
Abstract
Objective
Medial meniscus tear (MMT) is a common method to induce osteoarthritis in rats, but mimics secondary osteoarthritis. A novel method of carrying out a medial wedge closing tibial osteotomy (TO) has been recently developed to induce primary osteoarthritis. This study aims to validate it, compared to MMT.
Methods
Twenty rats were divided equally into 2 groups. Outcome measures such as histology graded according to Osteoarthritis Research Society International (OARSI) guidelines and computed tomography (CT) scans were analyzed at 6 weeks post-operatively. Observational gait analysis and serum biomarkers such as C-terminal cross-linked telopeptides of type II collagen (CTX-II) and interleukin-1 beta (IL-1β) were collected at 2-weekly intervals up to 6 weeks post-operatively.
Results
Serum CTX-II and IL-1β levels did not reveal a statistically significant difference across all time points between the 2 groups. CT grading was significantly more severe (2.80 ± 1.10 vs 1.40 ± 0.548, P = 0.0389) in the MMT group compared to the TO group. In addition, histological gradings such as calcified cartilage score (2.10 ± 1.91 vs 0.00 ± 0.00, P < 0.01) and cartilage degeneration score (4.80 ± 5.18 vs 0.00 ± 0.00, P < 0.01) revealed significantly more severe osteoarthritis in the MMT compared to TO group. Synovial membrane score did not reveal a statistically significant difference (1.10 ± 0.994 vs 1.00 ± 0.00, P = 1.00).
Conclusion
TO is a novel method in inducing primary osteoarthritis in the rat model compared to MMT between the 6 and 12 weeks’ time frame.
Introduction
Osteoarthritis is a debilitating disease caused by articular cartilage degeneration and destruction, causing patients persistent pain, disability, and a decrease in quality of life.1-3 Primary osteoarthritis is a subtype that is due to degeneration and is the more common subtype. 4 Secondary osteoarthritis, in contrast, is due to secondary causes and represents the minority. 4 The pathophysiology of osteoarthritis is currently poorly understood and is postulated to be due to multifactorial etiology from causes such as genetic or environmental factors. 5 To date, there is a lack of effective treatment of the condition. 6
As part of the study of osteoarthritis, there are various social and ethical difficulties in recruiting patients with early osteoarthritis to investigate therapeutic procedures and to study the pathophysiology of the condition. 7 As a result, various animal models have been developed as a work around this issue.8-10 This ranges from the type of animals used such as small animals, for example, rats or guinea pigs, to large animals, like monkeys or horses,11-14 to the method of induction of osteoarthritis—namely, spontaneous, chemical, or mechanical methods. 15 While spontaneous induction methods have been able to mimic the progression of primary osteoarthritis, they tend to involve waiting for a long period of time (months to years). On the contrary, while chemical or mechanical methods take a faster period of time (days to weeks), these methods commonly mimic the pathophysiology of secondary osteoarthritis instead. Previous studies have also shown that the pathophysiology of primary osteoarthritis involves many factors, ranging from systemic inflammation to biomechanics of the joint.16,17
A rat model offers a cheaper alternative to the various other animal models and is easier with the lower space requirements in housing and handling of the animals. 8 The most common methods for induction of osteoarthritis in these rat models include anterior cruciate ligament transection or medial meniscus tear surgery.18,19 However, as these methods involve causing joint instability, it mimics secondary osteoarthritis more than primary osteoarthritis. A novel method described by Britzman et al. 20 involved carrying out a medial wedge closing tibial osteotomy to alter the biomechanics of the knee and overload the medial compartment of the joint. The benefits described in that paper include a surgical procedure that does not involve intra-articular surgery that may potentially confound the pathology of the degenerative disease due to the added inflammation when breaching the joint capsule, as well as that it models primary osteoarthritis better. 20
To the authors’ knowledge, there is paucity in the literature comparing this novel method against existing methods in rodent studies. In addition, over the course of 14 weeks in that study, severe osteoarthritis was found at the end of the study period in the tibial osteotomy group. The authors hypothesize that the tibial osteotomy would likely be a better model in mimicking primary osteoarthritis and allowing us to study early changes. The aim of this study was hence to (1) validate that the tibial osteotomy method is a better method for inducing primary osteoarthritis in rats based on radiological grading and histology and (2) to find out if the tibial osteotomy method can be used to show early osteoarthritis instead of studying the pathology once it has reached severe stages.
Methodology
Ethical Considerations
Approval was obtained from Institutional Animal Care and Use Committee (IACUC) prior to commencing of this study (IACUC 2021/SHS/1647) and all procedures were performed strictly in accordance with guidelines and regulations. A total of 20 healthy adult, male Sprague-Dawley rats from a local vendor (InVivos Singapore) that were 12 weeks old and weighing between 350 g and 450 g were used for this study. During the entire study, they were kept in groups of 2 and 3 in individually ventilated cages that were at least 1500cm3 and were provided with food and water ad libidum. They were acclimatized for 1 week in the laboratory environment before handling was performed.
Groups
Twenty male Sprague-Daley rats were randomly divided into 2 groups by a laboratory assistant blinded to the study methodology. Ten rats underwent a medial closing wedge tibial osteotomy procedure as described below, to increase loading on the medial compartment of the right knee—TO group. The other 10 rats underwent a medial meniscus tear as described below as well to the right knee—MMT group. The left knee acted as the control in this study.
Pre- and Post-Operative Procedure
The rats were respectively anesthetized using inhalational anesthetic agents consisting of 5% isoflurane with oxygen as carrier gas in a gas chamber and maintained on inhalation mask at 2% isoflurane. The rat was subsequently placed on a heating pad covered with a non-sterile drape. Prior to commencing the surgery, prophylactic analgesia and antibiotics consisting of 0.05 mg/kg buprenorphine and 10 mg/kg enrofloxacin were administered subcutaneously. Fur on the leg was clipped liberally, before cleansing and draping as per standard surgical procedure. Sterile surgical instruments were used throughout the entire procedure.
Post-operatively, the rats were placed on the heating pad for 30 min and monitored for full recovery before returning to their single cages. They were monitored daily for pain and post-operative analgesia was given for a period of 5 days and subsequently on an as needed basis, as part of the study protocol. Upon reasonable recovery after approximately 10 days, they were returned to their original cages.
