
Abstract
The COVID-19 pandemic continues to pose an unprecedented challenge for the world as people strive to cope with this significant threat to their well-being. This intensive longitudinal study of the first 94 days of the COVID-19 outbreak in South Korea (Phase 1: initial outbreak, Phase 2: intense social distancing) examined individuals’ changes in well-being, in relation to their use of coping strategies and fear of infection. A sample of 10,464 South Koreans participated in surveys during Phase 1 and Phase 2, resulting in 35,846 observations. Multilevel growth models revealed a decrease in well-being while different coping strategies moderated the individual rate of change in well-being. Although preventive measures were associated with a greater decrease in well-being, cognitive appraisal and behavioral strategies predicted stable well-being during the pandemic. Coping strategies further mediated the association between fear of infection and deterioration of well-being.
The outbreak in 2019 of the infectious novel coronavirus disease (COVID-19) has impacted not only the physical but also psychological health of nearly every member of society. Prompt efforts by the research community have already shown that COVID-19 has resulted in significant deterioration of mental well-being, as evidenced by increased levels of anxiety, fear, and depression among the general population (Barari et al., 2020; Cao et al., 2020; Choi et al., in press; Vindegaard & Benros, 2020; Wang et al., 2020). The current conditions, worldwide, provide an unprecedented opportunity for researchers to investigate how people cope with shared threats to well-being. The present study investigated whether the various methods that people use to cope with the pandemic had consequences for well-being during the early days of the COVID-19 outbreak in South Korea. We focused on different types of coping strategies that we expected to be associated with threats caused by the epidemic: preventive measures, cognitive appraisal, social connection, and self-distraction. These strategies are well-established as effective in the distress regulation literature (Carver et al., 1989; Folkman & Lazarus, 1980).
Preventive Measures
COVID-19, due to its particularly contagious nature and mortality rate, has induced feelings of fear and insecurity among the population (Ahorsu et al., 2020). First and foremost, people have responded by taking measures to protect themselves and others from the virus (Zickfeld et al., 2020). The preventive behaviors described during previous epidemic outbreaks (e.g., H1N1 influenza, Middle East respiratory syndrome) have included hygiene practices, such as handwashing (e.g., Rubin et al., 2009), wearing facial masks (e.g., Tang & Wong, 2004), and social distancing (e.g., Morrison & Yardley, 2009; see Bish & Michie, 2010; Chew et al., 2020, for reviews). These measures can be viewed as “problem-focused coping” as opposed to “emotion-focused coping,” based on previous conceptualizations of coping, as they aim to directly circumvent the sources of stress (Lazarus & Folkman, 1984; Scheier et al., 1986). In addition, considering that these preventive behaviors are socially sanctioned, individuals may engage in them as a way to conform to the social norms and, thus, are in part extrinsically motivated.
Although recent research has found preventive behaviors to be effective for controlling outbreaks (Brooks et al., 2020; Ferguson et al., 2020), the effects of employing such coping strategies on well-being have not been well-studied. Therefore, we do not yet know whether preventive behaviors that are effective for disease containment are also beneficial to well-being by alleviating the fear and anxiety of infection or whether these behaviors are instead associated with costs that are detrimental to well-being due to the reduced autonomy and discomfort experienced when engaging in these behaviors.
Cognitive Appraisal
When there is a restricted range of strategies to control the stressors (Morling & Evered, 2006), as is the case for COVID-19, cognitive appraisal may be particularly beneficial. Prior literature describing existing theories associated with stress (Lazarus & Folkman, 1984), self-regulation (Carver & Scheier, 2012; Scheier & Carver, 1988), and emotional regulation (Gross, 2015) have all emphasized the critical role played by cognitive appraisal in the management of psychological distress. Changing how one thinks about the COVID-19 situation can have a powerful influence on the threat response. For instance, assessing the current epidemic as nonthreatening and psychologically distancing oneself from the stressor may reduce fear or anxiety (Folkman et al., 1986). In addition, focusing on positive aspects of the event such as finding benefits or positive meaning may help to deal with the constraints of the situation caused by the COVID-19 outbreak (Shiota & Levenson, 2012; Tennen & Affleck, 2002).
