
Abstract
Introduction:
Incident reporting systems are vital tools for enhancing safety, quality, and continuous improvement in biomedical and health care environments, yet they remain underdeveloped within biobanking, a sector characterized by complexity, high reliability, and multidisciplinary operations. This article addresses the implementation of incident management (IM) and corrective action/preventive action (CAPA) frameworks in biobanks, with a focus on minor- to mid-level incidents and nonconformities.
Methods:
We conducted a structured literature review using PubMed, Google Scholar, and ResearchGate resources and distinctive keywords or keyword combinations. Relevant articles were screened across biomedical, laboratory safety, and high-reliability domains. In addition, case studies from the literature and operational experiences in biobanks were analyzed, focusing on frequent but underreported incidents.
Results:
Findings indicate that robust IM and CAPA adoption align with the level of quality management system (QMS) implementation. Case studies highlighted the role of psychosocial factors—such as psychological safety, trust, and nonpunitive reporting—in addition to technical processes like root cause analysis. Effective IM is demonstrated to require more than formal structures; it depends on fostering psychological safety and a trust-based “Restorative Just” culture.
Conclusion:
We provide the first synthesis of challenges, best practices, and cultural adaptations for IM in biobanking. For the first time, our article provides a thorough synthesis of current challenges, best practices, and cultural adaptations needed to handle incidents, and also a practical toolkit consisting of clear definitions, incident categories, and an implementation guideline to develop efficient nonconformity management in biobanking.
Keywords
Introduction
Incident reporting schemes have become a cornerstone in efforts to enhance safety and quality across various health care and biomedical environments, including experimental and clinical laboratory premises.1–3 The development of these systems as a way to prevent major incidents is based on assumptions that date back to Heinrich’s injury triangle model. 4 The model presents two key assumptions. The first, referred to as the “safety iceberg” assumption, implies that for every major incident, there are numerous minor injuries and “near-misses.” The value of reporting near-misses remains a widely discussed topic in recent years, as these reports are expected to answer the who, where, when, what, why, and how of incidents, regardless of the sector in which they occur. 5 The second, known as the “identical causation” assumption, suggests that minor and mid-level incidents have the same underlying causes as major incidents. 4 By identifying and analyzing these smaller incidents, organizations can thus adopt a variety of strategies within the corrective action/preventive action (CAPA) framework to avert major accidents.
Despite the promising potential of incident reporting schemes for successful CAPA framework development, their implementation is challenged by several factors. Foremost is the trust in management’s fairness, which is essential for cultivating a work culture promoting quality and safety and for driving organizational progress.6,7 Irrespective of cultural diversity, the leadership’s role is critical in influencing employees’ safety practices and reporting behavior while avoiding excessive bureaucracy.8–11 Moreover, employees’ willingness to report incidents is essential, yet often withheld for other intra-and interpersonal reasons. The voluntary nature of reporting inherently leads to underreporting, influenced by personal relationships, the perceived severity of incidents, and whether they fall within the perceived percipient’s professional scope. 12 Minor- to mid-level incidents may also be underreported due to perceptions of their insignificance, causing severe frustration and fears of blame.9,12,13
Biobanks are considered highly reliable research infrastructures, characterized by multidisciplinary teams working across diverse domains (e.g., clinical, laboratory, informatics, regulatory, and quality assurance [QA]), and by complex organizational processes that require careful integration of human factors such as cross-domain communication, multilevel decision-making, and accountability, especially when managing incidents. Nevertheless, to date, there is a lack of evidence from the literature on the implementation of incident reporting schemes within the biobanking context.
Our article aimed to synthesize existing knowledge and draw parallels from related sectors and high-reliability organizations. To achieve this, we conducted searches in PubMed, Google Scholar, and ResearchGate using distinctive keywords and combinations, including: “incident”; “incident reporting”; “minor incident”; “common incident”; “incident management”; “corrective action”; “preventive action”; “CAPA”; “nonconformities”; “biosafety”; “safety culture”; “just culture”; “nonviolent communication”; “biobank”; “biorepository”; “biomedical research”; “research institute.” In addition, by presenting use cases from our own experience, our article seeks to foster discussion through proposing standardized definitions (Table 1), raise attention to the importance of managing incidents correctly, and offer practicalities in developing a generalized CAPA framework for the biobanking community. 1
Proposed Definitions to Standardize Incident Management Practices in Biobanking, Enabling Consistent Reporting and Knowledge Sharing
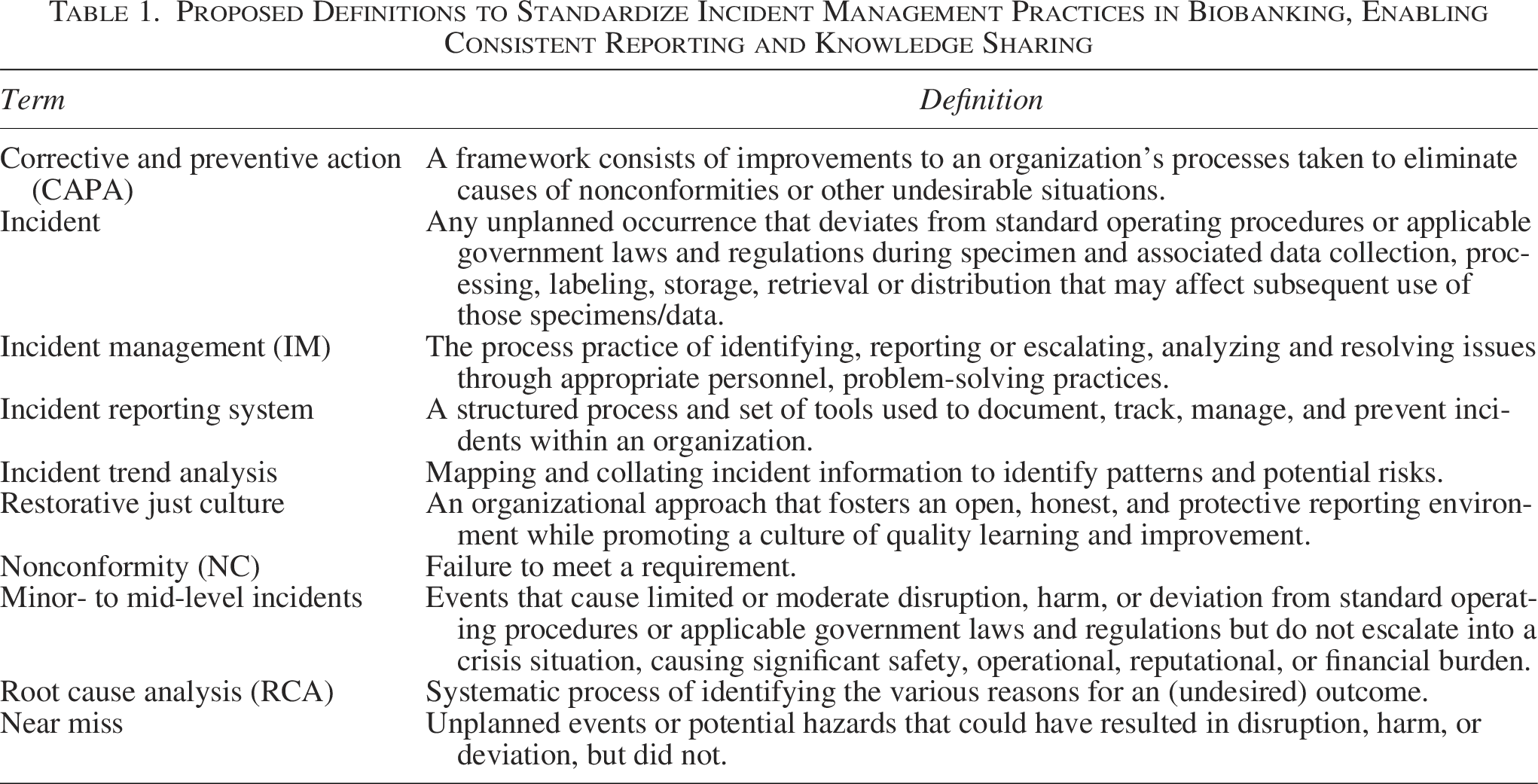
To clarify, this article focuses on minor- to mid-level incidents and nonconformities, excluding biobanking crises, disasters, and ethical issues. Although interlinked, concepts beyond the intended paper scope include crisis/emergencies, safety incidents (e.g., occupational health and safety), as well as patient or participant safety (e.g., medical and diagnostic errors; return of significant incidental findings).
