
Abstract
Objective
Currently, there is a wide range of therapeutics that can be used to treat ankle osteoarthritis (OA), but none of them are able to fully restore the function of the ankle joint long-term. In this narrative review, we aim to summarize the current progress of using bone marrow aspirate concentrate (BMAC) for treating ankle OA.
Design
PubMed was searched for publications that were published from 1990 until September 1, 2025 (moment of search). Key search terms were bone marrow aspirate concentrate and ankle OA. This yielded 17 hits, of which 10 were included in this narrative review.
Results
BMAC may enhance cartilage repair in ankle injuries and OA, especially when it is used in combination with other surgical techniques and biological treatments. However, the body of supporting evidence remains largely composed of Level II to IV studies (case-control and retrospective series). In addition, the independent role of BMAC remains unclear due to the lack of studies evaluating BMAC as a stand-alone treatment, as well as the unclear role that it plays as an adjuvant therapy.
Conclusions
In conclusion, the existing literature investigating BMAC for ankle OA is encouraging but remains inconclusive. High-quality randomized controlled trials with standardized protocols, longer follow-up, and head-to-head comparison against other treatment options are needed to establish both efficacy and cost-effectiveness. Establishing minimal reporting standards for BMAC composition is also critical to improve consistency across studies.
Keywords
Introduction
Articular cartilage has low spontaneous healing potential due to its avascular nature and lack of undifferentiated cells. 1 These characteristics contribute to increased joint susceptibility to osteoarthritis (OA) following damage to cartilage.1,2 OA is a degenerative joint disease that often leads to disability and pain. Approximately 1% of adults suffer from OA of the ankle, which is less prevalent than OA occurring in the other weightbearing joints of the lower limbs.2 -4 Post-traumatic OA (PTOA), though, is the most common OA etiology in the ankle, occurring in about 60% to 80% of cases, whereas it is only observed in about 10% and 2% of knee and hip OA patients, respectively.3,5,6 As a result, individuals with ankle OA arising from injury tend to experience an approximately 10-year earlier onset than those with age-related, mechanically induced, or genetically driven OA in other joints, leading to an increased duration of pain and disability.3,6 One contributing factor to this earlier onset is the prevalence of ankle injuries. 4
Ankle sprains are the most common non–combat-related injury and often result in osteochondral lesions of the talus (OLTs), which are one of the most common diagnoses for patients experiencing ankle problems and occur in about 29% of patients.3,6,7 Fractures of the tibial shaft, distal tibia, malleoli, and talus often lead to PTOA. Among these, syndesmotic instability and talar displacement represent 2 of the most significant risk factors to PTOA development.5,8 Additional risk factors include chronic malalignments (e.g., valgus and varus deformity) and increasing body mass index (BMI).5,9,10
