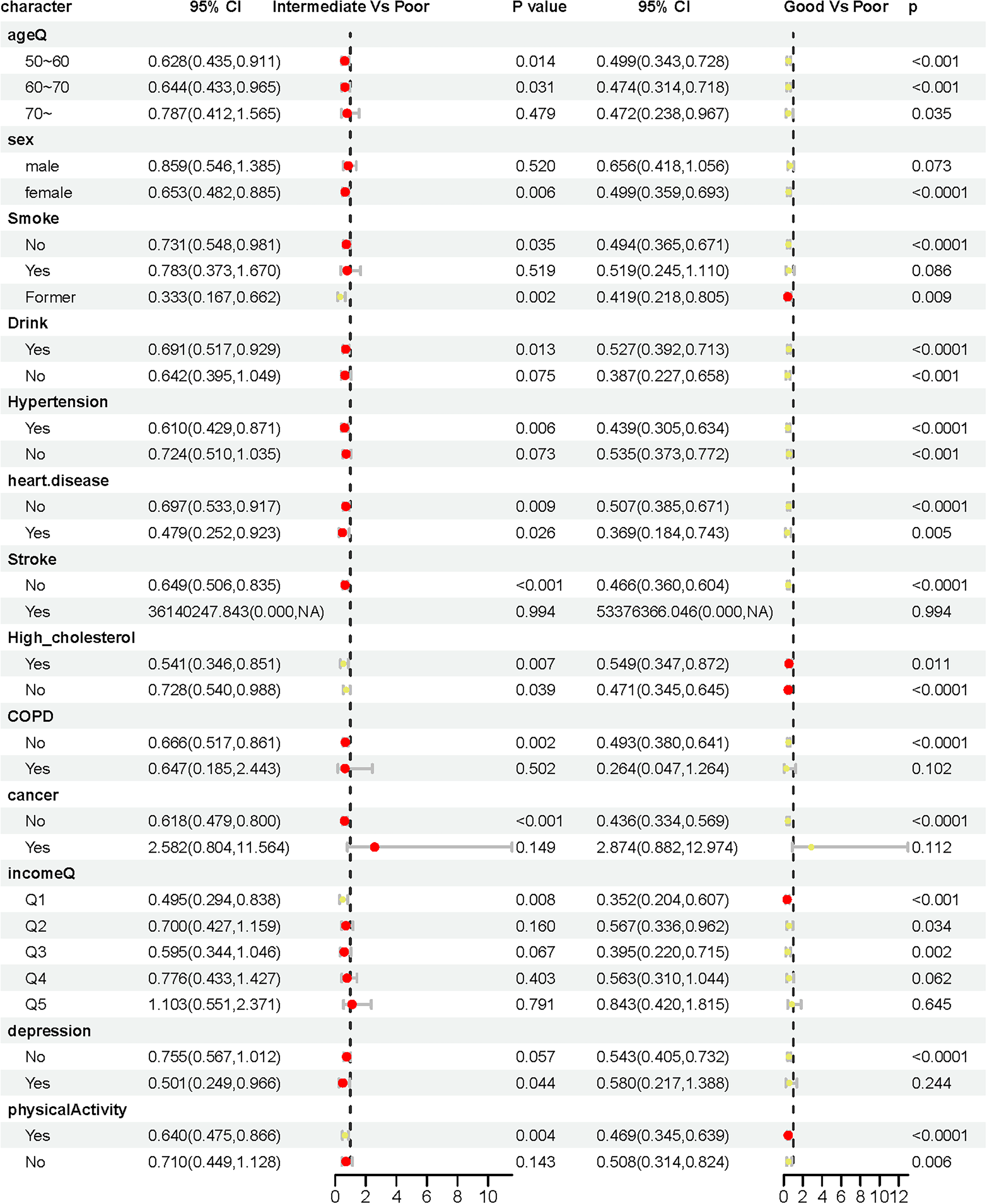
Subgroup analyses of the association between sleep quality and incident arthritis were conducted, as shown in Figure 3. Overall, across strata defined by age, sex, lifestyle factors, and comorbid conditions, the direction of association was broadly consistent: Moving from poor to intermediate or good sleep quality was generally associated with a lower risk of incident arthritis, and good sleep quality was linked to reduced arthritis risk in most subgroups. This protective association was particularly pronounced among women, individuals without depression, and those with sufficient physical activity. In some subgroups with multiple chronic conditions, the statistical significance of the association was attenuated; however, the effect estimates largely continued to indicate higher arthritis risk among those with poorer sleep quality.