Post-operatively, 3 rats had post-operative complications. One rat from the MMT group sustained wound dehiscence on post-operative day 1, while 2 rats from the TO group sustained wound dehiscence on post-operative days 1 and 2, respectively. These complications were found during wound dressing for the rats post-operatively, and wounds were cleansed with cetrimide and hexanol solution (chlorhexidine 2% and isopropyl alcohol 70%) before debriding and closing the dehisced wound. There were no further complications thereafter and the rats progressed uneventfully.
Medial Meniscus Tear
Ten rats underwent a surgical procedure to create a right knee medial meniscus tear. A curvilinear incision was made to the medial aspect of the right knee and bluntly dissected until the medial collateral ligament was exposed and transected. Dissection of the joint capsule was done to expose the medial meniscus, where a full-thickness radial tear was made. The surgical site was subsequently closed in layers and tissue glue was used to reinforce the skin closure.
Tibial Osteotomy
The other 10 rats underwent a right medial closing wedge tibial osteotomy, where the surgical procedure was done similar to the steps detailed in the study carried out by Britzman et al. 20 A longitudinal incision was made to the lateral aspect of the right proximal tibia of the rat, extending from just distal to the knee joint toward the ankle joint. With a pre-bent 30o metal plate temporarily secured to the proximal tibia with a screw, the medial wedge tibial osteotomy was performed. The osteotomy was then closed to match the pre-bent angle of the plate, and the rest of the screws were inserted for a total of 2 proximal and 2 distal screws. Closure and post-procedure care were done as described above. Figure 1 illustrates the steps undertaken for the procedure.
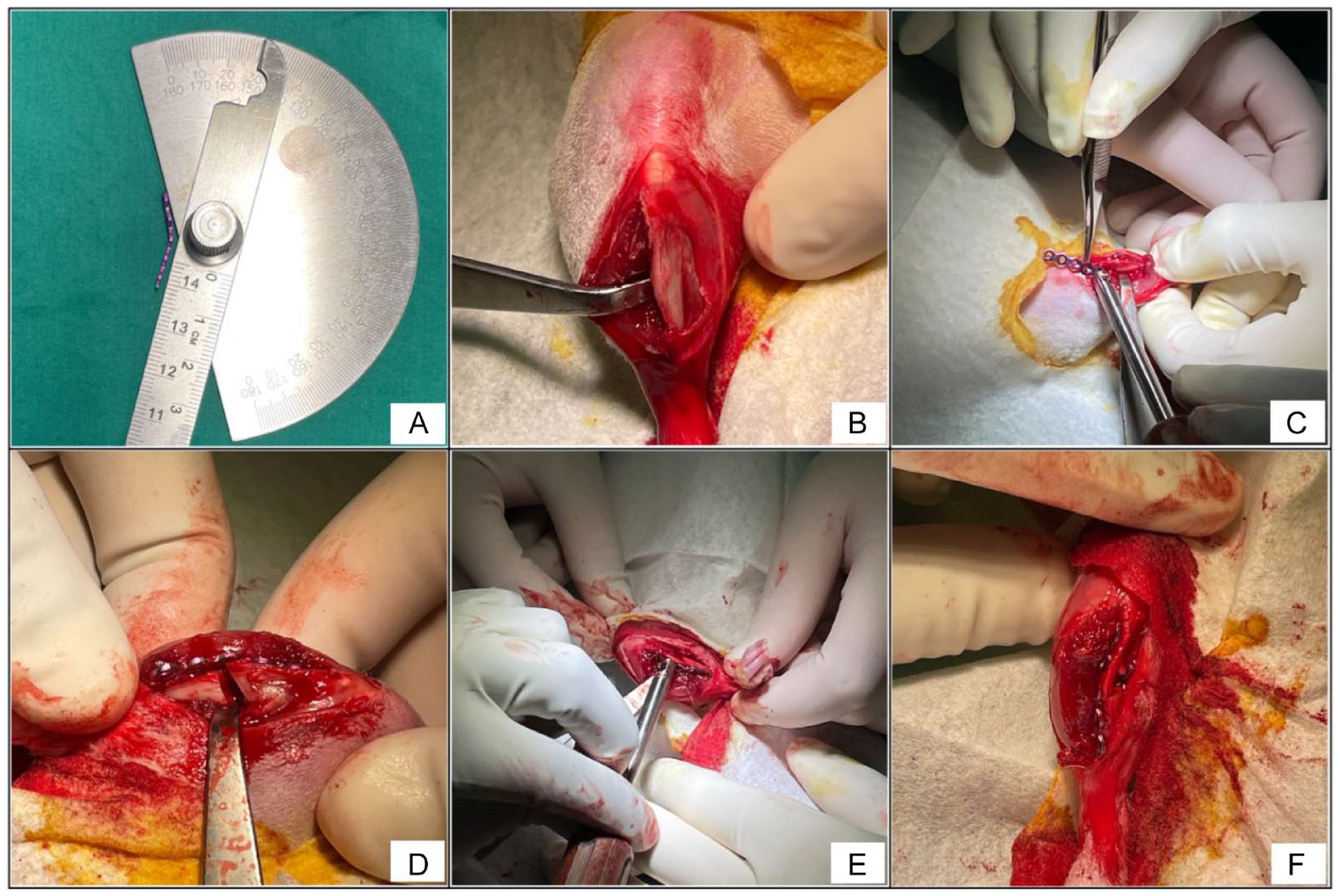
Intra-Operative Steps for Tibial Osteotomy. (
Animal Observations and Kinematics
The body weight of the rats was measured at 2-weekly intervals, and gait observation was performed pre-operatively and at 2, 4, and 6 weeks post-operatively, prior to euthanasia. The animals were allowed to walk around a 5m long platform to observe their gait (

Clinical photograph demonstrating gait observation along a platform.
Serum Analyses
Blood samples from the rats were collected from animals following the Animals Scientific Procedures Act 1986 (ASPA) guidelines pre-operatively and 2, 4, and 6 weeks post-operatively. They were collected from a peripheral vein using a 25- or 27-gauge needle under aseptic technique and placed in a 2-ml vacutainer for 30 min to allow the blood to clot. Following that, the samples were spun on a centrifuge at 1200g for 15 min. Serum was removed from the container with a pipette and separated into 50 µl Eppendorf tubes and frozen at −80°C until required. Blood samples were sent for serum pre-clinical CartiLaps® C-terminal cross-linked telopeptides of type II collagen (CTX-II) Enzyme Immunoassay (EIA) and rat interleukin-1 beta (IL-1β) enzyme-linked immunosorbent assay (ELISA) kit (R&D systems, Oxford, UK).
