
Abstract
Introduction:
Procurement of human spinal cord tissue for research is rare and typically occurs through deceased organ donation pathways. Existing tissue banking guidance, largely derived from surgical pathology practice, does not adequately address the ethical, anatomical, and operational constraints unique to donation-integrated spinal cord procurement.
Objectives:
The objective of this article is to describe institutionally implemented governance and prioritization practices for donation-integrated procurement and research banking of human spinal cord tissue within a tertiary academic hospital setting.
Methods:
This review summarizes practice-based governance guidelines developed and applied within an established organ donation program. The approach emphasizes conservative prioritization, strict separation of clinical and research roles, a tiered informed consent structure, explicit stopping rules, and defined governance structures for procurement decision making. The spinal cord is treated as the ethically defining and rate-limiting tissue, with biologically associated tissues considered only under conditional circumstances.
Results:
The governance practices delineate clear operative boundaries for when spinal cord procurement may proceed, establish decision hierarchies for inclusion of associated tissues, and define conditions under which procurement must be deferred. Operational experience from the institutional donation–integrated procurement program included 96 authorized research donors, of whom 92 were enrolled under the research protocol and 88 proceeded to successful spinal cord procurement and accessioning into the institutional biobank. Central principles guiding procurement include preservation of donor dignity, noninterference with organ donation workflows, maintenance of anatomical integrity, and irreversible transition of tissue from the clinical to the research domain under institutional custodianship.
Conclusions:
Governance-centered, practice-based approaches are essential for ethically grounded procurement of rare human spinal cord tissue in organ donation settings. Emphasis on upstream decision making, explicit scope limits, and conservative default thresholds supports translational research while preserving clinical primacy and ethical clarity. These principles may assist other centers seeking to integrate spinal cord research within established organ donation programs.
Keywords
Introduction
Human tissue banking for research is a routine activity in academic medical centers and is commonly supported by institutional practices derived from surgical pathology services.1,2 Within this paradigm, appropriately consented tissue exceeding diagnostic requirements may be allocated for research in accordance with established prioritization principles, with patient care and diagnostic sufficiency maintained as overriding obligations.3,4 These practices assume regular access to surplus tissue generated during surgical resections and rely on pathology-informed judgment to balance clinical and research needs. 5 Human spinal cord tissue does not fit this paradigm.6,7 Access to adult human spinal cord tissue is rare and typically occurs only through deceased organ donation pathways.8,9 Donors accessed through organ donation pathways are not selected on the basis of research-specific health criteria and may include individuals with diverse clinical backgrounds consistent with standard organ donation eligibility. Under these conditions, procurement decisions are made under heightened ethical and anatomical constraints, and research activities must be explicitly subordinated to transplantation priorities and clinical obligations.10,11 Unlike tissues obtained through elective surgery, spinal cord tissues cannot be sampled opportunistically, and inappropriate procurement decisions carry irreversible consequences. Despite growing interest in human-relevant models of spinal cord injury, neural stem and progenitor cell biology, neuromuscular disease, and neurodegeneration, access to healthy adult human spinal cord tissue remains extremely limited.12,13
Published guidance on research tissue banking has focused largely on surgical pathology–based procurement and does not adequately address donation-integrated acquisition of anatomically irreplaceable central nervous system tissue.14,15 As a result, institutions seeking to support spinal cord-based research often lack clear, practice-oriented guidance on how procurement decisions should be prioritized, how competing clinical and research obligations should be resolved, and how scope should be constrained to preserve ethical clarity. In the absence of such guidance, practices may become inconsistent or investigator driven, while overly restrictive approaches may unnecessarily limit access to an already scarce resource. 6 An additional consideration is the biological relationship between the spinal cord and surrounding or functionally associated tissues.16,17 Many neurological and neuromuscular disorders exhibit coupled pathological and molecular changes across central and peripheral tissues, including spinal cord, skeletal muscle, peripheral nerve, and associated vasculature, necessitating coordinated analysis across these compartments.18–20 Although access to associated tissues can enhance interpretive rigor and translational relevance in spinal cord–focused studies, their inclusion introduces additional ethical and operational constraints, particularly within the time-sensitive and highly regulated organ donation environment.9,21 Despite these competing scientific and ethical considerations, there remains limited practice-oriented guidance defining how associated tissues should be prioritized, constrained, or excluded within donation-integrated spinal cord research procurement. Clear prioritization and scope boundaries are therefore essential to prevent ethical ambiguity and scope creep. In this article, we summarize institutional practice guidelines for spinal cord–centered research tissue banking developed and implemented within a tertiary academic hospital. These guidelines are written from the perspective of an institutional biorepository and reflect practical experience integrating research procurement within established organ donation pathways. Central to these practices is the treatment of the spinal cord as the ethically defining and rate-limiting tissue, which establishes the conditions under which procurement may occur and under which biologically associated tissues may be considered. The purpose of this article is to provide a concise, practice-based reference that may assist other centers in developing consistent, ethically grounded approaches to the procurement and stewardship of rare human spinal cord tissue for research.
