
Abstract
Importance
For smart home modification (SHM) to translate into routine practice, clinicians need evidence that occupational therapist (OT)-led workflows are clinically useful, feasible, and scalable in community settings.
Objective
To evaluate the clinical utility of an OT-led SHM program and to identify implementation barriers and strategies that support adoption and sustainment in community practice.
Design
Sequential explanatory mixed-methods study.
Setting
Community-based practice settings.
Participants
Ten licensed OTs who implemented the SHM program in community services. Therapists’ implementation experience included delivering the program to 40 community-dwelling adults with physical disabilities (effectiveness outcomes reported separately).
Outcomes and Measures
OTs rated the clinical utility of 31 program recommendations using a structured evaluation form across appropriateness, applicability, and effectiveness (9-point scale) and documented whether each recommendation was applied. Semistructured interviews were conducted to explain rating patterns and to explore implementation barriers and improvement needs. Interview data were analyzed using thematic analysis by two coders with consensus procedures and an audit trail. Mixed-methods integration mapped themes to recommendation-level ratings.
Results
Overall, OTs rated the recommendations as highly clinically useful across domains. Applicability was comparatively lower for budget planning and for developing/implementing automation scenarios. Interviews indicated that cost constraints and technical complexity reduced feasibility, whereas OT-led goal prioritization, partial automation, simplification of operational steps, context-based training, and caregiver-inclusive education supported adoption. Revisits were most commonly linked to predictable maintenance events (e.g., unplugged power, device resets, battery depletion), underscoring the need for platform-based self-management resources and a triage pathway separating clinical OT tasks from technical support.
Conclusions and Relevance
OT-led SHM shows strong clinical utility in community practice when delivered through occupation-centered assessment, tailored training, and iterative refinement. Scalable implementation may be strengthened by feasible automation strategies, caregiver-inclusive education, and structured support pathways that reduce preventable follow-up.
Article Contribution
This study provides clinically grounded evidence for the utility of a manualized, OT-led SHM workflow and offers implementation strategies (partial automation, caregiver-inclusive training, platform-based self-management with triage) to support sustainable community delivery.
Plain-Language Summary
This study demonstrates the clinical utility of an occupational therapist-led smart home modification program for people with physical disabilities living in the community. Smart home devices—such as voice assistants, smart switches, and motorized curtains—can help people with physical disabilities manage everyday activities at home, including turning on lights, opening doors, and controlling appliances. Ten occupational therapists who delivered the program to 40 community-dwelling adults rated the program as highly useful overall, especially when devices were matched to each person's daily goals and home situation, and when family members joined the training. The biggest challenges were budget planning and setting up automation routines. The findings provide practical implementation strategies—including partial automation, caregiver-inclusive education, and a triage pathway separating clinical from technical follow-up—that occupational therapists can use to deliver sustainable smart home services in community settings.
Keywords
Introduction
In modern societies, supporting independent living has become a major priority, particularly in the context of population aging and the increasing prevalence of chronic conditions and disability (Martin et al., 2008; Reeder et al., 2013). Smart home technology, delivered through mainstream Internet of Things (IoT) devices (e.g., smart switches, plugs, sensors, and voice assistants), can enable monitoring, environmental control, and timely prompts that support everyday routines (Liu et al., 2016; Morita et al., 2023). In rehabilitation, particularly in occupational therapy, smart home modification (SHM) is of growing interest because it can extend traditional home modification by enabling remote control, automation, and context-aware supports within the home environment (Tian et al., 2024).
Emerging evidence indicates that SHM may improve outcomes that are clinically meaningful. For people with physical disabilities, qualitative work has described increased perceived autonomy, safety, and emotional stability when smart home solutions are integrated into daily routines (Mun et al., 2022). A systematic review of electronic aids to daily living and related technologies reported positive effects on activities of daily living, although the evidence base remains heterogeneous (Mun et al., 2021). In older adults, a longitudinal pilot study found that smart home technology may support quality of life (Aggar et al., 2023), and a recent meta-analysis suggested that smart home technologies may reduce falls in community and residential care settings (Lui et al., 2025). At the same time, the same body of qualitative evidence has reported persistent adoption barriers—including the user-reported “hassle” of operating electronic aids to daily living, usability demands, caregiver dependence, privacy concerns, and uneven fit between off-the-shelf devices and disability-specific needs—indicating that perceived benefits do not automatically translate into sustained routine use (Alzahrani et al., 2021; Dermody et al., 2024; Mun et al., 2022).
Cultural and policy contexts shape these adoption patterns. In Korea, the Act on Guarantee of Right to Health and Access to Medical Services for Persons with Disabilities and the Act on Support for Assistive Devices for Persons with Disabilities, the Elderly, and so on, together with public health center home-visit services and community care pilot programs, support closer postimplementation follow-up than is typical in settings such as Australia (Aggar et al., 2023), where smart home delivery more often depends on individual procurement and self-managed sustainment.
Despite these promising findings, important limitations and implementation barriers remain. Much of the literature relies on small-scale or pre–post designs, and high-quality trials with long-term follow-up are still limited (Dhamanti et al., 2023; Facchinetti et al., 2023; Liu et al., 2016; Moyle et al., 2021; Reeder et al., 2013). In practice, implementation may be constrained by device–user fit, usability demands, cost, maintenance burden, and social acceptance (Berridge & Wetle, 2020; Martin et al., 2008; Tian et al., 2024). These challenges highlight the need for feasible clinical workflows that support user-centered design, iterative matching, and coadaptation as needs and contexts evolve (Felber et al., 2024; Kim et al., 2020; Kokorelias et al., 2023).
These gaps are particularly relevant in Korean community care, where population aging and the rapid expansion of community-based rehabilitation services—including public health center home visits and community care pilot programs—have shifted rehabilitation from facility settings into users’ daily living environments. In this context, occupational therapists (OTs) are increasingly expected to deliver structured, manualized services that can be replicated across institutions and reimbursed through public programs. To address this need, Mun (2024) developed a Korean SHM program through a sequential evidence-building process: a systematic review (Mun et al., 2021), a national demand survey (Mun & Kim, 2025), a Delphi consensus study with multidisciplinary experts (Mun & Kim, 2024a), and a preintervention–postintervention clinical implementation with 40 community-dwelling adults with physical disabilities (Mun, 2025). However, whether the resulting OT-led workflow is clinically useful from the perspective of the therapists who deliver it remains unexamined—an essential prerequisite for scalable adoption in routine community practice.
Despite growing interest, few studies have examined SHM as a manualized, clinician-delivered service and evaluated its clinical utility in routine community practice, particularly when OTs systematically lead decision-making, training, and refinement (Ding et al., 2023; Mun & Kim, 2024a; Tian et al., 2024). Therefore, the purpose of this study was to evaluate the clinical utility of an OT-led SHM program delivered through a structured manual and to identify barriers and strategies that support adoption and sustainment. We used a sequential explanatory mixed-methods design in which OTs rated the clinical utility of 31 program recommendations across appropriateness, applicability, and effectiveness, followed by semistructured interviews to explain rating patterns and generate recommendations for program refinement. Specifically, we addressed three research questions: (1) How do OTs rate the clinical utility of an OT-led SHM program across appropriateness, applicability, and effectiveness? (2) Which implementation conditions and clinical reasoning processes explain higher- and lower-rated recommendations, particularly around feasibility, role delineation, and caregiver involvement? (3) What modifications to the manual, training, and service pathway do therapists propose to support sustained adoption in Korean community practice?
