
Abstract

Introduction
Hirschsprung’s disease (HD) is a rare congenital condition affecting approximately 1 in 5000 newborns. It results from abnormal development of the enteric nervous system, leading to digestive disorders, particularly severe constipation in young children. Diagnosis is based on identifying the absence of ganglion cells and increased acetylcholinesterase (AChE) activity, observed through frozen rectal biopsies (RB). 1 Several diagnostic approaches are used: (i) the standard method using hematoxylin and eosin staining to detect ganglion cell absence and nerve fiber hypertrophy; (ii) immunohistochemistry with specific antibodies (calretinin) to distinguish ganglion cells from nerve fibers; and (iii) the reference method (Gold Standard), which relies on histo-enzymatic analysis of AChE activity in RB freshly frozen in isopentane cooled with liquid nitrogen (LN2) (isopentane-NF). These techniques are complementary, and the AChE method remains the method of choice to confirm diagnosis. However, the freezing technique is restricted in some clinical settings due to safety concerns. Therefore, we adopted nitrogen vapor freezing (vapor-NF), which will allow biopsies to be collected safely at the patient’s bedside. This study evaluates the impact of our biobanking protocol, including the freezing technique, cold ischemia time (CIT), and storage duration (STD) at −80°C, on the diagnostic quality of frozen RB used for HD diagnosis.
Methods
This retrospective observational study, conducted between 2019 and 2024, included 47 patients (male and female) aged 2 months to 11 years who were investigated for suspected HD. The pathology department usually receives 2–3 biopsies per patient, each measuring 2–3 mm. The RBs were collected by the pediatric department and transported to the pathology laboratory in Petri dishes on sterile gauze moistened with 0.9% saline. Each sample was recorded in the DIAMIC database (Dedalus-France).The RBs were placed in plastic molds and embedded in OCT (Optimal Cutting Temperature, SAKURA-France) before being frozen within 30 minutes after excision using a Dry Shipper (CRYODIFFUSION-BS2002-France). This container is equipped with an internal porous material capable of absorbing LN2 and releasing it as nitrogen vapor. As with isopentane, nitrogen vapor prevents the occurrence of the Leidenfrost effect. Once frozen, the biopsies were transferred into labeled cryotubes and stored at –80°C until AChE activity analysis in a specialized laboratory. The diagnostic approach was based on morphological and qualitative assessment. This histoenzymatic technique allows microscopic visualization of the presence, localization, and intensity of enzymatic activity. We have demonstrated the effectiveness of this freezing method in our laboratory. 