Practice Guidelines for Donation-Integrated Procurement and Banking of Human Spinal Cord and Associated Tissues
The following guidelines describe institutional practice for the procurement and banking of human spinal cord tissue within deceased organ donation pathways. They are intended to clarify operative boundaries, prioritization principles, and stopping rules that govern when research procurement may proceed, rather than to prescribe technical procedures. Emphasis is placed on maintaining clinical primacy, anatomical integrity, and responsible stewardship of a rare and irreplaceable tissue. The donation-integrated operative sequence through which spinal cord tissue transitions from the clinical and organ donation domain to the research domain is illustrated in Figure 1.
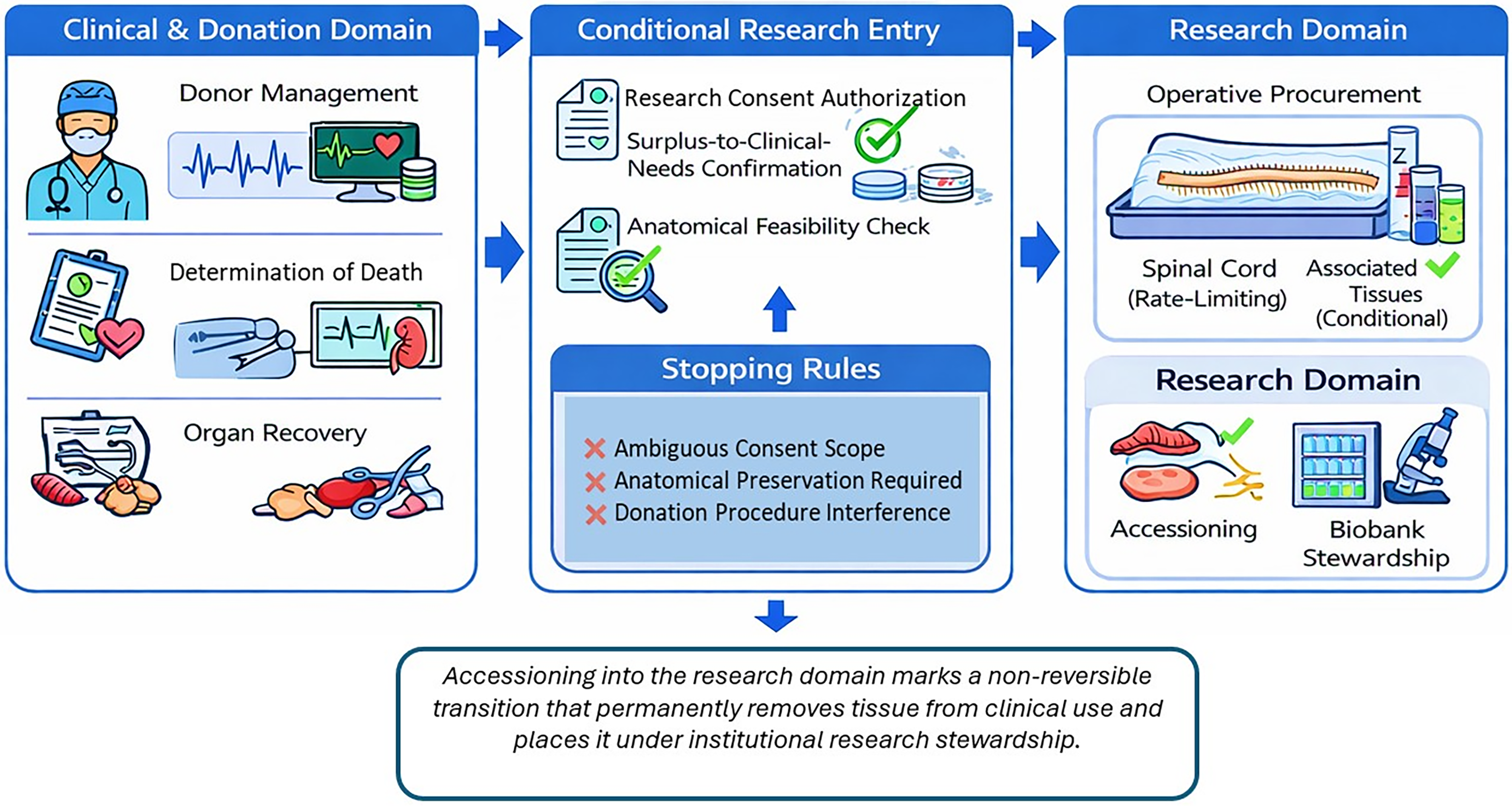
Donation-integrated operative workflow for spinal cord tissue procurement and research banking. Schematic representation of the donation-integrated operative sequence through which human spinal cord tissue may transition from the clinical and organ donation domain to the research domain. Clinical care, determination of death, and organ recovery retain absolute priority at all stages. Entry into research procurement is conditional upon confirmation that authorization for research tissue donation has been obtained through the organ donation consent process, confirmation that tissue procurement is unequivocally surplus to clinical and donation needs, and assessment of anatomical feasibility for spinal cord recovery. Explicit stopping rules, including ambiguous consent scope, anatomical preservation requirements, or interference with donation procedures, preclude research procurement. When these conditions are satisfied, operative procurement of the spinal cord (rate-limiting tissue) and, conditionally, associated tissues may proceed. Accessioning into the research domain marks a nonreversible transition that permanently removes tissue from clinical use and places it under institutional research stewardship.