Methods
Study Design
We used a sequential explanatory mixed-methods design to evaluate the clinical utility of an OT-led SHM program. First, OTs rated the clinical utility of each program recommendation using a quantitative form. Next, we conducted semistructured interviews to explain the rating patterns and to identify implementation barriers and improvement needs. We integrated quantitative and qualitative findings during interpretation through side-by-side comparison and joint interpretation of convergent and divergent results.
Program Overview: OT-Led SHM
In this manual, the SHM workflow is described as “tailored” because each step is customized along four explicit variables—the user's prioritized occupational goals, the user's body functions and capacities, the home environment (including network and device infrastructure), and the caregiver situation. The six-step Clinical Application Procedure (Section “Clinical Application Procedure”) operationalizes this customization, and the Role Delineation table (Section “Role Delineation: OT and Research Team”) clarifies which steps are led by the OT and which involve research-team technical support.
The SHM program uses a structured manual and implementation procedures. The workflow guides OT-led clinical decision-making across: (1) identifying activity limitations and priority goals, (2) determining feasibility for SHM adoption, (3) matching needs with appropriate smart home solutions, (4) installation/configuration and user training, and (5) monitoring and refinement based on user performance and context.
Manual Development (Tailored SHM Program and Evidence Base)
The tailored SHM program used in this study was based on a program developed by Mun (2024) using the Intervention Mapping Model. Program development followed a rigorous evidence-building process, including a systematic review (Mun et al., 2021), a survey (Mun & Kim, 2025), a case study (Mun & Kim, 2024b), and a Delphi survey (Mun & Kim, 2024a). In the present study, we focused on therapist-perceived clinical utility to inform real-world implementation, role delineation, and scalability in community practice.
Service Pathway and Institutional Context
The program was delivered through a structured service pathway embedded in Korean community-based rehabilitation. Referrals originated from public health centers, regional health and medical centers, and community rehabilitation institutions serving community-dwelling adults with physical disabilities. After intake, the responsible OT conducted one or more home visits to complete the occupational profile, functional assessment, and home-context analysis. Smart home devices were procured through collaborating vendors and installed during the OT home visit; when device configuration exceeded routine clinical setup (e.g., network connectivity or account provisioning), the research team provided limited technical support so that clinical decision-making remained with the OT. Each participant received up to $500 in funding for tailored SHMs, covering device costs and installation, consistent with the budget reported in the parallel effectiveness study (Mun, 2025). Follow-up visits and remote contacts were scheduled weekly through Weeks 1–4, with additional contacts through Week 10 as clinically needed (Figure 1).
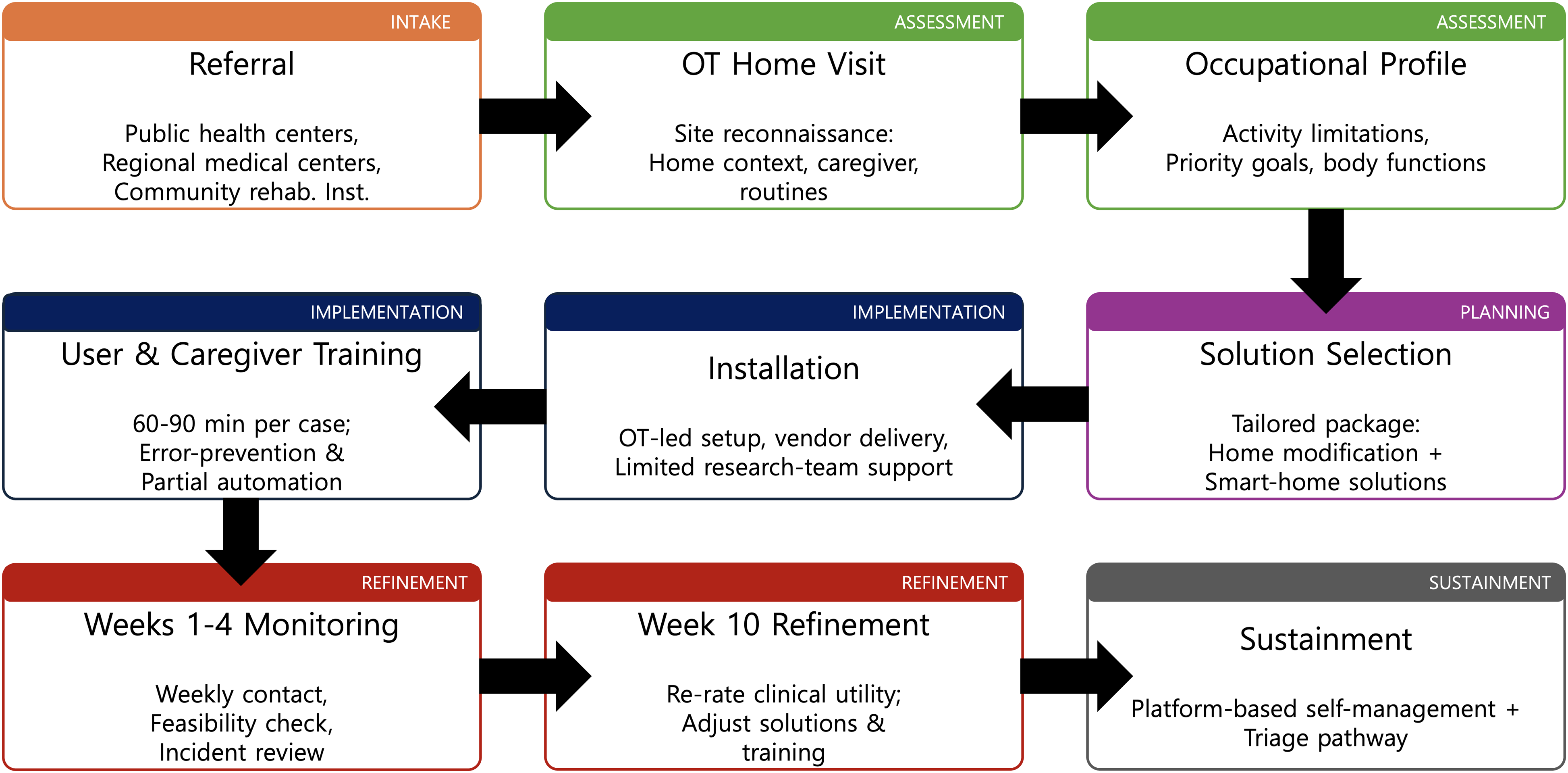
Occupational therapist-led smart home modification service pathway.
Participants and Setting
Occupational Therapists
We recruited 10 OTs, all holding a current occupational therapy license issued by the Korean Ministry of Health and Welfare. The inclusion criterion was completion of the SHM training program (described in the Section “OT Preparation and Implementation Support”); OTs who had not completed the training were excluded. OTs were recruited using purposive convenience sampling: invitations were sent to the lead OT at each community-based institution that had collaborated on the parallel implementation study (Mun, 2025)—public health centers, regional health and medical centers for persons with disabilities, and regional assistive technology centers in Seoul and Gangwon Province. All participants provided informed consent and completed both the quantitative ratings and the qualitative interview.
Clinical Cases
Before this evaluation, the same 10 OTs delivered the SHM program to 40 community-dwelling adults with physical disabilities—real clients prospectively recruited for the parallel implementation study, not previously enrolled clients of the participating OTs and not simulated cases. We reported the effectiveness outcomes of that clinical implementation separately (Mun, 2025). In this study, OTs drew on their real-world implementation experiences when evaluating clinical utility. Drawing on their experience with these 40 cases, the same 10 OTs rated the 31 program recommendations described in the Section “Quantitative: Clinical Utility Evaluation Form.”