Large amounts of shear and compressive forces on the articular surface at the time of initial joint injury can damage the cartilage matrix and, in turn, affect the subchondral bone.
11
Experimental models support this notion, indicating that a single axial impact can lead to articular damage that is not visible on a macroscopic scale but results in significant microscopic disruption. In addition, traumatic impact promptly alters the mechanical properties of cartilage.12,13 In addition to forces on the articular cartilage, there is also an increase in proinflammatory mediators (including interleukin-1, 6, and 8) and anti-inflammatory mediators (including interleukin-1 receptor antagonist [IL-1Ra] protein and interleukin-10).
14
PTOA occurs when there is an imbalance between proinflammatory and anti-inflammatory mediators, leading to chronic inflammation after an initial trauma. This inflammation contributes to the increased production of tumor necrosis factor-alpha (TNF-α) and other chemokines, which, in turn, contribute to the breakdown of articular cartilage (
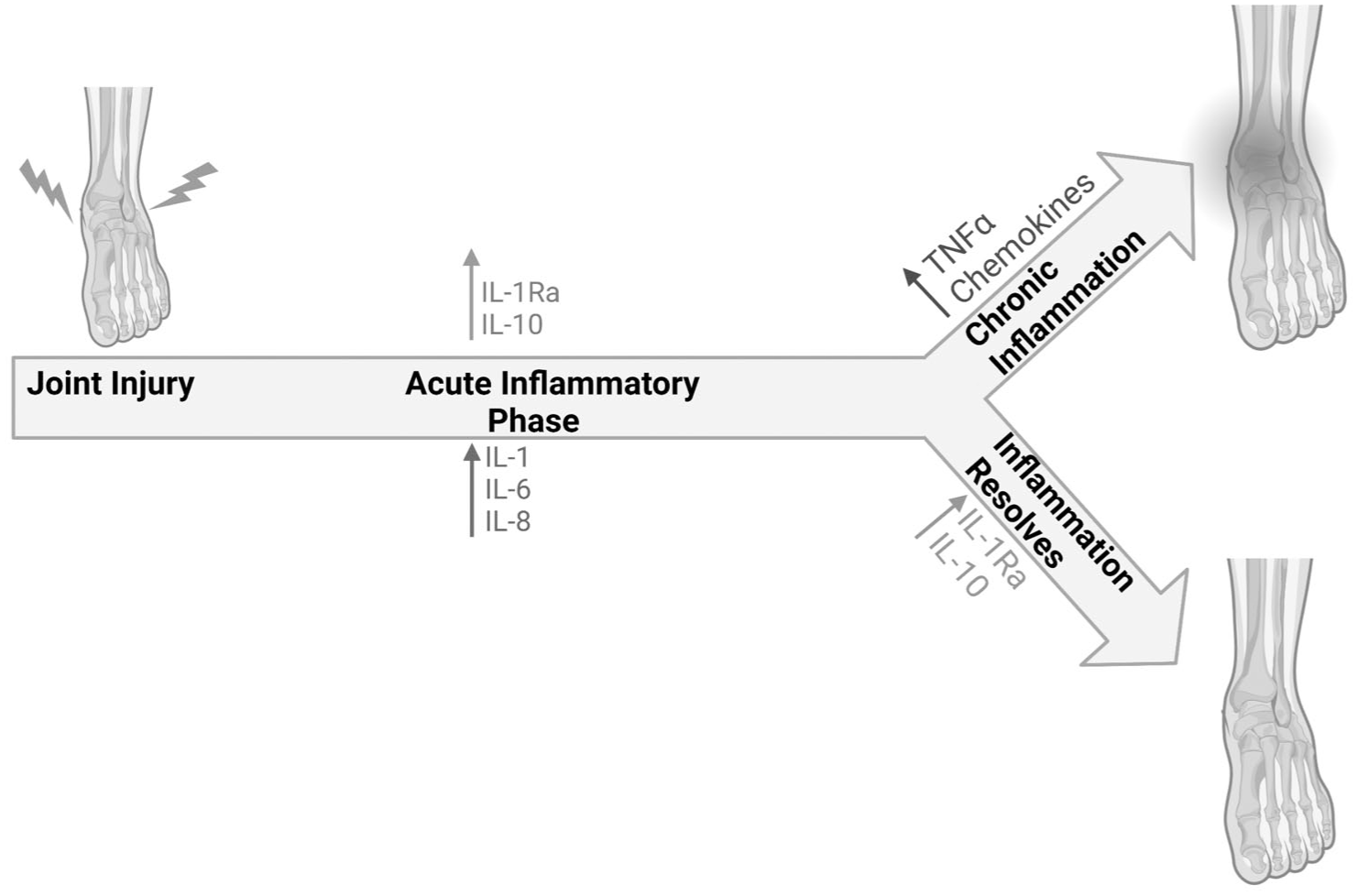
Progression of PTOA of the ankle. Initial joint injury causes acute inflammatory responses which generate both anti-inflammatory cytokines, including interleukin-1 receptor antagonist protein (IL-1Ra) and interleukin 10 (IL-10), and proinflammatory cytokines, including interleukins-1, 6, and 8. The production of anti-inflammatory cytokines in the early post-injury period can help to resolve inflammation and reduce the risk of PTOA. However, many factors can lead to chronic inflammation via the innate inflammatory pathway, which includes an upregulation of tumor necrosis factor-alpha and other chemokines, including repeated injury and the balance of pro- and anti-inflammatory cytokines. 14
Compared to OA at other sites, ankle OA is relatively understudied, which has led to a limited number of guidelines for diagnosis.15,16 In fact, there is no clinical definition for ankle OA; diagnosis is typically based on a combination of posttraumatic history, pain-related symptoms, and imaging and radiographic findings (e.g., Van Dijk or Kellgren and Lawrence classification). 15 Some diagnostic criteria have been proposed for the first metatarsophalangeal (MTP) joint, where clinical features like pain, dorsal osteophytes, crepitus, and restricted motion show good diagnostic accuracy. 17
The LaTrobe Foot Atlas has been created for radiographic assessment to evaluate osteophyte formation and joint space narrowing in the ankle and hindfoot. Osteophyte presence is rated on a scale of 0 to 3, with scores defined as follows: 0 for absent, 1 for small, 2 for moderate, and 3 for severe. Similarly, joint space narrowing is classified as none, definite, severe, or joint fusion, following the same scoring system (
LaTrobe Atlas.
