
Abstract
The “fitness-for-purpose” of biospecimens is paramount for reproducible genomic and proteomic research, yet is frequently compromised by preanalytical variability. To identify key determinants of sample quality in prostate cancer (PCa), a disease characterized by challenging tissue procurement, we conducted a retrospective quality audit of 300 radical prostatectomy specimens. Biospecimens were stratified based on Tumor Nuclei Percentage (TNP) against established thresholds for proteomic (TNP ≥ 20%) and genomic (TNP ≥ 50%) applications, revealing significant heterogeneity in the cohort’s overall quality. Subsequent analysis of preanalytical data revealed that the tissue procurement method—conventional macroscopic inspection, preoperative magnetic resonance imaging (MRI)-guidance, or biopsy-guidance—was the single most significant factor associated with achieving high-quality strata. For the stringent genomics-grade threshold (TNP ≥ 50%), guided procurement methods (MRI: 60.00%; Biopsy: 56.00%) more than doubled the yield of qualifying samples compared with conventional inspection (28.00%; p < 0.0001). This work establishes guided procurement not merely as a superior technique, but as an essential quality assurance standard for modern PCa biobanking, ensuring the collection of biospecimens that are truly “fit-for-purpose” in the era of precision medicine.
Introduction
The integrity and quality of biospecimens are foundational to modern biomedical research, yet a persistent “reproducibility crisis” undermines the reliability of scientific discovery and its translation into clinical practice. 1 A significant driver of this crisis is the failure to control for preanalytical variables—the myriad steps from specimen collection to analysis—which can introduce nonbiological variations that confound results and lead to the pursuit of unreliable biomarkers. 2 This systemic issue carries a staggering economic burden, with irreproducible preclinical research estimated to cost over $28 billion annually in the United States alone. 3 In response, major international initiatives, such as the National Cancer Institute’s Biospecimen Pre-analytical Variables Program, have been established to systematically assess and mitigate the impact of these variables on molecular data integrity.
Among these initiatives, the Clinical Proteomic Tumor Analysis Consortium (CPTAC) stands as a global exemplar, having established a “gold standard” for biospecimen quality through the implementation of exceptionally rigorous, standardized morphological quality control (QC) protocols. Our institution, serving as one of CPTAC’s international bioresource centers, has been deeply involved in the establishment and practice of these world-class procedures.4,5 This invaluable experience not only underscored the centrality of morphological assessment but also provided the direct catalyst for the present study: to apply this rigorous, quality-centric framework to systematically audit and optimize our own prostate cancer (PCa) biospecimen resource. 6 This endeavor was driven by the recognition that elite standards, honed in international consortia, must be translated into routine practice to ensure the local generation of globally competitive research data. 7
The challenge of managing preanalytical variability is particularly acute in the context of PCa biobanking.8,9 PCa is characterized by significant tumor heterogeneity, often presenting as multifocal lesions of varying grades that are difficult to identify through macroscopic inspection alone. 10 The tumor tissue is frequently intermixed with benign prostatic hyperplasia, stromal components, fibrosis, and inflammatory cells, further complicating accurate collection. 11 This challenge is starkly illustrated by data from The Cancer Genome Atlas (TCGA), where only 33% of biobanked PCa specimens were concordant with the final radical prostatectomy Gleason score, highlighting a systemic failure of conventional procurement to capture representative disease. 12 Consequently, conventional procurement, which relies on a pathologist’s subjective gross examination, frequently results in low “pathologic concordance,” where the biobanked tissue is not representative of the patient’s disease. 13 This discrepancy directly threatens the validity of downstream molecular analyses, as they may be performed on tissue with insufficient or nonrepresentative tumor content, thereby wasting precious patient material and research resources. 14
While the impact of preanalytical variables is widely acknowledged, 15 few studies have performed a systematic audit within a standardized workflow to isolate the single most critical determinant of sample quality for a specific cancer type. 16 This study was designed to fill that gap for PCa by using quantitative morphological assessment to identify and validate the paramount procedural factor driving biospecimen fitness-for-purpose. By leveraging our experience with CPTAC-level quality standards, we sought to establish an evidence-based framework for implementing quality assurance (QA) measures that dramatically improve the yield of molecular-grade samples and promote a new standard for high-quality tissue collection in translational PCa research.