Types of reportable incidents in biobanking: findings from the literature and personal experiences
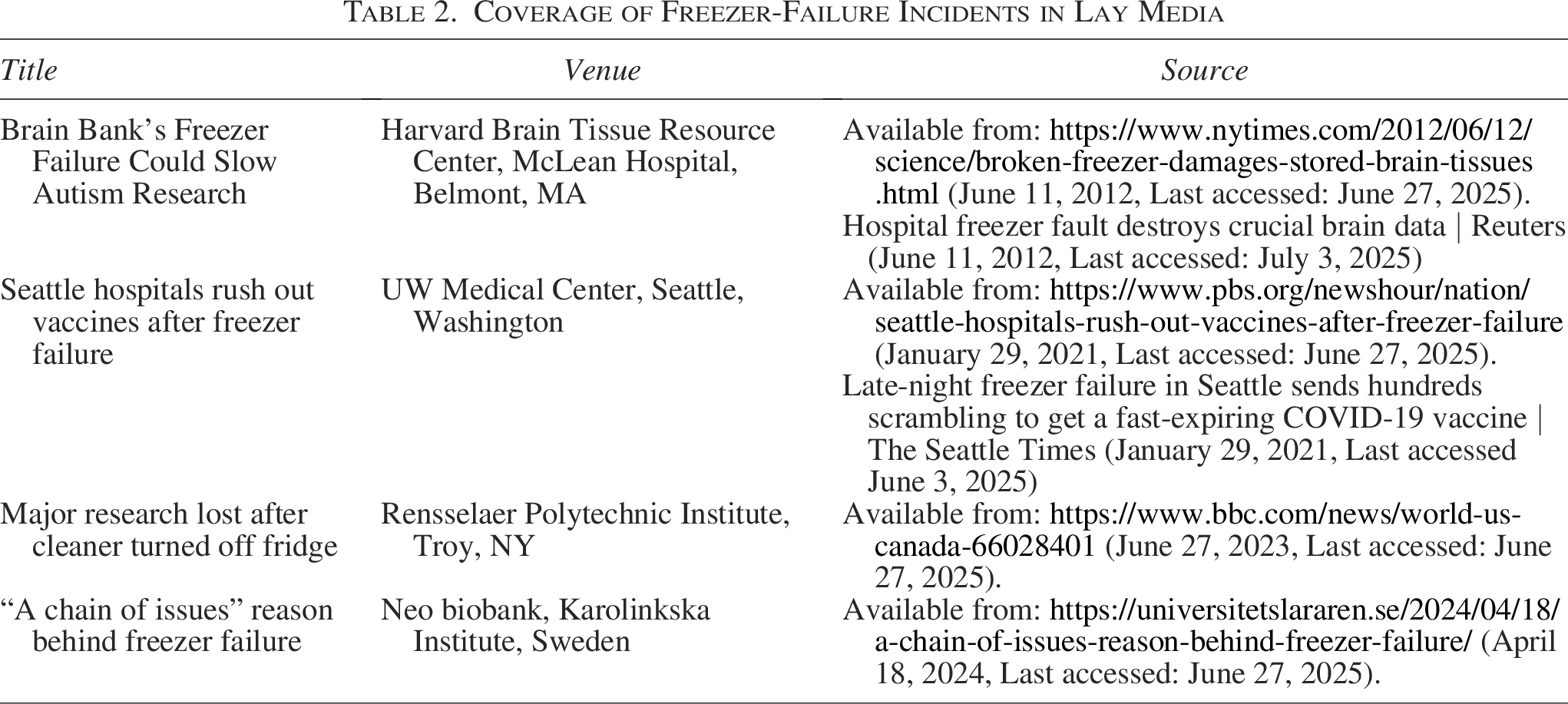
Not all common biobank incident types expected are well documented in the literature. Some of them arise more frequently, often linked to the need to document deviations from standard operational procedures (SOPs) 14 or improvements in practices following extreme disaster prompting preparedness (e.g., earthquake and tsunami/flood).15,16 Issues related to equipment failure and sample mislabeling are also more cited mid-level incidents; incidents related to data management, confidentiality, and safety are notably less discussed. Besides an overview of relevant incidents reported in the literature below, we listed biobanking incidents reported in mainstream media in Table 2. We provide an overview of frequently overlooked minor- to mid-level biobanking incidents and their associated risk categories based on our own professional experiences (Table 3). Additionally, recent use cases of real-world examples from the authors’ affiliated biobanks are presented to emphasize the importance of properly addressing such experiences.