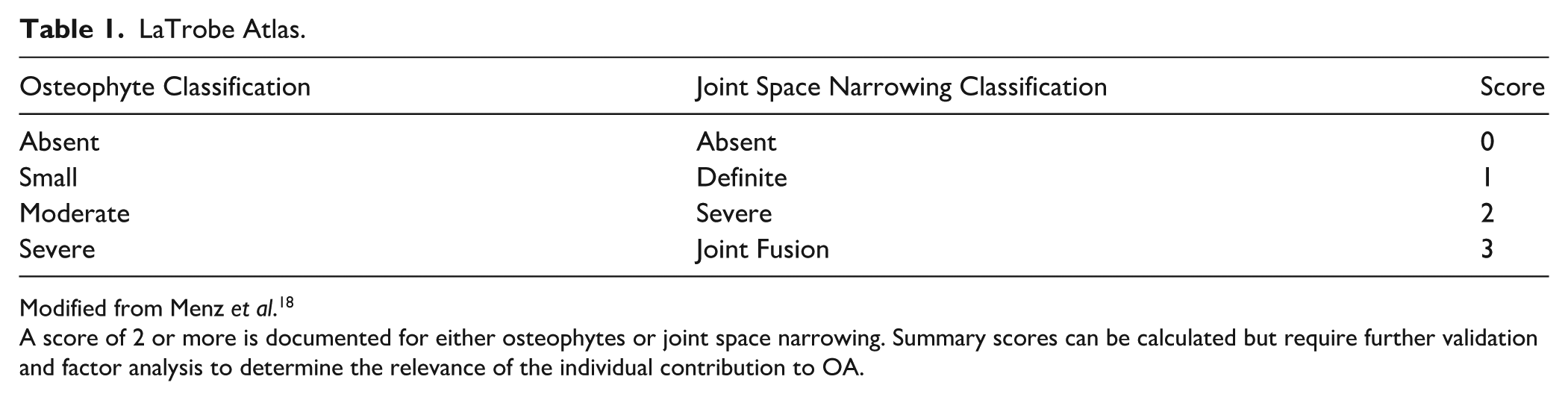
Modified from Menz et al. 18
A score of 2 or more is documented for either osteophytes or joint space narrowing. Summary scores can be calculated but require further validation and factor analysis to determine the relevance of the individual contribution to OA.
Current Treatments for Ankle Osteoarthritis
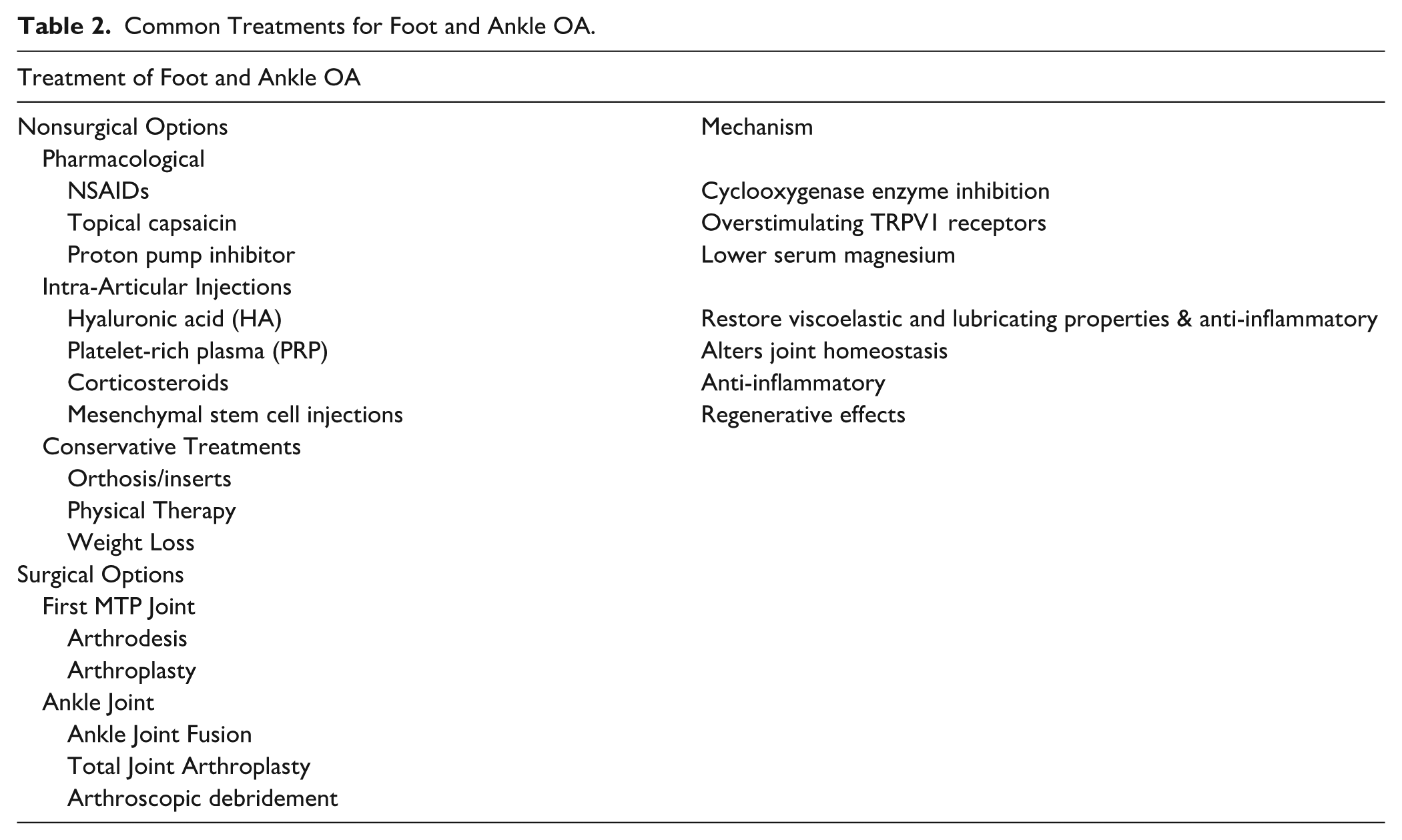
There are a wide range of therapeutic strategies for ankle OA, including lifestyle changes, surgeries, and biologic agents (
Common Treatments for Foot and Ankle OA.
