
Abstract
Introduction:
Polygenic scores (PGS) are used to investigate genetic predispositions for both medical and social traits. Their expanding application raises complex questions about data governance, societal impact, and research boundaries, particularly for biobank administrators who serve as custodians of the data enabling PGS research. Understanding the perspectives of biobank participants and the public on the development and use of PGS is essential for ensuring that governance and research practices align with participant values and societal norms.
Methods:
We surveyed participants from one biobank (n = 434) and members of the public (n = 1090) to assess perceptions of PGS research, with attention to differences by trait type (medical vs. social) and respondent category (biobank vs. public). Respondents received a brief explanation of PGS and examples of a medical and social trait. Using logistic regression models adjusted for sociodemographic and attitudinal variables, we examined support for PGS research, belief in its societal benefit, and comfort with personal data being used to develop PGS.
Results:
Trust in scientists was the strongest and most consistent predictor across all outcomes and respondent groups. The largest effect sizes appeared in attitudes toward PGS research on medical traits, with biobank participants showing an odds ratio (OR) of 3.26 (95% CI: 1.61–6.57) and public participants an OR of 4.60 (95% CI: 3.49–6.88). Biobank participants expressed greater endorsement of PGS for medical traits than public respondents, but both groups showed significantly less favorable views toward PGS for social traits.
Discussion:
Findings suggest that both groups, but especially biobank participants, hold clear reservations about applying genetic data to social outcomes. As biobanks increasingly support research beyond improving health outcomes, these results underscore the importance of transparent communication and participant engagement. Governance strategies must evolve alongside societal expectations to maintain public trust.
Introduction
Biobanks have become foundational to contemporary human genomic research, enabling large-scale studies that link genetic variation to a wide range of health and behavioral outcomes.1–3 Through the collection and storage of biological samples and data for use by researchers, biobanks are critical to the development of new instruments such as polygenic scores (PGS) (also called polygenic indices or polygenic risk scores). PGS, which have been created for a wide range of traits, estimate genetic predispositions to complex traits that are associated with multiple genetic variants.4–6 Biobanks provide large sample sizes that increase the statistical robustness and apparent generalizability of the genome-wide association studies (GWAS) that are used to create PGS.7–10
Most GWAS have focused on disease and biomedical traits,4,11,12 as has most PGS research. PGS for medical conditions such as cardiovascular disease, 11 type 1 diabetes, 12 and asthma 13 often aim to inform clinical prevention, diagnosis, and treatment.13–17 Conversely, PGS for social and behavioral traits (hereafter “social traits”) such as educational attainment, 18 risk tolerance, 19 and aggression 20 have primarily been intended for research purposes. Some have proposed using PGS for social traits in personalized education, akin to personalized medicine,18,19 which has garnered concern about the ethics of systematic screening for traits like educational attainment. 20 In fact, PGS for social traits are often met with apprehension and fears about possible misuse. 21 As research on the genomic influences on complex social traits continues to expand, biobank governance structures, such as data access committees, will face pressures to ensure that research aligns with the biobank’s mission and participants’ expectations.
Biobank participants play a central role in enabling PGS research, yet little is known about how they view the development and use of PGS. 17 Recent empirical studies have focused on the views of the public,22–25 patients, 24 students,26,27 and teachers27,28 on downstream applications of PGS in preimplementation polygenic screening22–24 and individualized education.26–29 However, understanding the upstream views of biobank participants and other members of the public on the development of PGS is essential for ensuring that biobank governance and research practices reflect participant values and societal norms. These two groups may differ in important ways: biobank participants may have greater familiarity with research processes and feel a stronger sense of investment or trust in science, while members of the public may approach these technologies with more skepticism or concern. The wide-ranging research uses of biobank data, made possible via the broad consent offered by participants, place obligations on biobankers to steward biospecimens and data to promote both scientific advancement and societal benefit, while upholding trust from biobank participants and the public. 30
This study presents findings from a survey designed to assess attitudes toward the creation and use of PGS for both medical and social traits. We focus on three core research questions: (1) How much do people support the development and use of PGS for these traits, and what factors influence their support? (2) How much do people believe these scores will benefit society, and what shapes those beliefs? and (3) How comfortable are people with their own genetic data being used to create PGS, and what influences their comfort level? For each question, we compare responses from biobank participants and members of the public, examining differences in attitudes toward medical versus social trait applications.
Our findings provide a baseline for understanding views on the expanding role of PGS in both clinical and social domains. They also offer insight into how these two key groups may perceive emerging uses of genetic data that expand beyond health research. Their perspectives are critical for informing biobank governance, public engagement, and policy development in ways that promote trust in science and support responsible biobanking.
Methods
Recruitment
Respondents were comprised of two distinct groups: (1) people enrolled in the Mayo Clinic Biobank (hereafter “BB respondents”) and (2) members of a public panel recruited through Qualtrics (hereafter “PP respondents”). For both groups, we aimed to recruit a diverse sample of adults with respect to gender identity, race and ethnicity, and age.
The two groups were recruited via different organizations. Personnel from the Mayo Clinic Biobank and from Qualtrics emailed potential BB respondents and PP respondents, respectively, with an invitation to participate in the study. The email included a brief description of the study and a link to the online survey. Recruitment for BB respondents occurred from September to November 2023, while recruitment for PP respondents took place from February through March 2024. The recruitment of the groups occurred nonsimultaneously due to both methodological and logistical considerations. Specifically, we added the PP group later in the study design to assess whether the perspectives of BB participants differed from those of the general population. Additional time was also needed to finalize ethics approvals, the sampling frame, and recruitment logistics for the panel.
The study was determined to be exempt from review by the institutional review boards of UNC-Chapel Hill, Mayo Clinic, University of Iowa, and George Washington University (i.e., the various institutions affiliated with the research team). Researchers from all four institutions were involved in survey development; researchers at UNC-Chapel Hill and Mayo Clinic led participant recruitment; and researchers at UNC-Chapel Hill and the University of Iowa conducted the data analysis.
Survey instrument
Survey questions were informed by existing literature on sociogenomics and public attitudes toward PGS for social traits25,31 and developed based on our study’s research questions. We piloted the survey instrument with members of the Mayo Clinic Biobank community advisory board and refined it prior to fielding. The survey included a range of items; in this paper, we focus on those related to attitudes toward PGS for social and medical traits, trust in scientists, genetic self-efficacy (GSE), genetic determinism (GD), and sociodemographic characteristics. The survey explained PGS for medical and for social traits prior to questions about attitudes toward their development and use (see Box 1).