Coverage of Freezer-Failure Incidents in Lay Media
Types of Common Minor- to Mid-Level Incidents in Biobanking, the Majority of Which Remain Underreported
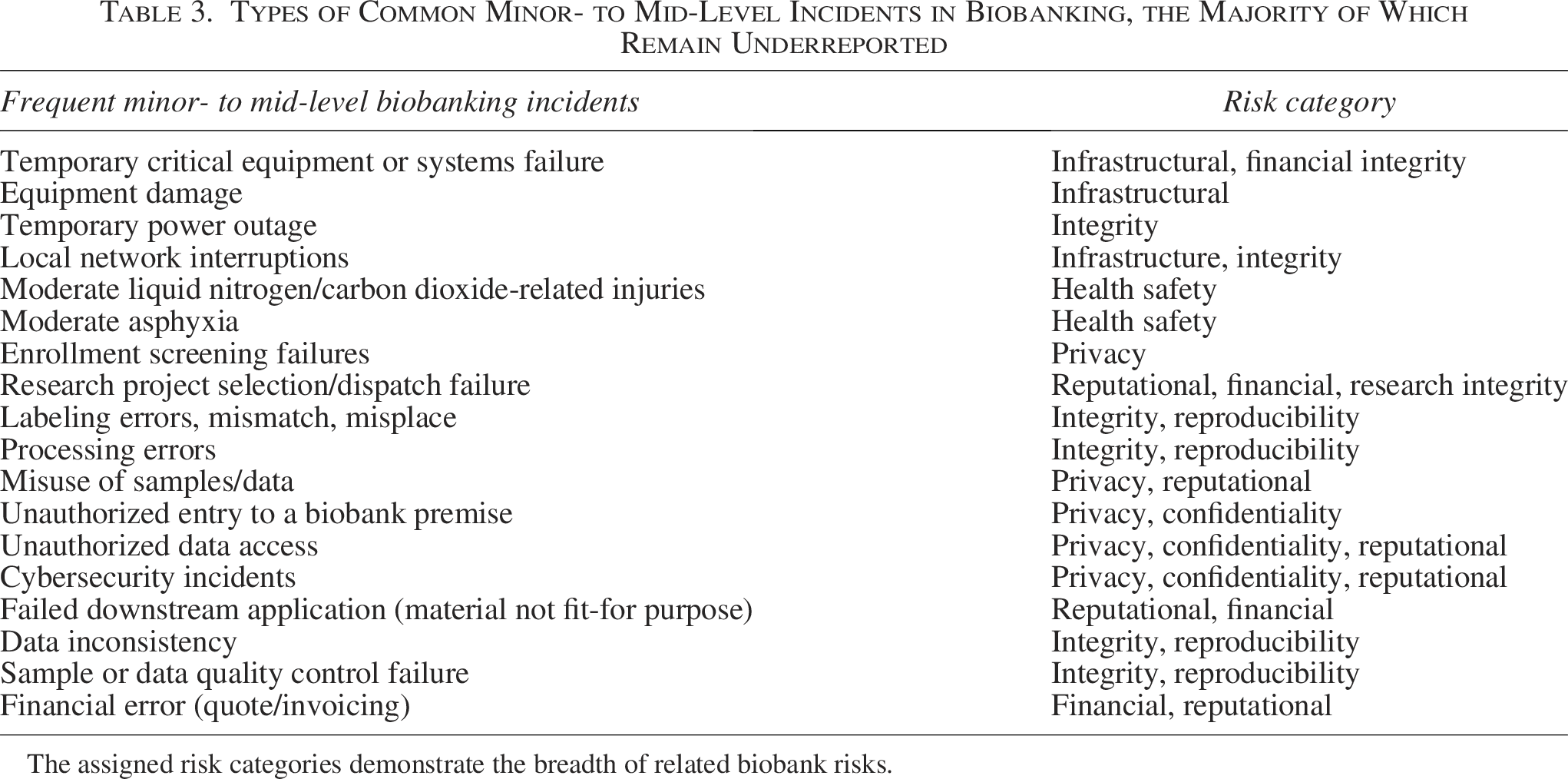
The assigned risk categories demonstrate the breadth of related biobank risks.
Freezer-related incidents
A typical mid-level incident scenario involves equipment failure or the loss of samples. Such incidents have been reported in the past as media news items (as listed in Table 2). Mainstream media provide some information on the root causes and actions taken. They refer to further investigation being done, as well as legal action. Only a few cases of freezer failure have been published as scientific papers, 17 or referenced in scientific papers. 18
Another notable example from the literature involving freezers pertains to sample mishandling, where samples were temporarily stored in an incorrect freezer. The report comes from a hospital-based Biobank in India, where tissues awaiting further processing were inappropriately stored at −70°C instead of +4°C, resulting in tissue damage, and making them unsuitable for the intended purpose. 19 The issue was subjected to a thorough root cause analysis (RCA), and a refresher training session was conducted for all the staff involved.
Freezer failure may have significant legal and financial consequences. Despite the fact that the extant data on this subject pertain to commercial biobanks, such as sperm banks, it is nevertheless applicable to research biobanks.20,21 Furthermore, such incidents have the potential to compromise the reputation of the biobank and the trust of donors and patients, thereby exerting a detrimental effect on the social dimension of sustainability. 22
Freezer failure serves as a prime example of process failures in general, which frequently go unreported. Tucker AL et al. classified process failures into two categories: problems and errors. An error is defined as the execution of a task that was either unnecessary or performed incorrectly and could have been avoided through the proper distribution of existing information. A problem arises when an employee is unable to perform a task. Either something is not available at the time of need, or location, condition, or quantity required. Or something is present that should not be, interfering with the designated task (e.g., missing Supplementary Data including SOPs). In both scenarios, the execution of the plan as intended is rendered unfeasible. Errors and problems represent a valuable source of information for identifying opportunities for improvement. 23 Transparent and efficient reporting systems support a culture of openness and learning within an organization. 24
Mislabeling
Further, frequent and underreported mid-level incidents in biobanking are mislabeling specimens or aliquots, with errors occurring at various stages of sample handling, or analysis. Two published case studies highlight their impact and the importance of reporting them for corrective measures to be taken 25 : In the Beaumont BioBank (Beaumont Health System, Royal Oak, MI), a routine audit revealed that plasma samples stored in white-capped vials had been incorrectly labeled as serum in the informatics system. The error was confirmed through a thrombin-clotting test, which distinguished plasma aliquots from serum. As a corrective action (CA), the samples were then accurately relabeled and returned to safe storage. During another incident at the same biobank, an entire set of samples was mislabeled due to an error in assigning the “BioBank Donor Alias.” Although donor-specific barcodes were correctly assigned, the alias duplication led to sample misidentification. The error was detected using a troubleshooting flowchart, and the mislabeled samples were subsequently corrected with the proper donor aliases and reintegrated into the inventory. 25
Safety
Regarding biological and chemical safety in biobanks, the same principles and regulations apply as in the laboratory safety realm, following the WHO Laboratory Biosafety Manual. 26 However, the number of publications on incidents that occurred in biosafety level −2, or 2+ laboratories—the biosafety containment levels of most human biobanks—or those which resulted in mild injuries are heavily limited. The need for consistent training on chemical and biological risks and preventive measures is critical, as is a trusting collegial environment to openly discuss all levels of safety issues, as revealed by several comprehensive survey projects.27–29
Confidentiality and data security
Data security and management incidents and their handling are expected to be a central focus in future discussions, particularly as the variety and frequency of data-related risks in academic environments and biomedical research continue to emerge.30,31 As data-sharing efforts and expectations grow with such initiatives as the European Health Data Space and International Open Science Clouds on the horizon, growing concerns about the confidentiality and privacy risks must be addressed with robust mitigation measures. Privacy-enhancing technologies (PETs) hold great promise to safeguard sensitive and super-sensitive data types and broaden their future usage, 32 although in many countries and biobanks, such advanced technologies are not available. Consequently, for nations with limited resources or a comparatively lower level of technological sophistication, the implementation of a systematic reporting protocol is imperative. The under-reporting of data breaches involving sensitive personal data is indicative of a general inadequacy in data reporting processes in these countries. 33 The importance of reporting and evaluating “near misses” in privacy and data handling matters will be an important strategy to reduce organizational risk in this evolving sensitive area of biobanking.