OT Preparation and Implementation Support
Therapists received training on the SHM manual and clinical workflow through two didactic lectures and one hands-on practice session. Training covered: (1) smart home concepts and common configurations, (2) manual-based procedures for SHM delivery, and (3) home-context analysis and solution selection aligned with users’ activity limitations and goals.
Role Delineation: OT and Research Team
OT Responsibilities
OTs conducted the initial assessment and goal setting with each of the 40 real community-dwelling clients (not simulated cases), selected and matched technologies to user needs, completed basic configuration steps specified in device manuals, provided 60–90 min of user/caregiver training, conducted weekly monitoring during Weeks 1–4, and provided follow-up contacts as needed through Week 10.
Research Team Support
When technical issues exceeded routine clinical setup (e.g., connectivity or configuration problems), the research team provided limited troubleshooting during installation/configuration. OTs retained responsibility for clinical decision-making and education.
Clinical Application Procedure
Therapists implemented the program according to the following procedures:
(1) Needs identification: Therapists documented activity limitations and established priority goals with the user (and caregiver when applicable). (2) Feasibility assessment: Therapists confirmed SHM suitability based on the home context and user capabilities. (3) Technology matching and planning: Therapists selected devices/features aligned with identified needs and the home environment. (4) Installation/configuration: Therapists installed devices and configured settings; they used research support only when issues exceeded routine setup. (5) User training: Therapists provided education and guided practice to support independent use, including strategies to simplify operation and prevent errors. (6) Monitoring and refinement: Therapists modified device settings and training strategies as needed to improve fit, usability, and satisfaction.
Measures and Data Collection
The clinical utility ratings and qualitative interviews were completed within 4 weeks after the Week 10 follow-up visit of the OT's implementation case (i.e., approximately 10–14 weeks after initial device provision).
Quantitative: Clinical Utility Evaluation Form
OTs assessed the clinical utility of the 31 program recommendations—the manual-level practice statements produced by the prior Delphi study (Mun & Kim, 2024a) that operationally define the OT-led SHM program—as applied during their implementation of the program with the 40 clients (Section “Clinical Cases”). For each recommendation (n = 31), OTs rated three domains, appropriateness, applicability, and effectiveness, on a 9-point scale (1 = lowest, 9 = highest). OTs also documented whether each recommendation was applied during implementation. We categorized scores as Good (≥6), Fair (3–5), or Poor (<3). Because no standardized clinical utility instrument existed for OT-led SHM with adults with physical disabilities at the time of the study, we developed a study-specific evaluation form. The form was constructed iteratively with the program manual: candidate items were derived from the 31 manual recommendations produced through the prior Delphi study (Mun & Kim, 2024a) and refined with two OTs and one assistive-technology researcher for clarity, nonoverlap, and representativeness. The three rating domains (appropriateness, applicability, and effectiveness) were adopted from Smart's (2006) clinical utility framework, which has been used in prior occupational therapy evaluation studies. Before the main study, we pilot-tested the form with two therapists who were not included in the main sample and revised item wording to reduce ambiguity.
Qualitative: Semistructured Interviews
After program implementation, we conducted in-depth semistructured interviews with therapists. Interview topics included assessment and planning workflow; feasibility judgment and technology matching; installation/configuration challenges and support needs; user/caregiver education processes; follow-up burden and strategies to streamline support; long-term sustainment issues (e.g., maintenance needs, device resets, and common user errors); perceived benefits and limitations in practice; and recommendations to improve scalability (e.g., accessible troubleshooting resources or a support platform for users and clinicians). Each therapist participated in one individual interview (10 interviews in total) conducted face-to-face in a private room at the therapist's institution, with an average duration of 60 min (range 50–75 min). Interviews were conducted by the first author, a male OT with a doctoral degree and prior qualitative research experience, using a semistructured guide organized by the topics above (see Table 1). All interviews were audio-recorded with written consent, professionally transcribed verbatim in Korean, and checked for accuracy against the recordings. Participants were offered the opportunity to review and amend their transcripts (member checking); no substantive changes were requested. Field notes on context and nonverbal cues were written immediately after each interview and integrated into the analytic memos.
Semistructured Interview Guide Used with Occupational Therapists (n = 10).
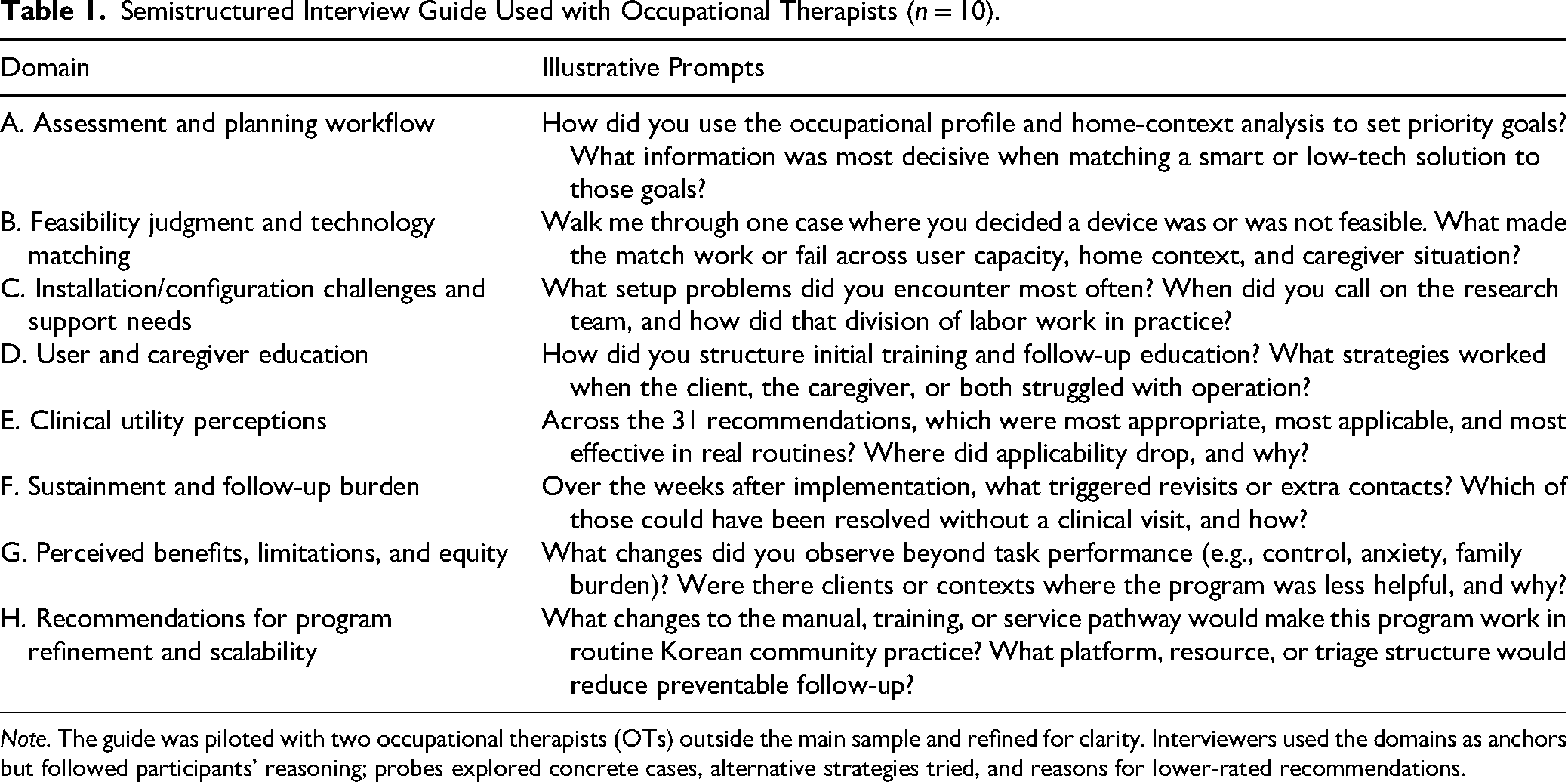
Note. The guide was piloted with two occupational therapists (OTs) outside the main sample and refined for clarity. Interviewers used the domains as anchors but followed participants’ reasoning; probes explored concrete cases, alternative strategies tried, and reasons for lower-rated recommendations.