Materials and Methods
Study design and biobank cohort
A comparative retrospective analysis of prospectively collected specimens was conducted on a cohort of 300 radical prostatectomy specimens collected between 2023 and 2024 at the Fudan University Shanghai Cancer Center (FUSCC). The inclusion criteria were as follows: (1) patients diagnosed with PCa who underwent radical prostatectomy; (2) availability of fresh-frozen tumor tissue samples in the biobank; (3) signed informed consent for biobanking and research use; and (4) complete clinicopathological data. Cases with insufficient tissue volume for research aliquoting without compromising pathological diagnosis were excluded. The study was performed in accordance with the Declaration of Helsinki and received approval from the Ethics Committee of FUSCC (Ethical code: 050432-4-2108).
Standardized biospecimen collection and biobanking workflow
To isolate the impact of the procurement methodology, all 300 specimens were processed under a strict, uniform workflow derived from the China Anti-Cancer Association (CACA) guidelines. 17 and institutional standard operating procedures (SOPs). The biobanking process began immediately in the operating theater, where the excised prostate was transferred to designated personnel. Under sterile conditions, tissue harvesting was performed targeting suspected tumor foci while avoiding necrosis, followed by immediate transport to the adjacent processing laboratory. Tissue was dissected into standardized aliquots (approx. 0.5 × 0.5 × 0.3 cm, weight ∼50 mg) and placed into prelabeled cryotubes. Critical data, including warm and cold ischemia times, were logged in the Laboratory Information Management System. Samples were cryopreserved in vapor-phase liquid nitrogen, with a strict control of total cold ischemia time (excision to freezing) to under 30 minutes for the entire cohort.
While the processing workflow was constant, the tissue procurement strategy varied by study design. Each case was assigned to one of three documented methods: (1) MRI-guided collection (n = 100): collection was directed to high-risk lesions (Prostate Imaging Reporting and Data System [PI-RADS] 4/5) identified on preoperative MRI; (2) Biopsy-guided collection (n = 100): collection was targeted to prostatic zones corresponding to positive cores in the patient’s preoperative biopsy report. (3) Conventional Macroscopic Inspection (n = 100): Tissue was sampled based solely on the pathologist’s gross visual and tactile examination of the specimen.
Morphological QC assessment
The primary outcome of this study was a quantitative measure of biospecimen quality. This was determined through a retrospective morphological assessment performed on 5-µm cryosections prepared from each of the 300 frozen tissue blocks. Sections were stained with hematoxylin and eosin (H&E). To ensure objectivity, two board-certified pathologists, blinded to the sample’s documented procurement method and all other clinical data, independently reviewed each H&E slide. The pathologists quantified the tumor nuclei percentage (TNP), defined as the percentage of viable tumor nuclei relative to the total number of all cell nuclei present in the assessed area of the section. The mean of the two pathologists’ scores was used for the final analysis. To validate the reliability of this assessment, inter-observer reproducibility was evaluated using the Intraclass Correlation Coefficient (ICC). The analysis demonstrated excellent concordance between the two pathologists (ICC = 0.991; 95% CI: 0.989–0.993), a result we attribute to strict prestudy consensus training.
Definition of quality strata and statistical analysis
To evaluate the “fitness-for-purpose” of each biospecimen for common molecular research applications, the cohort was stratified based on its measured TNP using two predefined quality thresholds. These thresholds were established based on guidelines from major research consortia: TNP ≥ 20% for proteomics-grade applications and TNP ≥ 50% for genomics-grade applications.
Statistical analyses were performed to identify associations between the documented preanalytical variable (procurement method) and the measured quality outcomes (TNP). Analysis of variance (ANOVA) was used to compare the mean TNP among the three procurement groups. The Chi-squared (χ2) test was employed to assess differences in the proportion of samples meeting the quality thresholds (qualification rates). Finally, multivariable logistic regression analysis was used to quantify the predictive value of the procurement method on the likelihood of achieving the quality thresholds. For this analysis, the Conventional Macroscopic Inspection group served as the reference category. All statistical tests were two-sided, and a p value of less than 0.05 was considered statistically significant. Analyses were performed using GraphPad Prism version 8.0.