Organ donation setting and operative boundaries
Procurement of spinal cord tissue for research occurs exclusively within established deceased organ donation pathways. Clinical teams responsible for donor care and organ recovery operate independently of research personnel throughout the donation process. Coordination between research personnel and donation or operating room teams is limited to communication necessary to ensure noninterference with donation workflows. Research procurement is undertaken only when it does not introduce delay, procedural complexity, or risk to organ recovery.
Identification of potential donor cases and notification pathway
Potential opportunities for spinal cord research procurement are identified through routine communication with the regional organ donation program responsible for coordinating deceased donor cases. Donation program personnel notify the institutional research biobank team when authorization for research tissue donation has been obtained and when operative conditions indicate that research procurement may be feasible without interfering with organ donation procedures. Notification typically occurs only after donation eligibility and consent scope have been confirmed within the clinical donation workflow. Research personnel do not participate in donor eligibility determination or donor management decisions and are involved only after donation program personnel confirm that research activity may be considered without compromising clinical priorities. When notification occurs under time-sensitive conditions, research procurement is considered only if required personnel and resources are available without introducing delay to donation procedures.
Separation of clinical judgment from research procurement
All decisions related to donor management, determination of death, timing of withdrawal of life-sustaining measures, and organ recovery remain within the clinical domain. Research personnel are not involved in these determinations. Consideration of spinal cord procurement for research occurs only after donation program personnel confirm that procurement may proceed without affecting organ donation procedures.
Operational decision authority and confirmation of procurement eligibility
Decision authority within donation-integrated spinal cord procurement is distributed across the clinical donation program, neurosurgical procurement personnel, and institutional biobank governance structures, each of which exercises defined responsibilities at different stages of the workflow. Donation services are responsible for confirming donor eligibility and verifying the scope of research consent. Neurosurgical personnel determine anatomical feasibility and procedural safety for spinal cord removal following completion of organ recovery procedures. The institutional biobank custodian confirms that procurement conditions satisfy institutional research governance requirements and authorizes accessioning of tissue into the research domain. Procurement proceeds only when confirmation is obtained at each of these stages. Any uncertainty regarding consent scope, interference with donation procedures, or anatomical preservation requirements triggers a default decision not to proceed. Stopping rules may therefore be activated by donation services, neurosurgical personnel, or institutional biobank leadership, each of whom retains authority to defer procurement when clinical, ethical, or institutional obligations cannot be clearly satisfied.
Eligibility determination and conditions under which procurement may proceed
Eligibility for spinal cord research procurement follows the general clinical eligibility criteria applied within the deceased organ donation program. Spinal cord procurement for research is considered only when appropriate authorization for research donation has been confirmed and when tissue is unequivocally surplus to donation and clinical needs. Confirmation from donation program personnel or operative teams is obtained in real time prior to procurement. When confirmation cannot be obtained, or when operative conditions change such that donation priorities may be affected, the default decision is not to procure tissue for research. Donors are not selected based on research-specific health criteria, and any individual eligible for organ donation may be considered for research tissue procurement unless specific clinical, anatomical, or consent-related constraints preclude procurement. Where jurisdictionally permitted, donors proceeding through Medical Assistance in Dying pathways may also be eligible for research tissue donation when such donation occurs within established organ donation and consent frameworks.
The spinal cord as the primary and rate-limiting anatomical resource
The human spinal cord is treated as the primary anatomical resource. Its anatomical irreplaceability, functional significance, and rarity impose the highest threshold for procurement among tissues considered for research banking. Spinal cord tissue is procured only when removal can be performed without compromising anatomical integrity, post-donation requirements, or institutional obligations. Decisions regarding all associated tissues are subordinate to spinal cord–centered considerations.
Tiered consent framework and confirmation of authorization
Authorization for research tissue donation is obtained through institutionally approved informed consent processes integrated with organ donation pathways. Consent is structured in a tiered format that allows donors or substitute decision-makers to specify the scope of permitted research uses. In operational practice, three principal consent tiers are distinguished: (i) spinal cord–specific procurement, permitting recovery of spinal cord tissue for neuroscience research; (ii) inclusion of biologically associated tissues, permitting recovery of additional tissues such as skeletal muscle, peripheral nerve, vascular tissue, or skin when these are considered necessary to support interpretation of spinal cord–centered analyses; and (iii) downstream research use, permitting molecular and cellular analyses including genomic or transcriptomic studies and, where authorized, sharing of coded specimens with external collaborators. In the time-sensitive donation setting, confirmation of consent scope is performed by donation program personnel responsible for donor authorization. Procurement proceeds only when consent explicitly permits the tissues and categories of research proposed. When consent documentation is incomplete, unclear, or inconsistent with requested tissue inclusion, procurement does not proceed. Any consent restrictions specified by donors or substitute decision-makers (e.g., limitations on genomic analysis or international data sharing) are recorded within institutional biobank documentation and enforced during downstream access review to ensure that tissue use remains consistent with the authorized scope of donation.