Scarcity of literature on biobanking incident management
Broadly, the majority of literature on incident management (IM) in biobanking is anecdotal and limited to a portion of the sample lifecycle, 34 presented as case studies informing recommendations, 23 examples of implementation of improved error-reporting systems, 35 or best practice development through a lessons-learned approach.15,16,36 The lack of literature on incidents in a biobank setting likely arises from fear of attracting reputation risk; insurance or financial vulnerability; informal reporting structures, fear of loss of trust; and perhaps even practices of under-reporting of minor- to mid-level incidents to management.
Anonymity in reporting may encourage individuals to share information without fear of reprisal, contributing to a more comprehensive understanding of potential risks. The implementation of reporting systems is indicative of an organizational commitment to transparency and openness, thereby cultivating a culture in which individuals feel empowered to communicate openly about safety concerns. 37 Investigating the willingness of health care professionals to report medical incidents found that organizational trust influenced this willingness significantly. The study concluded that establishing a “trust culture” is essential for improving incident reporting practices. 38 Research on corporate communication after cybersecurity incidents emphasizes the importance of transparency. A framework developed for effective corporate communication post-cybersecurity incidents suggests that transparent communication can mitigate reputational damage and reassure stakeholders. 39
Relevant use cases in biobanking
Use case 1: moderate-level incidents and their handling at the Hungarian Pediatric Oncology Network’s biobank
Background
The SCOPEDIS (Sample Collection of Pediatric Diseases) Biobank, which was established by the Hungarian Pediatric Oncology Network in 2022, supports global pediatric onco-hematology research through a quality-assured network of eight hospital collection and temporary storage sites across Hungary, along with a central long-term processing/storage facility. In 2024, the biobank experienced multiple mid-level incidents at different temporary storage sites located in different hospitals, involving ultra low temperature storage (ULT) malfunctions and failures of the ULT’s 24/7 centralized temperature-monitoring system. These incidents highlighted gaps in technical redundancy, off-hours response capacity, and formalized incident review procedures.
Scenarios and responses
Site A: Incident happened on July 13, 2024. The biobank manager received a “lack of communication” alert through the centralized phone application (corresponding with the “detection of nonconformity (NC)” step illustrated in the workflow in Fig. 1). The biobank manager confirmed −80°C freezer temperature on-site within 30 minutes (communication of NC occurrence and evaluation). Investigation of the incident (informal RCA) revealed no temperature signals were received from the ULT storing biobank samples for over 60 minutes due to a local area network failure after a storm-induced power outage, which disrupted the accessibility of the 0/24 temperature-monitoring system and triggered the alarm. Corrective actions (CAs) included ensuring individual access to a backup ULT and establishing an IT-support contact chain.
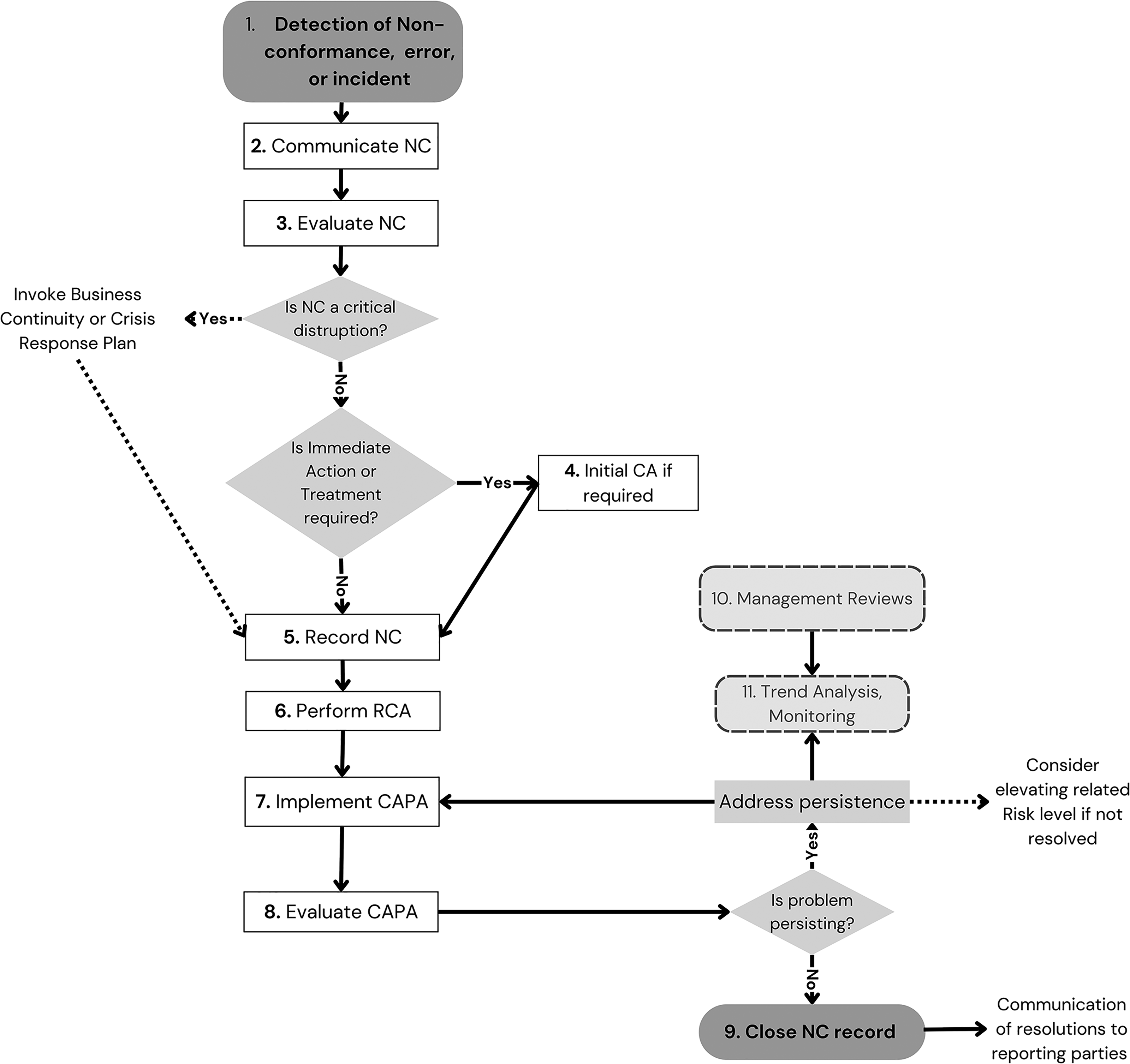
Proposed biobanking incident management process appropriate for implementation in a biobanking setting. Detailed explanatory notes are provided in Supplementary Table S1. CA, corrective action; CAPA, corrective action, preventive action; NC, nonconformity; RCA, root cause analysis.