Patient and public involvement statement
Patients were involved in the design, conduct, and dissemination plans of this research. Specifically, the study design included the collection of tissue samples from PCa patients undergoing radical prostatectomy, and patient consent was obtained for all participants. The involvement of patients was crucial in ensuring the study’s relevance to real-world clinical practices. Furthermore, feedback from patient representatives helped inform aspects of the research methodology and the interpretation of results. The findings will be shared with participants and the public through relevant dissemination channels, including publications and presentations aimed at improving PCa biobanking practices.
Results
Retrospective audit workflow and cohort-level quality profile
We conducted a retrospective audit of 300 radical prostatectomy specimens collected under a standardized biobanking workflow that controlled key preanalytical variables (e.g., ischemia time) and documented the procurement strategy for each case (Fig. 1). All specimens underwent uniform H&E review and TNP quantification against prespecified thresholds; the representative 20× fields in Figure 1 illustrate the heterogeneity observed across the cohort, with guided cases typically showing denser, well-preserved adenocarcinoma and conventional cases more benign glands and stroma. Across the cohort, tumor purity varied widely (mean TNP, 43.93%). To gauge fitness-for-purpose for molecular applications, we stratified the cohort by TNP thresholds: 208/300 (69.33%) met the proteomics-grade benchmark (≥20%), whereas only 144/300 (48.00%) achieved genomics-grade purity (≥50%), underscoring that nearly half of banked specimens would be unsuitable for high-value genomic analyses without explicit quality assessment.
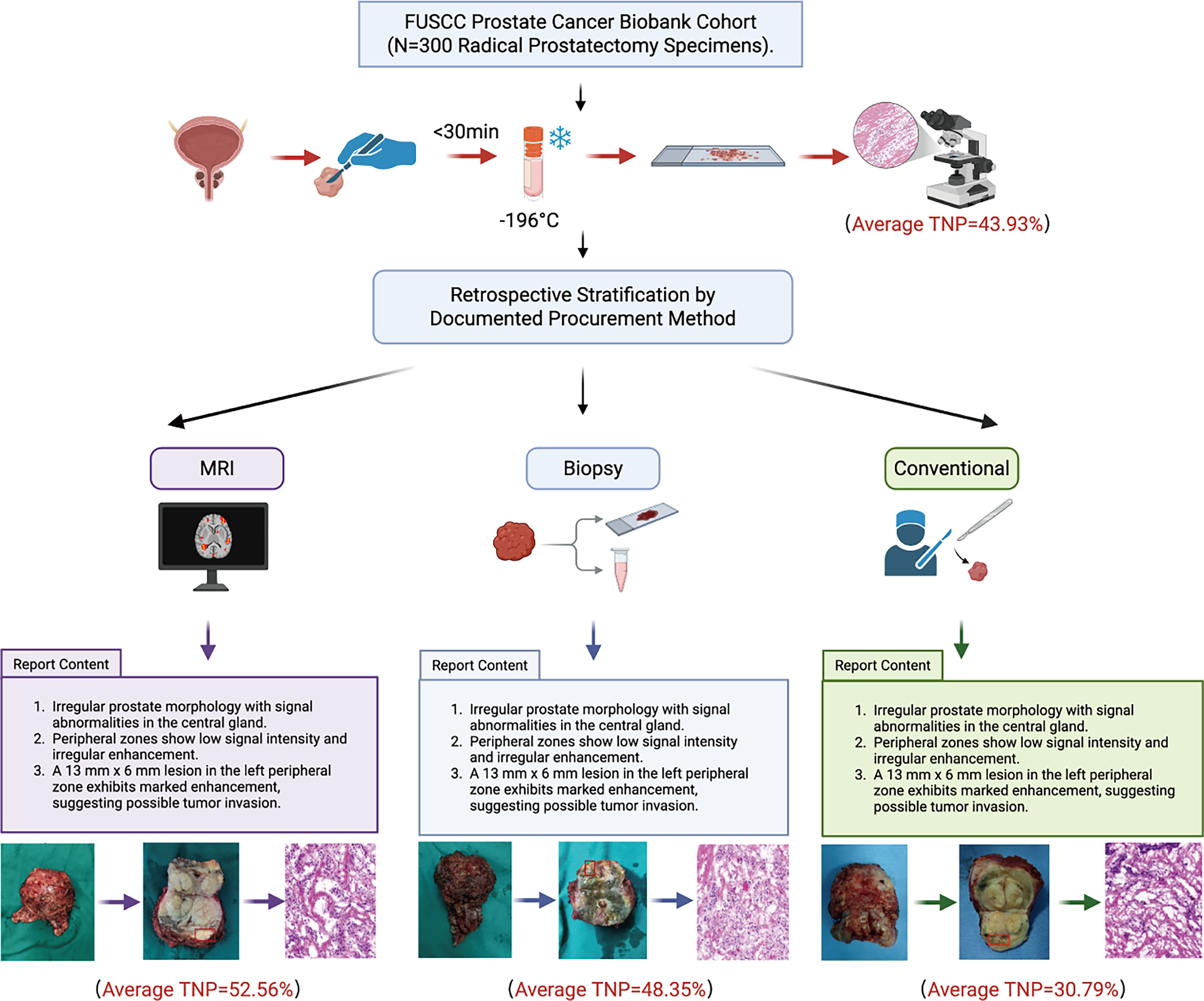
Study design and representative sampling workflows. The schematic illustrates the retrospective audit of 300 radical prostatectomy specimens collected under a standardized biobanking protocol (upper panel), featuring controlled cold ischemia time (<30 minutes) and vapor-phase liquid nitrogen storage. The cohort was stratified into three groups based on the documented procurement method: MRI-guided (targeting PI-RADS 4/5 lesions), Biopsy-guided (targeting positive core zones), and Conventional