Associated tissues included under conditional and subordinate criteria
Associated tissues, including paraspinal skeletal muscle, cardiac muscle, vascular tissue, peripheral nerve, and skin (epithelial tissue), may be included only secondarily and under strictly conditional circumstances. Their procurement is considered exclusively when spinal cord procurement is feasible, consent explicitly permits their inclusion, and removal does not interfere with donor management, organ donation procedures, or anatomical preservation requirements (Fig. 2). These tissues are not independently prioritized for banking and are obtained only when they provide clearly defined comparative information necessary for interpretation of spinal cord–centered analyses. In all cases, decisions regarding associated tissue inclusion remain subordinate to spinal cord–specific considerations and are deferred when tissue quantity, orientation, or institutional obligations impose competing constraints. In selected contexts, access to associated tissues may be necessary to support interpretation of spinal cord–centered molecular or cellular analyses by providing biologically relevant comparators, rather than serving as independent research targets.
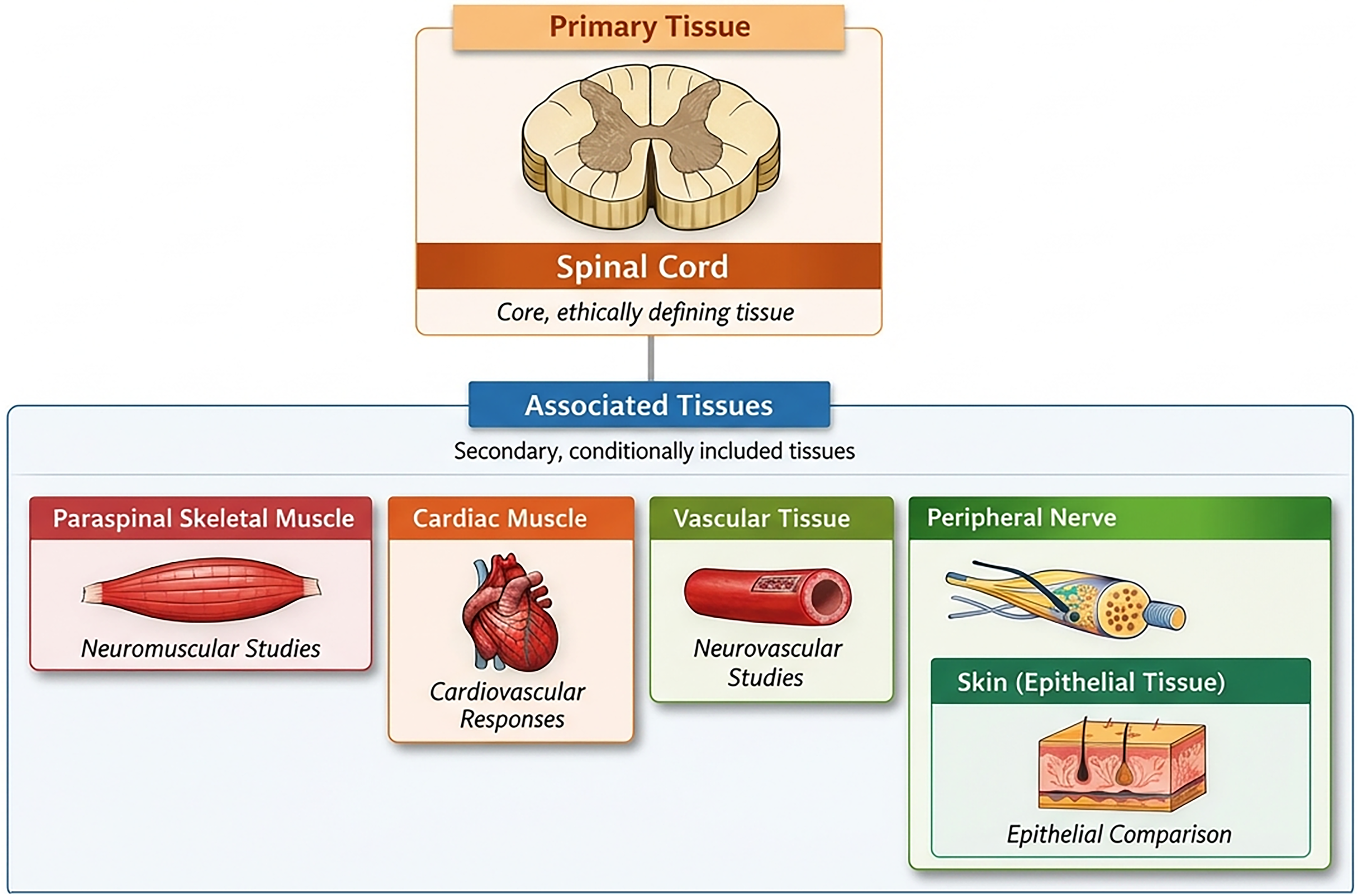
Decision hierarchy for tissue inclusion in spinal cord research banking. Conceptual schematic illustrating the decision hierarchy used to determine tissue inclusion in donation-integrated spinal cord research banking. The spinal cord is treated as the ethically defining and rate-limiting tissue, with biologically associated tissues considered only secondarily and under conditional circumstances, contingent upon the feasibility of spinal cord procurement, consent scope, and noninterference with organ donation or anatomical preservation requirements.