Site B: Incident happened on July 24, 2024. The biobank manager received a “low temperature alarm” through the centralized phone application (detection of NC). NC evaluation showed that the −60°C threshold was exceeded. Immediate action was required for this critical disruption. Without a backup ULT on-site, the samples were transferred to another storage site within 1 hour 15 minutes (from the moment the alarm was received) using dry ice, which was only stored at the backup site. Investigation and RCA of the incident pointed out that the temperature rise was caused by a compressor failure, and that the emergency procedure could be improved. As a result, preventive action (PA) included adding a CO2 backup system to the storage equipment, dry ice supply maintenance on-site, and encouraging local colleagues to take part in the notification/response chain.
Site C: Incident happened on October 9, 2024. The ULT’s independent “low temperature alarm” was triggered on-site, and the biobank manager was immediately alerted by phone by local personnel (detection and communication of NC). The centralized phone application’s alarm, however, was not triggered. As the temperature had risen above −54°C, the samples were relocated to a backup ULT in another building belonging to the site within 25 minutes. However, the transport was done at +4°C, without using dry ice (immediate action, to be improved). RCA could not elucidate the cause of the missing alarm notification. PA included installing a second temperature sensor equipped with an alarm function that transmits alerts via a Wi-Fi or local network-independent mobile communication module, maintaining dry ice storage on-site, and repeating the local staff’s training related to responding to ULT “low temperature alarms.”
Site D: Incident happened on November 15, 2024. A ULT failure at a newly relocated site, not yet integrated into the 24/7 temperature-monitoring system, led to insufficient incident reporting and management. The ULT’s independent “low temperature alarm” was triggered, local site staff transferred the samples to another building’s backup ULT, using dry ice. The incident and the handling process were reported to the biobank manager hours later, with no written documentation. CA was to immediately integrate the storage unit into the temperature-monitoring system. PA included installing a second temperature sensor, securing the notification/response chain, and training staff in the appropriate, timely IM and reporting process.
Lessons learned
Ensuring individual after-hours access to ULTs and establishing documented notification/response and IT-support contact chains; Technological enhancement by introducing CO2 backup systems, continuous dry ice reserves, and second temperature sensors where needed; Encouraging and training local personnel, integrating them into the response protocols, with emphasis on proactive participation and proper documentation; Fast-tracked integration of all storage units, including replacements, into the central temperature-monitoring system. Installation of a second temperature sensor equipped with an alarm function that transmits alerts via a local network-independent mobile communication module.
Use case 2: implementation of central incident management capabilities at the Victorian Cancer Biobank, a hospital-integrated biobank network
Background
Established in 2006, the Victorian Cancer Biobank (VCB) is a consortium comprising a Lead Agency and five hospital tissue banks from across major Metropolitan Melbourne, Australia. Historically, the VCB has followed a harmonized approach to operations, with risk and contingency typically managed at a site level by two to four staff per site. In 2018, with the increased centralization of systems (access, central database, etc.), the governing strategic advisory body identified value in creating a multisite contingency plan. In response, the Lead Agency, recognizing the close relationship between risk, contingency, and IM, developed a central framework covering all three key areas.
Scenario
Key implementation steps taken over a 2-year period using low-cost software (e.g., Microsoft Excel) included:
Development of VCB Risk, Incident, and Contingency policies, adapting the Lead Agency’s established framework to fit a multisite arrangement. This included incident escalation levels/pathways and a simple communications Action Plan; Compiling a central, multisite risk register, with mitigations, risk assessment, and mapping of key responsibilities (including where shared across sites, or non-VCB employees, e.g. hospital IT personnel); Implementing central incident reporting and register, later streamlining with an easy-to-fill form (<5 minutes) and incident categorization; Commenced incident trend analysis and reporting; Delivered all-staff training in risk, contingency, and incident response, with interactive (mock incident) workshops based on real-world scenarios.
Challenges specific to implementing an incident reporting system in a biobank setting included building transparency and trust, achieved through confidentiality, impartiality, and process-focused RCA; improving efficiency of multisite (complex) RCA; integrating with local (hospital) reporting requirements; and providing feedback to staff in both real-time and sensitivities, providing benchmark feedback to VCB member sites.
The centralized approach has led to several benefits for the VCB Consortium:
De-escalation of critical concerns. For example, framework and training allowed effective, rapid multisite escalation and response to a hospital cyber threat incident, resulting in minimal stakeholder and equipment/specimen impact despite 5-week mandated IT downtime at one hospital site. Cross-pollination of CAPAs across sites where possible, including incorporating lessons learned in continuous improvement of the annual consortium-wide refresher training. Central visibility of average of n = 17 incidents per year (Ave n = 3 per site) Effective risk management, with central organization risks and mitigations informed by incident trends and data. Data-led strategic development and prioritization for effective continuous improvement.
Use case 3: analysis of IT-related nonconformities in the first year after implementing a Biobank Information Management System
Background
An oncology-focused biobank with four full-time equivalent implemented both its own QMS and a Biobank Information Management System (BIMS). In the first year after the implementation of both, all IT-related NCs (n = 15) were analyzed jointly (trend analysis and monitoring).
Almost half of these issues (n = 7, 47%) were errors made during manual entry of data. A third of the issues (n = 5, 33%) were errors originating from too liberal definitions of rules and workflows in the BIMS. The remainder of the issues (n = 3, 20%) were errors originating during data import from other databases.
Scenario
The issues were routinely managed according to the QMS as illustrated in the workflow in Figure 1.
After initial registration (detection and communication of NC), the direct mitigation of the problem consisted in all these cases of manually correcting the errors, either case by case or through export and reimport of corrected batch files (immediate action).
RCA was performed for each of the issues. For multiple CAPAs, similar root causes were found and demonstrated the value of trend analysis (Fig. 1). These were jointly addressed as follows:
Rules and warning messages were optimized in the BIMS (n = 5, 33%). Changing from labeling the vials with adhesive labels to structurally 2D-barcoded vials allowed the scanning of each container during each process step, and this facilitated more automated registration in the BIMS, thereby further reducing manual registration issues (n = 3, 20%). Support from the central IT services enabled interoperability with source databases within the parent institute and automatic import flows (n = 3, 13%). Good communication between departments ensured that the wishes of the biobank were taken into account when new IT systems were implemented (both for the department of Pathology’s Laboratory Information Management System and the hospital’s electronic patient file system; (n = 3, 20%). In addition, one issue was resolved through continued validation of the data flow, and one was resolved by adding an additional control step in the workflow.