Data Analysis
Quantitative Analysis
We analyzed quantitative data using SPSS to compute descriptive statistics (means and standard deviations) for each domain and recommendation.
Qualitative Analysis
We analyzed interview data using thematic analysis. To enhance trustworthiness, we applied investigator triangulation: two researchers independently coded transcripts and iteratively refined a consensus-based codebook through repeated discussions. They resolved coding discrepancies through discussion and consensus and finalized themes through comparison across participants. We maintained an audit trail (e.g., analytic memos and coding logs) to document coding decisions and theme development. We used qualitative findings to explain quantitative rating patterns and to identify implementation barriers and improvement needs. Analysis followed Braun and Clarke's (2006) six-phase reflexive thematic analysis: (1) familiarization with the transcripts through repeated reading; (2) generation of initial codes across the entire data set; (3) searching for candidate themes by collating codes that shared meaning; (4) reviewing themes against the coded extracts and the full data set; (5) defining and naming themes to articulate each theme's scope and storyline; and (6) producing the report with illustrative quotes mapped to the quantitative rating patterns. We managed and coded transcripts manually in Microsoft Word using the highlight and comment features, with codebook entries and theme definitions recorded in a companion Word document, in order to preserve the context and nuance of Korean-language excerpts that could be distorted during translation into coding software. Themes were translated into English for reporting by the first author, with back-translation of representative excerpts by a bilingual colleague to confirm fidelity.
In practice, two coders independently performed line-by-line coding of the 10 transcripts, generating 79 initial codes. Through iterative comparison and discussion, codes were collated into 17 candidate categories. After review against the coded extracts and the full data set, the categories were refined and consolidated into the five reported themes. An audit trail (analytic memos, coding logs, and version-controlled codebook entries) documented coding decisions and theme development throughout.
Mixed-Methods Integration
During interpretation, we mapped qualitative themes to recommendation-level ratings as part of methodological triangulation to identify: (1) reasons for lower ratings, (2) conditions that supported successful implementation, and (3) modifications that could reduce follow-up burden and improve sustainability.
Results
Qualitative findings helped explain quantitative rating patterns. Lower applicability ratings were primarily linked to feasibility constraints (budget planning) and implementation complexity (automation scenarios). Therapists described practical strategies, particularly simplification, partial automation, caregiver-supported routines, and platform-based self-management resources, to improve real-world scalability.
General Characteristics of Participants
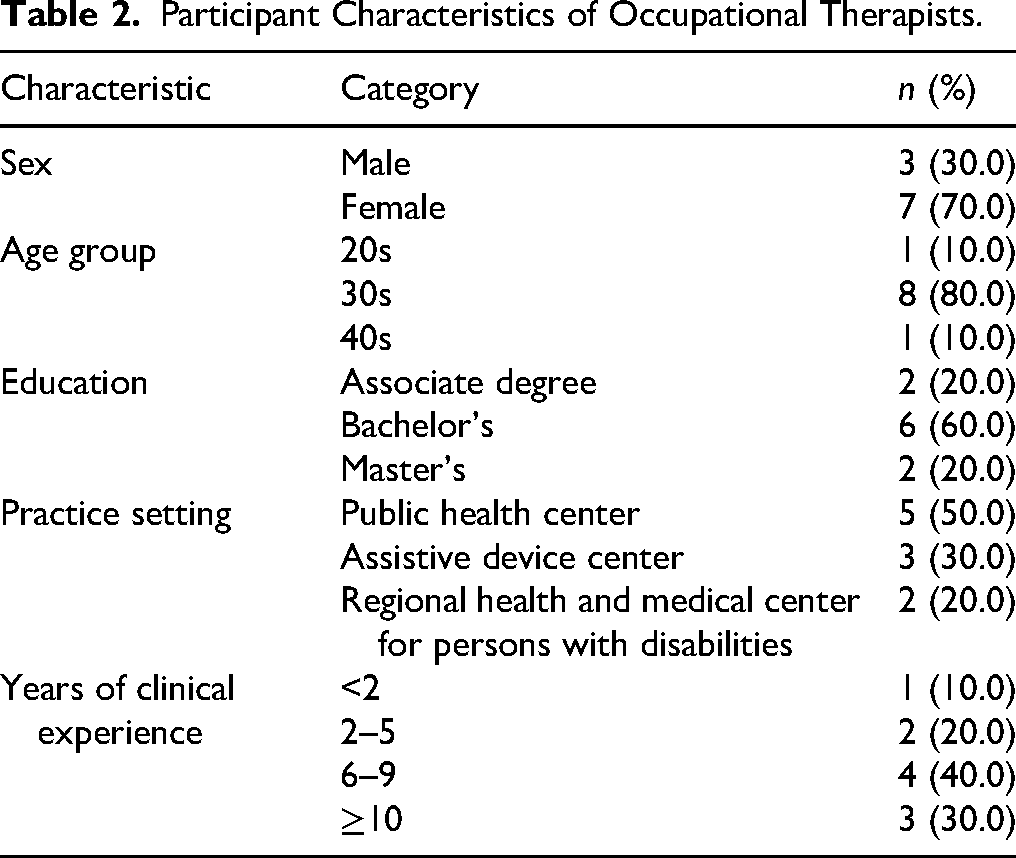
Ten OTs participated in the study; three were men (30.0%) and seven were women (70.0%). One OT was in their 20s (10.0%), eight in their 30s (80.0%), and one in their 40s (10.0%). Education levels were associate degree (n = 2, 20.0%), bachelor's (n = 6, 60.0%), and master's (n = 2, 20.0%). Practice settings included public health centers (n = 5, 50.0%), assistive device centers (n = 3, 30.0%), and regional health and medical centers for persons with disabilities (n = 2, 20.0%). Clinical experience was <2 years (n = 1, 10.0%), 2–5 years (n = 2, 20.0%), 6–9 years (n = 4, 40.0%), and ≥10 years (n = 3, 30.0%; Table 2).
Participant Characteristics of Occupational Therapists.
Quantitative Results: Clinical Utility Ratings
Overall, OTs rated the OT-led SHM recommendations as highly clinically useful. Mean (range) ratings were 7.45 (6.5–8.8) for appropriateness, 7.23 (4.6–8.2) for applicability, and 8.31 (7.4–9.0) for effectiveness (Table 3). Most recommendations were classified as Good (≥6): 31/31 for appropriateness, 29/31 for applicability, and 31/31 for effectiveness.
Clinical Utility Ratings of SHM Recommendations (n = 31).
