
Abstract
Background
Retrograde drilling is an established surgical technique to treat osteochondral lesions of the talus (OLT). It involves non-trans-articular drilling to induce subchondral bone revascularization and bone formation without damaging the overlying articular cartilage. The present study aimed to elucidate the heterogeneity of clinical studies on retrograde drilling for OLT.
Design
A systematic search of the MEDLINE, Web of Science, EMBASE, and Cochrane Library databases for studies published between January 1996 and August 27, 2022, was performed based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines by two independent reviewers. The included studies were evaluated for their level of evidence (LoE) and quality of evidence (QoE) using the Modified Coleman Methodology Score. Variables reporting surgical and clinical outcomes and complications were evaluated.
Results
Eleven studies with 207 ankles were included (mean follow-up period = 31.1 months). The mean LoE was 3.8 (LoE 3: two studies, LoE 4: nine studies), and the mean QoE was 50.8 (fair: three studies, poor: eight studies). Ten studies used the American Orthopedic Foot and Ankle Society (AOFAS) score, which improved from 57.9 preoperatively to 86.1 postoperatively. The period and protocol of conservative treatment, lesion character, surgical technique, and postoperative protocol were inconsistent or underreported.
Conclusions
This systematic review revealed that low LoE and poor QoE, coupled with heterogeneity among the included studies, impede definitive conclusions regarding the effectiveness of this technique. Consequently, well-designed clinical trials are essential to develop standardized clinical guidelines for using retrograde drilling in OLT.
Keywords
Introduction
Osteochondral lesion of the talus (OLT) is a common cartilage disorder of the ankle, typically resulting from traumatic damage to the articular cartilage and subchondral bone. 1 A systematic review published in 2010 identified that 50% of the primary symptomatic OLTs failed to resolve using conservative treatment, and operative management, including reparative procedures, was most effective with good-to-excellent clinical outcomes in about 85% of the patients. 2 Various surgical techniques, such as bone marrow stimulation, retrograde drilling, osteochondral transplantation, cartilage implantation, and chondrogenesis techniques, are available for treating OLTs; 3 however, it has been reported that none of these techniques was superior to others. 4 Despite the satisfactory outcomes of operative treatment, there are long-term clinical concerns regarding the biological deterioration of the repair. 5
Retrograde drilling is a well-known non-trans-articular procedure to induce subchondral bone revascularization and bone formation without disrupting the already damaged talar articular cartilage in OLT. 6 Lee and Mercurioin 7 first described this reparative procedure for knee lesions in 1981, and later, Taranow 6 applied it to the ankle joint in 1999. Eventually, Dahman et al. 3 reported a 68% to 90% success rate of the procedure in a systematic review based on 80 cases of OLT. 5 However, despite the substantial success rates, the authors mentioned that the heterogeneity in the included studies did not allow for pooling. Consequently, homogeneous reporting of outcome data is essential, which allows the pooling and comparison of results to propose and establish clinically relevant guidelines.
Since there is no clear approximation of the disparateness in the existing literature regarding retrograde drilling, this systematic review aimed to clarify the heterogeneity of clinical studies about retrograde drilling for OLTs. The hypothesis was that the existing literature on retrograde drilling in treatment for OLT were heterogeneity.
Methods
Study Design, Search Strategy, and Study Identification
This systematic review was carried out by two independent reviewers (Y.Y. and Y.S., both orthopedic specialists, each boasting over 10 years of experience in foot and ankle surgery, complemented by an extensive array of related publications.) according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 8 The MEDLINE, Web of Science, EMBASE, and Cochrane Library databases were individually searched from January 1996 to August 27, 2022, using the following keywords—“talus” OR “talar” OR “ankle” AND “cartilage” OR “osteochondritis dissecans” OR “chondral” OR “osteochondral” OR “osteochondrolysis” OR “transchondral” OR “osteochondral lesion” OR “OCL” OR “OCD” AND “retrograde drilling.” This search period was chosen based on the findings of a previous systematic review for OLT. 4
Article titles and abstracts were screened using specific inclusion and exclusion criteria, and full texts of potentially relevant studies were reviewed. Furthermore, citations and references of all relevant studies were manually assessed. No authors were contacted to identify unpublished data or scientific meeting proceedings. Studies were included based on the agreement of the two reviewers (Y.Y. and Y.S.); the principal author (M.T.) was consulted in the event of disagreement.