After the implementation of CAPAs, their efficiency was checked (evaluation of CAPA).
Lessons learned
Overall, the systematic management of NCs supported the ongoing improvement of the BIMS and the related workflows after their initial validation and implementation. After initial mitigation of the issues, the root causes of the majority of the issues could be efficiently addressed within a year. Specific issues were identified as requiring a change in IT systems or workflows that were not under the direct control of the biobank. However, identifying the needs of the biobank with regard to this, and maintaining clear communication with the departments involved, made it possible to implement a sound solution when these systems reached the end of their lifetime and new systems were acquired by the respective departments.
Applications of incident management or corrective action/preventive action frameworks in biobanking
The effective application of the CAPA framework, following a systematic process evaluation of the quality of the sample process, provides insight into the expected CAs that may occur in biobanking. 34 A study of the data management practices of principal investigators demonstrated how auditing can improve awareness of data quality and uncover nonconformities for correction. 40
A QMS usually incorporates practices for noncritical IM or deviations. Evidence shows that a professionally organized structure or larger organizations are best for QMS implementation (e.g., BBMRI members, consortia members, health care or testing laboratory integrated). 41 Further, the use of well-established quality standards, which focus on customer satisfaction and continuous improvement (International Organization for Standardization [ISO], n.d.), allows for effective IM implementation also. 34 The role of IM, including nonconformity management, is not new to biobanking, 42 however, applications have progressively increased in recent years with standardized quality system implementation now increasingly common (e.g., quality systems compliant with ISO 9001, ISO 20387, ISO 17025, College of American Pathologists’ Biorepository Accreditation Program-CAP). The majority of quality systems provide requirements and guidance for IM with or without third-party certification or accreditation of such standards.43,44
Notwithstanding the existence of comprehensive crisis and critical incident frameworks 45 and the well-documented worldwide benefits of ISO 9001 and standardization, there is a paucity of literature describing a framework that synthesizes the concepts related to “undesirable outcomes” in biobanking, including IM, risk management, crisis management and disaster preparedness, together with ongoing continuous improvement, for biobank practice.
Best practices in incident management and CAPA for biobanking
It is widely accepted that the reliability of research depends on the quality of systems and products. However, performing in-house or collaborative research, or scientific assessment of a biobank’s product quality appears to be the most common tactic to improve a biobank’s output quality.46–48
This is likely due to the biobanking field still working to understand the fundamental impacts of biospecimen science on quality outputs. However, with the rapid rise in establishing robust quality control (QC) metrics,49,50 allowing wider adoption of standardization and QA in biobanks globally, the role of systematic IM and CAPA reporting will only increase. The recently published ISBER Best Practices (5th edition) outline practices and general interplay of IM and CAPA within a Quality Management Framework of a biobank, as follows
51
:
Establish a process for documenting nonconformities (i.e., deviations from established policies and procedures or defects).
Documentation and investigation of nonconformities (e.g., lost or damaged specimens, client complaints, adverse safety occurrences) using an incident reporting system to:
Facilitate RCA for the event. Identify trends based on operational components (i.e., failing equipment, bad lots of reagents or consumables, an inappropriate SOP). Prevent such episodes from reoccurring. The CAPA process is centered on the development, implementation, and documentation of actions to correct an incident when it has already occurred (CA) or to avoid the occurrence of an incident (PA).
These actions help leadership determine and implement the appropriate response to correct the initial undesirable situation. Repositories should utilize quality indicators as a way to measure the effectiveness of the QA program and have plans to address deficiencies that may arise.
Regardless of human or nonhuman (environmental) domains, the likelihood of adoption of robust IM and CAPA practices appears to align with the level of QMS implementation that a given biobank has achieved (or has reported in literature). For instance, an extensive seeds/horticulture biobank describes a central QMS, however, does not include a description of CAPA system. 52 While various RCA methodologies are common practice in industries such as medical/pharmaceutical, military, aviation (Five-whys, Fishbone Diagram, Bow-tie Method), the investigation of nonserious harm incidents is less common, although it can be achieved through various root cause methodologies and resourcing, 53 and where possible should be systematic and thorough for best long-term outcomes. 13 Throughout the literature reviewed, there was limited discussion on influences on reporting incidents in biobanking, despite this being a well-advanced discussion in health care 54 and other industries.
As digitization and data harmonization efforts increase, there is an emerging use of digital data QC tools and auditing to improve data workflow and interoperability, while also systematically unlocking data entry for CAs.40,55 These tools can automate incident reporting of common data management and noncompliance issues, such as human error, data input inconsistencies between networks, or customer complaints. 56 Use of IM in clinical (population) data registries has been somewhat described, including ethical, legal and social issues (e.g., review of invalid consent incidence), managing multisite or multinational data capture (e.g., number of discrepancies). 57
Furthermore, building strong incident records may open up opportunities for the application of system analysis techniques, such as through cross-sectional staff surveys, 58 or natural language processing and text mining for critical incident assessment, categorization, trend analysis, or assessing personnel/team reporting culture. 59
Considerations from adjacent fields: adaptations to sociocultural differences and integrating psychosocial safety aspects
Research suggests that fear of punitive actions is a major barrier to error reporting, and reporting rates fall in case of blaming, 60 while environments characterized by psychological safety enhance collaboration and innovation. 61 In the global action on patient safety report, WHO states that fostering a culture of openness around incident reporting is essential to support learning. 62 In the European Regulation EU 376/2014, the handling of incidents in aviation safety requires the implementation of a Just Culture to promote openness.
Psychosocial aspects are at play when reporting issues, and lessons can be drawn from research in adjacent fields such as speaking-up behavior in hospital settings 63 and the implementation of Restorative Just Culture across industries.64,65 In the restorative approach to Just Culture, the focus is not primarily on the rules, violations and their consequences, but rather on the impact of the issue on people and the responsibilities of those involved, working toward repair. Applied to biobanking, Restorative Just Culture helps to conduct the RCA in an open, nonpunitive way, which supports creative problem solving. It helps to focus on all involved stakeholders and processes and promotes responsibility. Table 4 provides an overview of the identified key points, which are elaborated upon below.