Subgroup analysis of the association between sleep quality and incident arthritis.
Figure 4 presents the associations between sleep duration and incident arthritis across different subgroups. Using the lowest sleep-duration tertile (Q1) as the reference, both intermediate and longer sleep durations (Q2 and Q3) were generally associated with a lower risk of arthritis in most strata, with more consistent protective effects observed in certain subgroups such as men and individuals without severe chronic diseases. In some other subgroups, point estimates were mostly below 1, but the CIs crossed 1, suggesting limited statistical power. Taken together, the subgroup analyses support the main findings: Poorer sleep quality and relatively shorter sleep duration appear to be associated with an increased risk of incident arthritis, with some heterogeneity in effect size across population subgroups, but no evidence of associations in the opposite direction.

Subgroup analysis of the association between sleep duration and incident arthritis.
Sensitivity analyses
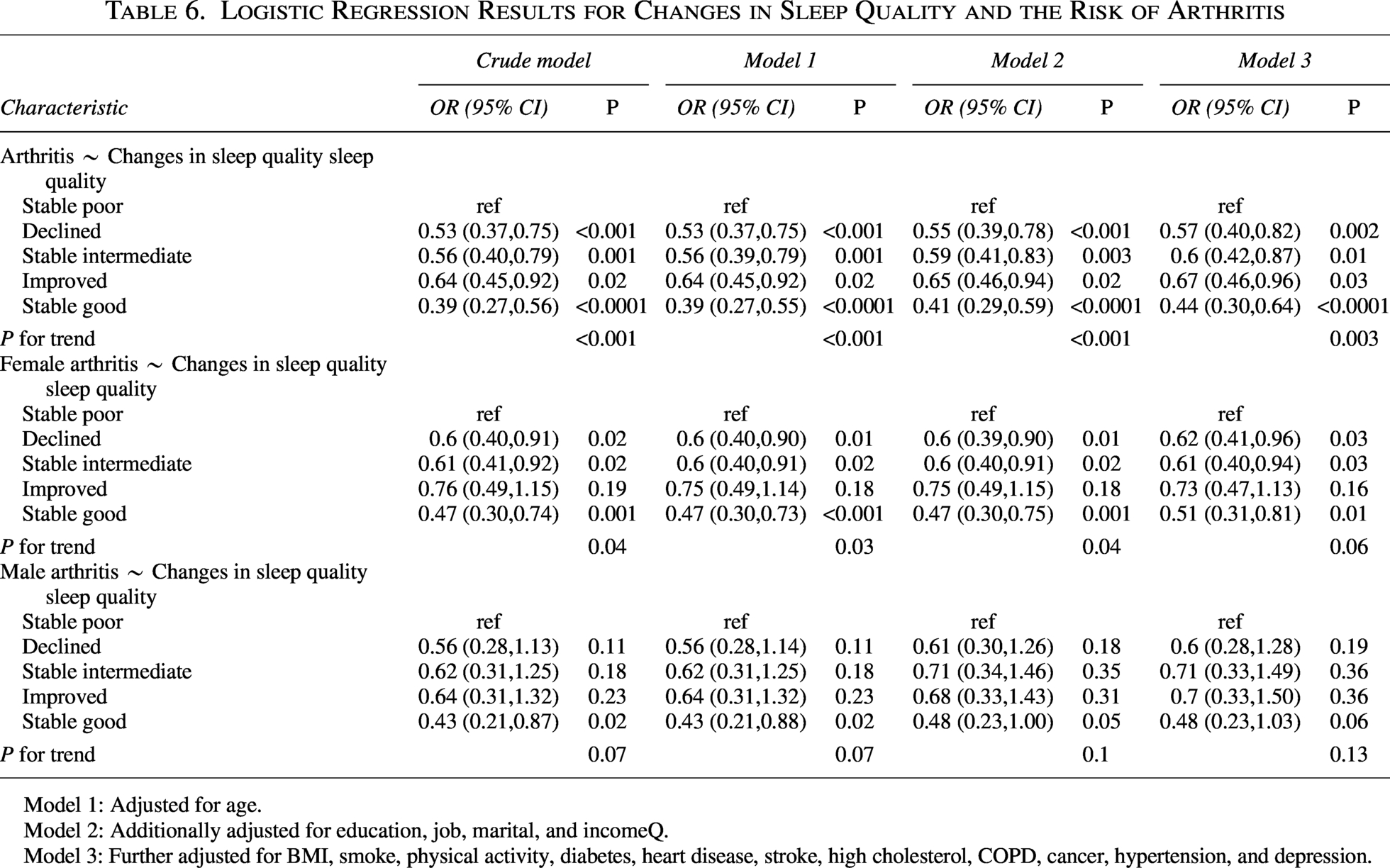
In sensitivity analyses, trajectories of sleep quality between waves 4 and 6 were examined in relation to incident arthritis (Table 6). Using the “stable poor” group as the reference, all other patterns—declined, stable intermediate, improved, and stable good—were associated with lower odds of incident arthritis in the