Anatomical feasibility and technical considerations
Spinal cord procurement is performed only by personnel with appropriate anatomical expertise and is conducted under neurosurgical supervision. Removal is undertaken with attention to preserving anatomical integrity and minimizing disruption of surrounding structures. When anatomical constraints, operative conditions, or personnel availability preclude safe or interpretable procurement, tissue is not harvested. Procurement is deferred rather than performed under suboptimal conditions.
Timing relative to organ recovery and ischemia considerations
Procurement is performed only after completion of organ recovery and without introducing avoidable delays. Warm and cold ischemia intervals, along with handling conditions prior to preservation, are recorded contemporaneously. Timing considerations inform downstream interpretation but do not override donation priorities or justify deviation from operative sequencing.
Preservation of rostro-caudal orientation and segmental identity
Where feasible, procurement preserves rostro-caudal orientation and segmental identity of the spinal cord, which are essential for downstream analyses requiring regional or spatial interpretation. When operative conditions do not permit reliable orientation or segmentation, tissue may be deemed unsuitable for research and procurement is deferred.
Documentation supporting traceability and downstream interpretation
Documentation is completed at the time of procurement and is sufficient to support traceability and later assessment of specimen suitability. Records include confirmation of consent scope, confirmation of donation priority status, tissues procured, timing parameters, handling conditions, and intended preservation route. Specimens are accessioned under coded identifiers. Identifying information is maintained separately under restricted access in accordance with institutional policy.
Transition from the operative field to the research domain
Following procurement, tissues are transferred from the clinical environment to the research domain and accessioned into the institutional biobank. Once accessioned, tissue permanently exits the clinical domain and is no longer available for diagnostic or transplant purposes. Custodianship of banked tissue is institutional rather than project specific.
Preservation strategies and downstream flexibility
Preservation strategies are selected to maintain future research utility rather than to meet immediate experimental needs. Where feasible, tissues are preserved in formats compatible with multiple downstream applications, including molecular, cellular, and histological analyses. Preservation modality and key handling parameters are documented at accession to support responsible allocation and interpretation.
Assessment of tissue suitability at the point of use
Routine destructive quality testing at accession is avoided for scarce tissues. Assessment of tissue suitability is performed at the point of downstream use, when analytical requirements are defined. Observations related to tissue integrity or usability, when obtained, are recorded to inform future allocation decisions and support accurate interpretation of downstream analyses.
Stewardship and controlled access to banked tissue
Access to banked spinal cord and associated tissues is restricted to qualified investigators with appropriate ethical approval and use consistent with consent. Requests are evaluated based on scientific merit, proportional use of limited material, and stewardship of a scarce anatomical resource. Investigators do not receive identifying information and are prohibited from attempting donor reidentification.
Governance of tissue allocation and conflict resolution
Requests for access to banked spinal cord and associated tissues are reviewed through an institutional governance process designed to ensure responsible stewardship of a scarce anatomical resource. Allocation decisions are evaluated by a biobank oversight committee composed of the institutional biobank custodian, representatives of the organ donation program, neurosurgical or clinical leadership involved in procurement, and scientific investigators with relevant subject-matter expertise. Where appropriate, institutional research ethics or governance representatives may also be consulted to confirm alignment with approved consent scope and institutional policies. Committee deliberations consider scientific merit, proportional use of limited material, feasibility of the proposed analyses, and consistency with donor authorization. Investigators requesting tissue do not participate in decisions concerning their own proposals and are recused from deliberations when conflicts of interest arise. Allocation decisions and associated conditions are documented within institutional biobank records to ensure transparency, traceability, and responsible stewardship of the tissue resource.
Contraindications and special situations
In the donation setting, spinal cord tissue is uniquely constrained by anatomical irreplaceability, time sensitivity, and overlapping clinical obligations. As such, procurement decisions are made conservatively, with priority given to donor dignity, completion of organ donation, and preservation of anatomical integrity over potential research utility. Decisions to defer procurement are therefore considered appropriate outcomes rather than missed opportunities. Furthermore, spinal cord and associated tissue procurement does not proceed under the following conditions: (i) post-donation anatomical preservation requirements cannot be met; (ii) completion of donation procedures cannot be confirmed in real time; (iii) consent scope is ambiguous or incomplete; (iv) tissue quantity is insufficient to preserve anatomical integrity; (v) orientation or segmentation required for meaningful interpretation cannot be maintained; or (vi) competing research requests would exhaust limited tissue without proportional justification. Accordingly, key decision points encountered during donation-integrated spinal cord procurement and their conservative practice–based resolution are summarized in Table 1. The table also identifies the institutional role responsible for confirming each decision point, clarifying operational decision authority within the governance framework.