Box 1. Survey text to explain PGS
Scientists have developed a new type of genetic testing that looks at small differences in a person’s genes. These small differences across many genes (“polygenic”) can be used to estimate a person’s risk of disease as lower, the same, or higher than the general population. This new type of testing results in a “polygenic score.” These scores might show that a person is, for example, twice as likely to develop diabetes when compared with other people of the same age and sex. However, while a high polygenic score for something like diabetes can estimate someone’s risk, it doesn’t mean someone will ever develop diabetes.
Scientists are now creating PGS for social traits, such as educational attainment or aggression. These scores for social traits are developed by combining genetic information and information about someone’s life, like their highest level of education or their lifestyle, eating habits, or exposure to pollution. However, questions remain about the accuracy and usefulness of these scores since both genetics and the environment can contribute to differences in social traits. PGS are often developed using information from biobanks. Biobank participants—or donors—provide blood samples and information about their lives (often through surveys), which biobanks share with scientists for their studies.
Outcomes
We examined three primary outcomes regarding PGS, each assessed separately for medical and social traits:
Support for PGS Research was measured by agreement with the statements “I support research on polygenic scores for [medical/social] traits,” using a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree).
Belief in Societal Benefit was measured by responses to “Overall, I think polygenic scores for [medical/social] traits would…” with options: benefit society, not benefit society, or have no effect on society. The variables for [medical/social] were dichotomized between those who believed in the benefit of PGS for society and those who believed they would have no effect or a negative effect.
Comfort with Data Use was measured by agreement with the statements “I am comfortable with my data being used to develop PGS for [medical/social] traits,” using a 5-point Likert scale (1 = strongly disagree to 5 = strongly agree). The variables were dichotomized between those who agreed/strongly agreed with being comfortable with their data used to develop PGS for [medical/social] traits and those who were neutral/disagreed/strongly disagreed.
Predictors
We examined three key predictors: GSE, GD, and trust in scientists:
GSE: We used an adapted six-item measure to assess confidence in understanding genetics, its relevance to health, and the ability to access genetic information. 32 Responses (1 = strongly disagree to 5 = strongly agree) were summed and modeled as a latent variable using Confirmatory Factor Analysis (CFA). The model demonstrated good fit (Comparative Fit Index (CFI) = 0.93), and the resulting GSE score was analyzed as a continuous variable.
GD: Respondents rated the perceived influence of genetics versus environment on an adapted set of 17 traits, including health conditions, intelligence, and personality characteristics. 33 Responses were categorized as only/mostly environmental, both, or only/mostly genetic. A GD score was generated using Item Response Theory.
Trust in Scientists: We created a three-item measure that assessed agreement with the following questions: (1) I trust scientists to think about the social implications of their research; (2) I trust scientists to think about the risks or harms of their research; (3) In general, I would trust scientists with my genetic information. Responses ranged from 1 (strongly disagree) to 5 (strongly agree) and were summed and modeled using CFA to assess the latent variable of individuals’ level of trust in scientists. The model demonstrated good fit (CFI: 1.00). The trust score was analyzed as a continuous variable.
Sociodemographic characteristics
The survey collected self-reported data on age, disability/chronic condition status, race/ethnicity, gender identity, education level, and political views.
Age was measured continuously using year of birth. Disability/chronic condition status was assessed with a binary item: “Do you identify as someone with a disability or other chronic condition?” For race and ethnicity, respondents were able to select more than one response among white, Black or African American, Hispanic, American Indian or Alaskan Native, Native Hawaiian or Pacific Islander, Middle Eastern or Northern African, Asian, or something else. Due to small sample sizes in some groups among BB respondents, race/ethnicity was grouped as Hispanic and/or Non-white, Non-Hispanic white, or multiple for analysis. For gender, respondents were allowed to select more than one among woman, man, transgender, nonbinary, or self-description. Similarly, due to small numbers in some categories, gender was treated as a binary variable (woman vs. man) for analysis. Education level was categorized as less than an associate’s degree, associate’s degree, bachelor’s degree, or graduate/professional degree. Political views were categorized for analysis as liberal (very liberal/liberal), moderate (slightly liberal/moderate/slightly conservative), or conservative (conservative/very conservative).
Statistical analysis
Descriptive statistics were used to summarize sociodemographic characteristics and the distribution of outcome variables (i.e., Support for PGS Research on both medical and social traits; Belief in Societal Benefit of PGS for medical and social traits; and Comfort with Data Use for PGS research on medical and social traits). Means and standard deviations were calculated for continuous predictors (GSE, GD, and trust in scientists). Differences between BB and PP respondents were assessed using independent samples t-tests for continuous variables and chi-squared (χ2) tests for categorical variables.
Adjusted logistic regression models were used to examine associations between predictors and each of the three outcomes, separately for medical and social traits. Statistical analyses were conducted separately for the BB and PP respondent groups, resulting in a total of 12 models. Each model was adjusted for age in years, education level, gender, race/ethnicity, disability or chronic condition status, and political views and included scores for GSE, GD, and trust in scientists as predictors. All analyses were conducted using Stata version 17. 34
Results
Study sample
A total of 467 BB respondents and 1122 PP respondents completed the survey (Fig. 1). Both samples were subject to analytic restrictions based on completeness of participant responses, and respondents who did not answer all outcome variables were excluded from the analyses (BB: n = 16; PP: n = 6). In addition, due to small numbers, respondents who reported a gender other than woman only or man only, or did not provide complete sociodemographic information, were excluded (BB: n = 17; PP: n = 26). The final analytic sample included 434 BB respondents and 1090 PP respondents.