overall sample, with the greatest risk reduction in the “stable good” group (fully adjusted OR = 0.44, 95% CI: 0.30–0.64; P for trend = 0.003). In women, stable intermediate and stable good trajectories remained significantly protective, whereas in men, estimates were directionally similar but less precise, with only the stable good pattern approaching statistical significance.
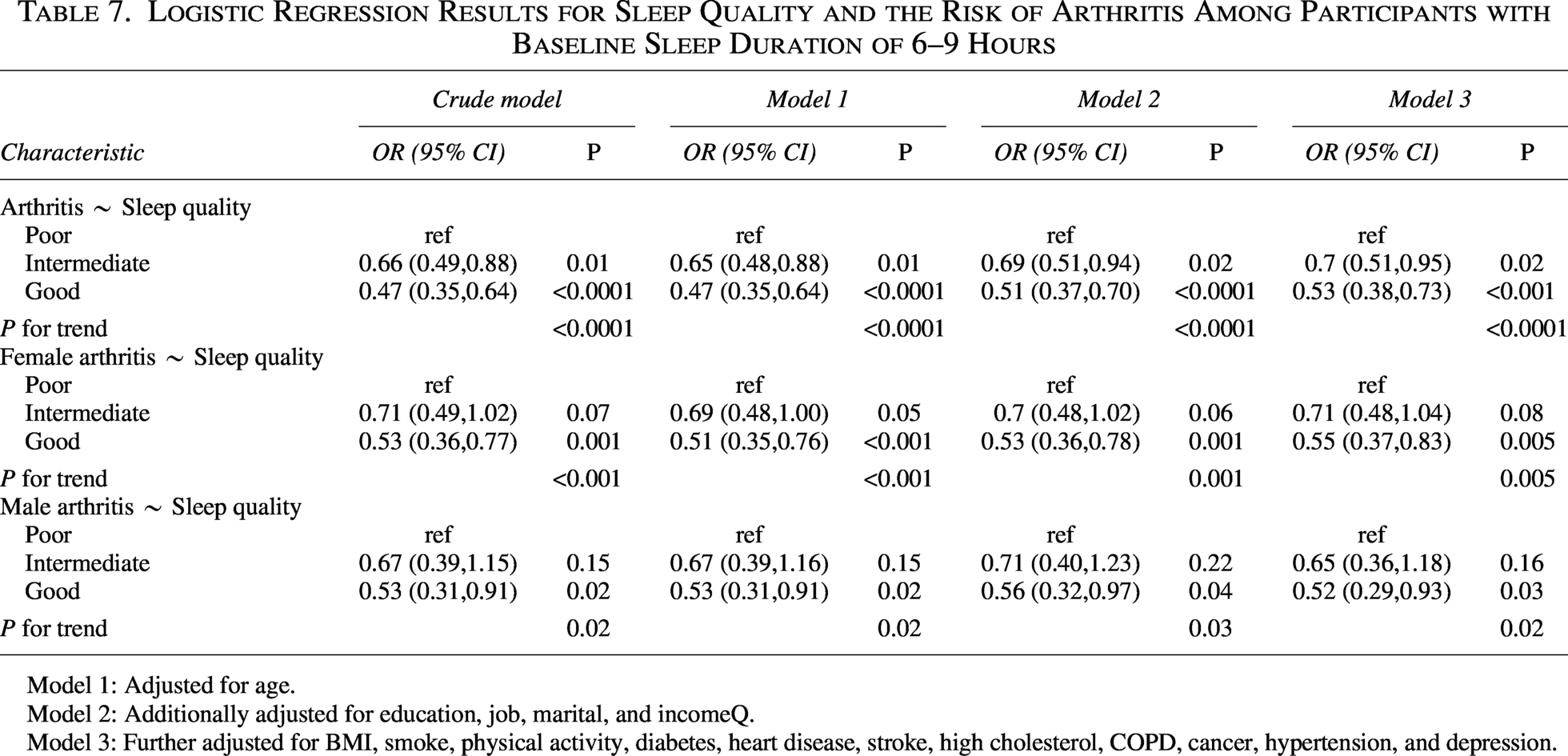
The sample was further restricted to participants with baseline sleep duration of 6–9 hours and reexamined the association between sleep quality and incident arthritis (Table 7). Using poor sleep quality as the reference, both intermediate and good sleep quality remained significantly associated with a reduced risk of arthritis in the fully adjusted model (OR intermediate = 0.70, 95% CI: 0.51–0.95; OR good = 0.53, 95% CI: 0.38–0.73; P for trend < 0.0001). In sex-stratified analyses, good sleep quality continued to show a protective effect in both men and women, with ORs of 0.52 and 0.55, respectively, and trend tests remaining statistically significant. These findings indicate that, even after excluding individuals with extreme sleep duration, the inverse association between sleep quality and incident arthritis remains robust.
Logistic Regression Results for Sleep Quality and the Risk of Arthritis Among Participants with Baseline Sleep Duration of 6–9 Hours
Model 1: Adjusted for age.
Model 2: Additionally adjusted for education, job, marital, and incomeQ.
Model 3: Further adjusted for BMI, smoke, physical activity, diabetes, heart disease, stroke, high cholesterol, COPD, cancer, hypertension, and depression.
To further evaluate whether the magnitude of sleep-quality change influenced the observed associations, the original improved and declined trajectory categories were separated into small and large changes. In this refined trajectory analysis, participants with stable poor sleep quality had a high incidence of arthritis, whereas those with stable good sleep quality had the lowest incidence. Compared with the stable poor group, small improvement, stable intermediate sleep quality, small decline, and stable good sleep quality were associated with lower odds of incident arthritis in the fully adjusted model. The strongest association was observed for stable good sleep quality (OR = 0.42, 95% CI: 0.29–0.61), followed by small decline (OR = 0.50, 95% CI: 0.35–0.72), stable intermediate sleep quality (OR = 0.59, 95% CI: 0.41–0.84), and small improvement (OR = 0.64, 95% CI: 0.44–0.93). Large improvement and large decline were not statistically significant, likely because these groups contained relatively small numbers of participants and incident cases. The overall trend remained significant (P for trend < 0.0001). Detailed event counts and regression results are provided in Supplementary Tables S3 and S4.