What Is Bone Marrow Aspirate Concentrate: Collection and Components
BMAC is a promising new biologic therapy for a variety of musculoskeletal conditions due to the combined anti-inflammatory and regenerative effects stemming from the complex mixture of cellular and soluble components, described in detail later on. 29 Specifically, BMAC is composed of mesenchymal stem cells (MSCs), hematopoietic precursors, monocytes, endothelial cells, lymphocytes, and platelets, as well as a complex milieu of cytokines, chemokines, and growth factors. 29 Its clinical use is currently approved by the United States Food and Drug Administration (FDA) under the classification of “minimally manipulated” tissue. This differentiates BMAC from other cell therapies that involve ex vivo expansion or extensive processing and are subject to more rigorous regulation for clinical use.29 -32
BMAC is typically produced by aspirating bone marrow from the iliac crest or alternative sites with anticoagulant-assisted collection, followed by centrifugation (~15 minutes) to enrich the buffy coat layer containing nucleated cells and platelets. It should be noted that exact collection techniques have varying specific protocols.29,32
-34 The exact composition of BMAC is influenced by the aspiration technique, harvest volume, and centrifugation protocol (
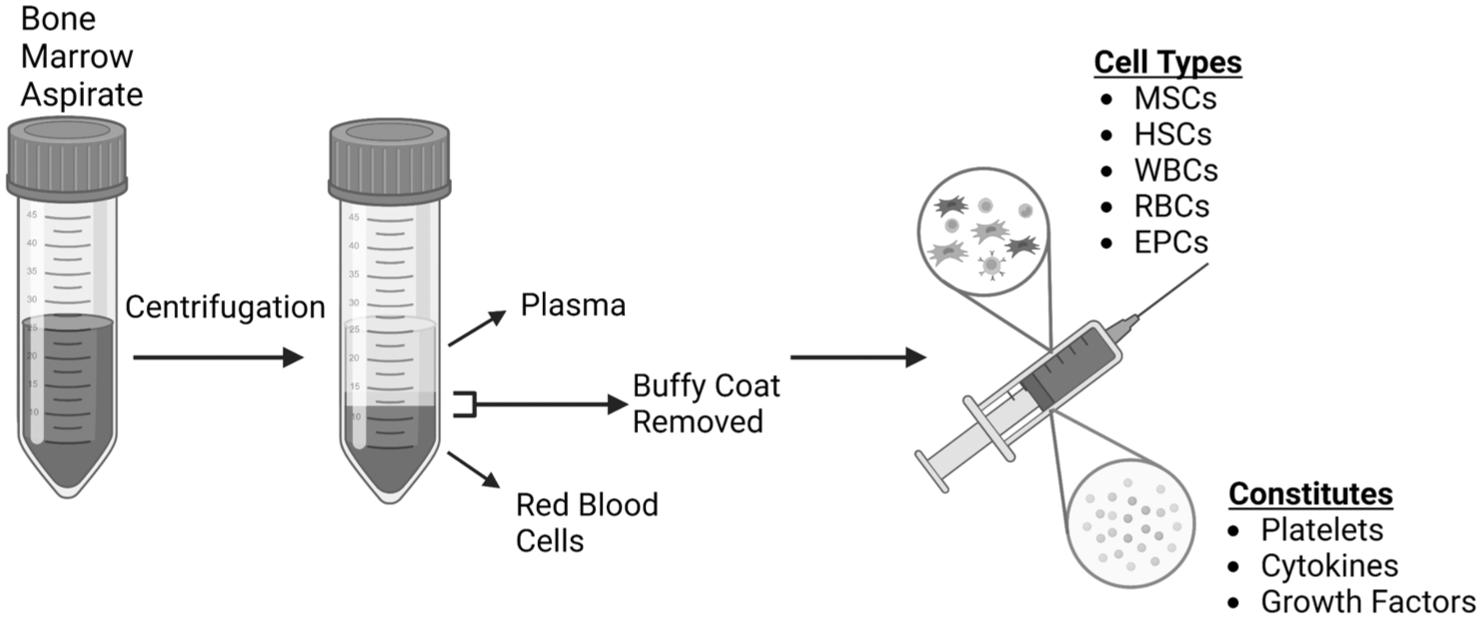
Processing of BMAC. Approximately 60 ml of bone marrow is aspirated using an anticoagulant-coated syringe. It is then filtered into a 50-ml tube and centrifuged with most protocols calling for about 15 minutes. The buffy coat layer is then removed, and the remainder is recentrifuged. BMAC consists mainly of the buffy coat, plasma, and the top layer of red blood cell layer without disturbing the cell pellet. MSCs: mesenchymal stem cells; HSCs: Hematopoietic stem cells; WBCs: white blood cells; RBCs: red blood cells; EPCs; endothelial progenitor cells.