Operational Decision Points and Governance-Based Resolution in Donation-Integrated Spinal Cord Tissue Procurement
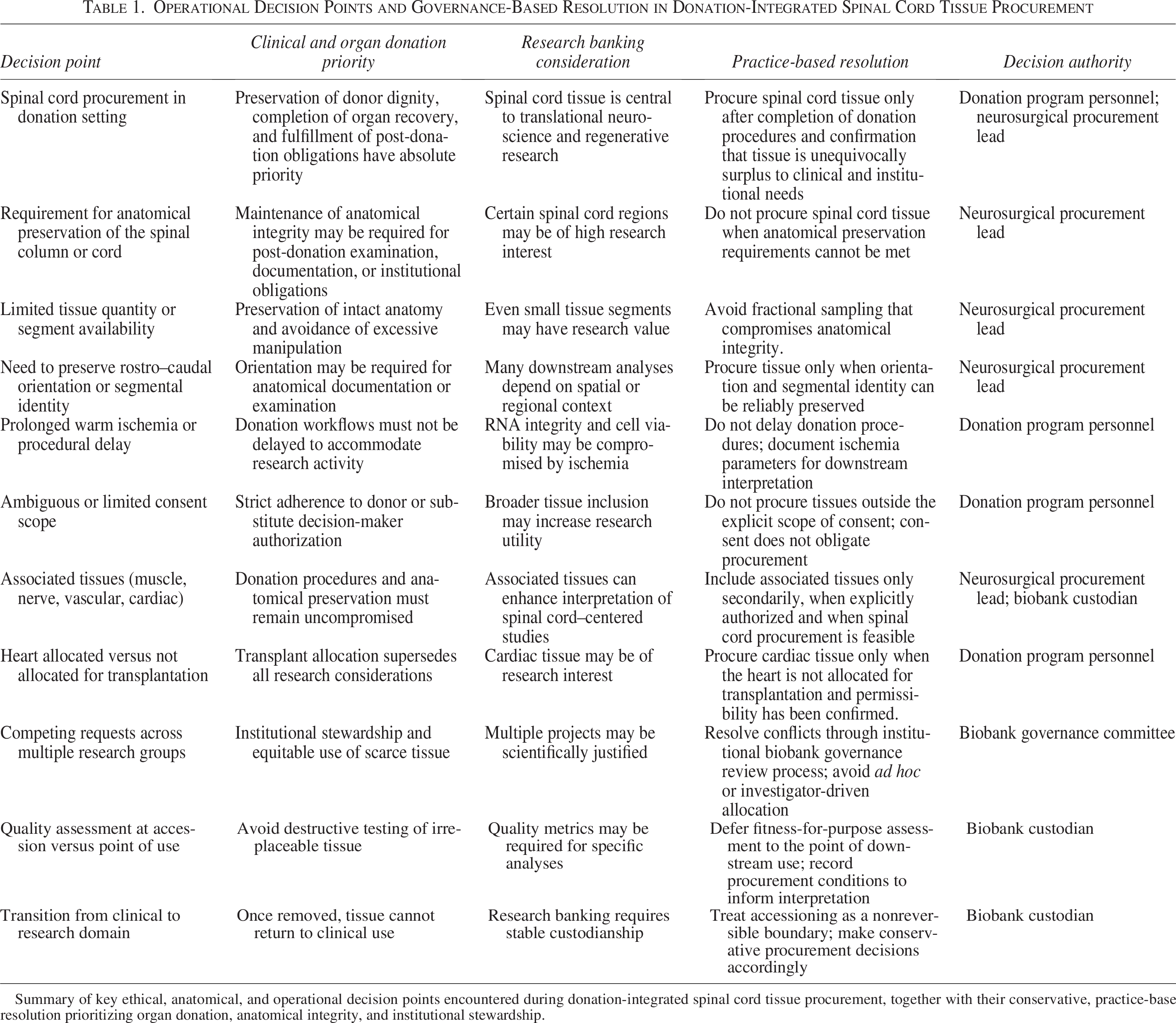
Summary of key ethical, anatomical, and operational decision points encountered during donation-integrated spinal cord tissue procurement, together with their conservative, practice-based resolution prioritizing organ donation, anatomical integrity, and institutional stewardship.
Operational experience with donation-integrated spinal cord procurement
Operational counts from the institutional donation–integrated spinal cord research program are presented to contextualize implementation of the procurement framework described above based on cumulative cases evaluated within the institutional program over a 10-year period. Potential donor cases are identified through the institutional organ donation referral pathway, and research tissue procurement is considered only after confirmation that authorization for research donation has been obtained through the organ donation consent process. Within this program, 96 individuals provided authorization for research tissue donation, of whom 92 donors were subsequently enrolled under the research protocol. Eighty-eight donors proceeded to operative procurement, with spinal cord tissue accessioned into the institutional research biobank. In a small number of authorized cases, procurement did not proceed due to operational constraints inherent to the donation environment, including anatomical preservation requirements, competing clinical priorities during organ recovery, or logistical limitations within the donation workflow. These operational outcomes reflect both the feasibility and the practical constraints associated with integrating spinal cord tissue procurement within established organ donation pathways (Fig. 3).