Discussion
This prospective analysis based on the ELSA cohort followed 3028 arthritis-free middle-aged and older adults (≥50 years) from wave 4 (2008–2009) for up to 8 years to examine the association between baseline sleep characteristics and incident arthritis. By wave 8, 559 new cases of arthritis had been identified, corresponding to a cumulative incidence of ∼18.5%. The study population was broadly balanced by sex (49.54% women), with a mean age around 60 years, and the majority were married/cohabiting and had at least secondary education, consistent with the overall profile of the ELSA cohort. Previous studies have shown that higher socioeconomic and educational levels tend to be associated with lower disease activity and better outcomes in arthritis, potentially through healthier lifestyles, greater health literacy, and better access to medical care. These findings align with the baseline differences observed in education, income quintiles, and arthritis risk in the current study. 18 Against this sociodemographic background, sleep quality, sleep duration, and their trajectories were evaluated as the main exposures, applying multivariable logistic regression, RCSs, and extensive subgroup and sensitivity analyses. Overall, the findings indicate that poor subjective sleep quality and relatively short-sleep duration are significantly associated with a higher risk of incident arthritis, consistent with recent cohort evidence on the link between sleep and arthritis risk.19,20
The biological mechanisms by which sleep quality and sleep duration influence arthritis—particularly osteoarthritis—are not yet fully elucidated. A growing body of experimental and epidemiological research suggests that sleep disturbances and circadian rhythm disruption may promote the onset and progression of autoimmune and inflammatory diseases by altering immune function and metabolic homeostasis. 21 On the one hand, sleep restriction or fragmented sleep can activate innate immune responses and upregulate pro-inflammatory cytokines such as IL-6, IL-1β, IL-17, and TNF-α,22,23 all of which have been implicated as key mediators of cartilage degradation and synovial inflammation in osteoarthritis.24,25 On the other hand, sleep disturbances may disrupt the secretion of circadian hormones such as melatonin and thereby alter the expression of pro-inflammatory cytokines, cartilage-degrading enzymes, and inflammatory mediators, ultimately accelerating structural joint damage. 26
From a metabolic standpoint, short sleep is strongly linked to obesity, insulin resistance, and metabolic syndrome, 27 all of which are established risk factors for osteoarthritis. 28 In addition, sleep restriction has been shown to disturb the rhythmicity and composition of the gut microbiota.29,30 Emerging “gut–bone axis” research indicates that gut microbiota and their metabolites modulate local joint inflammation and cartilage metabolism.31,32 Collectively, these findings suggest a complex interaction network linking sleep, immune activation, metabolism, gut microbiota, and osteoarthritis.
Clinically, several studies have suggested a bidirectional relationship between sleep and chronic pain. In patients with arthritis, joint pain and functional limitation may disturb normal sleep architecture by activating the sympathetic nervous system and altering pain modulatory pathways. 33 Conversely, sleep impairment can lower pain thresholds and enhance central sensitization, thereby amplifying the experience of pain and perpetuating a “pain–insomnia” vicious cycle. Pro-inflammatory cytokines can act directly on sleep-regulating centers in the hypothalamus, disrupt circadian regulation, and stimulate peripheral nociceptive pathways, further intensifying pain perception.34,35
At the psychological level, poor subjective sleep quality frequently co-occurs with depressive and anxiety symptoms. Depression has been identified as an important predictor of incident arthritis in middle-aged and older adults. 36 The clustering of poor sleep quality, higher depressive burden, and elevated arthritis risk observed in our study may therefore reflect, at least in part, the combined influence of inflammatory activation, neuroendocrine dysregulation, and psychosocial stress.