Radiological Imaging
Radiological investigation was done through a Positron Emission Tomography-Computed Tomography (PET-CT) scanner (MultiScan™ LFER PET/CT) at 6 weeks post-operatively, with each rat anesthetized through the protocol as described above. Specimens were scanned with an X-ray source with a power of 80 kVp/250 μA. The voxel size was medium with an exposure time of 200 ms. The cross-sectional images were reconstructed using the Interview FUSION Software, where 710 projections were reconstructed over the knee joint (
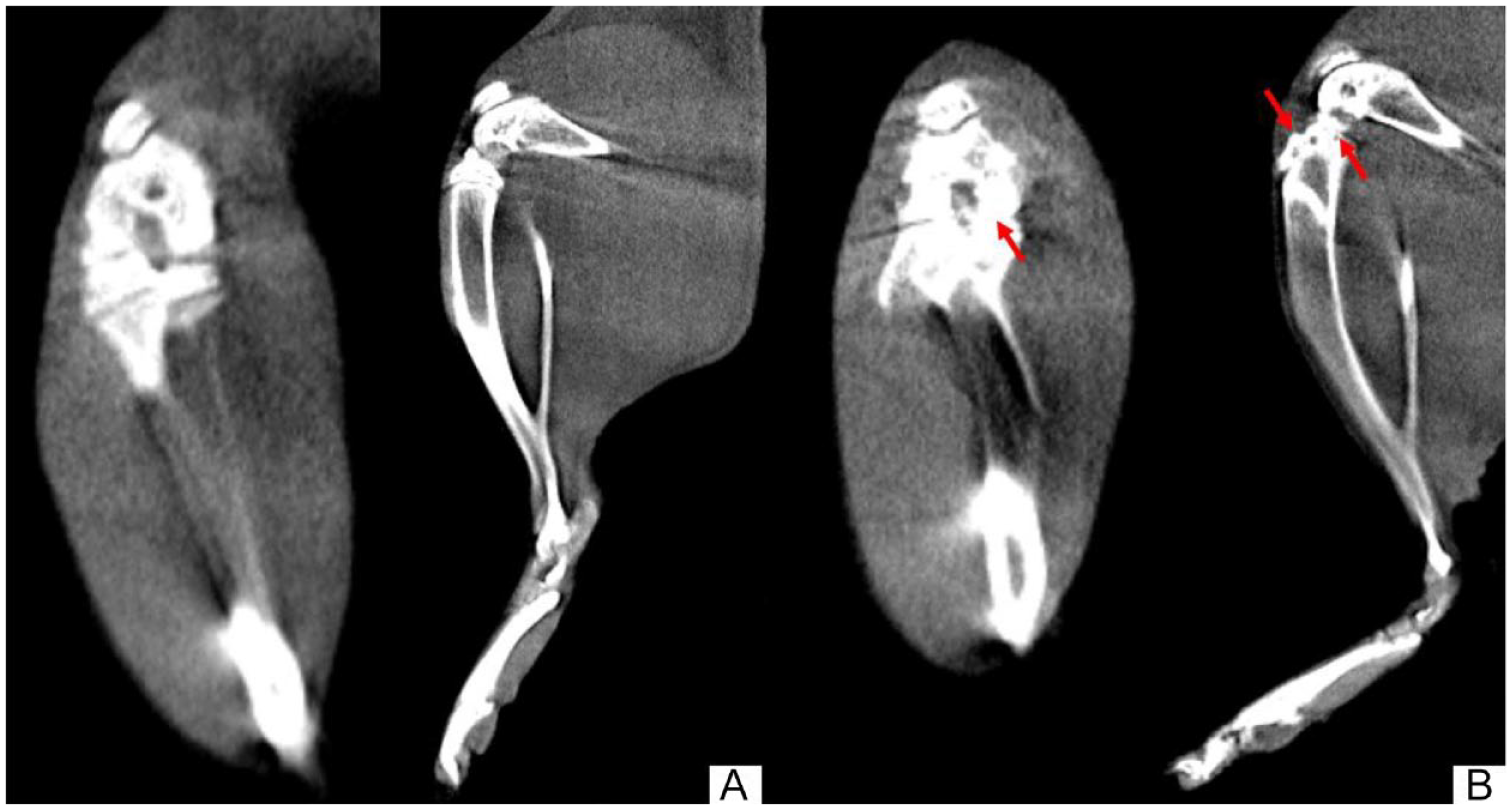
Computed Tomography (CT) Scan of the Rat’s Right Knee in Coronal and Sagittal Planes. (
Histological Evaluation
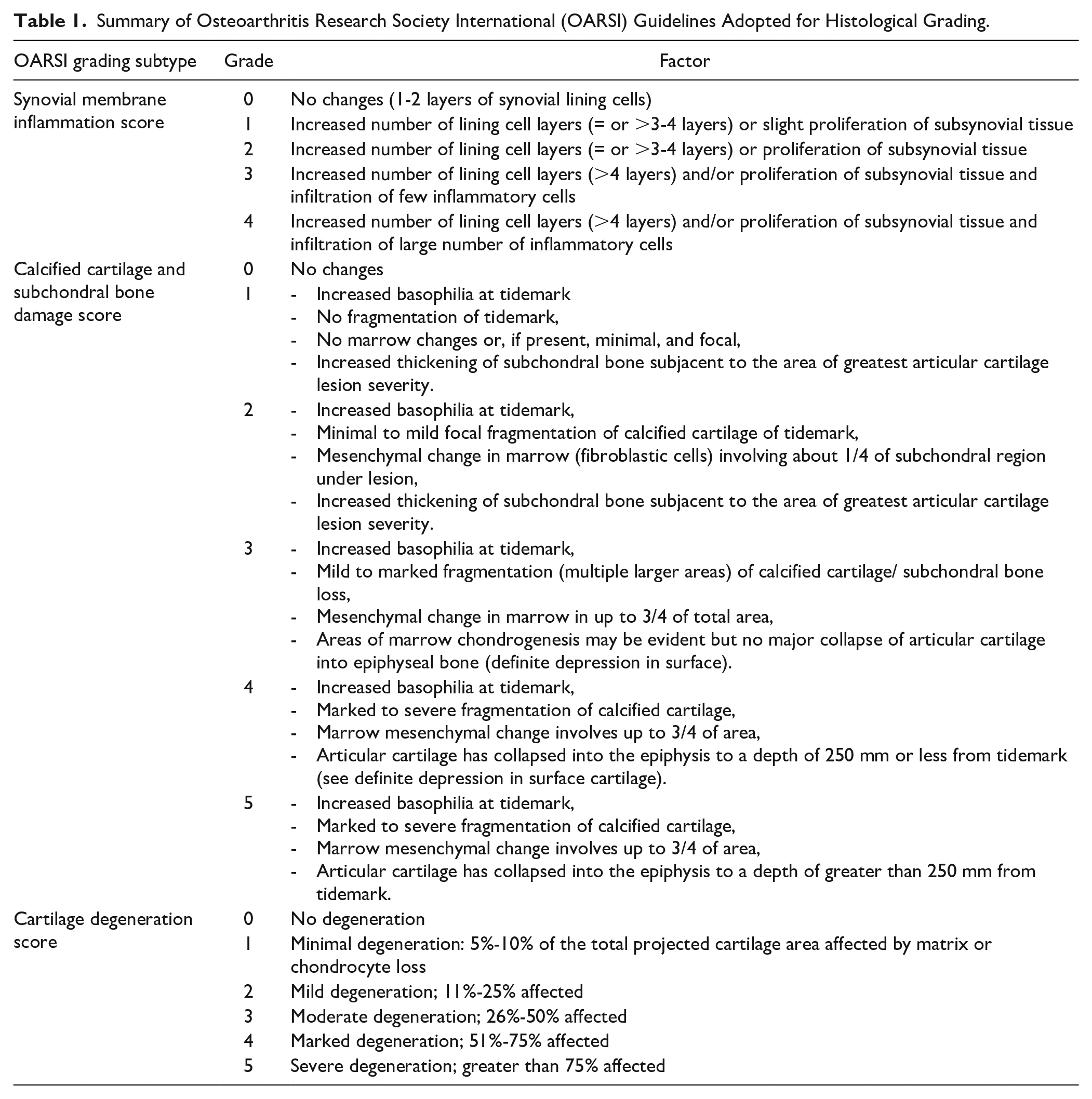
After final investigations were done on the animal specimens, the rats were subsequently euthanized by overdose intraperitoneal injection of pentobarbitone at 6-week post-operative period. The knees were dissected