Eligibility Criteria and Study Selection
We used the following criteria for including the studies: (1) describing the clinical outcomes of retrograde drilling in OLT, (2) published in peer-reviewed journals, and (3) written in the English language. The exclusion criteria were (1) animal studies, (2) case reports, (3) studies based on <5 patients, (4) studies with inadequate or deceptive reporting of clinical outcomes, (5) studies with a combination of the surgical site and result not separated, (6) in vitro studies, and (7) review articles.
Assessing the Level and Quality of Evidence
The relevant data from each study were extracted using a standardized data sheet consisting of pre-determined fields. The level of evidence (LOE) for the included studies was assessed using the criteria published by Wright et al. 9 and Marx et al. 10 The methodological quality of evidence (QoE) was scored using a Modified Coleman methodology score, which was adapted for bone marrow stimulation for OLT in a previous study (Table 1).11-13 The QoE for each study was classified as excellent quality (score = 85-100), good quality (70-84), fair quality (55-69), and poor quality (<55).12,13 Instances of discrepancy were resolved by consensus, and if any disagreement persisted, a senior author was consulted, and a consensus was reached.
Modified Coleman Methodology Score.

MRI = magnetic resonance imaging; ROM = range of motion; WB = weight-bearing.
Data Extraction
Both reviewers independently extracted the data into an Excel spreadsheet (Microsoft 365 MSO, version 2207). Data related to the following study characteristics were compiled: author, title, year of publication, study design, LoE, QoE, diagnostic modality for OLT, OLT classification system, clinical scoring systems, the regime of preoperative conservative treatment, and follow-up period. Furthermore, patient data, consisting of the number of ankles affected, age, sex, location of the lesion, size of the lesion, cyst, method of drilling-guidance to aim lesion, size of the drill diameter, treatment (with/without bone grafting or bone void substitutes, or other biologics), clinical outcomes, surgical complications, and postoperative protocol. For evaluating the clinical outcomes, the preoperative and postoperative clinical results, radiological outcomes, the rate of patients returning to sports (RTS), and the period of RTS were collected.
Statistical and Data Analysis
All statistical analysis was performed using JMP Pro version 15.1.0 (SAS Institute Inc., Cary, NC, USA).
Results
Literature Search
Using the aforementioned search strategy, 189 studies were selected for evaluation, of which 11 studies were included in the review (Figure 1 and Table 2).6,14-23 Two of these 11 studies14,21 had an LoE of 3, while the remaining nine6,15-20,22,23 had an LoE of 4. The mean LoE was 3.8 ± 0.4. The mean QoE was 50.8 ± 6.9 (range = 43-62), with the QoE being classified as “fair” for three studies (27.3%)14,16,17 and “poor” for eight studies (72.7%).6,15,18-23 None of the studies could be classified as excellent or good quality.

Flow diagram of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
Characteristics of Included Studies.

SD = standard deviation; FU = follow up; LoE = level of evidence; QoE = quality of evidence.
Gao et al. 21 includes two groups; above: retrograde drilling, below: retrograde dripping with extracorporeal shock wave therapy.
Non-description, either prospective or retrospective study.
Study and Patient Characteristics
The 11 studies reviewed included a total of 207 ankles with OLT (see Table 2). 6,14-23 The weighted mean age of the patients included was 34.4 years; 53% of the patients were males and 47% were female. The weighted mean follow-up period was 31.1 months (range = 8-69 months) in 10 of 11 studies. 6,14-20,22,23 one study reported a follow-up period in years. 21 No study reported the outcomes for >5 years of follow-up. The duration of preoperative conservative treatment varied among studies, and the regimen was described in only six studies.6,14,15,18,19,22
Lesion Character
OLT was diagnosed using two or more imaging modalities in all studies.6,14-23 The standard plain radiograph was used in all studies,6,14-23 magnetic resonance imaging (MRI) in 10 studies,6,14-21,23 computed tomography (CT) in one study, 22 and arthroscopy in 10 studies (see Table 3). 6,14-20,22,23 Regarding the classification of OLT, nine of the 11 studies6,14,16-18,20-23 used at least one classification; of these, five articles used two14,16-18,20 or three classification systems. 6 The arthroscopic classification was the most frequently used system (used by seven studies),6,14,17,18,20,22,23 MRI-based classification was employed by six studies.6,14,16,18,20,21 It is noteworthy that the MRI and arthroscopy-based classifications were inconsistent among included studies.