2 We noted the observations documented in the pathology report and assigned a quality rating to the samples details in Table 1. A comparison was made between the vapor-NF and Isopentane-NF methods, including a historical cohort from 2009 to 2013 (20 patients aged 4 days–5 years). Statistical analyses were performed on quantitative variables using Student’s t-test and on qualitative variables using the chi-squared test or Fisher’s exact test. A multivariate logistic regression was conducted to assess the factors influencing tissue quality.
Descriptive and Comparative Analysis According to Tissue Quality and Age Classes Duration
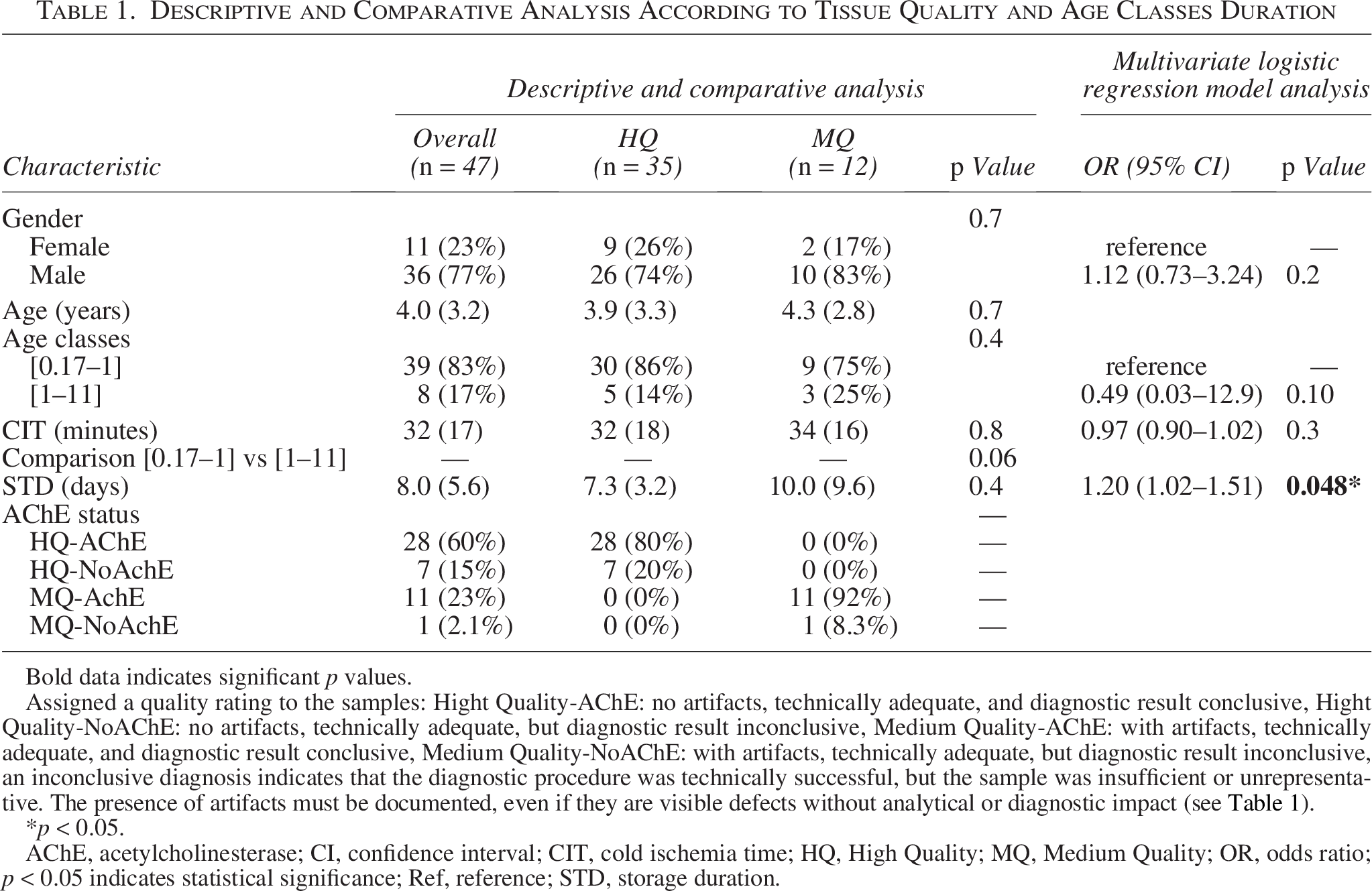
Bold data indicates significant p values.
Assigned a quality rating to the samples: Hight Quality-AChE: no artifacts, technically adequate, and diagnostic result conclusive, Hight Quality-NoAChE: no artifacts, technically adequate, but diagnostic result inconclusive, Medium Quality-AChE: with artifacts, technically adequate, and diagnostic result conclusive, Medium Quality-NoAChE: with artifacts, technically adequate, but diagnostic result inconclusive, an inconclusive diagnosis indicates that the diagnostic procedure was technically successful, but the sample was insufficient or unrepresentative. The presence of artifacts must be documented, even if they are visible defects without analytical or diagnostic impact (see Table 1).
*p < 0.05.
AChE, acetylcholinesterase; CI, confidence interval; CIT, cold ischemia time; HQ, High Quality; MQ, Medium Quality; OR, odds ratio; p < 0.05 indicates statistical significance; Ref, reference; STD, storage duration.
Results
For all age groups, 74% were classified as high quality (HQ) and 26% as medium quality (MQ). The CIT time was 32 minutes (SD = 17), with no significant difference between the HQ and MQ groups (p = 0.8). STD at −80°C was 8.0 days (SD = 5.6), with 7.3 days for the HQ samples and 10.0 days for the MQ samples (p = 0.4). All samples (100%) were usable, and 83% were suitable for AChE analysis: 80% in the HQ group and 92% in the MQ group. The comparison of age [0.17–1] versus [1–11] STD was significantly associated with tissue quality (OR = 1.20; 95% CI [1.02–1.51]; p = 0.048). The isopentane-NF method yielded 80% high-quality results, compared with 72.3% for the vapor-NF method. The comparison of tissue quality results between the isopentane-NF (n = 20) and vapor-NF (n = 47) methods (Table 2): for Isopentane-NF, 16/20 cases (80%) were “good,” 1/20 (5%) “medium/fair,” and 3/20 (15%) “poor.” For vapor-NF, 34/47 cases (72.3%) were “good,” 13/47 (27.7%) “medium/fair,” and none were “poor” (0/47, 0%). A specific analysis of the “poor” category was conducted. Fisher’s exact test (2 × 2) showed a significant difference between the two techniques (isopentane: 3/20 vs. vapor: 0/47; p = 0.024).