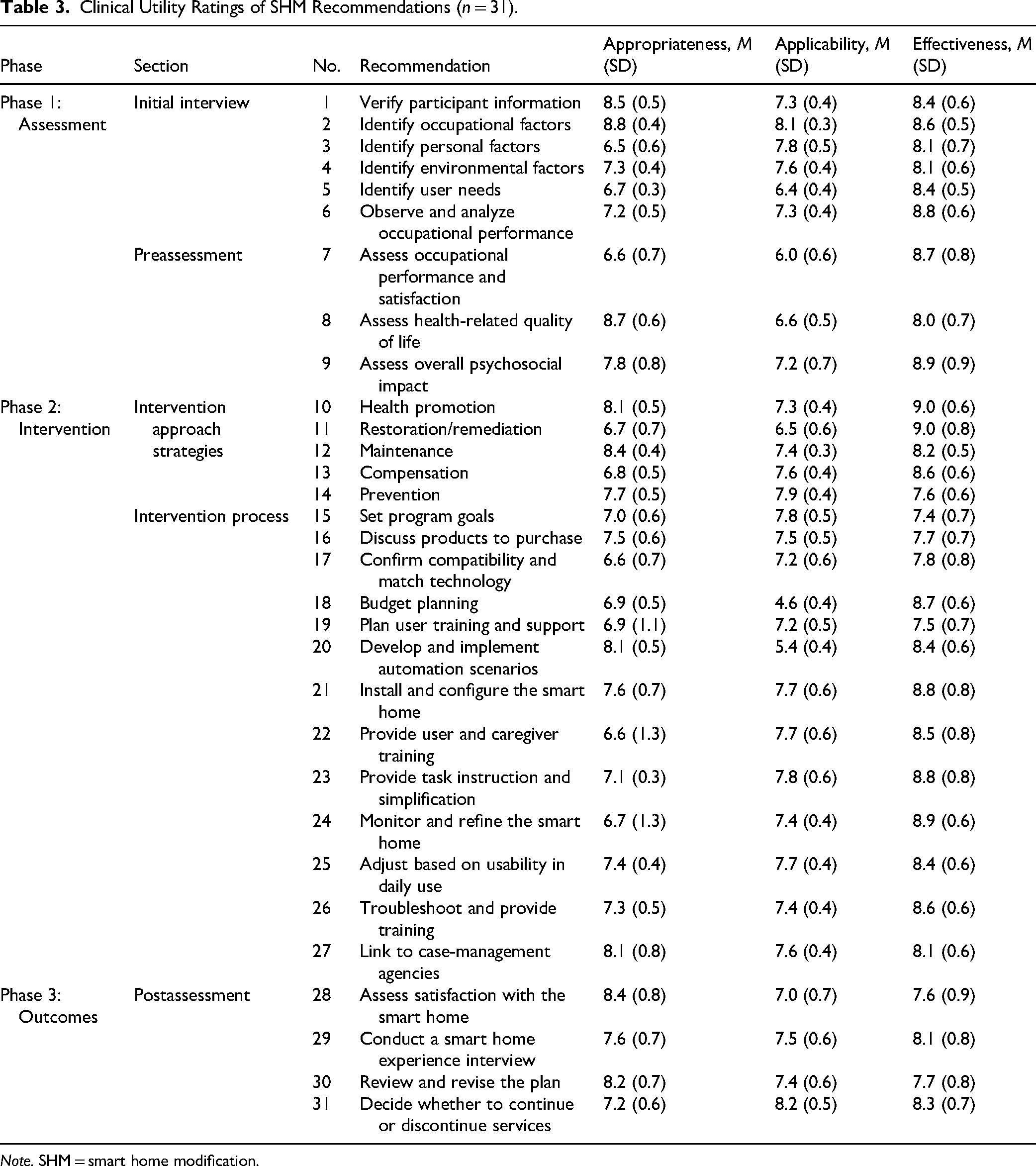
Note. SHM = smart home modification.
Two recommendations showed comparatively lower applicability ratings: budget planning (M = 4.6) and developing/implementing automation scenarios (M = 5.4). These items were typically constrained by contextual feasibility (e.g., cost, variable home infrastructure) and technical complexity.
Qualitative Results: Themes from Semistructured Interviews
Theme 1: OT Profiling Strengthened Clinical Fit Through Integrated Home Modification and Smart Solutions
OTs emphasized that clinical utility depended on OT-led occupational profiling and functional assessment, followed by integrating traditional home modification with smart home solutions. They viewed the program's strength as selecting and shaping solutions based on occupational demands, body functions, and home context, rather than “installing devices.” This approach reduced the level of physical assistance required and expanded opportunities for independent occupational performance. This was not about putting devices in the home, we first mapped where help was needed using the occupational profile, then combined home modification with smart functions to support doing more independently. (OT 4) We were not choosing devices from a catalog; we were asking what the client needed to do today, where that is blocked, and which combination of environmental modification and smart function would remove the barrier. (OT 2) Even when the same device went into two different homes, the occupational meaning was completely different. For one client a switch robot at the bedroom door was primarily a nighttime fall-prevention solution; for another, the same device was how she received guests independently when her spouse was at work — including a gas-meter-reader visit she handled alone for the first time. (OT 8)
Theme 2: Early Implementation Barriers were Manageable Through OT-Led Simplification, Alternatives, and Clear Role Delineation
OTs commonly encountered early barriers related to connectivity/configuration (e.g., Wi-Fi instability, pairing failures, app changes) and usability (e.g., fine-motor demands, unclear controls, multistep operations). OTs framed these barriers as mismatches among user capacities, task demands, and technology requirements. They addressed them by reassessing breakdown points, simplifying workflows (e.g., fewer steps, partial automation), using alternative solutions to meet the same goal, and providing error-prevention training. OTs also highlighted that clear role delineation—with OTs leading assessment, matching, training, and refinement, and technical issues escalated to support—improved feasibility in practice. The issue was not that the device “didn’t work,” but that it was too complex for the client's function and home context, so we reduced steps, used partial automation, and taught how to prevent common errors. (OT 1) Pairing failures and app updates looked like a technology problem, but once we restructured the operation, partial automation, fewer steps, a clearer visual cue, the same device became usable. (OT 5) Some barriers needed more than OT-led simplification. With one auto-door-closer installation, the family was so reluctant to ask us to return that they unplugged the device rather than report a recurring fault; we only learned about it during routine monitoring. The fix required bringing the manufacturer back to re-tune the motor strength and conducting a separate education session for the whole household — not just the user — before the workflow stabilized. (OT 9)
Theme 3: Coresiding Caregivers Extended Training and Reduced Disruption from Environmental Change
OTs reported that caregiver involvement functioned as an extension of training and promoted carryover into daily routines. Caregivers supported repeated practice, addressed minor problems before they led to abandonment, and helped users adapt to changes in the home environment without confusion. OTs described that caregiver participation reduced unnecessary service contacts by enabling basic checks and routine maintenance. When caregivers learned with the client, use became a routine, and small issues didn’t turn into discontinuation, so re-visits decreased. (OT 3) The caregiver became a second trainer: they repeated steps, corrected small mistakes in the moment, and called us only when the issue was real, so the intervention kept running between visits. (OT 6) Caregiver involvement was not always facilitative. In one household the caregiver feared frequent operation would break the smart curtain and actively discouraged the client from using it independently; the program only stabilized after a separate caregiver-counseling session in which we reframed independent operation as the clinical goal. Without that conversation, the device would have sat unused even though the user could operate it. (OT 4)
Theme 4: Perceived Benefits Extended Beyond Task Gains to Control, Stability, and Reduced Family Burden