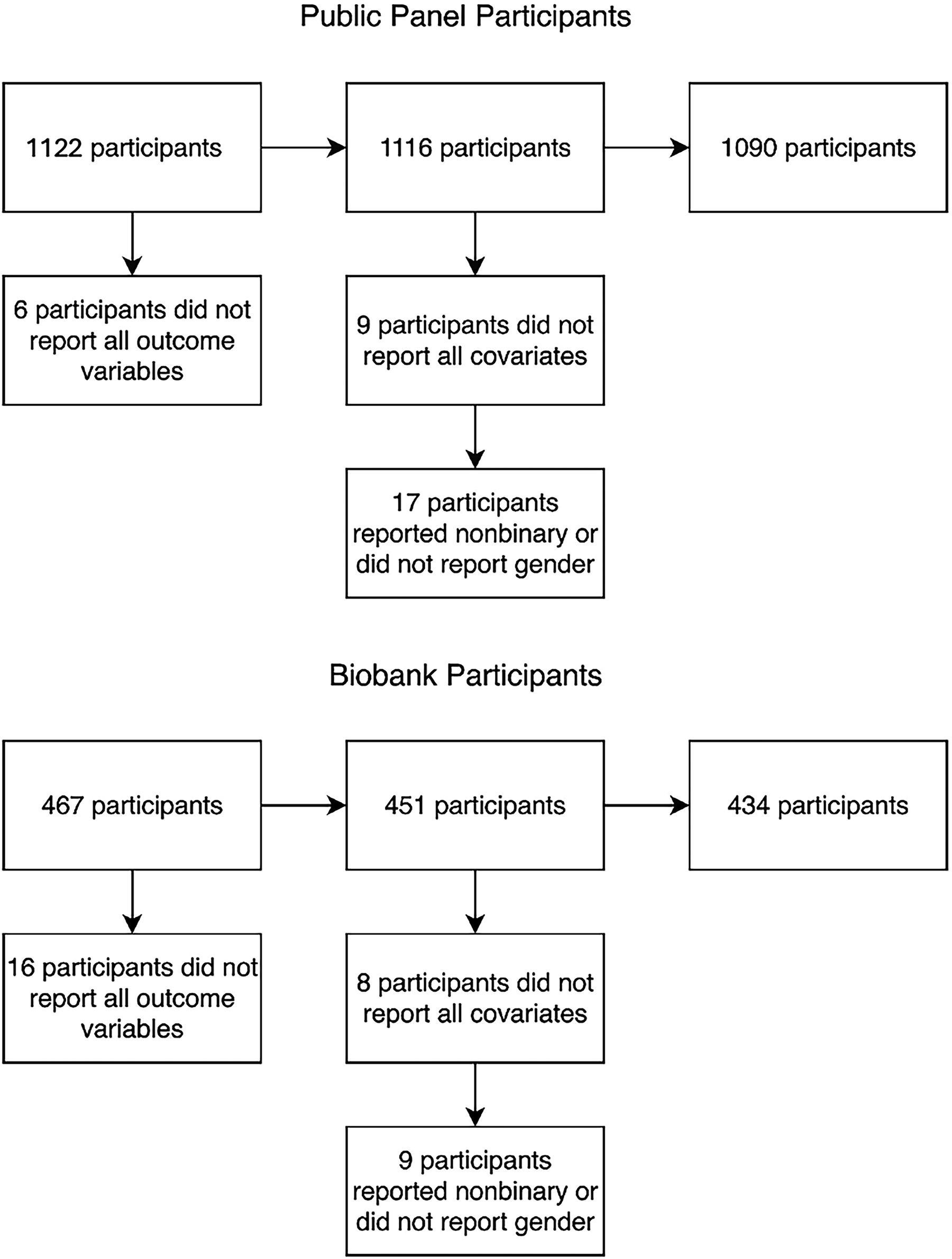
Flowcharts of respondents included in this analysis.
Table 1 provides an overview of the sample characteristics of each group. Statistical comparisons confirmed significant differences between the two samples across several demographic variables that are consistent with the underlying populations reflected in each group. BB respondents were significantly older, more highly educated, and more likely to report a disability or chronic condition. The PP sample exhibited significantly greater racial and ethnic diversity, although no significant differences were observed in gender distribution or political orientation. The mean scores for GSE, GD, and trust in scientists were all significantly higher among BB respondents compared with PP respondents.
Descriptive Analysis of Independent Variables
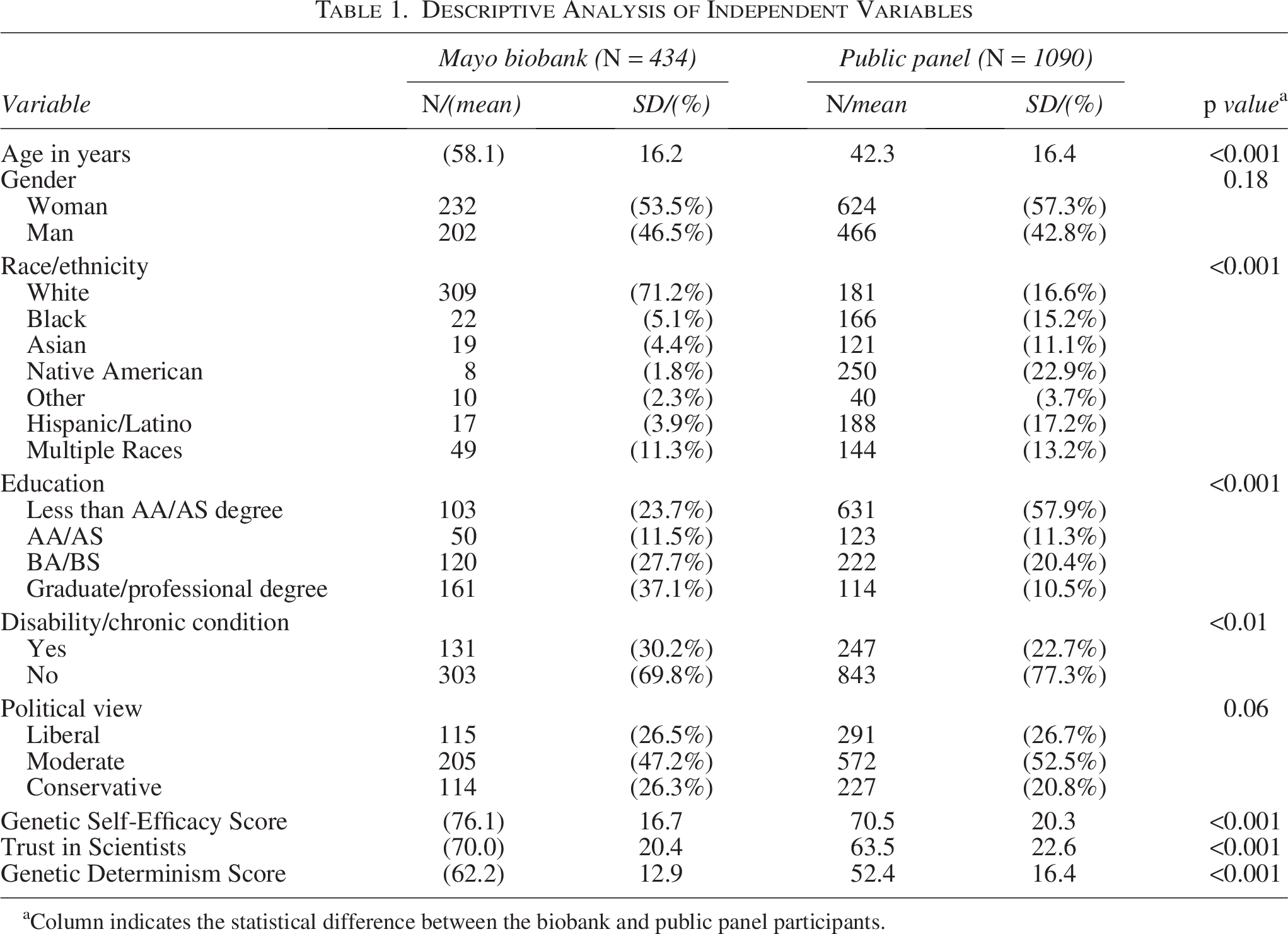
Column indicates the statistical difference between the biobank and public panel participants.