and kept in 10% neutral buffered formalin (NBF). Following the preparation of the knee joint as specimens, 10-µm sections were taken every 100µm through the specimen and stained with toloudine blue. Two sections per knee were scored for lesion width, depth, and area as per Osteoarthritis Research Society International (OARSI) guidelines and final scoring was done for synovial inflammation, calcified cartilage, and cartilage degeneration scorings. 22 Histological analysis and grading were carried out by a pathology research assistant blinded to the study. Figure 4 illustrates the histological samples comparing different OARSI grades, and Table 1 summarizes the OARSI histological grading subtypes used in this study.
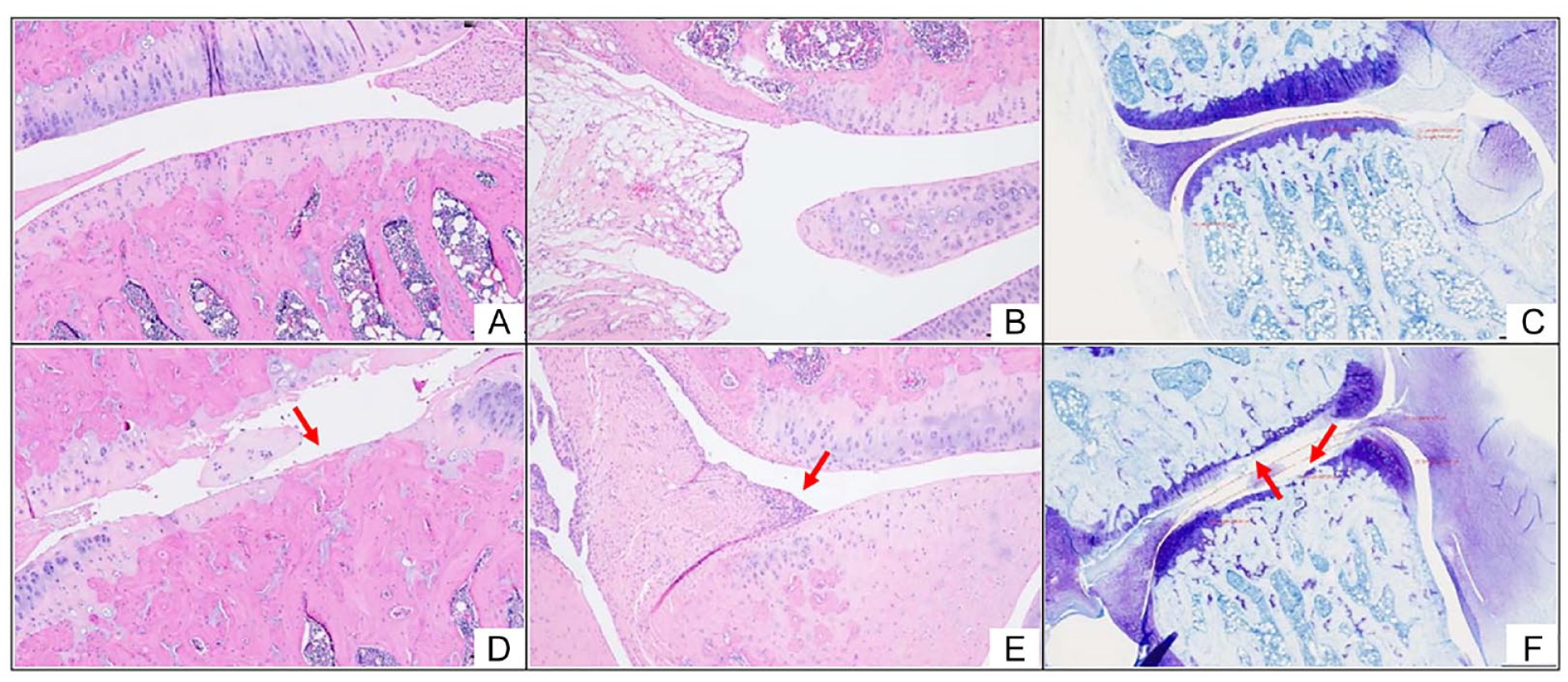
Histological findings comparing findings of different OARSI grades. (
Summary of Osteoarthritis Research Society International (OARSI) Guidelines Adopted for Histological Grading.