OTs described psychosocial gains, including increased perceived control, reduced anxiety, and emotional stability. Even when task-level changes appeared modest, OTs considered improved predictability and reduced reliance on others as clinically meaningful outcomes that could influence quality of life and family interactions. It wasn’t only that one task improved, feeling “I can manage at home” reduced anxiety, and the home felt more stable and predictable. (OT 7) Clients often said “I can manage at home now” before any task metric improved, the perceived control itself was a clinically meaningful change, especially for anxious caregivers. (OT 10) The reported benefits did not always fit the “emotional stability” frame. For one client the strongest benefit was practical and even economical: “I don’t have to wait for anyone, and I feel I’m saving electricity.” For another, the meaning was a role reversal — when her caregiver came home, she could open the door for them with the smart lock, and she described it as something she could finally do for them again rather than always receiving help. (OT 3)
Theme 5: Sustainment Required Minimized Follow-up, User Self-Management, and a Platform-Based Support Pathway
OTs reported that long-term use was common, but intermittent revisits occurred due to predictable maintenance events: unplugged power, system resets after moving or smartphone changes, and sensor battery depletion. OTs emphasized time-cost efficiency and recommended minimizing follow-up intensity while strengthening self-management. They suggested a platform-based support pathway (e.g., checklists, FAQs, short guides/videos, step-by-step recovery instructions, remote contact routes) so users and clinicians could address common issues quickly. OTs proposed routing clinical decision-making and occupational performance training to OTs, while escalating pure technical issues (e.g., network/account/device configuration) to technical support (IT/research team/vendor) through a clear triage pathway. Most re-visits were not because the intervention failed, but because of predictable management issues, power unplugged, resets, battery problems, so a platform and triage pathway could reduce visits. (OT 10) The question was not whether it kept working, but who handles predictable maintenance, if we built a platform-based self-help path, clients could do the routine resets themselves and we could triage the rest. (OT 7) Not every re-visit was a predictable maintenance event. One household needed clinical re-engagement because a family member kept unplugging the auto door closer rather than reporting the fault; in another, a smart plug controlling a mood light flickered for four days because of a backend platform issue, and only an in-person re-pairing with the Heyhome app resolved it. These were not intervention failures, but they show that triage needs to separate hardware events, household-dynamics events, and platform-connectivity events. (OT 1)
Illustrative Case Vignette
To illustrate the cross-theme reasoning, we summarize one representative case drawn from the implementation records. A community-dwelling adult with a severe physical disability and limited upper-limb function, living with his parents in a Wi-Fi-equipped apartment and with prior experience operating mainstream IoT switches at home, identified two priority occupational goals: independent control of the front-door opening for visitors and reduced nighttime fall risk during indoor mobility (Theme 1). The OT delivered a tailored package combining a smart hub and smart switch for room lighting, a smart plug for computer power control, a smart lock paired with an accessible auto door closer, and a motorized curtain (Theme 1; Table 4). The lighting and lock components stabilized within the first week because the user already operated similar devices confidently, and the user reported reduced nighttime fall risk during bedroom mobility—a benefit beyond the original task framing (Theme 4). The auto door closer, however, presented cascading challenges: the door's lower undercut prevented full closure, and the close-time interval did not match the household's routine. Simplification within the OT scope was insufficient, and the vendor was re-engaged for a motor-strength adjustment (Theme 2). At Week 3, routine monitoring revealed that the user's father had unplugged the device because he was dissatisfied with how it sealed and felt apologetic about asking the team to return; the concealment surfaced only through the scheduled monitoring contact (Theme 3—caregiver involvement functioning as obstacle rather than facilitator). The OT then conducted a separate, family-wide education session, and by Week 4 all members of the household were operating the device confidently (Theme 3). At Week 10, the therapist rated the overall package as Good on appropriateness and effectiveness, and Fair on applicability for installation and configuration items because the door-closer event had exceeded routine clinical scope (Theme 5). The case illustrates how OT-led tailoring (Theme 1), barrier resolution beyond clinical scope (Theme 2), conditional caregiver dynamics (Theme 3), benefits beyond task-level outcomes (Theme 4), and triaged sustainment (Theme 5) jointly shape clinical utility in real community delivery.
Personal Goals Addressed by the OT-Led SHM Program and Implementation Frequency (n = 40).
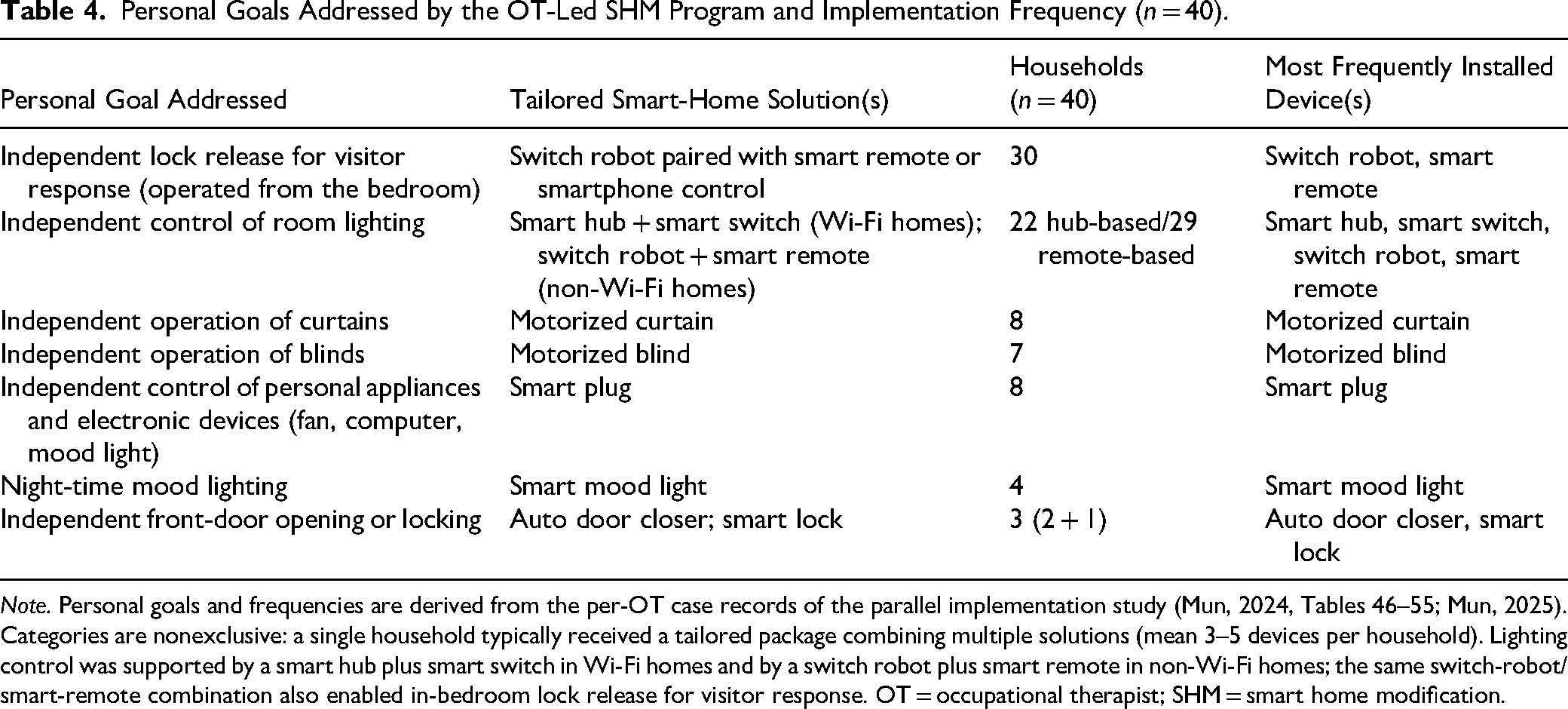
Note. Personal goals and frequencies are derived from the per-OT case records of the parallel implementation study (Mun, 2024, Tables 46–55; Mun, 2025). Categories are nonexclusive: a single household typically received a tailored package combining multiple solutions (mean 3–5 devices per household). Lighting control was supported by a smart hub plus smart switch in Wi-Fi homes and by a switch robot plus smart remote in non-Wi-Fi homes; the same switch-robot/smart-remote combination also enabled in-bedroom lock release for visitor response. OT = occupational therapist; SHM = smart home modification.