Descriptive differences in attitudes towards PGS for medical and social traits
Table 2 depicts the descriptive distribution of our outcome variables. A large majority of BB respondents (86%) supported research on PGS for medical traits compared with 64% of PP respondents. Support for PGS related to social traits was notably lower across both groups, with BB participants less supportive of PGS for social traits compared with PP respondents (BB: 37% vs. PP: 42%).
Descriptive Analysis of the Dependent Variables
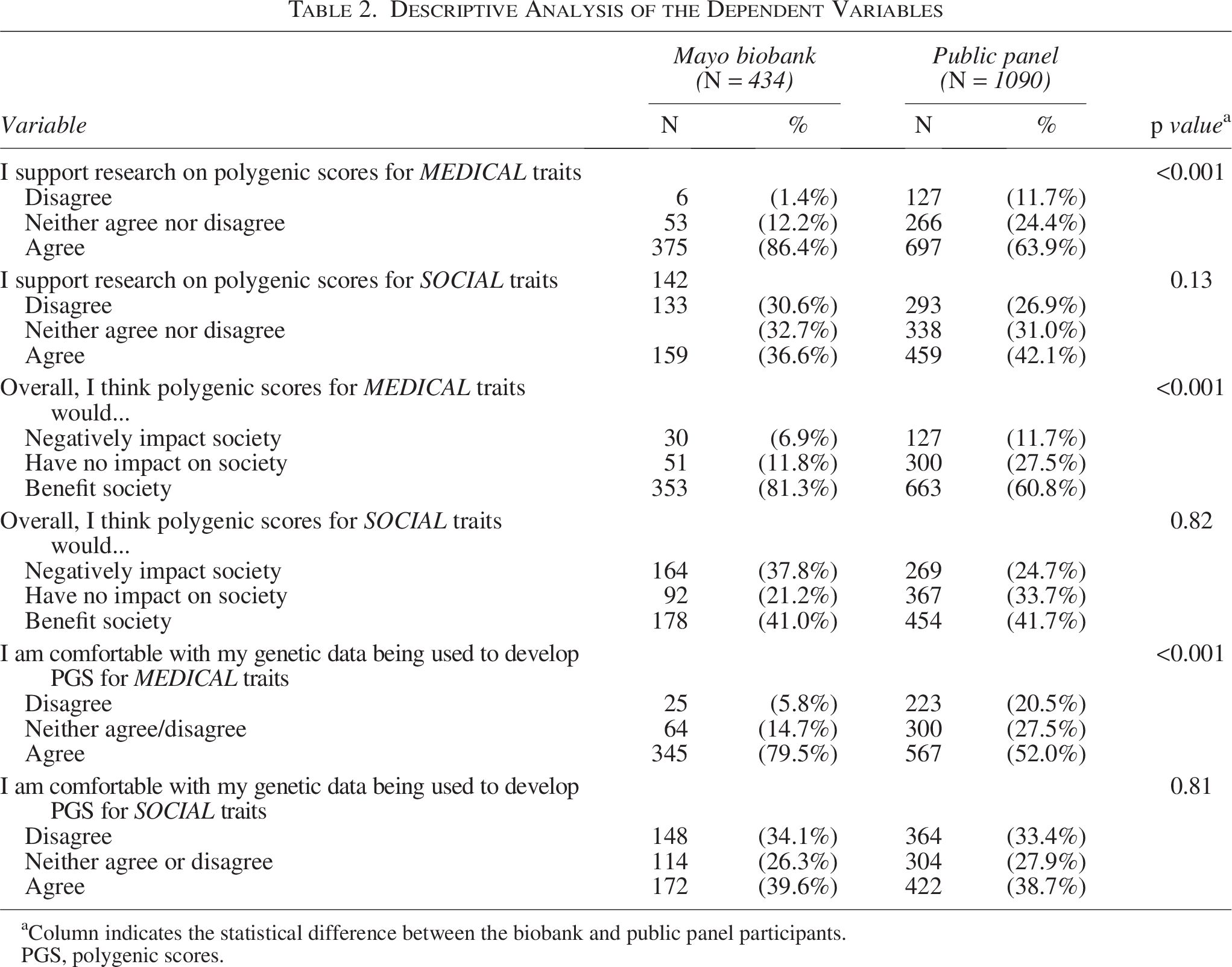
Column indicates the statistical difference between the biobank and public panel participants.
PGS, polygenic scores.
Over three-fourths of BB respondents believed that PGS for medical traits would benefit society (81%) versus 61% of PP respondents. However, only 41% of BB and 42% of PP respondents believed that PGS for social traits would benefit society.
Comfort with the use of personal genetic data being used to develop PGS for medical and social traits followed a similar pattern. Most BB respondents (80%) reported being comfortable with their data being used to develop PGS for medical traits, compared with 52% of PP respondents. However, when asked about the use of their data for developing PGS for social traits, only 40% of BB respondents and 39% of PP respondents reported being comfortable, with BB respondents again showing a more pronounced decline in comfort from medical trait PGS to social traits PGS research.