Statistical Analysis
All continuous variables were expressed as a mean and standard deviation from the mean. Statistical significance was defined at an alpha of 0.05 (p ≤ 0.05). To ensure a large enough sample size, a power analysis was performed using G*Power 3.1 23 using histological parameters from the study conducted by Elsaid et al. 24 on the ACLT rat model of OA. The power analysis indicated that a minimum of 5 animals in each group is required to obtain 95% power to detect significant differences at the 0.05 level of significance. The authors chose to include 10 animals in each group to account for unforeseen complications or issues during the course of the study where animals were excluded to prevent confounding of results. Unpaired and paired T-Tests were conducted on normally distributed variables between or within the surgical groups, respectively, while Wilcoxon Signed-Rank test and non-parametric tests such as Mann-Whitney U tests were carried out on non-normally distributed variables. All statistical tests were performed using Python 3.9.7 and its publicly available statistical libraries (Pandas 1.4.3, SciPy 1.9.0, and NumPy 1.23.0).
Results
Overview
There was no statistically significant difference between the weight of MMT vs TO rats across the pre-operative and 2, 4, 6 weeks post-operative timepoints, respectively (396 ± 21.1 vs 409 ± 18.1, P = 0.0961; 404 ± 36.9 vs 399 ± 38.6, P = 0.820; 438 ± 34.4 vs 450 ± 26.1, P = 0.406 and 451 ± 44.8 vs 471 ± 35.4, P = 0.252). The rats were ambulating well and there was also no significant difference when comparing their gait between the two groups ( Table 2 ). Across all time points, none of the rats exhibited signs of acute stress reactions such as significant weight loss or poor intake of food.
Weight and Gait Comparison between MMT and TO.
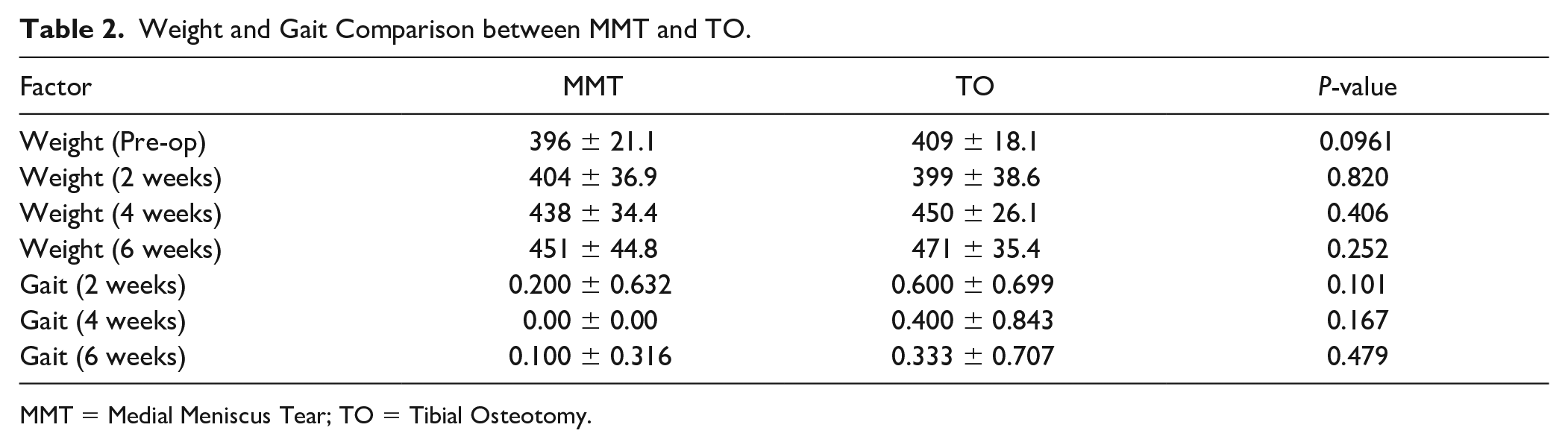
MMT = Medial Meniscus Tear; TO = Tibial Osteotomy.
Operated Leg Vs Control Leg
In both groups, osteoarthritic changes were seen when comparing the operated (right) leg against the control (left) leg as shown when comparing CT grading as well as histological results. For the MMT group, CT grading in the operated leg showed significantly worse osteoarthritis as compared to the control leg (2.80 ± 1.10 vs 0.200 ± 0.447, P = 0.0123). Histological results showed a similar trend where synovial membrane inflammation score (1.10 ± 0.994 vs 0.00 ± 0.00, P = 0.0158), calcified cartilage score (2.10 ± 1.91 vs 0.00 ± 0.00, P = 0.0235) and cartilage degeneration score (4.80 ± 5.18 vs 0.00 ± 0.00, P = 0.0273) were worse in the operated leg as compared to the control leg ( Table 3 ).
Outcomes Within MMT Group—Operated Vs Control Leg.