The harvest procedure of BMAC allows for an on-site, 1-step method that can be used in clinics and during surgical procedures for the treatment of joint injuries or degenerative orthopedic conditions such as OA. Studies have shown that this is a safe procedure with no severe adverse effects related to injection. The most commonly reported adverse effects are temporary pain or joint swelling during the first few weeks after BMAC injection, with most complications spontaneously resolving weeks after BMAC harvest and injection. 29
One of the main advantages of BMAC is that it contains many types of cells that can facilitate tissue regeneration or suppress inflammation. For example, MSCs only make up 0.001% to 0.01% of the cells within BMAC, but they are important due to their immunomodulatory, anti-inflammatory, and anti-apoptotic effects.30,38 -40 The local delivery of MSCs helps to promote an anabolic environment and release paracrine signals to recruit endogenous MSCs.38 -40 While the ability of MSCs to differentiate into chondrocytes, osteoblasts, and adipocytes has been demonstrated in vitro, the current evidence suggests that their primary contribution in vivo is via trophic and immunomodulatory pathways rather than direct engraftment and tissue replacement.34,41 These mechanistic pathways have been investigated extensively in preclinical models, yet translation to clinical outcomes remains less consistent.42,43 Other bioactive molecules and cell types found within BMAC include lymphocytes, neutrophils, monocytes, and platelets in various stages of differentiation, all of which contribute to more effective chondrogenesis than bone marrow itself. 40 Hematopoietic stem cells (HSCs) are found within the BMAC and are important for the regulation of the immune system and are able to drive tissue regeneration by upregulating cytokine release and stimulating endogenous stem cells.23,34,39
Many growth factors, cytokines, and chemokines, including the transforming growth factor-beta (TGF-β) family, platelet-derived growth factor (PDGF), bone morphogenic proteins 2 and 7 (BMP2 and BMP7), vascular endothelial growth factor (VEGF), granulocyte-macrophage colony-stimulating factor, and IL-1Ra can be found within BMAC. The complex milieu of growth factors and cytokines contributes to the regeneration and immunomodulation.29,30,38,40 Specifically, TGF-β is a critical factor for chondrogenesis by inhibiting inflammation, and it is important in the composition of collagen type II fibers that make up the extracellular matrix (ECM) of cartilage.40,41 PDGF has a specific role in cartilage regeneration and homeostasis maintenance by promoting wound healing via MSC proliferation, collagen synthesis, and enhancement of BMP-2 and BMP-7, which contribute to ECM and chondrocyte proliferation. The concentration of PDGF, TGF-β1, and TGF-β2 is found to be greater within BMAC compared to whole blood. 38 Similarly, there is a higher concentration of IL-1Ra in BMAC when compared to both whole blood and PRP. 38 IL-1Ra acts to inhibit interleukin-1 beta (IL-1β), which plays a major role in the pathogenesis of OA by inducing chondrocyte inflammation and apoptosis pathways. However, the relative proportions of these factors vary substantially between preparations, and standardized reporting of BMAC composition is lacking.
Importantly, BMAC has been found to contain various proinflammatory cytokines and components that may have complicating effects. 44 However, the extent to which these factors impact clinical outcomes is not well understood. One study found that BMAC contains various proinflammatory cytokines, including IL-8 and IL-1β, and various matrix metalloproteinases (MMPs). 44 While this study quantified these components, it did not look at the active role they have clinically. Another study comparing BMAC and PRP found that BMAC contains a ratio of IL-1Ra:IL-1β that is sufficient to counteract the inflammatory effects of IL-1β. 45 Overall, there is a paucity of research that goes into the mechanism of BMAC treatment and how all of the bioactive molecules work to promote regeneration and healing.
Bone Marrow Aspirate Concentrate As A Treatment Modality
Methods
A narrative review methodology was employed to evaluate the current literature on the use of BMAC in the treatment of ankle osteoarthritis and cartilage injuries. A comprehensive search of the PubMed database was conducted, with results collected through September 2025. Search terms included combinations of “bone marrow aspirate concentrate,” “BMAC,” “ankle osteoarthritis,” and “ankle OA.” Articles were considered for inclusion if they reported clinical trials or clinical case series evaluating BMAC as a therapeutic intervention for ankle OA or cartilage injury in the ankle. Both studies assessing BMAC as a stand-alone treatment and those using BMAC as an adjunct to other surgical or biological interventions were included. Exclusion criteria were studies limited to basic science models, reviews, and those not directly evaluating clinical outcomes in ankle pathology.
The initial search identified relevant publications, which were then screened by title and abstract for eligibility. Full texts were reviewed to confirm inclusion criteria. Data extracted included study design, patient population, harvest site, volume of BMAC, adjunctive interventions, follow-up duration, outcome measures, and reported complications.