Support for research on PGS for medical and social traits
Table 3 shows the predictors of support for research on PGS for medical and social traits among BB and PP respondents. Trust in scientists emerged as the strongest and most consistent predictor across models for support in both samples. Greater trust was associated with significantly greater odds of supporting research on PGS for medical traits for BB participants (odds ratio [OR]: 3.26, 95% CI: 1.61–6.57) and PP participants (OR: 4.90, 95% CI: 3.49–6.88). Trust was also positively associated with support for research on PGS for social traits for both groups, although the effect was smaller than for PGS for medical traits (BB OR: 1.92, 95% CI: 1.12–3.28; PP OR: 2.68, 95% CI: 1.96–3.67).
Logistic Regression Odds of Support for PGS for Medical and Social Traits
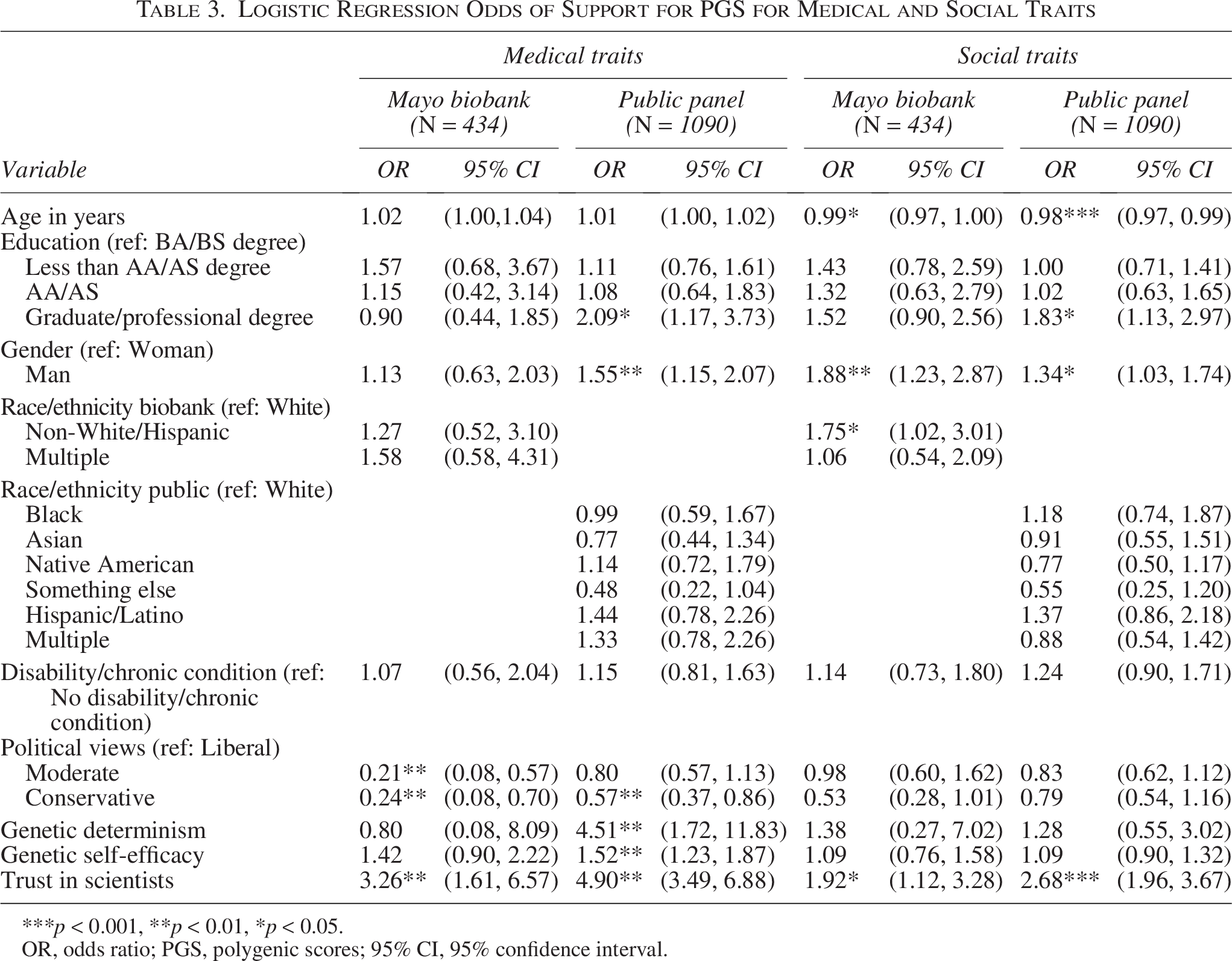
***p < 0.001, **p < 0.01, *p < 0.05.
OR, odds ratio; PGS, polygenic scores; 95% CI, 95% confidence interval.
Regarding age, among PP respondents, there was a significant, although small, negative relationship between age and support for research on PGS for social traits: for every additional year of age, the odds of support decreased by 2% (OR: 0.98, 95% CI: 0.97–0.99).
Education was a significant predictor among PP respondents. Compared with those with bachelor’s degrees, those with graduate/professional degrees had higher odds of supporting research on PGS for both medical traits (PP OR: 2.09, 95% CI: 1.17–3.73) and social traits (PP OR: 1.34, 95% CI: 1.03–1.74). No significant associations were found between education and support among BB respondents.
Regarding gender, compared with women, PP men had higher odds of support for research on PGS for both medical traits (PP OR: 1.55, 95% CI: 1.15–2.07) and social traits (PP OR: 1.34, 95% CI: 1.03–1.74). But among BB respondents, men only had higher odds of supporting research on PGS for social traits, with the increase indicating a more substantial difference between genders in the BB respondents (BB OR: 1.88, 95% CI: 1.23–2.87).
Race/ethnicity was significantly associated with BB respondents’ support of research on PGS for social traits. Compared with those who identified as non-Hispanic white, respondents who did not identify as white had higher odds of support for social traits (BB OR: 1.75, 95% CI: 1.02–3.01).
For political orientation, identifying as liberal for both samples was associated with higher odds of support for research on PGS for medical traits compared with those identifying as conservative (BB OR: 0.24, 95% CI: 0.08–0.70; PP OR: 0.57, 95% CI: 0.37–0.86). Among BB respondents, identifying as liberal was also associated with higher odds of support than identifying as moderate (BB OR: 0.21, 95% CI: 0.08–0.57), with the difference in support between liberals and moderates being even greater than that between liberals and conservatives. Political views were not significantly associated with support for research on PGS for social traits in either group.