Key Attention Points Regarding Psychosocial Aspects in Incident Management
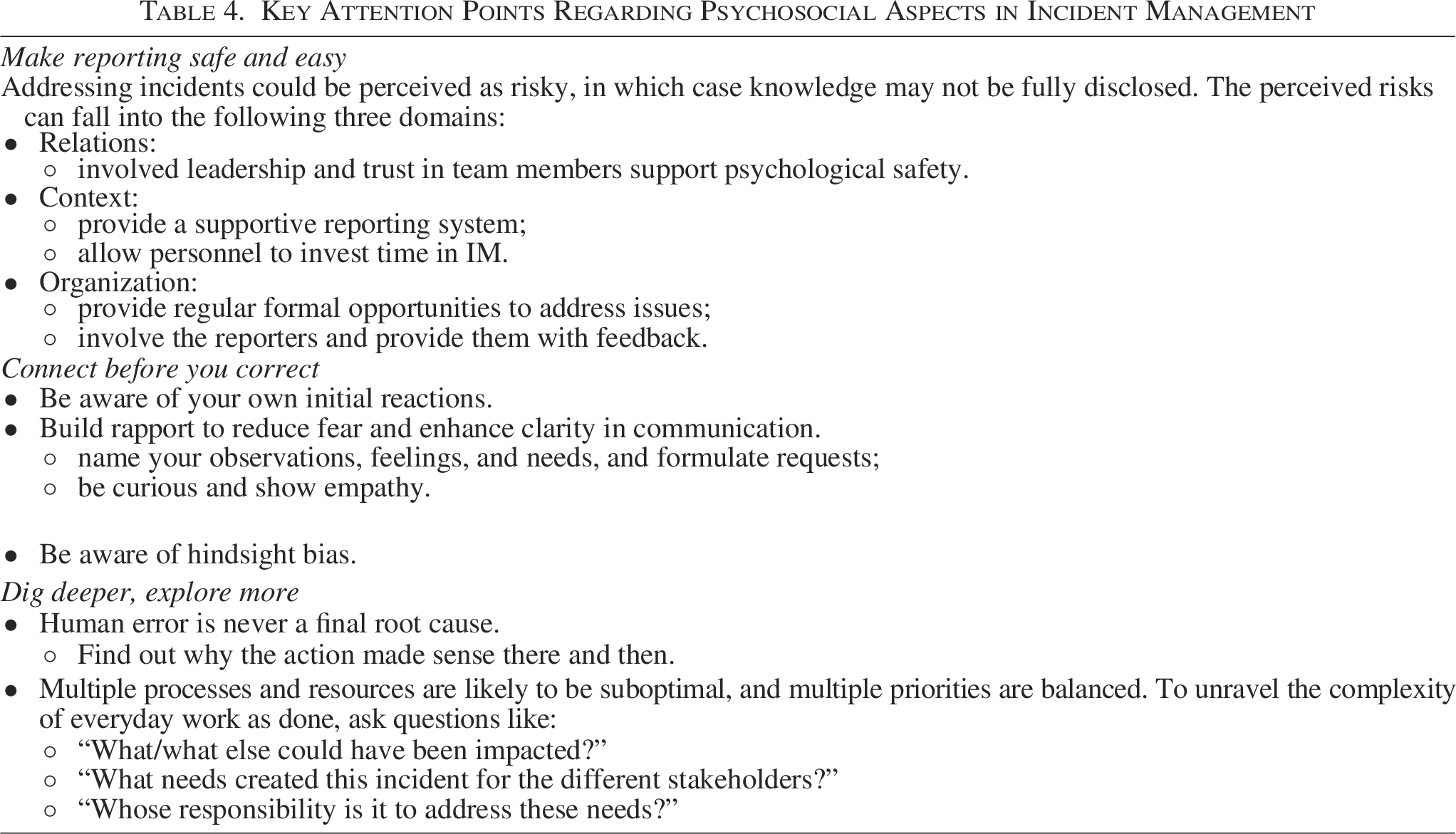
In general, addressing incidents could be perceived as risky. Negative consequences could be feared by those who address the issue, both toward themselves and toward their colleagues. People involved in the incident have valuable knowledge that may not be fully disclosed in case of suboptimal psychological safety. As a result, valuable opportunities for learning and improvement may be missed.
The implementation of tools for systematic incident reporting in the context of basic academic research is already demonstrated by the high popularity of the LabCIRS web-based, open-source software tool among the research community at Charité Universitätsmedizin Berlin. 1 However, as highlighted by a more recent publication in the Journal of Clinical Epidemiology, there remains a pressing need to extend such structured approaches to academic clinical research. 66 Initial concerns about a “culture of surveillance” that would stifle scientific creativity proved to be unfounded. 1 Focusing more on the quantity of incidents reported than on the quality of investigations and improvement actions can lead to a number of interrelated problems. Rather than being seen as a mechanism for data collection and analysis, incident reporting should be viewed as a process of participatory learning. 13
Make reporting safe and easy
Experiencing a power imbalance can add to the perceived risk, and perceptions of insufficient knowledge and competencies can add to this. Both positive and negative experiences of addressing issues in the past can modulate these individual factors.
Relational factors can include hierarchical differences as well as the presence and quality of the relationship. Addressing the root causes often involves the cooperation of others and other departments. Employee psychological safety allows collaborative problem solving and organizational learning. Leadership can facilitate this psychological safety by being available and involved, and by installing a culture of open communication without fear of retribution (e.g., when people raise awareness of a problem, they are heard and lessons are learned from the issue; language is constructive and supportive). Trust within teams is facilitated when staff members participate in mutual support (e.g., disagreements are resolved appropriately, personnel reciprocally help and support each other). In such an environment, personnel are more willing to take chances to contribute to continuous improvement. Involved and available leadership is essential here, as well as trust in team members. 67
Contextual factors can include the perceived severity of the problem, the presence of other people when addressing the problem, and the workload. Staff need to have the time to address the underlying causes of the problem, rather than implementing workarounds. 68 Ideally, report systems are voluntary, nonpunitive, and sufficiently protect confidentiality.
Organizational factors can include the institutional culture of the biobank, the presence of regular formal opportunities and systems to capture and address issues, and the explicit support of leadership to do so. In order to motivate personnel for continued reporting, it’s important to provide feedback to the reporters, to involve them in efficient improvement actions, and communicate evidence of change.
A biobanking use case demonstrates how the Lean Six Sigma approach to improvement resulted in the implementation of a user-friendly error-reporting module while empowering the biorepository staff to actively participate in CAPA management, and cultivate a culture of continuous improvement. 35
Connect before you correct
When a problem is addressed, the reception of the message is influenced by both the sender and the receiver. 69 Fear can be reduced and clarity enhanced by clear communication and building of rapport. We propose nonviolent communication (NVC) as a method to facilitate this. Originating from concepts in person-centered therapy, it has been applied in a variety of organizational settings to support mutual understanding and teamwork. NVC creates clarity by the separation of concepts28,65,70: the cluster of judgements, thoughts, strategies and demands is considered separate from the cluster of observations, feelings, needs, and requests. Conscious use of the latter elements promotes self-awareness, authentic expression, and empathic listening.
Learning about an incident can trigger initial impulsive reactions. Self-awareness and awareness of possible biases can support optimal RCA. 71
Empathy not only validates individual experiences but also fosters mutual respect and helps build rapport. Using this approach may facilitate psychological safety during error investigations and thus may remove barriers for thorough RCA.