Social Connection and Self-Distraction
One critical challenge in the COVID-19 pandemic is the need for people to adapt to the changes in the environment and lifestyle caused by following social distancing, which have been associated with increased levels of negative emotions such as loneliness, boredom, and frustration (Barari et al., 2020; Brooks et al., 2020). Researchers have proposed strategies for coping with these abrupt interruptions in well-being associated with social distancing (Brooks et al., 2020; Fiorillo & Gorwood, 2020; Holmes et al., 2020). Among the recommended coping responses is the activation of one’s social support system, which is especially relevant for social life disruptions and has been extensively studied as an effective method for reducing psychological distress (Kim et al., 2008; Thoits, 1995). Connecting with others, even remotely, should be particularly beneficial during this period of social distancing. In addition, self-distraction, that is, engaging in activities to distract oneself from stressors, has been a commonly reported response to social isolation during past epidemic outbreaks (Chan et al., 2007; Rabelo et al., 2016). Although self-distraction has also been associated with pessimism and, therefore, considered to be dysfunctional for general well-being (Carver et al., 1989, 1993), self-distraction may not only reduce psychological distress, by encouraging disengagement from the negative emotions associated with stressors (Klinger, 1975), but may also help combat boredom and helplessness associated with the lack of social connection during the pandemic (Polizzi et al., 2020).
Present Research
Although recent research has examined which coping strategies individuals use in response to the COVID-19 outbreak (Huang et al., 2020; Man et al., 2020) or what factors predict the use of coping strategies (Zickfeld et al., 2020), few studies have empirically examined their presumed relationships with well-being. Moreover, those studies exploring the role of coping strategies have primarily been performed with a cross-sectional design (Li et al., 2020a, 2020b); therefore, in the present research, we used an intensive, longitudinal design to examine whether and how the changes in well-being are predicted by different coping strategies over approximately 13 weeks (94 days) during the COVID-19 outbreak in South Korea. We predicted that, based on previous findings on stress and coping (Skinner et al., 2003), strategies that are aimed at adjusting to the stressor (i.e., threats due to the COVID-19) would be adaptive in buffering against the harmful effects of COVID-19-induced stress on well-being. As an exception, we do not have an a priori hypothesis for preventive measures, which may have both intrinsic and extrinsic underlying motivations.
An additional factor that is potentially important for understanding the coping process is the extent to which a person fears contracting COVID-19 (Pakpour & Griffiths, 2020). Despite its negative implications for mental health (Krueger et al., 2018), fear is also an emotional experience that motivates self-protective actions (Harper et al., 2020). Therefore, how fear of infection affects coping strategies and whether strategies meant to cope with feelings of fear can influence well-being should be tested empirically. Because the COVID-19 outbreak is ongoing and continues to require the maintenance of social distancing, identifying healthy stress management techniques during the pandemic would be invaluable for the public in coping with this unusual situation. Thus, as an exploratory analysis, we further examined whether the extent of an individual’s fear of COVID-19 predicts either the use of coping strategies or changes in well-being.
Method
Procedures and Participants
Figure 1 depicts the procedures followed during the present study. The data set used was collected from an online survey, which was conducted by Kakao Corporation, one of the largest internet companies in South Korea. The company provided the survey through its main smartphone application, KakaoTalk, which is widely used by Koreans (approximately 86% of Korea population), and its website (http://together.kakao.com/hello). The users were able to access and respond to the survey, voluntarily, at any time, and were able to submit multiple responses (see Suk et al., 2020, for a detailed description of the Kakao data set). The participants included in the present analysis were volunteers who completed the survey between January 20, 2020, when the first COVID-19 case was confirmed in South Korea, and April 22, 2020 (94 days later). At the midpoint of this period (March 22, 2020), the South Korean government announced “intensive social distancing,” which significantly restricted face-to-face contact. The study period, therefore, includes two phases: Phase 1, from January 20, 2020, to March 21, 2020 (after COVID-19 confirmation but before intensive social distancing), and Phase 2, from March 22, 2020, to April 22, 2020 (after intensive social distancing was enacted). The final sample consisted of 10,464 participants, who responded to the well-being survey at least once during both Phase 1 and Phase 2 and completed the coping and fear of infection questionnaires that were collected during Phase 2. A total of 35,846 well-being observations with an average of 3.43 observations per participant were included. 1 The participants consisted predominantly of female and young adults: 88.6% female and 26.1% in their 20s (M age = 33.83 years, SD age = 12.20 years; Table 1). We tracked individuals who reported their well-being both prior to (Phase 1: January 20 to March 21) and postintensive social distancing (Phase 2: March 22 to April 22) and examined how their well-being changed over time (i.e., well-being growth rate).