Regarding GD and GSE, among PP respondents, higher GD scores and higher GSE scores were both associated with higher odds of supporting research on PGS for medical traits (GD PP OR: 4.51, 95% CI: 1.72–11.83; GSE PP OR: 1.52, 95% CI: 1.23–1.87). Neither predictor was significantly associated with support for research on PGS for social traits in either group.
Belief in positive benefit of PGS for medical and social traits
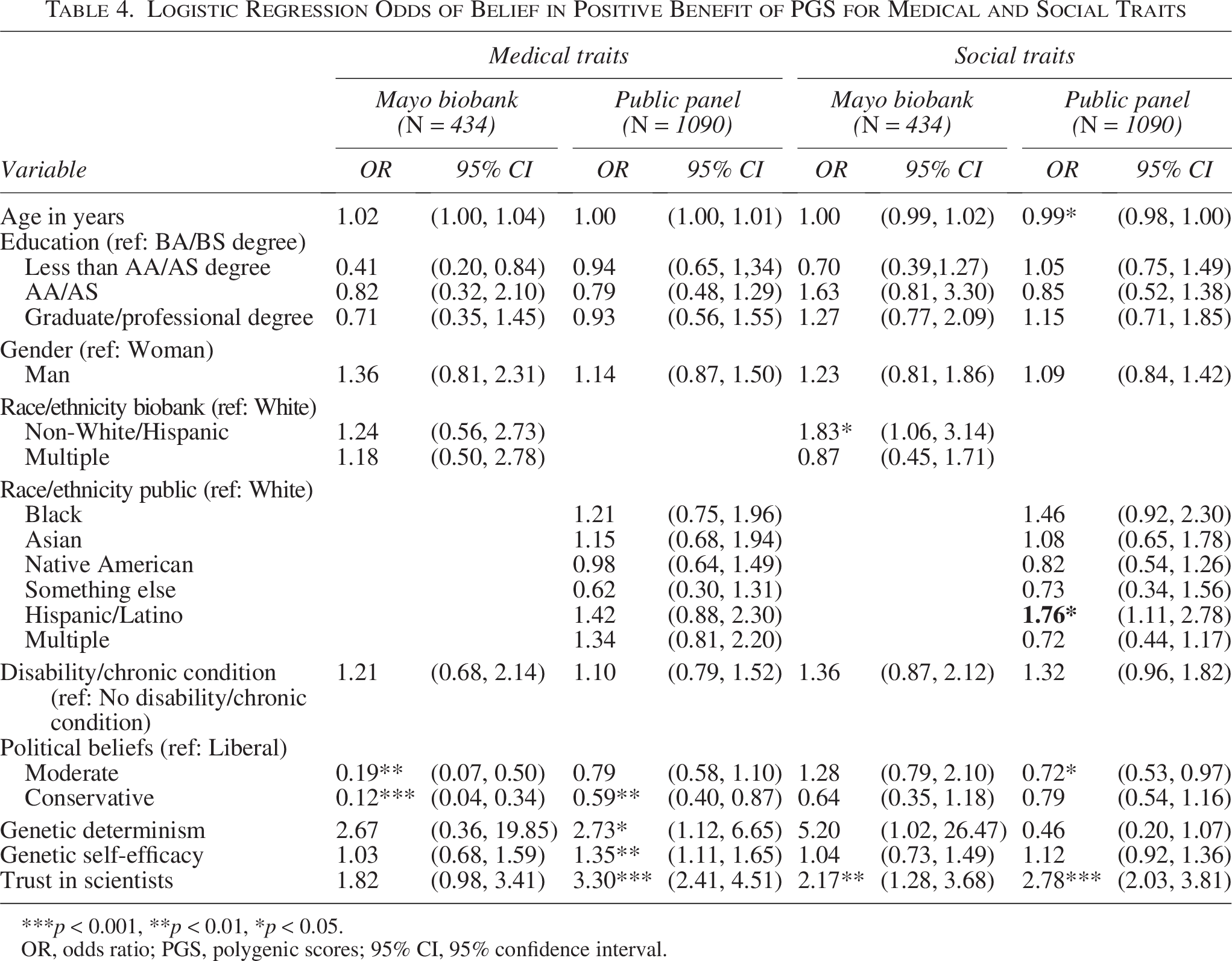
Table 4 displays the predictors of believing that PGS for medical traits and social traits would benefit society. Trust in scientists was a significant predictor of perceived benefit, particularly for PGS for social traits. Higher trust was associated with higher odds of believing that PGS for social traits would benefit society for both BB and PP respondents (BB OR: 2.17, 95% CI: 1.28–3.68; PP OR: 2.78, 95% CI: 2.03–3.81). For medical traits, trust was a significant predictor only among PP respondents (PP OR: 3.30, 95% CI: 2.41–4.51).
Logistic Regression Odds of Belief in Positive Benefit of PGS for Medical and Social Traits
***p < 0.001, **p < 0.01, *p < 0.05.
OR, odds ratio; PGS, polygenic scores; 95% CI, 95% confidence interval.
Political orientation was significantly associated with belief in the benefits of PGS for medical traits. BB and PP respondents who identified as liberal had higher odds of endorsing societal benefits compared with conservatives (BB OR: 0.12, 95% CI: 0.04–0.34; PP OR: 0.59, 95% CI: 0.40–0.87). Among BB respondents, liberals also had higher odds of endorsement compared with moderates (BB OR: 0.19, 95% CI: 0.07–0.50). For social traits, PP respondents who identified as liberal had higher odds of endorsing benefits compared with moderates (OR: 0.72, 95% CI: 0.53–0.97). But there was no significant association between political views and beliefs about the benefits of PGS for social traits among BB respondents.
Race/ethnicity was not significantly associated with belief in the benefits of PGS for medical traits. However, for social traits, BB respondents who identified as something other than white, compared with those who identified as white, had higher odds of believing that PGS for social traits would benefit society (BB OR: 1.83, 95% CI: 1.06–3.14). Among PP respondents, those who identified only as Hispanic had higher odds of believing PGS for social traits will benefit society compared with non-Hispanic white PP respondents (PP OR: 1.76, 95% CI: 1.11–2.78).