This study has several notable strengths. First, it is based on a nationally representative cohort with a prospective design and up to 8 years of follow-up, allowing a temporally robust assessment of the relationship between sleep status and incident arthritis. Second, we simultaneously considered sleep quality, sleep duration, and their temporal trajectories and applied multiple complementary statistical approaches—including multivariable adjustment, RCSs, subgroup analyses, and sensitivity analyses—to systematically and rigorously evaluate the associations between sleep and arthritis risk. The findings were highly consistent across different models and population subgroups. Third, by quantifying sleep quality using the continuous JSS score, we identified a potential risk threshold at JSS ≥ 8, which may serve as a practical reference for identifying high-risk individuals in clinical and public health settings. The sex-stratified findings further suggest that sleep-related interventions may confer particularly pronounced benefits in women, providing a rationale for more targeted prevention strategies.
Nonetheless, several limitations should be acknowledged. First, sleep quality, sleep duration, and arthritis were all assessed by self-report, which introduces the possibility of recall bias and misclassification, and we lacked objective sleep measures such as polysomnography or wearable device–based monitoring. In addition, although the JSS has been used in previous studies of older adults, its psychometric properties were not reevaluated in the current analytic sample. Therefore, sample-specific internal consistency, such as Cronbach’s alpha, and additional evidence of construct validity could not be reported. However, self-reported sleep metrics remain widely used and prognostically informative in large-scale population studies. Second, due to data constraints, we were unable to distinguish among different types of arthritis (e.g., knee osteoarthritis, rheumatoid arthritis, psoriatic arthritis), which precluded exploration of potentially differential effects of sleep on specific arthritis subtypes. Our conclusions should therefore be corroborated in cohorts with more refined phenotypic characterization. Third, although we adjusted for a broad range of socioeconomic factors, lifestyle behaviors, and comorbidities, residual confounding—such as baseline pain severity, detailed medication use, and occupational joint loading—cannot be completely ruled out. Finally, because our participants were middle-aged and older adults living in the United Kingdom, the generalizability of these findings to younger populations or to populations with different cultural and ethnic backgrounds remains to be established.
Conclusion
In conclusion, this large prospective cohort study provides robust evidence that poor sleep quality and insufficient sleep are associated with an increased risk of incident arthritis in middle-aged and older adults. Future research should integrate objective sleep assessments, inflammatory biomarkers, and imaging data across diverse populations to clarify the causal pathways linking sleep, inflammation, and joint structural degeneration and to identify effective intervention strategies that mitigate the incidence and progression of arthritis by improving sleep patterns.
Author’s Contributions
H.Y.: Designed the study, performed the statistical analysis, and drafted the manuscript. B.L.: Supervised the study, contributed to the study design, and revised the manuscript critically. Z.W.: Contributed to data curation, validation, and visualization. All authors read and approved the final manuscript.
Data Availability
This study analyzed data from ELSA conducted by the UK Data Services.
Ethics Approval and Consent to Participate
All methods were performed in accordance with the Declaration of Helsinki. This study protocol was reviewed and approved by the NRES Committee South Central—Berkshire on November 28, 2013 (13/SC/0532), the South Central—Berkshire Research Ethics Committee on September 23, 2015 (15/SC/0526), and the South Central—Berkshire Research Ethics Committee on May 10, 2018 (17/SC/0588). All participants in ELSA provided written informed consent to participate.
Footnotes
Acknowledgments
The authors are grateful to all participants who took part in this study, the staff at the research center, and the data management team for their invaluable efforts in contributing to the ELSA during all these years.
Author Disclosure Statement
All authors declare no conflicts of interest.
Funding Information
This work was supported by grants from the Shandong Provincial Natural Science Foundation (No. ZR2022LZY003), the National Natural Science Foundation of China (No. 82074453), and the Key Research and Development Program of Shandong Province (No. 2021CXGC010501).
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.