inspection (targeting palpable nodules). The lower panels display a representative case for each strategy, showing the specific diagnostic data used to guide sampling (clinical reports/MRI), the corresponding gross tissue extraction, and the resulting H&E-stained cryosection used for tumor nuclei percentage (TNP) quantification. Cohort-wide mean TNP values are indicated below each group. H&E, hematoxylin and eosin; MRI, magnetic resonance imaging.
Collection method emerges as a key determinant of sample quality
To isolate the procurement method as the primary driver of quality, we first assessed potential confounding factors. Technical preanalytical variables (e.g., cold ischemia time, freezing protocols) were standardized across the cohort (as described in Section 2.2), ensuring technical consistency. Biological variables were also strictly balanced: as detailed in Supplementary Table S1, there were no significant differences between the three cohorts regarding International Society of Urological Pathology (ISUP) grade (p = 0.999), cribriform growth (p = 0.817), or intraductal carcinoma of the prostate (IDC) status (p = 0.879).
With these confounding variables controlled, analysis revealed a strong and statistically significant relationship between the measured TNP and the procurement method (Fig. 2). The mean TNP was highest in the MRI-guided subset (52.56%), and biopsy-guided subset (48.35%), both of which were substantially higher than the conventional method (30.79%; ANOVA p < 0.0001). The difference between the two guided methods was not statistically significant (p = 0.787), indicating that both represent comparably effective strategies for enriching tumor content. The practical consequence of this difference is illustrated by the method-to-tier alluvial view (Supplementary Fig. S1): guided procurement (MRI or biopsy) provided the predominant share of genomics-grade specimens—116/144 (80.60%)—whereas the conventional arm contributes disproportionately to < 20% tier. Finally, to ensure robustness, we stratified qualification rates by ISUP category (Supplementary Fig. S2). Trends were concordant across all grades—with guided collection consistently exceeding the conventional method for both quality benchmarks—conforming that the superiority of guided procurement is robust and independent of tumor aggressiveness.