Integrative Summary: Linking Quantitative Ratings to Qualitative Themes
Triangulating the two data sets, the quantitative and qualitative findings converged on a coherent pattern. Items rated Good across appropriateness and effectiveness clustered around OT-led occupational profiling and integrated home-modification–smart-solution selection (Theme 1) and around user and caregiver training with iterative refinement (Themes 2 and 3). The two lower applicability items mapped directly onto qualitative explanations: budget planning (M = 4.6) was constrained by reimbursement and device-cost variability, which therapists described as an institutional rather than a clinical barrier, and automation scenario implementation (M = 5.4) was constrained by configuration complexity that therapists addressed through simplification, partial automation, and clear role delineation (Theme 2). Perceived benefits reported in interviews—including increased control, emotional stability, and reduced family burden (Theme 4)—were consistent with the high effectiveness ratings (M = 8.31) even when task-level change appeared modest, suggesting that clinical utility in this context is a multidimensional construct. Therapists’ recommendations for sustainment via platform-based self-management and triage (Theme 5) were framed as a service-design solution to the same maintenance burden that lowered applicability ratings on a small number of items. Table 4 summarizes how recommendations were translated into tailored device packages across the most common occupational goals in the 40 implemented cases.
Cross-Cutting Dilemmas, Novel Solutions, and Emergent Insights
Beyond the within-theme patterns, three cross-cutting findings emerged from the qualitative phase that the quantitative ratings alone could not surface.
Dilemma of household-level concealment. In multiple cases, families concealed recurring device problems out of consideration for the research team, with one family unplugging an auto door closer rather than reporting a fault. This dilemma reframes caregiver-only counseling as a distinct clinical task—not as an extension of user training but as a separate session in which the OT renegotiates the household's relationship with the device.
Novel solution: four-way triage of revisits. Therapists collectively described a triage logic that organized revisits into four event types: hardware events (e.g., switch-cover mounting failure), household-dynamics events (e.g., a family member unplugging a device), platform-connectivity events (e.g., a 4-day mood-light flicker resolved by re-pairing with the Heyhome app), and clinically necessary events. This four-way triage extends the conventional clinical/technical division and offers a service-design pathway for sustainable community delivery.
Emergent insight: practical and reciprocal dimensions of perceived benefit. Reports of benefit were not limited to the emotional-stability framing. Therapists also documented practical/economic accounts (“I feel I’m saving electricity”) and role-reversal accounts (using a smart lock to open the door for an arriving caregiver as a reciprocal action the user could finally perform). These extend the multidimensional construct of clinical utility (Smart, 2006) and complicate frameworks that privilege task-completion outcomes alone (Figure 2).
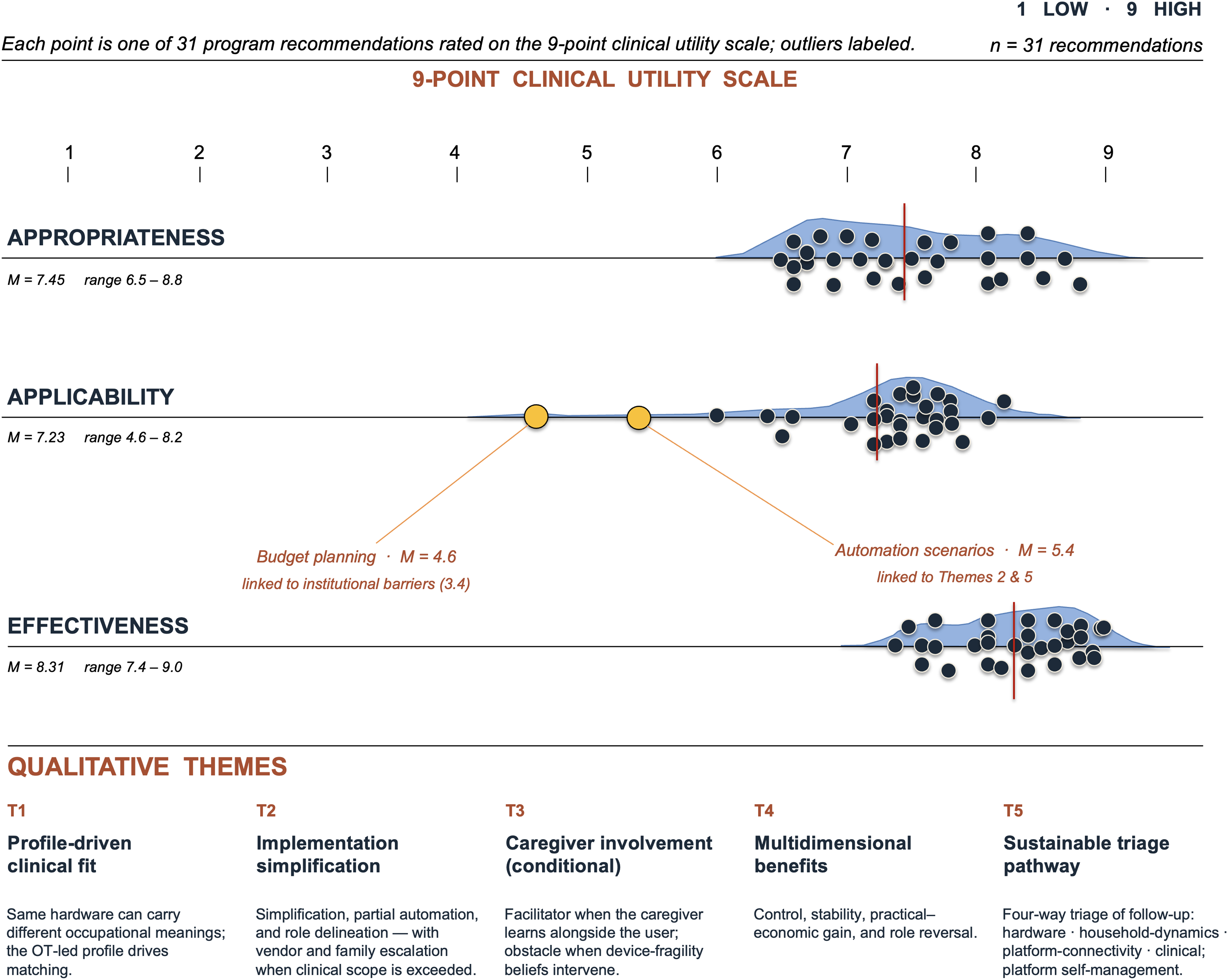
Mapping of five qualitative themes to mean clinical utility ratings across the three domains.
Discussion
This study evaluated the clinical utility of an OT-led SHM program using a sequential explanatory mixed-methods design. Overall, OTs rated the 31 recommendations as highly appropriate, applicable, and effective. Applicability was comparatively lower for budget planning and for developing/implementing automation scenarios, suggesting that feasibility constraints and technical complexity may limit routine delivery in some contexts. Qualitative findings explained these rating patterns and identified conditions that supported effective implementation and sustainment, including OT-led tailoring, caregiver-inclusive training, and a platform-based support pathway with triage.