Diagnostic Tools and Lesion Character in Included Studies.

XP = x-ray photograph; CT = computed tomography; MRI = magnetic resonance imaging; B/H = Berndt & Harty; ICRS = international cartilage research society; m/c/l = medial/central/lateral.
The OLT location was reported in 10 studies6,14-20,22,23 however, one study with a case-control design did not describe the location of OLT in each group. 21 The majority of OLTs were medial lesions—118 cases of medial lesions, 10 cases in the center, and 10 cases of lateral in the 138 available cases. The size of OLT was described in five studies.17,18,20,22,23 Of these, three studies had reported lesion areas on MRI,17,18,20 and two described the diameters of the lesion on CT.22,23 All OLTs were <15 mm in diameter or <150 mm2 in area, except for one study which performed endoscopic core decompression with artificial bone grafting. 20 Three studies reported the presence of subchondral cysts associated with OLT; all patients (n = 8) in one of the studies had subchondral cysts 15 and the other two had one case each.16,20 There was no mention of the size of the bone cysts in either article.
Surgical Technique
Of the 11 included studies, 10 reported the use of arthroscopic examination to evaluate the condition of the OLT before drilling (see Table 4).6,14-20,22,23 Subsequently, retrograde drilling was performed under the guidance of an imaging modality. Fluoroscopy was used in all studies.6,14-23 one study used 3-dimensional imaging-based computer-assisted retrograde drilling as a device to capture lesions accurately. 21 There was considerable variation in the diameter of the drill used—five of the used a drill with a diameter within 2 mm,14,19,21-23 three used a drill diameter within 3 to 5 mm,6,16,18 and the remaining three used a drill with a diameter >6 mm.15,17,20 Out of the six studies using a drill diameter of >3 mm,6,15-18,20 four studies implanted the bone holes created by drilling with autogenous or artificial bone in four studies.6,15,17,20 One case series investigated the usefulness of extracorporeal shock wave therapy as a postoperative augmentation therapy. 21
Surgical Techniques in Included Studies.

BMC = bone marrow cell; ESWT = extracorporeal shock wave therapy.
Postoperative Rehabilitation
The protocol for regaining the range of motion was described in eight studies.6,14,16-19,22,23 The most commonly reported time for commencing range of motion was within the first week (88%),6,14,16-19,23 followed by 4 weeks postoperatively (12%). 22 These eight studies also clearly described their protocol for weight-bearing.6,14,16-19,22,23 Regarding the period after which partial weight-bearing was permitted, one study stated the duration as 3 weeks, 23 three studies used a period of 4 weeks,14,18,22 one delayed it till 6 weeks, 6 and two studies did not clarify this.16,17 Table 5 summarizes the results of postoperative rehabilitation protocols used by different studies.
Postoperative Rehabilitation of Included Studies.

PWB = partial weight-bearing; FWB = full weight-bearing; RTS = return to sport.
While five studies started the full weight-bearing 6 weeks postoperatively,14,16,18,19,22 other studies were unclear regarding the exact time points. Regarding physical activity, seven studies described the duration and type of physical activity possible after the procedure.14,16-19,22,23 Of these seven, four studies stated that the patients were able to return to jogging at 3 months postoperatively.14,18,22,23 The time to return to full activity was described in five studies;14,18,19,22,23 the most commonly reported time was 6 months postoperatively in four studies,14,18,22,23 followed by 3 to 4 months in one study. 19
Outcomes
The American Orthopedic Foot and Ankle Society (AOFAS) score was the most frequently used tool to assess clinical outcomes.6,14-21,23 The 10 studies which used the AOFAS score described that the weighted mean AOFAS score improved from 57.9 points preoperatively to 86.1 points at a weighted mean period of 31.1 months of follow-up.6,14-21,23 The rate and time of return to play were reported by only one study as 6 months for all included patients. 23 Eight studies utilized postoperative MRI evaluation, of which most of the studies roughly reported improvement or healing of the lesions. 6,14,16-18,20,21,23 The radiological outcomes are summarized in Table 6.