Because this is a narrative review rather than a systematic review, formal quality assessment and meta-analysis were not performed. Instead, findings were synthesized descriptively and organized thematically, with particular focus on the clinical application, report outcomes, and limitations of BMAC therapy for ankle OA.
BMAC has demonstrated promising therapeutic potential for OA across various joints. In knee OA, a systematic review by Keeling et al. 46 evaluated the efficacy of isolated BMAC injection. The review included 8 studies with a total of 299 knees from 36 patients. Of these 36 patients across the 8 studies, 34 declared significant improvement from the baseline to the latest follow-up. The findings suggest that BMAC can be used as a therapeutic treatment for OA, although 3 of the comparative studies in this article show that it does not show superiority over already existing biologic therapies. 46 It should be noted that these studies did not rule out the possibility of a placebo effect and lavage joint effect.
The existing literature investigating BMAC for ankle OA is encouraging but remains inconclusive. For example, 1 small retrospective study observed patients with symptomatic subtalar OA who underwent subtalar distraction arthroplasty (DA) with BMAC injection in an attempt to avoid joint fusion. 47 The results were promising, as the ankle osteoarthritis scale score improved, and the radiographic findings showed a decrease in subchondral sclerosis. However, confounding surgical variables and the lack of a control group made it difficult to understand the role BMAC played in the healing process. In addition, this study represents a case series, which limits the strength of conclusions.
As described above, ankle injuries that involve cartilage can progress to PTOA, causing a need for treatment to promote the growth and repair of healthy hyaline cartilage. Ankle sprains are a common injury that often results in OLTs, which, due to the low regenerative potential of cartilage, can progress to PTOA if left untreated. OLTs show good success with current treatment options, including grafts and bone marrow stimulation, with success rates found between 17% and 100% with a mean success rate of 90%.48,49 Utilizing BMAC in the treatment of OLTs is hypothesized to promote healing and regeneration of the cartilage. Seven studies were found to observe BMAC as an adjunct treatment for OLTs, but no studies investigated BMAC as a stand-alone treatment (
Clinical Trials for BMAC in OA and OCLs.
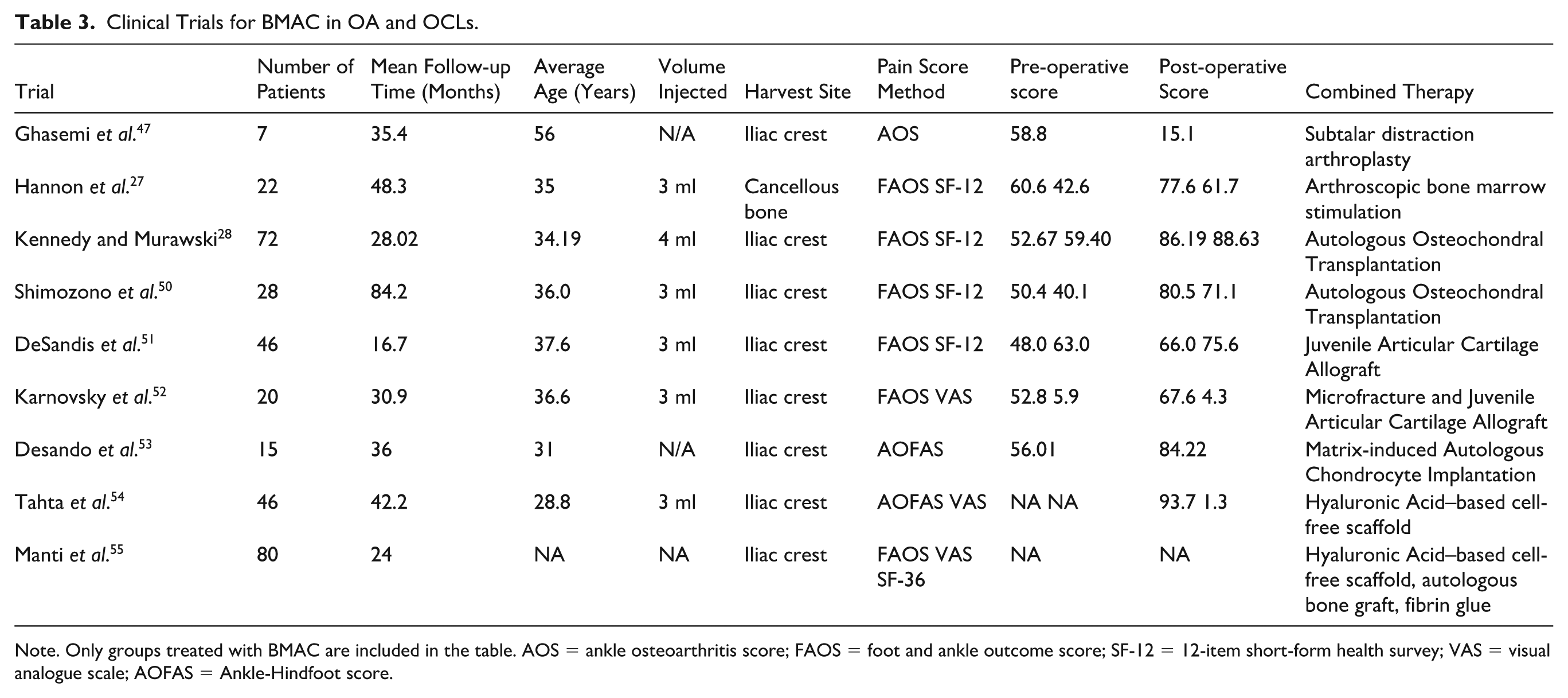
Note. Only groups treated with BMAC are included in the table. AOS = ankle osteoarthritis score; FAOS = foot and ankle outcome score; SF-12 = 12-item short-form health survey; VAS = visual analogue scale; AOFAS = Ankle-Hindfoot score.