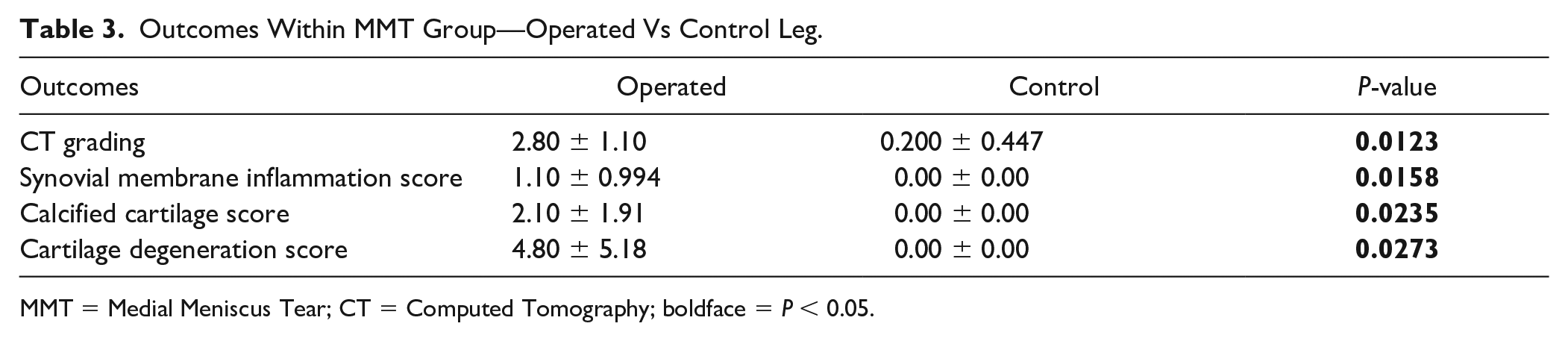
MMT = Medial Meniscus Tear; CT = Computed Tomography; boldface = P < 0.05.
In the TO group, CT grading was similar (1.40 ± 0.548 vs 0.00 ± 0.00, P = 0.0625) when comparing the operated knee against the control knee, respectively. Despite not being statistically significant, CT grading in the operated knee trended to more severe osteoarthritis when compared to the control. Histological grading showed similar results of early osteoarthritis in the operated knee, where only synovial membrane score showed significantly worse osteoarthritis when comparing operated leg (1.00 ± 0.00 vs 0.20 ± 0.00, P < 0.01) to the control. Calcified cartilage score and cartilage degeneration score did not show any statistically significant differences ( Table 4 ).
Outcomes Within TO group—Operated vs Control Leg.
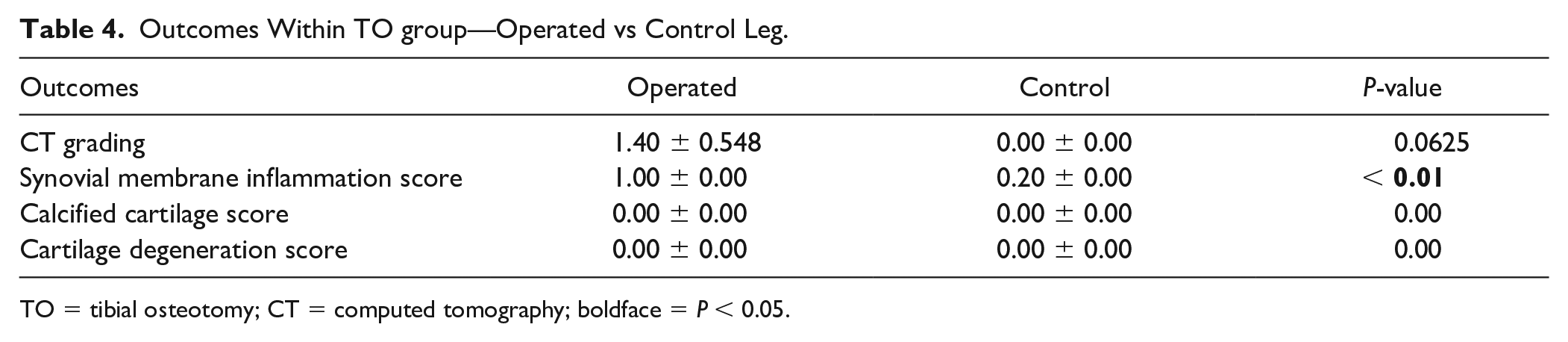
TO = tibial osteotomy; CT = computed tomography; boldface = P < 0.05.
MMT Leg Vs TO Leg
When comparing the operated knees between groups, rats that underwent MMT surgery appeared to have more significantly severe osteoarthritic changes noted on CT grading at the end of the 6 weeks (2.80 ± 1.10 vs 1.40 ± 0.548, P = 0.0389). In addition, histological scores also revealed significantly severe osteoarthritis in the MMT group as compared to the TO group. These include calcified cartilage score (2.10 ± 1.91 vs 0.00 ± 0.00, P < 0.01) and cartilage degeneration score (4.80 ± 5.18 vs 0.00 ± 0.00, P < 0.01). However, synovial membrane inflammation score did not reveal statistically significant differences when comparing MMT versus TO, respectively (1.10 ± 0.994 vs 1.00 ± 0.00, P = 1.00).
Serum Analysis
In terms of Serum CTX-II levels, comparison between the 2 groups did not reveal a statistically significant difference at pre-operative, 2-weeks, 4-, and 6-week levels, respectively (58.2 ± 12.9 vs 65.2 ± 18.6, P = 0.8125; 48.2 ± 14.0 vs 52.3 ± 18.6, P = 0.307; 41.9 ± 8.31 vs 44.5 ± 10.0, P = 0.623 and 26.6 ± 11.0 vs 29.7 ± 5.96, P = 0.427). A similar trend was found for serum IL-1β levels across the same timepoints (12.8 ± 7.15 vs 9.98 ± 11.8, P = 0.8125, 13.34 ± 20.4 vs 15.6 ± 14.1, P = 0.448; 9.68 ± 10.3 vs 10.3 ± 3.99, P = 0.618 and 10.5 ± 22.7 vs 4.93 ± 7.97, P = 0.894). Serum CTX-II levels in the MMT group appeared to be down-trending across the 6 weeks, with the TO group displaying a similar pattern. Serum IL-1β levels in both groups appeared to follow a similar down-trending pattern throughout the specified time period. Table 5 summarizes the results, while Figure 5 provides a visual illustration of it.
Outcomes Between MMT Versus TO.