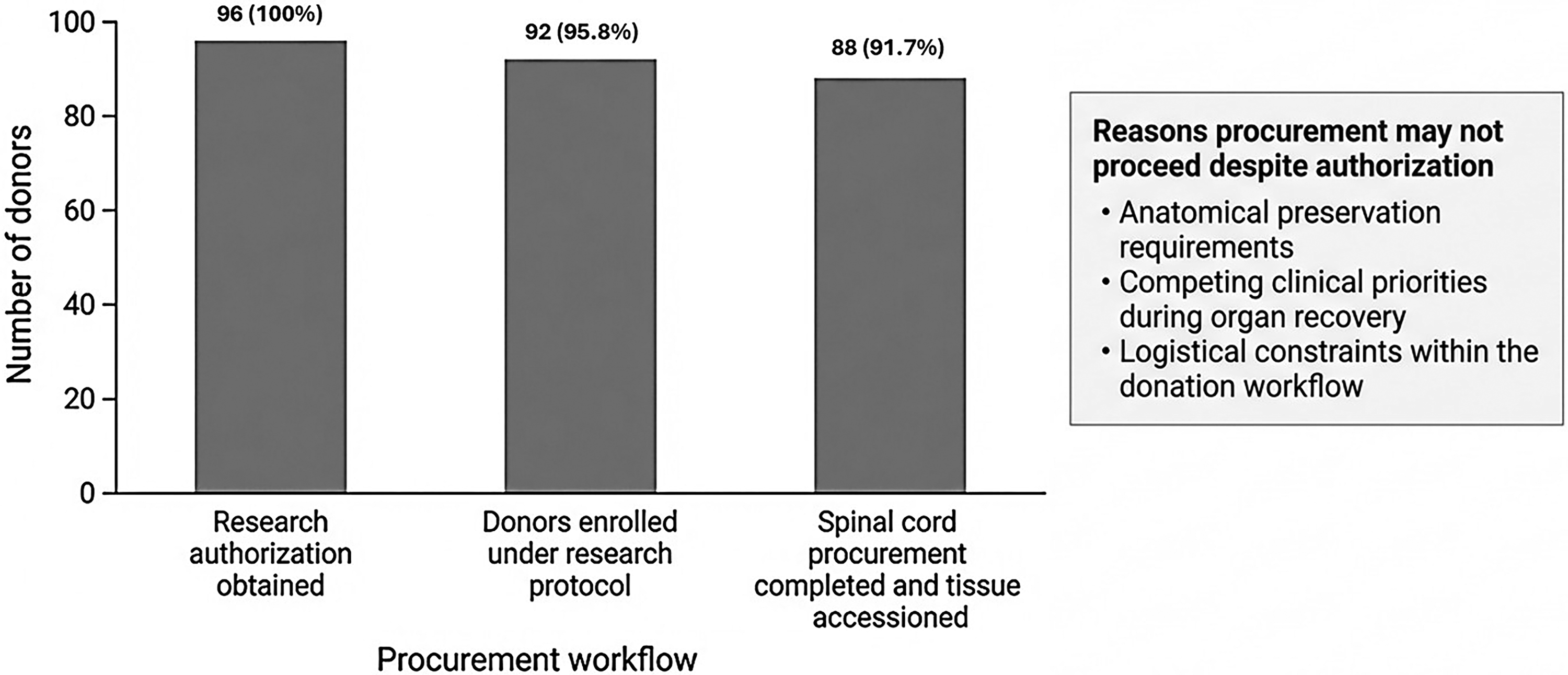
Operational outcomes of donation-integrated spinal cord tissue procurement. Bar graph summarizing workflow outcomes from the institutional donation-integrated spinal cord research program. Operational counts represent cumulative cases evaluated within the institutional program. The number of individuals providing authorization for research tissue donation, donors subsequently enrolled under the research protocol, and donors in whom spinal cord procurement proceeded with successful accession into the institutional biobank are shown. Percentages indicate the proportion of authorized donors progressing through each stage of the procurement workflow. Differences between authorization and successful procurement reflect operational constraints inherent to the donation setting, including anatomical preservation requirements, competing clinical priorities during organ recovery, and logistical limitations within the donation workflow.