Comparison of Quality Outcomes between Two Methods: Freezing in Isopentane Cooled with Liquid Nitrogen Versus Nitrogen Vapor Freezing
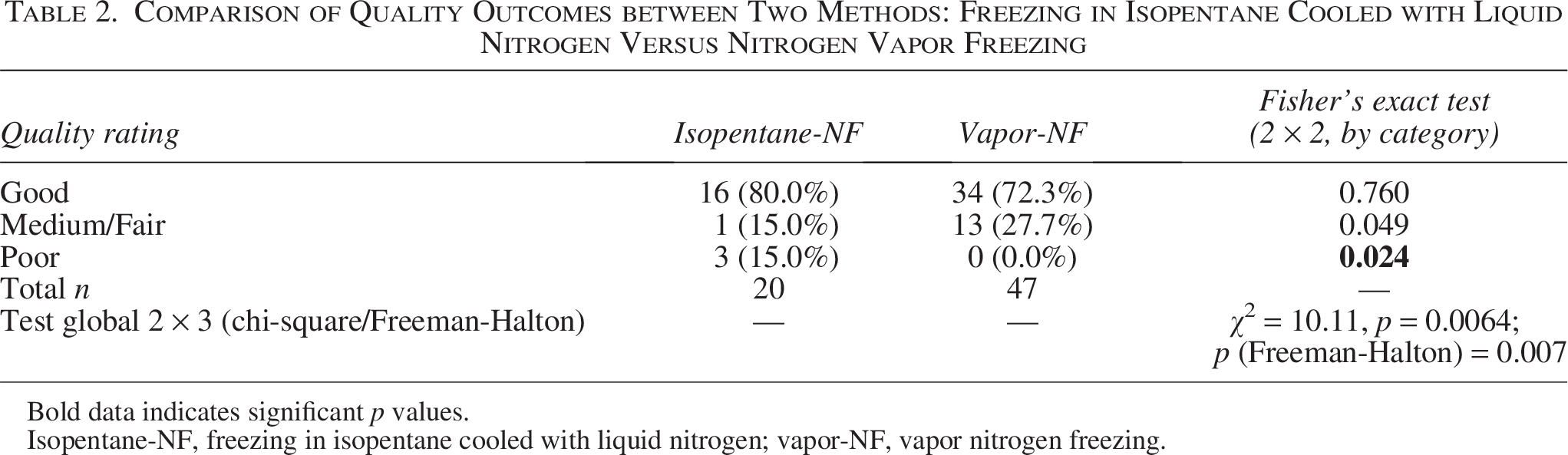
Bold data indicates significant p values.
Isopentane-NF, freezing in isopentane cooled with liquid nitrogen; vapor-NF, vapor nitrogen freezing.
Discussion and Conclusion
The management of HD, which affects approximately 1 in 5000 births with a male predominance (4:1), requires a multidisciplinary clinical and surgical approach. Proper storage conditions and control of CIT are essential to maintaining tissue integrity. In the overall study sample, the mean CIT was 32 minutes, a value close to that recommended for biobanks, 30 minutes after excision.3,4 Neither CIT nor STD at –80°C significantly impacted tissue quality. It is important to note that the interpretation of AChE profiles remains complex and subject to variability. 1 Among infants ([0.17–1] year group), STD at –80°C significantly influenced tissue quality. AChE activity also varies with age. In infants, a neonatal pattern predominates, with numerous AChE-positive nerve trunks in the muscularis and submucosa and low activity in the lamina propria. 5 The myenteric plexus also changes with age. 6 Some studies also suggest an age-adapted approach to performing biopsies. 7 Thus, the timing of biopsy sampling and tissue morphology are key diagnostic factors. Taking into account the sample size in the study, the vapor-NF method appears to offer a slight advantage over isopentane-NF: no poor-quality samples were observed, while MQ samples were more frequent. Rectal suction biopsies, often performed in young patients, may require particular attention to CIT and STD at –80°C. Although no specific study is available, the impact of these factors on sample quality is well known. 8 Cryopreservation may also influence the distribution of neuronal subtypes. 9 At the 2018 European Meeting on Neuromuscular Pathologies, it was recommended that CIT should not exceed 15 minutes for biochemical or enzymatic analyses. 10 This represents a real challenge. A realistic compromise could be a CIT between 15 and 30 minutes, with storage at below –80°C. The vapor-NF method has the practical advantage of being performed at the patient’s bedside. Larger-scale studies are needed to confirm these findings.
Authors’ Contributions
R.T. and M.G. contributed to conception and design of the study. R.T. data collection and analysis. F.O., helped in data collection. RT drafted the article. J.-F.I., M.G., and R.T. performed critical revision of the article. All the authors read, and approved the submitted version.
Footnotes
Acknowledgments
The authors thank Momar Diouf for statistic’s advice and Mathieu Fournier for his technical assistance.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
No funding was received for this article.
Informed Consent
The requirement for informed consent from the patient’s guardians was substituted by an opt-out process, considering the retrospective nature of this study. The entire institutional procedure with reference CHUFO2357 was carried out for the study approved by the ethics committee by Amiens-Picardie University Hospital Center, in accordance with the 1964 Helsinki Declaration and its subsequent amendments.