Summary of Outcomes.
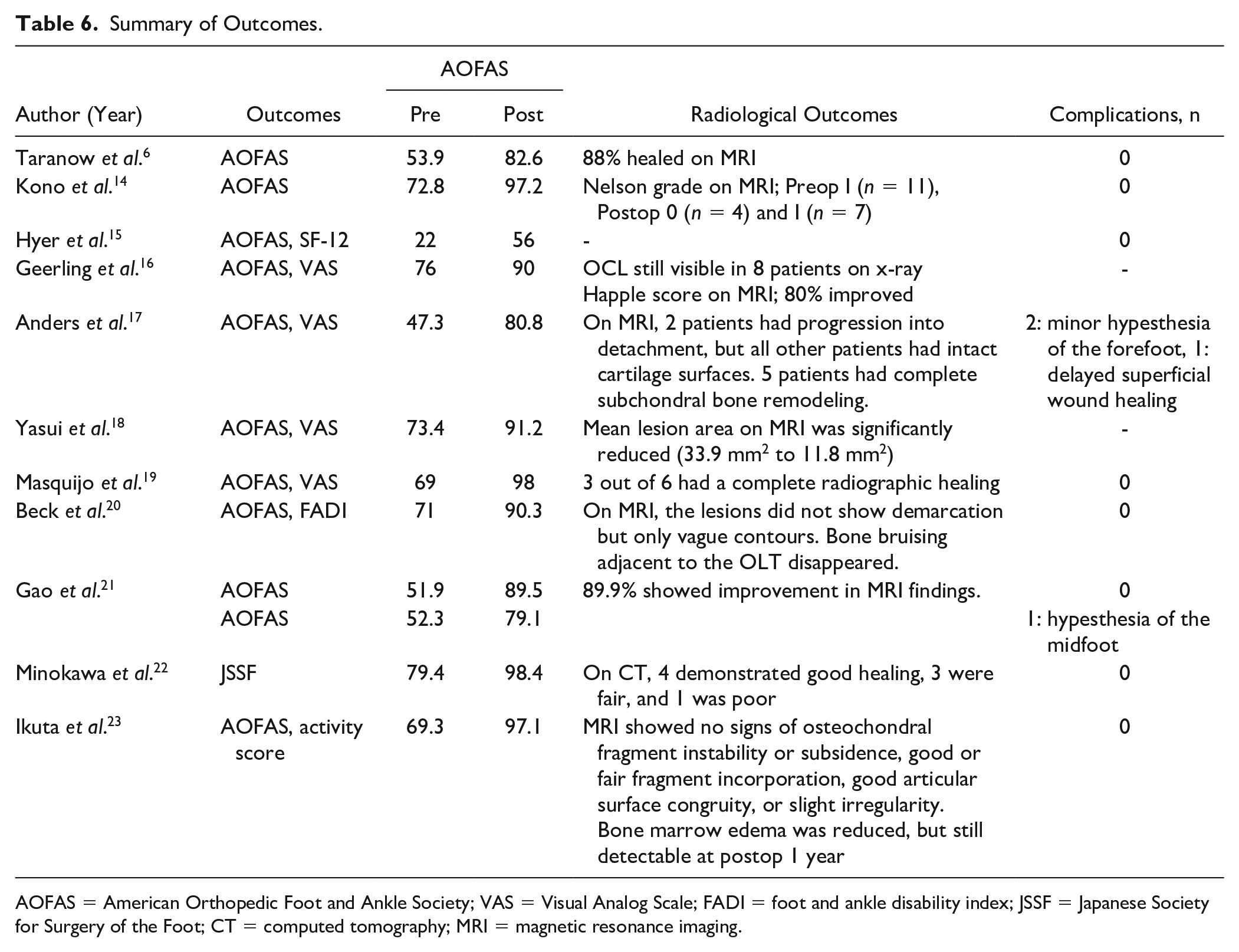
AOFAS = American Orthopedic Foot and Ankle Society; VAS = Visual Analog Scale; FADI = foot and ankle disability index; JSSF = Japanese Society for Surgery of the Foot; CT = computed tomography; MRI = magnetic resonance imaging.