Discussion
This study describes institutional practices for donation-integrated procurement of human spinal cord tissue for research, developed in response to limitations of existing tissue banking guidance. While research biobanking practices are well established in surgical pathology–based settings, those approaches are poorly suited to tissues that are anatomically irreplaceable and available only through organ donation pathways. 22 In such settings, procurement decisions must be made definitively at the point of acquisition, with limited opportunity for revision once tissue transitions from the clinical to the research domain.23,24 Most existing biobanking guidance emphasizes downstream considerations, including preservation strategies, quality control metrics, and allocation frameworks. 25 By contrast, the practices described here place primary emphasis on upstream decision making, particularly the initial determination of whether procurement should proceed at all. This shift reflects the irreversible nature of spinal cord procurement and the need for conservative upstream decision making before tissue transitions from the clinical to the research domain. Similar constraints have been reported in postmortem brain banking programs, where procurement decisions must also balance donor authorization, anatomical preservation, and downstream research utility26,27; however, spinal cord procurement introduces additional constraints related to anatomical continuity, segmental identity, and proximity to critical structures, which limit opportunities for partial or opportunistic sampling.28,29 These practices were developed through repeated evaluation of donation-integrated spinal cord procurement opportunities over an extended period within a tertiary academic hospital organ donation program. Procurement decisions were refined iteratively as consent, anatomical, operative, and institutional constraints were encountered. In many instances, procurement did not proceed, and such deferrals were treated as appropriate outcomes rather than missed opportunities. The framework presented here therefore reflects accumulated operational experience rather than a theoretical or single-instance model.
A distinguishing feature of the practices described here is the explicit treatment of the spinal cord as the primary anatomical resource. Unlike surgical pathology–based biobanking models, where tissue allocation decisions may be iterative or revisited as diagnostic priorities evolve, spinal cord procurement in the donation setting is binary and irreversible. Once tissue transitions from the clinical to the research domain, it cannot be returned, subdivided, or reallocated for clinical, educational, or transplant-related purposes. This irreversibility necessitates heightened emphasis on upstream decision making and conservative default thresholds. While some multi-tissue repositories encourage broad tissue collection when consent permits, 5 the conditional approach adopted here constrains procurement scope by requiring that associated tissues be considered only when spinal cord procurement can be achieved without compromise. This contrasts with more expansive collection strategies reported in other biobanking efforts 30 and reflects a deliberate effort to prevent incremental scope expansion driven by research demand rather than anatomical feasibility or ethical justification. Additionally, the separation of clinical judgment from research procurement described in this study aligns with ethical principles articulated in organ donation and clinical research guidance but is applied here in a more restrictive manner. In many research settings, clinical teams may play an active role in identifying or prioritizing samples for research use.31,32 By contrast, in donation-integrated spinal cord procurement, neurosurgical involvement is confined to procurement after donation priorities are satisfied, and research considerations do not influence donor management, determination of death, or operative sequencing. This separation reduces potential conflicts of interest and supports consistency across cases and institutions over time. Notwithstanding these strengths, several limitations warrant acknowledgment, including reliance on established organ donation pathways, availability of experienced surgical personnel, and coordination with institutional biobanking infrastructure, which may not be present in all settings. The approach outlined focuses on procurement decision making rather than optimization of tissue preservation or downstream analytical performance, and evolving research methodologies may therefore necessitate periodic reassessment of decision criteria. Implementation assumes the presence of integrated donation programs, neurosurgical expertise, and institutional governance structures and may not be directly transferable to centers lacking such infrastructure. In such settings, alternative or regional models may be needed to support ethically grounded spinal cord research procurement.
Conclusions
Procurement of human spinal cord tissue for research requires governance practices and decision principles that account for the unique constraints of donation-based access to an anatomically irreplaceable tissue. Emphasis on upstream decision making, explicit scope limits, and clearly defined stopping rules help preserve ethical clarity, donor dignity, and clinical primacy within organ donation settings. Rather than extending investigator-driven tissue collection models, spinal cord research banking is best situated as an institutional stewardship responsibility. While implementation depends on established donation pathways, neurosurgical expertise, and biobanking infrastructure, the decision principles articulated are not procedural mandates and can be adapted to local regulatory and operational environments. In this way, a governance-centered approach may assist centers seeking to integrate spinal cord research within organ donation programs without compromising clinical or ethical obligations.
Authors’ Contributions
S.K.J.: Conceptualization, methodology, writing—original draft, and writing—review and editing. R.V.S.: Methodology and writing—review and editing. E.C.T.: Conceptualization, methodology, writing—review and editing, and supervision.
Footnotes
Ethics Approval Statement
The spinal cord tissue procurement program operates under approval from the Ottawa Health Science Network Research Ethics Board (Protocol 20150544-01H). Tissue procurement and research banking are conducted in accordance with institutional organ donation policies and the Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans (TCPS2). Authorization for research use of donor tissue is obtained through the established organ donation consent process. The present article reports the governance framework and operational characteristics of the procurement program; no identifiable donor information is presented.
Informed Consent Statement
Institutionally approved informed consent documents have been developed to support the potential future procurement and banking of human spinal cord tissue and associated tissues. Consent is obtained from donors or their legally authorized representatives in accordance with approved ethics protocols and institutional policies. Consent is voluntary, tiered, and explicitly separated from clinical care and organ donation decision making. No identifiable personal information is included in this article.
Data Availability Statement
The article reports aggregate operational counts from an institutional tissue procurement program to illustrate implementation of the governance framework described. No individual-level datasets were generated or analyzed during the current study, which reports governance practices rather than experimental findings.
Author Disclosure Statement
The authors declare no competing financial or nonfinancial interests related to this work.
Funding Information
This work was supported by the