Multiple biases may arise during RCA. Knowing the outcome and retrospectively analyzing how the event unfolded introduces a hindsight bias in understanding the event. Empathy allows for a better understanding of what the situation was at the time of the incident, and the unfolding of events. A thorough RCA is supported by tracking back far enough in space, time, management of resources, process inputs, and organizational environment.
Dig deeper, explore more
Human error (unfortunate decisions, inaccurate assessments, deviations from rules, etc.) is typically a symptom of a problem deeper in the operational setting. 72 Rather than considering human error as the conclusion of an RCA, much can be learned about the operation and organization by tracing the cause of human error back to the processes and resources handled. In such cases, RCA can be done by walking step by step back into the operational decisions, organizational conditions, and technology, and understanding why the issue unfolded the way it did, what input the stakeholder had, what multiple goals they were pursuing, what trade-offs were in play, and why it was logical for any human involved to act the way they did, unaware that their well-intended actions would lead to the incident. RCA can thus reveal why it made sense to them in their shoes, rather than to the person who analyzes the incident in hindsight.
Because of the systematic connection with suboptimal processes and resources, and the balancing of multiple priorities and goals, looking through the window of the issue into the everyday complexity of work as done provides an opportunity to learn and grow, and to prevent recurrence in similar circumstances. Valuable questions to ask include “What/what else could have been impacted?,” “What needs created this incident for the different stakeholders,” and “Whose responsibility is it to address these needs?”
Limitations
This article addresses a range of issues in IM, but there are some limitations. The literature uses different IM terminology, so relevant literature may be missed. This article offers defined terms to help address the value of IM/noncompliance in biobanking, as an emerging concept in the life science research sector, arguably undergoing a quality revolution. There is also a lack of reporting of IM in biobanks and repositories. This is especially true for minor- to mid-level incidents. Addressing this gap requires transparent professional discussion.
Application of IM and CAPA frameworks at biobanks varies due to disparate resourcing and expertise, varied maturity of QMS implementation, and institutional integration (leading to reporting elsewhere). This affects the comparability of practices and outcomes.
Further limitations may be attributable to the sociocultural and psychological barriers to incident reporting. These barriers are rather complicated to tackle efficiently, especially in settings where traditional hierarchical workplace dynamics and a lack of psychological safety act as a disincentive for open discussions about errors. The literature studied in this aspect pertains to related fields such as Restorative Just Culture and “speaking up” behavior in aviation and hospital settings. Mentions of these aspects in biobanking are sparse, 34 and further research is needed to establish to what extent they apply as well in the specific context of biobanking.
Finally, the consideration of the authors’ own experiences in managing various IM systems is provided to inform the recommended practices and contextualize the topic to biobanking. While use cases have been employed to illustrate certain points regarding effective IM, including in settings of limited resources, the authors recommend the implementation of future structured surveys of biobanks on this topic. The objective of such surveys would be to establish real-world data on the number and types of incidents, as well as the influences on capabilities to prevent or resolve nonconformities.
Recommendations and concluding remarks
Evidence from high-reliability industries, including offshore gas and oil production, nuclear power plants, and aviation, highlights the significance of fostering a culture that encourages the reporting of near-misses and incidents to enhance systemic safety and quality.5,73 In a similar vein, the implementation of a robust and time-efficient incident reporting system is of paramount importance for patient safety and the reduction of errors in medical diagnostics and treatments. Despite the intricacies of incidents and their management in these sectors, which give rise to their complex regulatory implications and are considered critical, valuable lessons can be learned from these established processes and are adaptable to biobanking without requiring any significant financial investment.
A step-by-step process for managing incidents is proposed for adaptation to biobanking (Fig. 1), with further descriptions provided in Supplementary Table S1. Complementary to this, our proposed definitions (Table 1) will guide consistent discussion and reporting of IM in biobanking.
A key IM implementation objective is to promote psychological safety, transparency, and to encourage system-wide reporting of minor and mid-level incidents. Furthermore, the goal is to enhance the overall organizational culture through better communication, psychological safety, and quality improvements.
For biobanks, especially those at varying stages of development or located in low- and middle-income countries (LMICs), the implementation of scalable and context-sensitive IM frameworks is essential. This includes the creation of modular toolkits that offer low-cost solutions for detecting, communicating, and reporting incidents, such as paper-based or simplified digital solutions, regular training sessions, and appropriate communication channels. These tools should be aligned with a CAPA process that facilitates RCA and team efforts, rather than individual punitive outcomes. Integration with existing quality management systems—whether based on ISO 9001, ISO 20387, or international “Best Practice Guidelines”—should be encouraged to facilitate structured follow-up and ongoing process optimization. What is more, systematic incident reporting is both feasible and valuable in these settings, even if it is implemented by basic digital tools which are presented in the paragraph below. Introducing simple reporting templates, prioritizing simple, yet robust process-control steps on the most common minor- to mid-level error-prone processes (such as sample-labeling and freezer maintenance), and embedding a culture of trust and transparency can serve as effective entry points. Over time, these approaches can be expanded into structured CAPA processes and aligned with international best practices.
Moreover, digital tools, where feasible, can further support incident-tracking and -analysis. Even basic digital systems (e.g., an Excel file with structured variables and categories, for which version history is documented in a SharePoint environment; a software that manages a database of CAPAs with an audit trail) can assist in identifying trends, facilitating audits, and monitoring long-term progress. As biobanks increasingly operate within complex, data-rich environments, the scope of IM must also address data governance and cybersecurity concerns.
Finally, the effectiveness of an IM system must be regularly evaluated. Metrics should go beyond counting reports and instead assess the timeliness and quality of CAPA actions, staff perceptions of psychological safety, and evidence of organizational learning. Feedback gathered from periodic staff surveys and audits can provide insight into cultural health and help guide future improvements.
To the best of our knowledge, this is the first article to systematically address the issues and possibilities of incident and nonconformity management/reporting in biobanking. To gain a deeper understanding of this important topic, conducting surveys or structured interviews is recommended to uncover best practices and challenges within more localized settings—such as specific regions of LMICs or newly established biobanks. This approach could also inform the exploration and development of both current and emerging biobanking tools, including the integration of large language models for RCA and trend monitoring, as well as digital tools/systems for incident reporting and process oversight.
Authors’ Contributions
E.T.: Conceptualization, data curation, methodology, project administration, visualization, writing—original draft, writing—review and editing. A.D.W.: Conceptualization, data curation, methodology, project administration, visualization, writing—review and editing. D.S-D.: Conceptualization, data curation, methodology, writing—original draft, writing—review and editing. S.H.: Conceptualization, data curation, methodology, project administration, visualization, writing—review and editing.
Footnotes
Acknowledgments
The Victorian Cancer Biobank through the Cancer Council Victoria as Lead Agency is supported by the Victorian Government through the Department of Health (VIC), Australia. The BBMRI.be Quality coordinator is financed by BELSPO as part of the B3-ISO project in the framework of the ESFRI-FED call.
Author Disclosure Statement
There are no conflicts of interest related to this article.
Funding Information
No funding was received for this article.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.