The complications following the retrograde drilling were reported in nine studies.6,14,15,17,19-23 Of the total of 191 ankles in these nine studies, three patients had hypesthesia of the foot and one had a superficial wound infection.
Discussion
The present systematic review established the heterogeneity in clinical studies on retrograde drilling for OLT. Since there was underreporting of data regarding classification systems, surgical technique, and postoperative protocols, a comparison of results was not possible. Therefore, there is a need for standardized guidelines for diagnosis, treatment techniques, and postoperative rehabilitation for OLT. A majority (82%) of the included studies were classified as LoE = 4, and none of the studies could be classified as excellent or good quality. These findings highlight the need to re-evaluate the evidence upon which standard paradigms and prognostic indicators for OLT are based. In addition, our review acknowledges and contrasts with the findings of another recent systematic review published in 2023, 24 which concluded the efficacy of retrograde drilling for OLT based on existing literature. Our analysis distinctively highlights the lack of reproducibility and methodological rigor in these studies due to their heterogeneity, leading us to a different conclusion from the aforementioned review. By identifying these gaps, our review complements and broadens the scope of the current literature, offering a more comprehensive and nuanced understanding of the effectiveness of retrograde drilling.
We observed that there were significant inconsistencies in the existing literature regarding the modalities and period of conservative treatment for OLTs. Although most studies have described the period of conservative treatment, the duration was variable. Furthermore, the detailed protocol was not described appropriately in any of the studies reviewed. Currently, various conservative treatment options for OLT are available, such as nonsteroidal anti-inflammatory drugs or acetaminophen, rest and activity restriction, and cast immobilization.
25
Since the evidence regarding the best conservative treatment for OLTs remains contentious, in 2018, the International Consensus Meeting on Cartilage Repair of the Ankle (ICCRA) published consensus statements.
25
They stated that the optimal protocol for conservative management of an acute nondisplaced osteochondral lesion of the ankle is immobilization for 4–6 weeks with touchdown weight-bearing. Nonsteroidal anti-inflammatory drugs (NSAIDs) can be prescribed in cases of significant pain and swelling unless otherwise medically contraindicated
and “the duration of treatment for conservative management is highly individualized, but in general, may result in clinical improvement over the course of 3-6 months.”
In contrast to the inconsistency about the conservative treatment modalities, the process of diagnosis and indications for retrograde drilling were nearly identical across all studies. In clinical settings, a conventional radiograph is the primary imaging tool used in the diagnostic process, but the sensitivity of a plain radiograph for detecting OLT is moderate. 26 Therefore, additional imaging, such as MRI and CT, is recommended in association with clinical suspicion to increase the chances of detecting OLT. 26 Notably, most of the included studies applied arthroscopy to decide on carrying out retrograde drilling. As per the literature, retrograde drilling is commonly indicated in isolated subchondral lesions with an intact overlying articular cartilage visualized arthroscopically. 27
There were some interesting revelations regarding the lesion character. First, there was general agreement among studies regarding the location of the lesions, with medial lesions accounting for the majority (86%). A recent systematic review revealed that medial lesions accounted for approximately 70% of OLTs, 28 while another systematic review by Dahmen et al. 3 reported a 77% incidence for medial lesions. A probable reason for the significantly higher incidence of medial OLTs in the present systematic review may be due to the surgeon’s policy of performing retrograde drilling only on medial lesions in the included studies,15,20 and the fact that lateral lesions are more prone to superficial injury than medial lesions. 29 Second, the classification of OLTs varied among the included studies. Although all included studies evaluated articular cartilage properties and performed retrograde drilling, the variability in disease classification systems makes it challenging to compare results across studies. To date, many classifications for OLT have been proposed. Therefore, the ICCRA tried to establish a comprehensive classification in 2019; however, the consensus statement announced that it was difficult to establish a comprehensive classification system for OLT over the course of a single meeting. 30 Third, we observed that 45% of the included studies described the lesion size. Traditionally, retrograde drilling is classified as a bone marrow stimulation technique in which the size of the OLT is the most critical in determining whether bone marrow stimulation is indicated. 12 A systematic review by Ramponi et al. 12 in 2016 reported that bone marrow stimulation is recommended for lesions measuring <10.2 mm in diameter and 107.4 mm2 in the area. Further research is warranted to clarify whether lesion size would affect the surgical outcomes in the OLTs treated with retrograde drilling. Finally, there was no mention of the size of the subchondral cyst in any article. The ICCRA consensus statement published the following: 27
Question: For what types of lesions can bone grafting be considered? Answer: Bone grafting can be utilized in cases of lesions with large subchondral cysts, as well as in cases with large and/or deep lesions with or without subchondral cysts. Lesions with a diameter >1 cm, depth >1 cm, and cysts >100 mm3 require bone grafting. For cystic lesions, bulk bone transplantation (e.g., osteochondral autograft/allograft) should be considered.