GD and GSE. Among PP respondents, both higher GD and GSE scores were associated with greater odds of believing that PGS for medical traits would benefit society (GD PP OR: 2.73, 95% CI: 1.12–6.65; GSE PP OR: 1.35, 95% CI: 1.11–1.65). Neither GD nor GSE scores were significantly associated with beliefs about social trait PGS among PP respondents. Among BB respondents, neither type of score was a significant predictor for either trait type.
Age was negatively associated with belief in the benefits of PGS for social traits among PP respondents. With every additional year, the odds of thinking PGS for social traits will benefit society were lower (PP OR: 0.99, 95% CI: 0.98–1.00).
Comfort in data use for PGS for medical and social traits
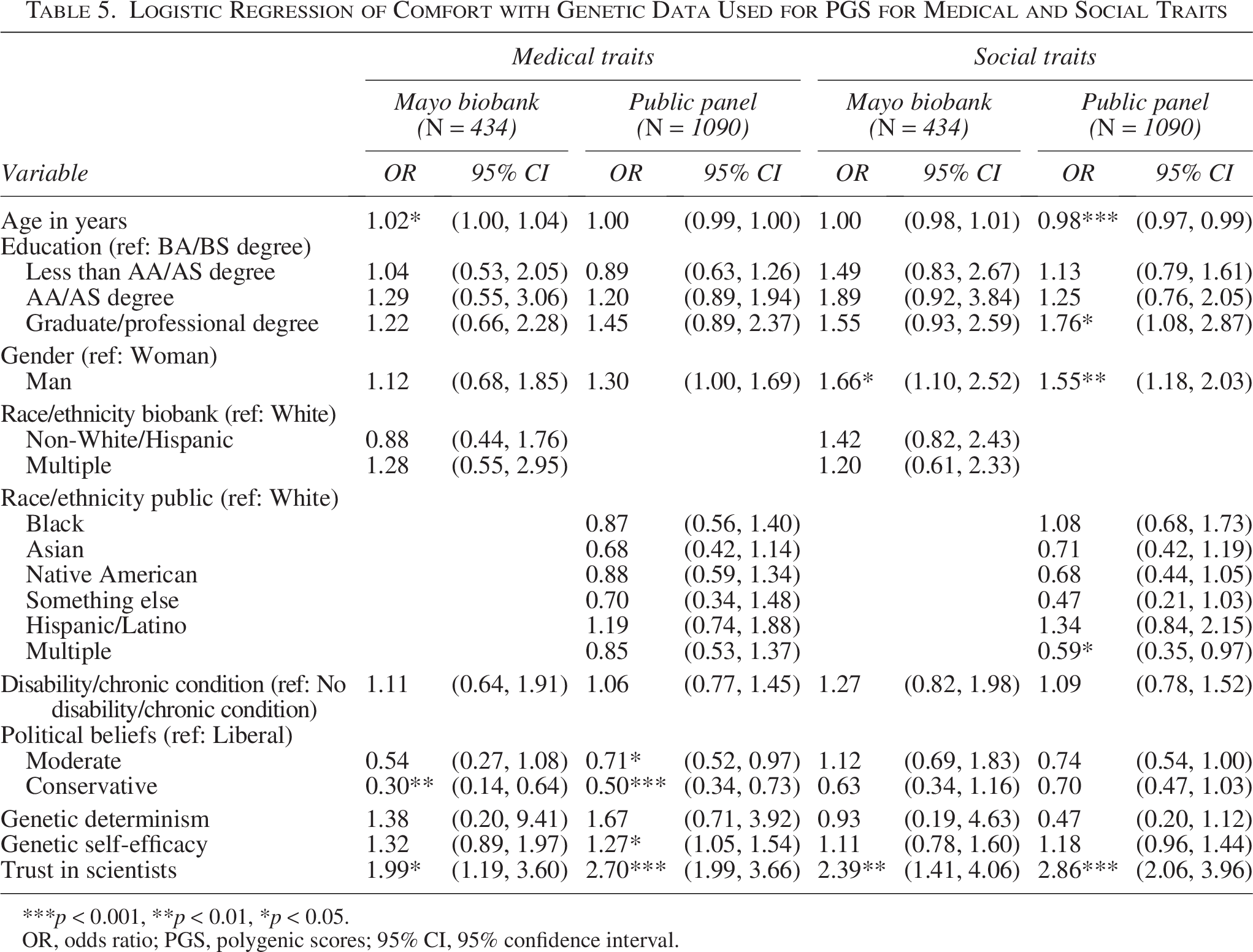
Table 5 presents the predictors of respondents’ comfort with the use of their own genetic data for the development of PGS for both medical and social traits. Consistent with prior models, for both groups, greater trust in scientists was associated with higher odds of being comfortable with use of one’s data to develop PGS for medical traits (BB OR: 1.99, 95% CI: 1.19–3.60; PP OR: 2.70, 95% CI: 1.99–3.66) and PGS for social traits (BB OR: 2.39, 95% CI: 1.41–4.06; PP OR: 2.86, 95% CI: 2.06–3.96).
Logistic Regression of Comfort with Genetic Data Used for PGS for Medical and Social Traits
***p < 0.001, **p < 0.01, *p < 0.05.
OR, odds ratio; PGS, polygenic scores; 95% CI, 95% confidence interval.
For political orientation, both BB and PP respondents identifying as liberal had higher odds of being comfortable with data use compared with conservatives (BB OR: 0.30, 95% CI: 0.14–0.64; PP OR: 0.50, 95% CI: 0.34–0.73). Among PP respondents, liberals also had higher odds of comfort compared with moderates (PP OR: 0.71, 95% CI: 0.52–0.97). Political views were not significantly associated with comfort regarding data use for PGS for social traits in either group.
Gender was significantly associated with comfort for social traits only. In both groups, men had higher odds of being comfortable with their data being used for PGS for social traits compared with women (BB OR: 1.66, 95% CI: 1.10–2.52; PP OR: 1.55, 95% CI: 1.18–2.03).
Older age was associated with higher odds of comfort with data being used for medical trait PGS among BB respondents (BB OR: 1.02, 95% CI: 1.00–1.04), but not among PP respondents. For social trait PGS, older age was associated with lower odds of comfort with data use among PP respondents (PP OR: 0.98, 95% CI: 0.97–0.99), but not among BB respondents.