Study procedure.
Demographic Characteristics of the Respondents.
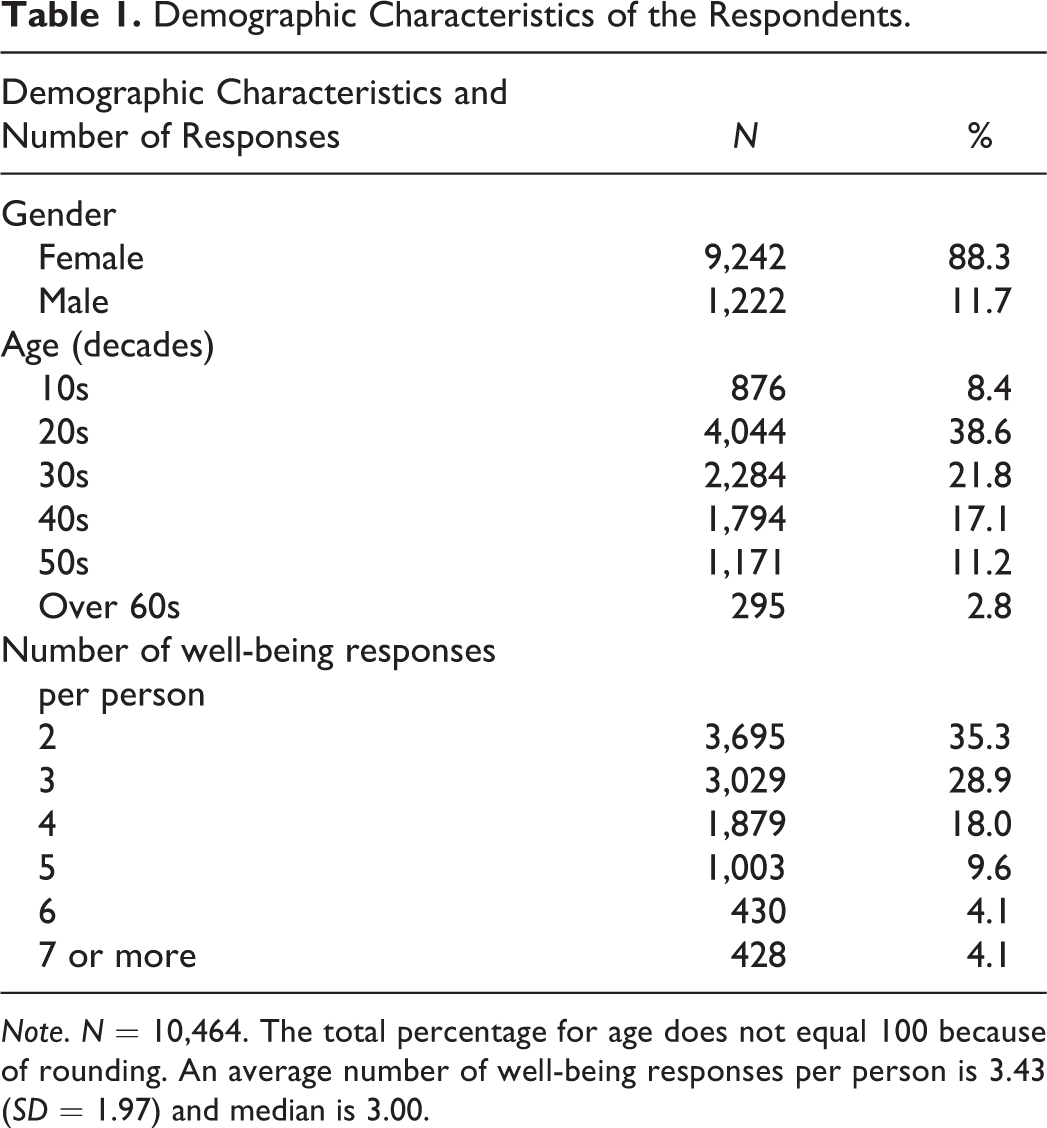
Note. N = 10,464. The total percentage for age does not equal 100 because of rounding. An average number of well-being responses per person is 3.43 (SD = 1.97) and median is 3.00.