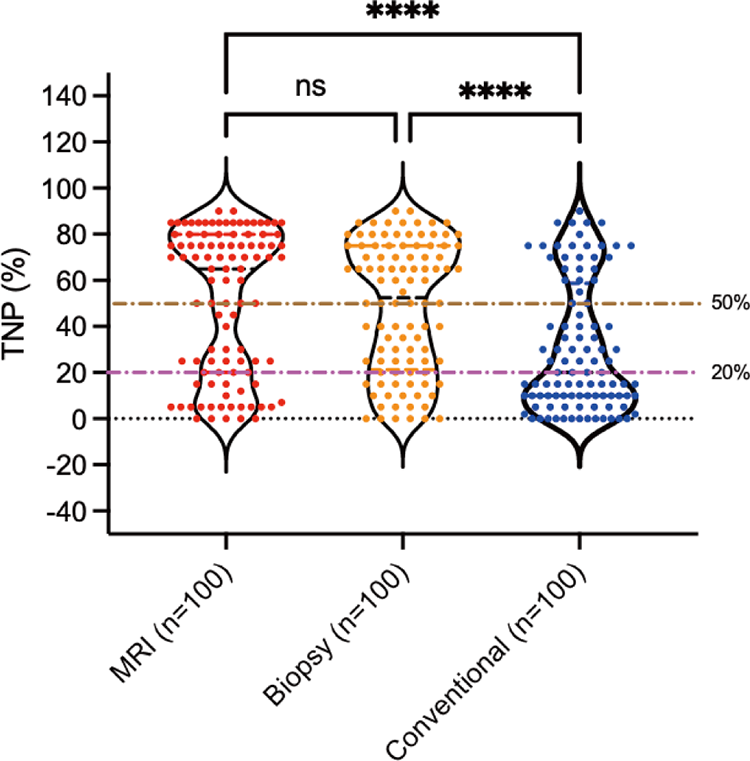
Distribution of mean tumor nuclei percentage (TNP) stratified by procurement method. Violin plots with overlaid jittered points (each dot = one specimen) show TNP distributions for MRI-guided (n = 100), biopsy-guided (n = 100), and conventional (n = 100) sampling. Horizontal reference lines within the violins indicate the median, and dotted quartiles indicate the interquartile range. Horizontal reference lines across the graph indicate the prespecified quality thresholds at 20% and 50% TNP. Statistical comparisons were performed using one-way ANOVA with post hoc pairwise analysis. Significance is indicated as: ****p < 0.0001; ns not significant (p > 0.05). Both guided methods yielded significantly higher TNP compared with the conventional method, with no significant difference between the MRI and biopsy groups. ANOVA, analysis of variance; MRI, magnetic resonance imaging.
Quantifying the predictive value of guided procurement
To quantify the strength of this association, a multivariable logistic regression analysis was performed, confirming that the procurement method was a powerful predictor of achieving quality thresholds (Fig. 3; detailed statistics provided in Supplementary Table S2). The analysis provided striking quantitative evidence of the superiority of guided methods. For the stringent genomics-grade threshold (TNP ≥ 50%), the odds of acquiring a qualifying sample were 3.85 times higher with MRI guidance (95% CI: 2.20–6.41) and 3.27 times higher with biopsy guidance (95% CI: 1.92–5.56) compared with conventional inspection. Conversely, the model’s intercept revealed that the odds of success for a conventionally procured sample were significantly less than one (OR = 0.39), indicating that failure to meet the genomics threshold is the statistically more likely outcome when using the traditional, nonguided method.
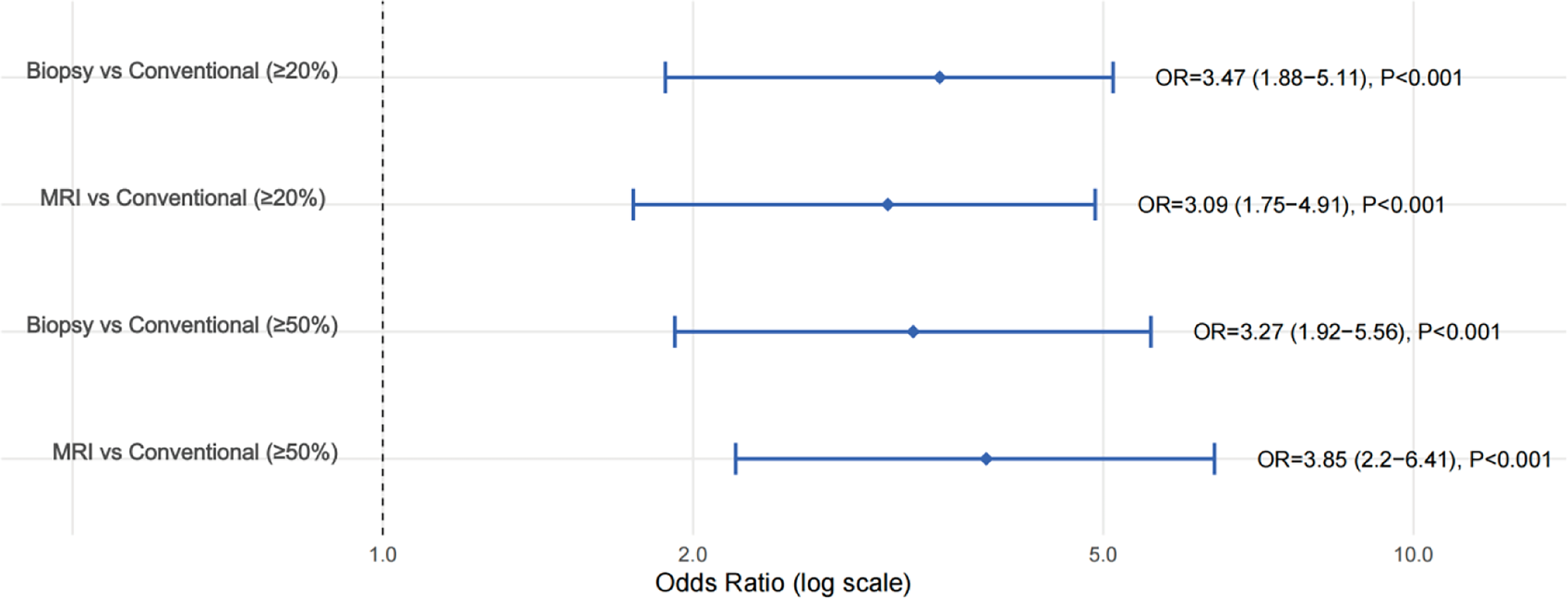