Across multiple studies, the use of BMAC in conjunction with bone marrow stimulation (BMS) has been associated with improved cartilage repair quality, as evidenced by higher Magnetic Resonance Observation of Cartilage Repair Tissue (MOCART) scores and greater rates of complete defect fill as outcome measures. 27 Functional outcome scores, such as those measured with the Foot and Ankle Outcome Score (FAOS) and 12-item short-form survey (SF-12), were often comparable to those of BMS alone. These results suggest that BMS in conjunction with BMAC can lead to better integration and less evidence of fissuring and fibrillation on the MRI compared to BMS alone, yet treatment does not yield better functional results for patients. 27
Similarly, when used alongside autologous osteochondral transplantation (AOT), BMAC appears to reduce postoperative cyst formation and may enhance cartilage repair quality. 28 A comparative study done by Shimozono et al. 50 reviewed patients treated with AOT and BMAC compared to patients who underwent AOT alone. The study included 54 patients who underwent AOT between 2004 and 2008; FAOS and SF-12 were used to assess clinical outcomes. MOCART scoring system was used for MRI analysis, and cyst formation was also evaluated on postoperative MRI. The results showed a significant improvement in mean FAOS and SF-12 scores, but no significant difference between the 2 groups, meaning that BMAC in conjunction with AOT does not yield better clinical outcomes. Similarly, no significant difference was found between the 2 groups in the postoperative MOCART scores. However, cyst formation evaluated on the postoperative MRI showed a significantly higher rate of cyst occurrence in the AOT-alone group. 50 While this study suggests lower cyst formation with BMAC, the functional outcome improvements did not reach statistical significance compared to AOT alone, raising questions about clinical relevance.
Juvenile allogenic chondrocyte implantation (JACI) combined with BMAC was observed in 2 studies.51,52 In a retrospective review of 46 patients treated with JACI and BMAC, most of the patients had improved SF-12 and FAOS scores postoperatively, although the quality of tissue repair found on the MRIs was not ideal, and the presence of fibrocartilage composition was observed, which directly contradicts the tissue quality repair of the AOT and BMS in conjunction with BMAC. 51 Another study comparing patients who received DeNovo NT for JACI-BMAC treatment to patients undergoing repair with microfracture (MF) found similar improvements in FAOS and MOCART scores pre- to postoperatively, with no significant differences between the groups. Hypertrophy was observed in 70% of the JACI-BMAC group and 30% of the MF group. 52 While both studies suggest a functional improvement, the specific contribution of BMAC remains unclear without a BMAC-only control and a no-BMAC control. These JACI-BMAC studies were retrospective with no randomization, introducing potential for selection bias. Moreover, the high rates of fibrocartilage repair and hypertrophy highlight concerns about tissue quality despite short-term symptomatic improvement.
In a study comparing the effects of autologous matrix-induced BMAC (mBMAC) and matrix-induced autologous chondrocyte implantation (mACI), patients treated with mACI had greater improvement in the American Orthopaedic Foot and Ankle Score (AOFAS) and more favorable tissue remodeling. In the mBMAC group, higher expression of fibrous and hypertrophic markers was observed when compared to the mACI group. 53 This finding indicates that while mBMAC may support defect filling, the resulting repair tissue may be mechanically inferior and less durable compared to the cartilage generated with mACI and may explain the superior functional outcomes observed in the mACI group.
Another study comparing hyaluronic acid–based cell-free scaffold (HACS) with BMAC to nanofracture (NF) in patients with OLTs found that the HACS-BMAC group had significantly higher AOFAS score, visual analog score, and MOCART scores. These results provided evidence of good clinical results, pain relief, and an organized hyaline-like chondral tissue from the HACS-BMAC group. 54
A recent retrospective study of 81 ankles with OLTs evaluated a single-stage arthroscopic technique combining autologous iliac crest bone graft, cell-free HA matrix scaffold, and BMAC fixed with fibrin glue. 55 Patients demonstrated significant improvements in pain, function, and quality of life scores at >1 year follow-up, with MRI confirming defect filling, higher MOCART scores, and reduced bone marrow edema. Early full weightbearing correlated with better outcomes, while younger age and lower BMI predicted better recovery. The authors concluded that integrating BMAC with scaffold and bone graft provides both biological support for cartilage regeneration and mechanical stability, offering a promising strategy to improve ankle joint preservation and potentially delay OA progression. While the findings are promising, this study lacks a control or comparison group, making it very difficult to determine the independent contribution of BMAC versus the autologous bone graft, HA scaffolds, or the MF itself, and they do not include the volume of BMAC incorporated. The retrospective design and single-center setting also introduce potential bias, and outcomes may not be generalizable.