Our findings lend support to prior work showing that smart home technologies can facilitate daily activity performance and safety (Ding et al., 2023; Mun et al., 2021). However, OTs emphasized that clinical utility did not come from “installing devices.” OT-led SHM is clinically useful when occupational profiling and functional assessment guide solution selection, home modification and smart solutions are integrated around real routines, and training/refinement occur in response to performance in context. This OT-forward process helps explain why most recommendations were rated as clinically useful in community practice.
Explaining Lower Applicability and How It May Be Addressed
Two recommendations, budget planning and automation scenario implementation, showed lower applicability. Budget planning appeared to be constrained by real-world costs, reimbursement pathways, and variability in service contexts. Automation scenario implementation was frequently described as technically complex and highly customized, which may reduce feasibility for routine workflows (Alzahrani et al., 2021; Dermody et al., 2024; Tian et al., 2024). OT-led SHM is clinically useful when complexity is managed through goal-prioritized selection and partial automation that reduces operational steps and cognitive load. This approach aligns with user-centered, iterative adaptation processes in technology adoption studies and may preserve clinical benefit while improving feasibility (Felber et al., 2024; Kim et al., 2020; Kokorelias et al., 2023).
Caregiver Involvement and Adaptation in Coresiding Households
OTs identified caregiver involvement as a key facilitator of adoption and sustained use, consistent with prior evidence. When caregiver participation is positioned as extended training, it supports carryover into daily routines (Dermody et al., 2024; Lee et al., 2024; Tian et al., 2024). When caregivers coresided, OTs reported less confusion related to environmental change and more consistent routine maintenance, which may help prevent minor issues from escalating into discontinuation (Dermody et al., 2024; Wei et al., 2023).
Sustainment, Service Efficiency, and a Platform-Based Support Pathway
OTs reported that long-term use was common, yet intermittent revisits still occurred. Revisits were often triggered by predictable maintenance events (e.g., unplugged power, resets after moving or smartphone changes, battery depletion) rather than failure of the clinical intervention. Sustainment was strongest when follow-up was time–cost efficient and emphasized user self-management for predictable issues. A platform-based support pathway could operationalize this approach by providing on-demand resources (e.g., checklists, FAQs, short guides/videos, step-by-step recovery instructions, remote contact routes). A triage structure is essential: OTs lead clinical decision-making and occupational performance training, while pure technical issues (network/account/device configuration) are routed to technical support (IT/research team/vendor).
Integrative Implications: Theoretical, Practical, and Policy Dimensions
Taken together, these findings contribute three integrative insights. Theoretically, they reframe SHM from a device-centered intervention to an occupation-centered service in which clinical utility emerges from the fit among occupational demands, user capacities, the home environment, and caregiver participation, consistent with person–environment–occupation frameworks (Christiansen & Townsend, 2011; Law et al., 1996). The observation that perceived control and emotional stability accompanied modest task-level change supports a multidimensional construct of clinical utility in assistive technology (Smart, 2006) and argues against outcome frameworks that privilege task completion alone. Practically, the study operationalizes a tailored, OT-led workflow that is replicable in community settings through a structured manual, clear role delineation between OTs and technical support, and caregiver-inclusive training. Lower applicability items (budget planning and automation scenarios) point to two concrete refinements: (1) a preimplementation budget template aligned with local reimbursement and device-cost ceilings, and (2) prevalidated automation scenarios packaged as tier 1 (single voice command), tier 2 (short routine), and tier 3 (conditional automation) to match user readiness and home context. At the policy level, the sustainment pattern documented here—predictable maintenance events rather than clinical failures—suggests that community care systems should recognize a distinct assistive-technology maintenance service line, supported by a platform-based self-management resource and a triage pathway, so that OTs’ time is reserved for clinical decision-making rather than routine resets. For Korea specifically, these implications align with the ongoing expansion of community care and public health center home-visit services, providing an initial evidence base for scalable, reimbursable OT-led SHM delivery.
Caregiver involvement should be assessed and addressed as a distinct clinical task—not assumed to be facilitative—because the qualitative data documented households in which caregiver beliefs about device fragility actively impeded independent operation; this finding strengthens the argument for caregiver-only counseling sessions as a reimbursable component of the service line.
This study provides clinically grounded evidence that an OT-led, manualized SHM workflow can be feasible and clinically useful in community practice. Beyond perceived utility, the study clarifies why certain recommendations may be less applicable and proposes practical strategies (partial automation, caregiver-inclusive training, and platform-based self-management with triage) to support sustainable delivery.
Several limitations should be considered. First, the therapist sample was small and drawn from community-based settings, which may limit generalizability to other contexts (e.g., hospitals, rural services). Second, qualitative findings relied on participant accounts, although credibility was strengthened through triangulation and an audit trail. Third, service efficiency outcomes (e.g., time saved, costs avoided, reduced revisits) were not directly quantified. Future studies should (1) test platform-based self-management supports and triage workflows, (2) quantify efficiency outcomes alongside clinical outcomes, (3) examine implementation across diverse service settings and populations, and (4) explore technology ecosystems that may affect feasibility (e.g., interoperability standards such as Matter and integration with social robotics).
Two further limitations follow from the present design. First, the clinical utility evaluation form is study-specific and tied to the 31 manual recommendations of the OT-led SHM program; psychometric validation across other manualized AT services is needed before the form can be used as a generalizable measure. Second, we used purposive convenience sampling because the eligible pool was limited to OTs who had completed the SHM training and delivered the program; selection bias toward early adopters of manualized SHM cannot be ruled out.
Implications for Occupational Therapy Practice
OT-led SHM is clinically useful when occupational profiling and functional assessment guide solution selection, training, and refinement in real-life routines.
Therapists can improve feasibility by prioritizing goal-critical functions, using partial automation to reduce operational steps, and providing error-prevention education tailored to users and caregivers.
Clear role delineation supports scalable delivery: OTs lead clinical decision-making and occupational performance training, while technical issues (e.g., network/account/device configuration) should be routed to technical support.
To reduce preventable follow-up, community services may benefit from platform-based self-management resources (e.g., checklists, FAQs, brief guides/videos, step-by-step recovery instructions) paired with a triage pathway.
Conclusions
OTs rated the OT-led SHM program as highly clinically useful. Clinical utility appeared strongest when OTs applied occupation-centered reasoning to integrate home modification with smart solutions, deliver context-based training, and refine strategies based on performance in daily life. Applicability barriers were primarily linked to feasibility constraints and technical complexity; these may be mitigated through goal-focused simplification (including partial automation), caregiver-inclusive education, and a platform-based self-management and triage pathway.
Footnotes
Author Note
For citation consistency, all self-citations by the first author appear under the romanization “Mun, K.”; earlier publications under “Moon, K. T.” refer to the same author. Two same-year self-citations are disambiguated as “Mun and Kim (2024a)” (Delphi survey) and “![]() ” (cervical spinal cord injury study) per APA 7th edition.
” (cervical spinal cord injury study) per APA 7th edition.
Acknowledgments
The authors thank the 10 occupational therapists and the 40 participants for their time and candor, and the collaborating public health centers and community-based rehabilitation institutions in Korea for supporting program implementation.
Ethical Considerations
The study was conducted after receiving approval from the Yonsei University Mirae Campus Institutional Review Board (approval number 1041849-202309-SB-163-03).
Informed Consent
Informed consent was obtained from all subjects involved in the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korean government (Ministry of Education; No. NRF-2022-NR071369).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available for reasons concerning the participants’ privacy.