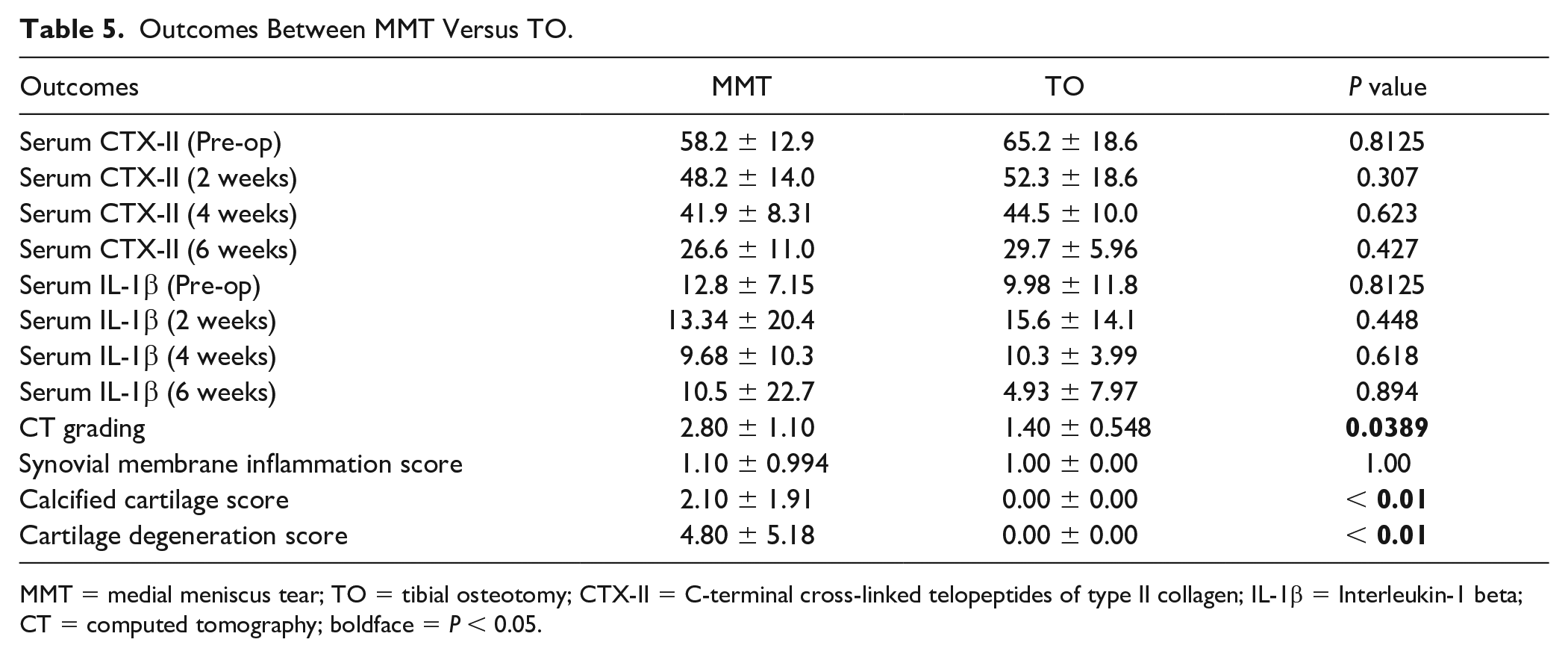
MMT = medial meniscus tear; TO = tibial osteotomy; CTX-II = C-terminal cross-linked telopeptides of type II collagen; IL-1β = Interleukin-1 beta; CT = computed tomography; boldface = P < 0.05.
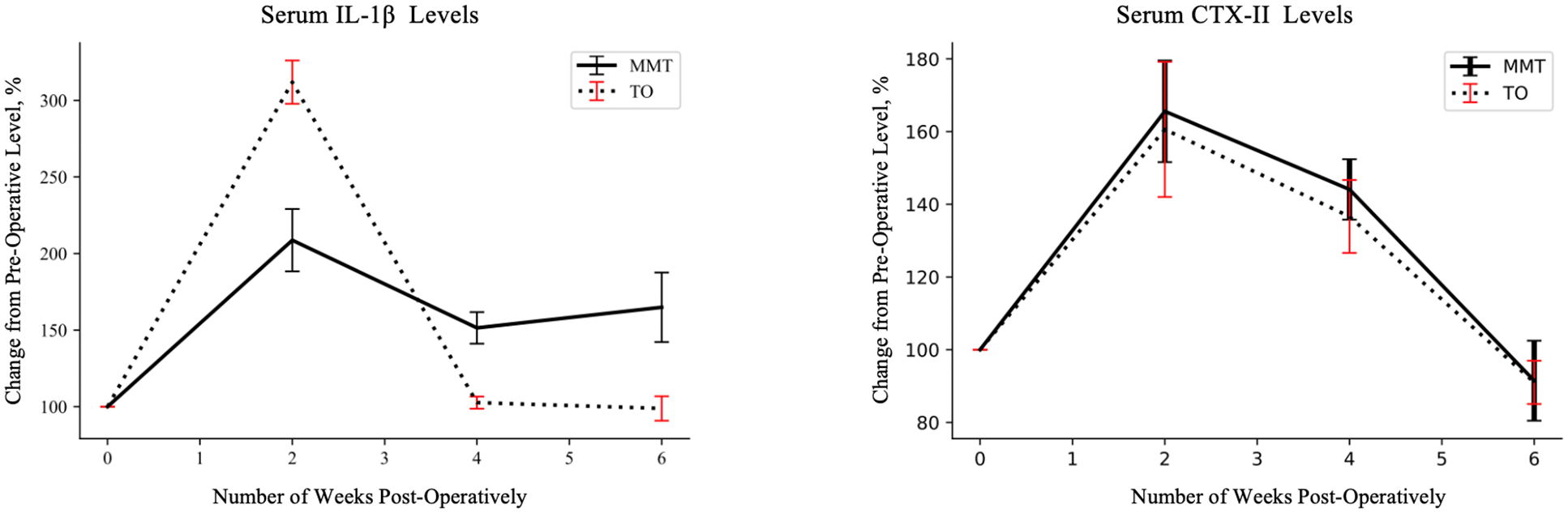
Serum analysis levels taken across the study period at 2-weekly intervals, compared to pre-operative levels.