Although the studies included in the present systematic review were published before the ICCRA consensus statement in 2018, four of the 11 studies used autogenous or artificial bone for implantation.6,15,17,20 There is a paucity of clinical evidence to support bone grafting; therefore, we suggest that further work is needed to clarify whether lesion size and the presence of bone cysts affect clinical outcomes in retrograde drilling.
Retrograde drilling is a surgical challenge since inappropriate targeting has been reported to be as high as 20%.6,31 Accordingly, several imaging modalities have been used, such as fluoroscopy, 3D-based navigated drilling, 16 MR guidance, 32 and electromagnetic navigation method. 33 Despite the introduction of multiple imaging modalities, the present systematic review revealed that most of the included studies conducted retrograde drilling under fluoroscopy with arthroscopy. The ICCRA consensus group endorsed the following recommendations regarding intraoperative imaging and a targeting device: 30 “Question: Should computer-aided navigation/robot-assisted surgery be utilized when performing retrograde drilling for a subchondral lesion of the ankle? Answer: It is unnecessary to use computer-aided navigation/robot-assisted surgery when performing retrograde drilling for a subchondral lesion of the ankle.” While the clinical outcomes reported in the included studies were generally acceptable, the limitation of fluoroscopy in consistently identifying the lesion, thereby complicating the targeting process, is noted. Although a targeting device can be used in such cases, the device is sometimes too huge for the ankle joint leading to iatrogenic cartilage injury. Also, 3D-based navigated drilling, 16 MR guidance, 32 and electromagnetic navigation method, 33 may help aim the lesion; however, their use is still uncommon in clinical settings. Although the results of the present systematic review do not shed light on the incidence of such cases, it is desirable to develop an accessible surgical technique or device that can perform accurate retrograde drilling in such cases.
We also observed that the diameter of the retrograde drill was inconsistent among the included studies. Currently, the diameter of the retrograde drill is under discussion, 27 although bone marrow stimulation techniques for OLT offer favorable outcomes.4,12 A recent challenge has been the inevitable deterioration of the regenerated or grafted cartilage. 34 Several risk factors for this deterioration have been described—recent clinical studies regarding microfractures suggest that subchondral bone deterioration may be one of the risk factors. 27 A recent systematic review of animal studies stated that the issue of subchondral bone damage and restoration should be addressed by these bone marrow stimulation techniques. 35 An experimental cadaveric study showed that smaller drill holes (1 or 1.25 mm) posed less damage to the subchondral bone compared with larger drill holes (2 mm). 36 Therefore, it is reasonable to suggest that a small-diameter drill may help avert or at least minimize damage to the subchondral bone. Retrograde drilling of the OLT was first introduced by Taranow et al. 6 in 1999; they used 3.5 to 4.5 mm diameter drills. Subsequently, smaller diameter drills were used. The consensus group published the following comment on the drill diameter: 27
Question: What size drill can be utilized for retrograde drilling of a subchondral lesion of the ankle? Answer: A 1–2 mm diameter K-wire can be utilized for retrograde drilling of a subchondral ankle lesion. Care should be taken not to overdrill the subchondral lesion and cause iatrogenic damage to the subchondral bone.
In our experience, retrograde drilling performed using a small-diameter drill requires caution, especially in young OLT patients, because the drill may bend or break in the relatively hard bone during the procedure. Although such complications were not confirmed in the included studies, further research is warranted to identify the ideal drill diameters to ensure adequate short- and long-term clinical results and prevent intraoperative drill breakage.
