
Abstract
Purpose
To clarify and standardize sagittal tibial tubercle-trochlear groove (sTTTG) numerical values in the literature.
Results
Sagittal tibial tubercle-trochlear groove distance has been recently popularized as a quantitative marker of patellofemoral contact forces and correlated to patellofemoral chondral lesion incidence, size, and osteoarthritis. There remains controversy over the precise definition of sTTTG.
Conclusion
The current erratum clarifies that a relatively anterior tibial tubercle compared to the trochlear groove is quantified as a positive sTTTG, whereas a relatively posterior tibial tubercle compared to the trochlear groove is quantified as a negative sTTTG.
Lansdown DA, Christian D, Madden B, et al., “The Sagittal Tibial Tubercle-Trochlear Groove Distance as a Measurement of Sagittal Imbalance in Patients with Symptomatic Patellofemoral Chondral Lesions.” Cartilage. 2021 Dec;13(1_suppl):449S-455S. doi: 10.1177/1947603519900802. 1 In this article published in the December 2021 issue of Cartilage, the authors stated, “The mean sTTTG [sagittal tibial tubercle-trochlear groove] was significantly more posterior in group 1 (5.9 ± 5.5 mm posterior to the trochlear groove) [cohort undergoing patellofemoral cartilage procedures] relative to group 2 (0.8 ± 5.3 mm posterior; P = 0.018) [control cohort undergoing partial meniscectomy with normal patellofemoral cartilage].” The wording of this result was ambiguous, as the senior author’s intent was to classify more posterior tibial tubercles relative to the trochlear groove as more negative sTTTG values; i.e., 5.9 mm posterior to the trochlear groove is an absolute value of an sTTTG = −5.9 mm. As the first description of sTTTG in the literature, this has led to significant confusion and heterogeneity in the literature. There has been appropriate usage by several recent studies, with Kaplan et al. and Bi et al. demonstrating more negative sTTTG values (greater absolute values, more relatively posterior tibial tubercles) of −2.5 ± 5.9 mm and −4.8 ± 4.9 mm, respectively, correlated with incidence of patellofemoral (PF) chondral lesions as well as size of PF chondral lesions.2,3 Namiri et al. 4 demonstrated that decreased sTTTG values (8.4 ± 12.7 mm) were associated with patellofemoral osteoarthritis (PFOA) versus 11.1 ± 12.8 mm in those without PFOA. In this case, since the overall cohort mean sTTTG was positive, a decreased absolute value represents a lower sTTTG and a more posteriorized tibial tubercle relative to the trochlea.
Two recent studies, however, reported greater, or more positive, sTTTG values were associated with trochlear dysplasia and represented a more posterior tibial tubercle, which is the opposite positive/negative value assignment of the sTTTG measurement.5,6 Any confusion by readers or surgeons should refer to the study by MacLean et al. 7 and the senior author of the original study. 1 Maclean et al. 7 demonstrated that increasing knee flexion angle on magnetic resonance imaging (MRI) artificially posteriorized the tibial tubercle, leading to decreased, or more negative, sTTTG values, and as a separate note, any measurements of sTTTG on MRI or computed tomography must be done with the knee in full extension.
The senior author would like to make a definitive statement that for sTTTG, when the tibial tubercle sits relatively more posterior to the trochlear groove, these should be quantified with negative sTTTG values (
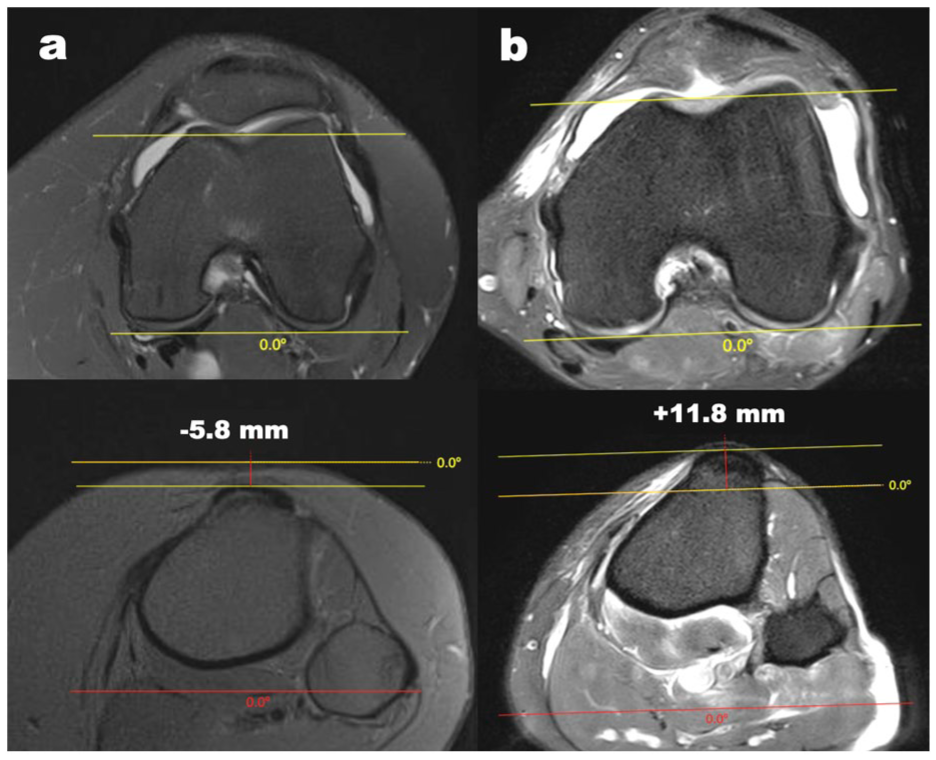
T2 axial magnetic resonance imaging (MRI) scan of a left knee in full extension with a tibial tubercle in (A) relative posterior position compared to the trochlear groove, representing a negative sagittal tibial tubercle-trochlear groove (sTTTG) value, with an example distance of −5.8 mm and (B) relative anterior position of the tibial tubercle compared to the trochlear groove, representing a positive sTTTG value of +11.8 mm. The measurement method is as follows: first, the nadir of the trochlear groove is identified on the axial MRI and a line is drawn parallel to the posterior condylar axis. Next, the most prominent aspect of the tibial tuberosity with patellar tendon attachment is marked on the axial MRI. The sTTTG is measured between these parallel lines perpendicular to the posterior condylar axis.
Footnotes
Ethical Considerations
No patients were included in this erratum.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
No data were used for this erratum.