Discussion
The most important finding of this study was the more severe radiological and histological osteoarthritic changes in the MMT group compared to the TO group, which itself had significant pathological changes when comparing it to the control group. Currently, one of the most common methods of the surgical induction of osteoarthritis in the rat model involves an MMT surgery. 15 However, the MMT model in rats tends to mimic post-traumatic osteoarthritis more, and involves intra-articular surgery which compounds the synovial inflammation in the study, leading to an inaccurate representation of primary osteoarthritis.20,25 A recent study carried out by Britzman et al. 20 showed that a novel method of carrying out a medial wedge closing tibial osteotomy in rats to load the medial compartment in the knee joint was an effective way of circumventing these challenges and expediting the progression of primary osteoarthritis in the knee. Despite showing this, the aforementioned study showed that TO induced severe primary osteoarthritis at 12 weeks post-surgically, without comparing it to an MMT model within the study. 20 In contrast, this study has suggested that the TO model is indeed a better model for inducing early primary osteoarthritis in rats as compared to the MMT model, which already showed signs of severe osteoarthritis at the 6 weeks post-operative time period, where CT grading was more severe in MMT compared to TO. To the authors’ knowledge, this has not been done before among existing studies, and there is crucial value in identifying early osteoarthritis in rat models. In the study of osteoarthritis, there are various therapeutics that have been administered and trialed.26-28 However, these are given early or even immediately post-operatively after the surgical procedure has been carried out to illustrate how these therapeutics delay the onset of the condition. 29 This is of seemingly little value as few studies have looked into the efficacy of these therapeutics, but instead, only the preventive value of these drugs, which may not translate to clinical benefits as most primary osteoarthritis in humans would have already begun.
When comparing histological results between the two groups, more severe calcified cartilage and calcified degeneration scores were found in the MMT group compared to the TO group. This reflects the more severe and extensive osteoarthritis that has formed in the MMT group. Synovial membrane inflammation score was, however, similar between the two groups. Synovial tissue inflammation is one of the first few effects and stages in early osteoarthritis, whilst cartilage calcification and degeneration happen during the later stages. 30 The authors postulate that this could be the reason behind the histological results, where synovial membrane inflammation has occurred in both groups as a result of the surgical intervention, but MMT has reached more severe osteoarthritis compared to the TO group, causing cartilage calcification and degeneration to occur as well. Hence, the TO rat model has value in allowing us to pick up early osteoarthritis for the study of the pathology and interventions. This is further supported by histological findings within the respective surgical techniques where synovial membrane inflammation score was more severe in the operated compared to the control leg in the TO group, in contrast to the MMT group where all histological grading subtypes reflected more severe osteoarthritis in the operated leg.
Earlier stages of osteoarthritis were found in the TO group when comparing CT grading results against those of the MMT group. However, within the respective groups, MMT was found to have more severe osteoarthritis CT changes when comparing the operated leg against the control leg. On the contrary, there was no statistically significant difference in that of the TO group. However, CT grading trended to the operated leg having more severe changes than the control leg. This further supports the histological results as well, where early primary osteoarthritis was likely picked up in the TO group before obvious radiological changes could be picked up by the conventional CT scan. This is supported by previous studies that have shown that CT scans have limited use in early osteoarthritis due to their relatively poor tissue contrast and ability to delineate soft tissue anatomy but are useful in later stages of osteoarthritis.31,32 In this study, it is important to recognize the limitations of CT scans and the use of the grading system the authors have adopted. Conventional CT scan was used as compared to a micro-CT scan, which will be more ideal in providing better resolution to the small knee joints in rats. 33 In addition, the authors have adopted the Kellgren-Lawrence classification for radiological grading of the severity of osteoarthritis which has not been validated in the rat model. This was done as there were no other validated models used to grade the severity of osteoarthritis in a rat model, to the authors’ knowledge. Despite these limitations, there were sufficient radiological details to show significant differences in severity between MMT and TO groups.
CTX-II is a marker of degradation of type II collagen, and serum concentrations have been found to be not only a good marker for diagnosing early osteoarthritis but also the severity of osteoarthritis as well,20,34 while serum IL-1β has been shown to be a marker of inflammation and has been associated with the risk of developing osteoarthritis.35,36 It has been shown to be found at high levels within the cartilage, subchondral bone, and surrounding synovial tissue of patients with osteoarthritis. 36 The trends in both serum markers of osteoarthritis were similar when comparing between the two groups. Findings in this study echoed that found in Britzman et al. 20 , where serum CTX-II levels were gradually down-trending for the first 6 weeks. However, in the referenced study, it subsequently up-trended till week 12, before falling sharply. As other studies have shown that synovial fluid IL-1β levels are closely associated with the degree of inflammation within the knee joint,36,37 the authors postulate that it may take some time for inflammation within the affected joint to become severe enough for systemic markers to start to increase, which is beyond the time limits of this study. Based on serum markers alone, it is difficult to rule out whether early osteoarthritis has happened, but future studies may look into a time frame that is between 6 to 12 weeks when this is likely to happen.
Limitations
There are several limitations to this study, in addition to the radiological limitations as discussed above. Firstly, the animal model in this study was insufficient for use clinically in humans, as rats are small animals with thinner cartilage, and the pathophysiology or response to therapy after induction of osteoarthritis may differ from humans. In addition, markers of osteoarthritis such as IL-1β levels would have ideally been studied via a knee aspiration to find out local inflammation within the knee joint. However, as there were limited effusions in the joint spaces of the animal samples in addition to the small joints, it was clinically difficult to attain enough synovial fluid for investigation without causing further joint inflammation which may affect the results.
Conclusion
In summary, TO is a novel method that mimics primary osteoarthritis and may be a better method of induction of osteoarthritis in the rat model compared to MMT. Furthermore, this study has further allowed an approximate time frame of between 6 and 12 weeks to be a good marker to pick up sufficiently early osteoarthritis in this rat model, instead of assessing interventions or studying pathology before 6 weeks which may be too early.
Footnotes
Acknowledgements and Funding
The authors would like to express our heartfelt appreciation to the SingHealth Duke-NUS Academic Medicine (AM) for the research grant, and for supporting and funding this study; Prof Duncan Angus McGrouther for his stellar mentorship, Prof Anthony Bull for inspiring this work, Ms. Zheng Lin for her care of the animals during the study period and for supporting our surgical procedures; Dr. Lee Bing Howe, Dr. Joseph Wan, Dr. Tammy Chan, and Dr. Oliver Huang for assisting during the surgical procedures; and all other staff at SingHealth Experimental Medicine Centre (SEMC) for their assistance in the study.
SingHealth Duke-NUS Academic Medicine (AM) Research Grant, grant number: AM/TP057/2021.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
Approval was obtained from Institutional Animal Care and Use Committee prior to commencing of this study.