In several studies, bone grafting or bone void substitutes were applied through a retrograde approach in lesions, offering satisfactory clinical outcomes,6,15,17,20 whereas retrograde drilling alone was effective in others.5,16,18,19,22,23 Technically, subchondral cysts are filled with bone grafts or bone substitutes via the bone hole made during retrograde drilling. However, using a bone graft to fill a defect for a saucer-shaped cyst through a retrograde approach may be challenging. In these cases, bone void substitutes are preferred because they flow to all irregularly shaped defect recesses, thereby eliminating the risk of iatrogenic cartilage damage.37,38 To our knowledge, no studies have compared the efficacy of autogenic cancellous bone grafting versus bone void substitutes. We recommend additional research to clarify the indications and benefits of bone grafting.
Despite the extensive use of retrograde drilling, the present systematic review revealed inconsistencies in the optimal time points to progress postoperative rehabilitation. This variability obscures an objective comparison of these studies. Recently, the ICCRA consensus group proposed the general idea of postoperative rehabilitation: 39
In general, the rehabilitation strategies allow the patient to return to activities by (1) allowing biological healing through limiting shear forces and (2) progression of activities based on a clinical evaluation. The clinical evaluation when deciding whether to progress rehabilitation activities is based on the following factors: pain, proprioception, stability, and swelling. Ideally, shear forces on the OLT should be limited to 3 months when rehabilitation/training can be progressed. Generally, sport-specific training is considered 3 to 6 months after the surgery, and return to competition after ankle cartilage repair is considered 6 months to 1 year after the surgery.
We found that the clinical outcomes following retrograde drilling were satisfactory. Most studies have reported a >85-point increase in the postoperative AOFAS scores at short-term follow-up.6,14-21,23 Despite significant success rates, the generalizability of the current literature is limited by a lack of follow-up studies evaluating the long-term outcomes after retrograde drilling for OLTs. In addition, the rate and time of return to play were reported by only one study, 23 which underscores the need for future clinical research. Regarding radiological outcomes, most of the studies reported improvement or healing of the lesions on postoperative MRI, but there is a lack of data on the extent of subchondral change. As subchondral bone damage is gaining importance in recent research in the field of bone marrow stimulation procedures, 35 changes in the subchondral bone over time after retrograde drilling should be carefully investigated.
There were certain limitations to this review. The first limitation was that the search was conducted nearly 1 year ago. The systematic review conducted by Livas revealed that the average time from literature search to publication of systematic reviews in orthodontics is approximately 13.2 months. 40 This duration is irrespective of the journal type and reflects the typical processing time within academic publishing. Our study’s timeline, therefore, falls within the standard range observed in similar scholarly works. Second, most studies were retrospective case series with a wide range of inconsistencies of reporting variables. The level and quality of evidence offered by the included studies were limited. Moreover, the included studies had short to mid-term follow-ups, causing a considerable risk of bias. Also, due to the low number of included patients in each study, a well-powered novel prospective study is necessary. The most reported clinical outcome in the included studies was the AOFAS score; although a strong measurement tool for functional outcomes after a foot and ankle injury, this score has never been validated for retrograde drilling for OLTs. Therefore, there is a significant chance of bias due to overestimation or underestimation. Finally, recent advancements include techniques using adipose-derived stem cell augmentation via either conventional 2.7-mm arthroscopes with a 30° viewing angle 41 or needle arthroscopy. 42 These methods potentially enhance surgical outcomes through biological augmentation. Accordingly, the results of the present summative analysis on retrograde drilling should be interpreted with caution.
Conclusion
The review revealed heterogeneity in the existing literature on retrograde drilling for OLT treatment, with findings of low LoE and poor QoE among the included studies. Several surgical considerations of this technique confound the interpretation of its clinical outcomes. Based on the present review, we recommend that future research on retrograde drilling should aim to offer high-quality evidence through consistent data reporting. For this purpose, well-designed clinical trials with standardized criteria for patient selection, lesion characterization and classification, surgical technique, postoperative protocol, and validated outcome measurements are warranted to develop clinical practice guidelines for retrograde drilling for the treatment of OLT.
Footnotes
Acknowledgments and Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.