Logistic regression-derived probabilities of achieving quality thresholds by procurement method. Adjusted odds of meeting predefined TNP thresholds by procurement method. Forest plot of multivariable logistic regression comparing MRI-guided and biopsy-guided sampling with the conventional method (reference). Outcomes are achieving tumor nuclei percentage (TNP) ≥ 20% (“proteomics-grade”) and ≥ 50% (“genomics-grade”) on H&E. H&E, hematoxylin and eosin; MRI, magnetic resonance imaging.
Guided procurement mitigates quality loss in biologically challenging specimens
A sub-analysis was conducted on a subset of 82 cases that had received prior neoadjuvant therapy, a clinical variable known to reduce tumor cellularity. As expected, treated specimens exhibited significantly lower mean TNP across all procurement groups compared with their untreated counterparts (Fig. 4). In the conventional group, mean TNP dropped from 34.65% in untreated cases (n = 66) to 23.66% in treated cases (n = 34). However, even in this challenging context, the procurement method remained a critical determinant of quality. The guided methods still yielded samples with higher tumor content (MRI-treated: 32.14%; Biopsy-treated: 35.58%) than the conventional method in treated cases. This finding reinforces the primary discovery, highlighting that in biologically challenging scenarios where tumor content is inherently low, the use of a guided procurement strategy can be the deciding factor between obtaining a usable or an unusable biospecimen.
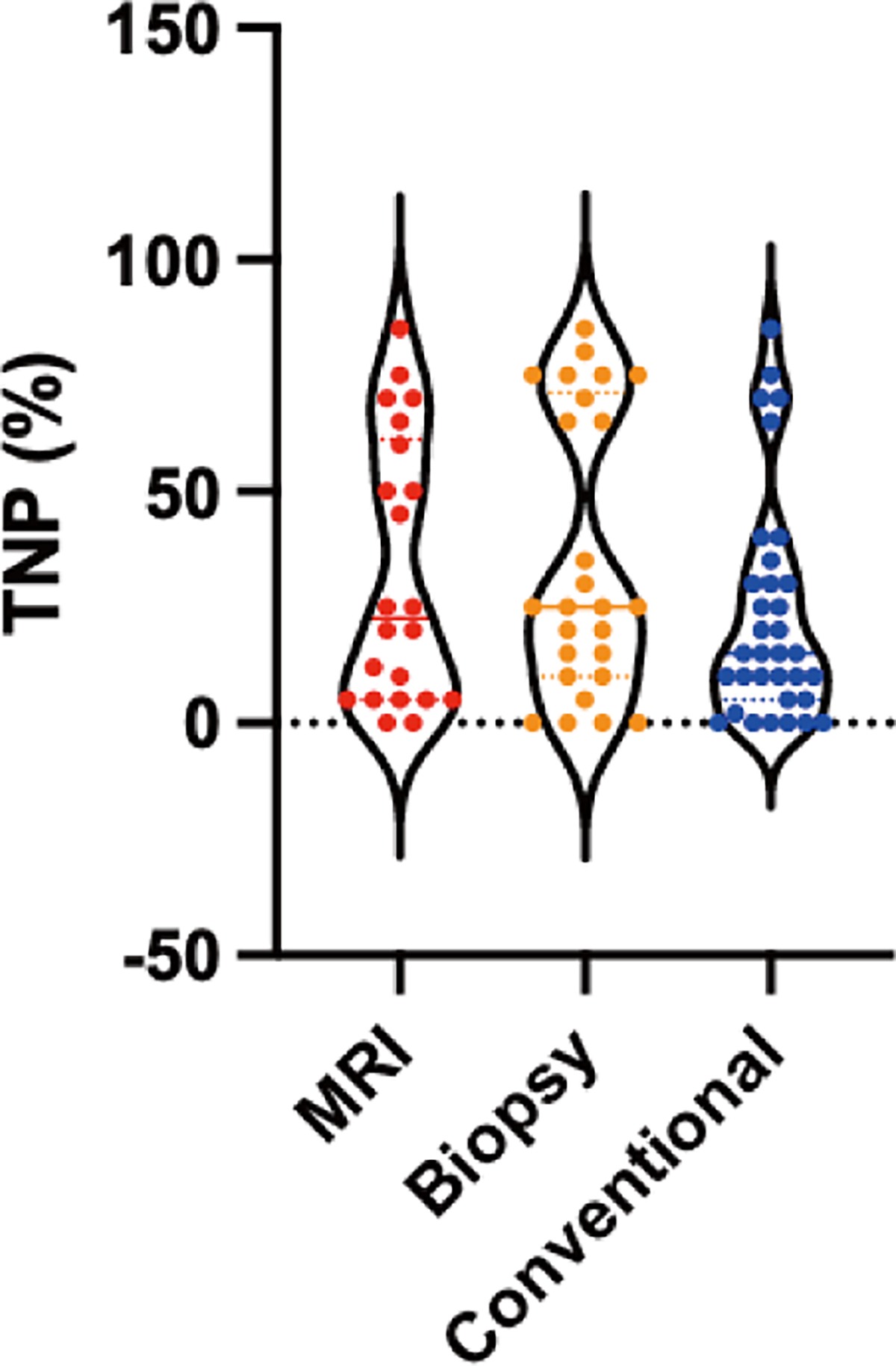
Impact of neoadjuvant therapy on tumor nuclei percentage (TNP) Yield across Procurement Strategies. Violin plots illustrate the distribution of TNP (measured as a percentage, Y-axis) for specimens derived from untreated patients (left violins) versus those who received neoadjuvant therapy (right violins), stratified by procurement method. MRI-guided (red), Biopsy-guided (orange), and Conventional (blue) groups are shown with unfilled outlines; colored elements represent individual data points/means. Solid horizontal lines indicate the median, and dotted lines represent the quartiles (25th and 75th percentiles).