Overall, current evidence suggests that BMAC may enhance cartilage repair in ankle injuries, especially when it is used in combination with other surgical techniques and biological treatments. However, the independent role of BMAC remains unclear due to the lack of studies evaluating BMAC as a stand-alone treatment, as well as the unclear role that it plays as an adjuvant therapy. Larger, prospective controlled trials are needed to better define its clinical utility in ankle pathology. In addition, the body of supporting evidence remains largely composed of Level II to IV studies (case-control and retrospective series). The absence of adequately powered randomized controlled trials means efficacy claims should be considered preliminary.
Current Limitations and Future Perspectives
OA of the ankle is widely understudied compared to OA of other joints, such as the hip and knee. Cartilage of the knee and ankle varies in both biomechanical and metabolic properties, creating a need for studies specifically focused on the ankle joint. This includes testing potential therapeutics in preclinical animal models that are specific to the ankle joint. However, there is currently a lack of models that accurately mimic PTOA within the ankle, making it difficult to carry out these studies. 6
Despite the need for a method that optimizes the regenerative effects of BMAC, current research suggests that harvesting BMAC is safe and has minimal complications and a low rate of infection. 56 There is a paucity of research observing BMAC as a method of treatment for both OA and injuries that can lead to the progression of PTOA in the ankle. Current studies suggest BMAC to be a safe and reliable source of MSCs and growth factors that can aid in stem cell migration and modulation of the local environment. These factors help to exert an anti-inflammatory and regenerative effect within damaged joint tissues, but more thorough investigation into the percentage of the beneficial components within BMAC, such as MSCs and cytokines, is needed to limit dose variation. 33 In addition, there is no standardized method of harvesting BMAC, and more research is necessary to define a standard protocol for harvesting, processing, and characterizing concentrate composition that results in maximal regeneration and immunomodulation outcomes. 46 Establishing minimal reporting standards for BMAC composition is thus critical to improve consistency across studies. For example, a small sample of BMAC will be taken, and the level range of regenerative factors can be defined with enzyme-linked immunosorbent assay (ELISA). The ratio of the total number of MSCs in BMAC can be calculated using the known surface biomarkers.
Current clinical findings suggest that BMAC may play a role in supporting good clinical outcomes, but most available studies that can be found often include BMAC in conjunction with other treatment methods and have no control group, making it difficult to understand the independent influence of BMAC on the healing process of injuries or OA.27,47,50 -54 More research is necessary to find the optimal treatment method using BMAC, including studies investigating BMAC as a stand-alone treatment, studies that include a control group when employing BMAC as an adjunct treatment, and comparative trials against other biologics such as platelet-rich plasma (PRP). Studies have shown that BMAC is most effective in treating early to moderate stages of OA in the knee and hip, specifically K-L grades I, II, and III, yet studies have also shown improvement in pain and function for patients with severe OA.40,57 Therefore, BMAC may be reserved for mild ankle OA, which, however, requires further clinical investigation. In addition, the study with the longest follow-up time was Shimozono et al. 50 with a mean of 84.2 months. The longevity of the potential benefits of BMAC needs to be further investigated.
For future studies that may investigate the benefits of BMAC injection for ankle OA, high-quality randomized controlled trials with standardized protocols, longer follow-up, and head-to-head comparison against other treatment options (e.g., PRP or HA) are needed to establish both efficacy and cost-effectiveness. Incorporating validated reporting guidelines will strengthen the evidence base. Furthermore, it would be worth exploring if more than 1 injection could provide a more beneficial outcome. If so, research would be needed to figure out proper intervals of injections. Finally, investigations to identify the active key components and mechanisms of BMAC that are responsible for clinical improvements, alongside the use of standardized functional outcome measures, will be critical to advance this therapy.
Footnotes
Acknowledgements
The authors thank the support from the Department of Orthopaedic Surgery and the Orland Bethel Family Musculoskeletal Research Center (BMRC) at the University of Pittsburgh School of Medicine, University of Pittsburgh Medical Center,and the Albert B. Ferguson, M.D. Orthopaedic Fund of the Pittsburgh Foundation.
Ethical Considerations
Ethical approval was not required for this study, as it is a narrative review of previously published literature and did not involve human participants, identifiable human data, or human tissue.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received financial support from the Department of Orthopaedic Surgery and the Orland Bethel Family Musculoskeletal Research Center (BMRC) at the University of Pittsburgh School of Medicine, University of Pittsburgh Medical Center, and Albert B. Ferguson, M.D. Orthopaedic Fund of the Pittsburgh Foundation for the research of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.