GSE was positively associated with comfort among PP respondents to develop PGS for medical traits only (PP OR: 1.27, 95% CI: 1.05–1.54). GSE was not significantly associated with comfort for social traits among either group.
Education was a significant predictor among PP respondents for social traits. Those with graduate or professional degrees had higher odds of being comfortable with data use for PGS for social traits compared with those with a bachelor’s degree (PP OR: 1.76, 95% CI: 1.08–2.87).
For race and ethnicity, only PP respondents identifying with multiple categories had lower odds of being comfortable with their data being used for PGS for social traits compared with non-Hispanic white respondents (PP OR: 0.59, 95% CI: 0.35–0.97).
Discussion
This study contributes to the small but growing body of research on public perspectives of PGS.22–25,35 By including both biobank participant (BB) and public panel (PP) respondents, it offers a comparative analysis of perspectives on the development and use of PGS from those who contribute genomic data and those who may be affected by its downstream use. Across both medical and social traits and across all outcomes, trust in scientists emerged as the most consistent and powerful predictor, significant in every regression model. Although political orientation, gender, education, and age were associated with specific outcomes, none were as consistently associated as trust in scientists. These findings highlight the importance of engendering and maintaining trust, especially if researchers intend to use biobank data for PGS studies on traits that are less clearly aligned with traditional health research goals.
Despite demographic and attitudinal differences between the BB and PP groups, including age, education, race/ethnicity, trust in scientists, GSE, and belief in GD, both groups expressed low endorsement of PGS for social traits, particularly when compared with their views on PGS for medical traits. This suggests that both groups perceive meaningful distinctions between medical and social traits and may be more skeptical about using genetic data to predict social outcomes. These distinctions may reflect concerns about fairness, misuse, or the broader implications of labeling people based on genetic predispositions for complex social and behavioral traits. It is perhaps unsurprising that BB respondents, who contributed their genetic biospecimens and associated data for research, were significantly more likely than PP respondents to endorse PGS for medical traits across our three outcomes of interest. However, their stronger endorsement, coupled with being more trusting of scientists, makes their sharp drop in support of PGS for social traits particularly important for biobankers adjudicating data access to consider.
In addition, the ambiguity of what constitutes a medical versus social (or behavioral) trait reflects a broader challenge for biobank governance. As biobanks consider proposals for PGS research, they will face difficult questions about what qualifies as health-related research and how to align data use with their organizational missions. These decisions may be especially complex for biobanks that were established with a specific clinical or health-focused objective.
Although our findings suggest that BB participants are distinct in their views, we cannot assume that all biobank populations are homogenous. The Mayo Clinic Biobank does not focus on a particular disease, and participants were recruited regardless of health history; responses may differ among participants in biobanks focused on specific conditions. Furthermore, respondents in this study responded to the survey via an email from Mayo Clinic Biobank personnel, suggesting a relatively high level of awareness of their enrollment in the biobank. But knowledge of biobank participation varies widely across biobanks: individuals may not recall consenting, may not have been explicitly informed, or may not fully understand how their data are used.36,37 These factors may dramatically impact perceptions of PGS. In fact, the views of PP respondents in our study may better reflect how biobank participants who are unaware of their participation may view PGS for medical and social traits. Consequently, it is important for biobankers to consider not only the perspectives of biobank participants but also those of the broader public, whose views may be shaped less by direct experience and more by limited awareness, media portrayals, and social norms about genetics, privacy, and data use.
This study has limitations. While a key strength is the dual-sample population design, the descriptive differences between BB and PP respondents raise important questions about generalizability. BB respondents were predominantly non-Hispanic white, older, and highly educated, which is consistent with the demographics of Mayo Clinic Biobank participants. 38 Historically, biobanks have struggled to enroll diverse populations, which results in limitations for numerous biobank-enabled research studies. Future research should explore attitudes toward PGS in more diverse biobank cohorts, such as the All of Us Research Program. 39 Our findings also reflect the views of a U.S.-based sample; international perspectives may differ given global variations in trust in science, privacy norms, and the governance of genetic data. Finally, we used a binary measure to identify participants with disabilities or chronic conditions, limiting our ability to capture variation in type, severity, or lived experiences. This may have masked important differences in how individuals interpret PGS, which should be a focus of future research.
Our survey also included a brief explanation of PGS, with examples of diabetes and educational attainment to illustrate medical and social traits, respectively. However, we did not provide a standardized list of traits, which may have introduced variability in how respondents interpreted these categories. The GD measure, which asked respondents to rate the perceived genetic versus environmental influence of 17 traits, appeared earlier in the survey and may have shaped later responses about PGS use in unintended ways. Future research should consider how trait framing may influence responses.
Conclusion
As PGS research continues to pursue the prediction of complex social and behavioral traits, understanding how both data contributors and the broader public perceive this work is essential. This study highlights the central role of trust in scientists in shaping attitudes toward PGS for both medical and social traits. It also, however, underscores that both biobank participants and the public make important distinctions between PGS for medical and social traits. Biobank participants demonstrated a particularly large divergence in their views. While highly supportive of PGS for medical traits, they expressed significantly lower support for social trait applications. These results underscore the importance of engaging biobank participants and the public early and transparently, particularly when research ventures into areas that may challenge health-focused missions of some biobanks. Future studies should explore how trust, cultural context, and governance structures shape public and participant attitudes across diverse populations. Careful governance of genetic data is critical to ensure that the development of PGS technologies is aligned with participant and public values and used in ethically responsible ways.
Authors’ Contributions
A.M.L.: Formal analysis, methodology, data curation, writing—original draft, writing—review and editing, and visualization; M.W.: Conceptualization, methodology, writing—review and editing, and supervision; N.M.: Formal analysis, data curation, validation, and writing—review and editing; M.K.: Formal analysis, data curation, and writing—review and editing; R.J.C.: Conceptualization, methodology, writing—original draft, writing—review and editing, supervision, and funding acquisition.
Footnotes
Acknowledgments
Thank you to the people who completed the survey. Thank you also to the Mayo Clinic Biobank and the Center for Individualized Medicine for their assistance.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
Funding provided by the U.S. National Human Genome Research Institute (NHGRI) (R01HG012402 Prince and Cadigan, MPIs). The views expressed here are our own and not necessarily reflective of NHGRI.
Data Sharing
Data supporting this study are available upon reasonable request and subject to approval. Access to the data is restricted due to participant privacy concerns.