Discussion
Systematic morphological quality assessment served as a critical discovery tool in this study revealing that over half (52.00%) of our prospectively collected specimens initially failed to meet the stringent criteria for genomics-grade research (TNP ≥ 50%). Our audit traced this systemic deficit to a single preanalytical determinant: the tissue procurement method. The stark contrast in mean TNP between guided (MRI: 52.56%; Biopsy: 48.35%) and conventional (30.79%) methods provides unequivocal evidence that the procurement procedure is the primary driver of quality. These findings are strongly contextualized by broader trends in the biobanking literature. The low qualification rate in our conventional arm (28.00%) parallels the challenges reported by TCGA, where only 33% of prostate specimens achieved concordance with the final surgical pathology, 12 confirming that blind collection is a systemic limitation of standard practice.
In contrast, the superior performance of our guided cohorts validates emerging precision biobanking strategies. 18 Our genomics-grade qualification rate (60.00%) aligns with the high targeting success rates (∼70%) reported by Heavey et al. using MRI-guided pathways.19,20 Crucially, our study advances this field by providing direct comparative evidence: multivariable logistic regression confirmed that guided collection increases the odds of obtaining a genomics-grade sample by nearly 4-fold (OR = 3.85) compared with conventional inspection. This demonstrates that integrating diagnostic data transforms sample procurement from a “morphological gamble”—often failing to capture occult tumors in heterogeneous tissue—into a strategic, evidence-based intervention.
Critically, this study controlled for the potential confounding effect of collection volume. By strictly standardizing the dimensions of every banked aliquot (approx. 0.5 × 0.5 × 0.3 cm ∼50 mg) as per our SOP, we ensured that the denominator for TNP assessment remained constant across all groups. Unlike studies where ad hoc collection sizes might introduce bias—where larger excisions inadvertently include more benign stromal tissue—our standardized approach isolates the procurement method (MRI-guided, biopsy-guided, vs. conventional) as the primary driver of sample quality. Thus, the higher TNP observed in the guided groups reflects superior localization accuracy rather than reduced tissue collection volume.
From an operational prospective, these findings advocate for a paradigm shift from passive, retrospective QC to active, prospective QA.21,22 A QC-based approach merely identifies failure after resources have been expended, whereas a QA-based strategy prevents failure from the outset. By more than doubling the yield of high-purity samples, guided procurement directly optimizes “biobankonomics,” mitigating the opportunity costs associated with storing “morphologically unqualified” tissues.23,24 This quality-centric philosophy, championed by consortia like CPTAC, reframes operational costs as a direct investment in reproducible science.
We acknowledge that the definition of “fitness-for-purpose” is evolving. While we utilized a rigorous ≥ 50% TNP threshold to align with historical “gold standards” from consortia like TCGA and CPTAC, modern Next-Generation Sequencing pipelines are increasingly capable of deriving valid data from samples with lower tumor cellularity (e.g., 30%–40%). Importantly, our data demonstrate that the superiority of guided procurement is robust to threshold de-escalation. As shown in our logistic regression analysis (Fig. 4), guided methods maintained a 3-fold statistical advantage (OR > 3.0) over conventional inspection even when the qualifying threshold was lowered to ≥ 20%. Thus, whether aiming for the stringent purity required for deep multiomics or the more flexible thresholds of clinical sequencing, guided procurement consistently maximizes the yield of usable biospecimens.
Another important consideration is the potential bias introduced by small tumor foci. Small or multifocal lesions, particularly those below the resolution of MRI or impalpable during gross inspection, are inherently prone to being missed during procurement. This “missed” fraction is likely disproportionately higher in the conventional inspection group, contributing significantly to the lower TNP and qualification rates observed in that arm. Consequently, this introduces a selection bias wherein the biobanked cohort is naturally skewed toward tumors with larger volumes or higher detectability. While guided methods significantly mitigate this by targeting radiographically visible yet macroscopically occult lesions, they cannot entirely eliminate the risk of missing microscopic foci. Therefore, researchers utilizing these resources should be aware that biobanked specimens may not fully represent the earliest stages of low-volume disease.
While this study establishes a robust framework, its limitations highlight avenues for further refinement. A single H&E cryosection provides only a two-dimensional snapshot of a three-dimensional tissue block’s inherent heterogeneity. 25 Furthermore, regarding the scalability of quality assessment, while our study achieved high inter-observer reproducibility (ICC = 0.991) using expert pathologists, manual assessment is inherently time-consuming. The integration of emerging AI-based cellularity assessment tools represents a critical future direction. By replacing manual scoring with automated, algorithmic quantification, biobanks can further standardize quality metrics and reduce the operational burden on pathology staff. Finally, low tumor cellularity is not just a dilution factor; it is a direct threat to the validity of molecular data, increasing the risk of false-negative results in downstream assays. 26
In conclusion, this audit establishes that the tissue procurement method is the critical determinant of biospecimen fitness-for-purpose. Adopting MRI- or biopsy-guided strategies is a necessary evolution for PCa biobanking, ensuring that collected resources are truly fit for the era of precision medicine.
Authors’ Contributions
M.X., B.L., Q.W., and M.S. conceived the study, performed the literature search, and prepared the figures. G.Q., Y.G., F.D., W.J., and Q.H. helped with data collection, analysis, and interpretation. M.X., B.L., and Q.W. wrote and revised the article. All authors read and approved the final article.
Footnotes
Author Disclosure Statement
The authors declared no potential conflicts of interest in terms of the research, authorship, and/or publication of this article.
Funding Information
This work was supported by the Shanghai R&D Public Service Platform Project (Grant number: 12DZ2295100).
Data Availability
All data generated and described in this article are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the Ethics Committee of FUSCC, and all patients provided informed consent (Ethical code: 050432-4-2108).
Consent for Publication
Consent for publication has been obtained from the participant.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.