Measures
Well-being
A 10-item questionnaire was used to measure various aspects of well-being, including life satisfaction (LS), meaning in life (MIL), stress, positive affect (PA), and negative affect (NA). LS, MIL, and stress were measured with a single question, asking how the participants were feeling at the time of the response (i.e., “How satisfied are you with your life right now?”). PA and NA were measured by three items (happy, pleasant, and relaxed) and four items (bored, annoyed, depressed, and anxious), respectively. Each item was rated on an 11-point scale ranging from 0 to 10 (e.g., 0 = not satisfied, 10 = very satisfied). The overall well-being index was calculated by averaging all 10 items (with the NA items reverse-scored; between-person α = .978 and within-person α = .862; see Geldhof et al., 2013, for multilevel reliability estimates). The aggregated well-being scores were used to estimate an individual slope of well-being during the outbreak.
Day
Ninety-four days, from January 20, 2020, to April 22, 2020, were used to create the day variable, which indicated the day on which the well-being indices were reported. The day variable was coded by setting the first day (Jan 20, 2020) to 0 and the last day (Apr 22, 2020) to 93 so that the intercept can be interpreted as the initial level of well-being. Next, the day variable was divided by the total number of days to have a range from 0 to 1 to balance its scale range with other variables.
Coping strategies
Coping strategies were modified from the Brief COPE Scale (Carver, 1997). Preventive measures were assessed by three items, namely, hand hygiene, mask-wearing, and social distancing. Cognitive appraisal was measured by three items, psychological distancing, positive reappraisal, and acceptance. Behavioral strategies included social connection, self-distraction, and religion. Religion was explored because people often turn to religion in times of crisis (Carver, 1997; Lazarus & Folkman, 1984; Pargament, 1997), and engagement with religion has been shown to reduce the emotional distress caused by highly unpredictable events such as the COVID-19 crisis (Bentzen, 2020). Participants indicated the extent to which they used each coping strategy on a 5-point scale (1 = never, 5 = very much; see the Supplemental Material for the exact wording of the items and descriptive statistics).
Fear of infection
Participants indicated the degree to which they feared being infected with the coronavirus (1 = never, 5 = very much).
Analytic Strategy
We performed confirmatory factor analysis (CFA) of the measurement model for coping strategies to determine the fit of the conceptualized latent coping model. Subsequently, multilevel growth modeling (Luke, 2004) was conducted to accommodate the nested nature of the data. Multiple responses of well-being (Level 1) are nested within persons (Level 2). Because participants were free to respond to the well-being questionnaire as many times as they wanted, the number of responses per person ranged from two to 42 and spanned the entire study period, which is unique from typical longitudinal studies with fixed time points and intervals. This asynchronous time structure, containing different intervals for well-being reports among the participants, supported the adoption of a multilevel modeling (MLM) approach (Jackson, 2010; Wu et al., 2009). The use of multilevel models also circumvented the effects of response frequency imbalances on estimation accuracy and statistical power (Cools et al., 2009). The measurement and multilevel models were estimated using Mplus Version 7.4 (L. K. Muthén & Muthén, 2012). Because approximately 64% of participants reported three or fewer responses, and a nonlinear model can make relationships among variables difficult to interpret (Kwon & Lee, 2020), we fit a linear (vs. polynomial) growth curve to the data.
The null model was examined first to estimate the sources of variance in well-being and to obtain intraclass correlations (ICCs). ICC was .691, indicating that differences across participants accounted for 69.1% of the variability in well-being. The significant between-person (2.958) and within-person variance (1.322) in well-being supported the use of a nested structure, which requires MLM. Three models, specified following the multilevel model building process, were tested sequentially, controlling for gender and age (Aguinis et al., 2013; Geiser, 2013; Luke, 2004): Model 1 (random intercept model), Model 2 (random intercept and slope model), and Model 3 (intercept and slope as outcomes model). Model 1 included the day variable at Level 1 to predict changes in individual well-being over time (i.e., well-being growth rate) during Phases 1 and 2, while allowing only the well-being intercepts to vary across individuals. Model 2 allowed variation in both the intercepts and the slope coefficients across individuals. Model 3 specified both random intercepts and random slopes; it included the day predictor at Level 1 and latent coping strategy variables at Level 2, resulting in a cross-level interaction effect between coping strategies and day on well-being. This procedure determines whether initial well-being and the well-being growth rate differ depending on coping strategies (see Figure 2 for a conceptual model: Kline, 2011; L. K. Muthén & Muthén, 2012). The Level 2 variables were centered at its mean for meaningful interpretation (Enders & Tofighi, 2007).
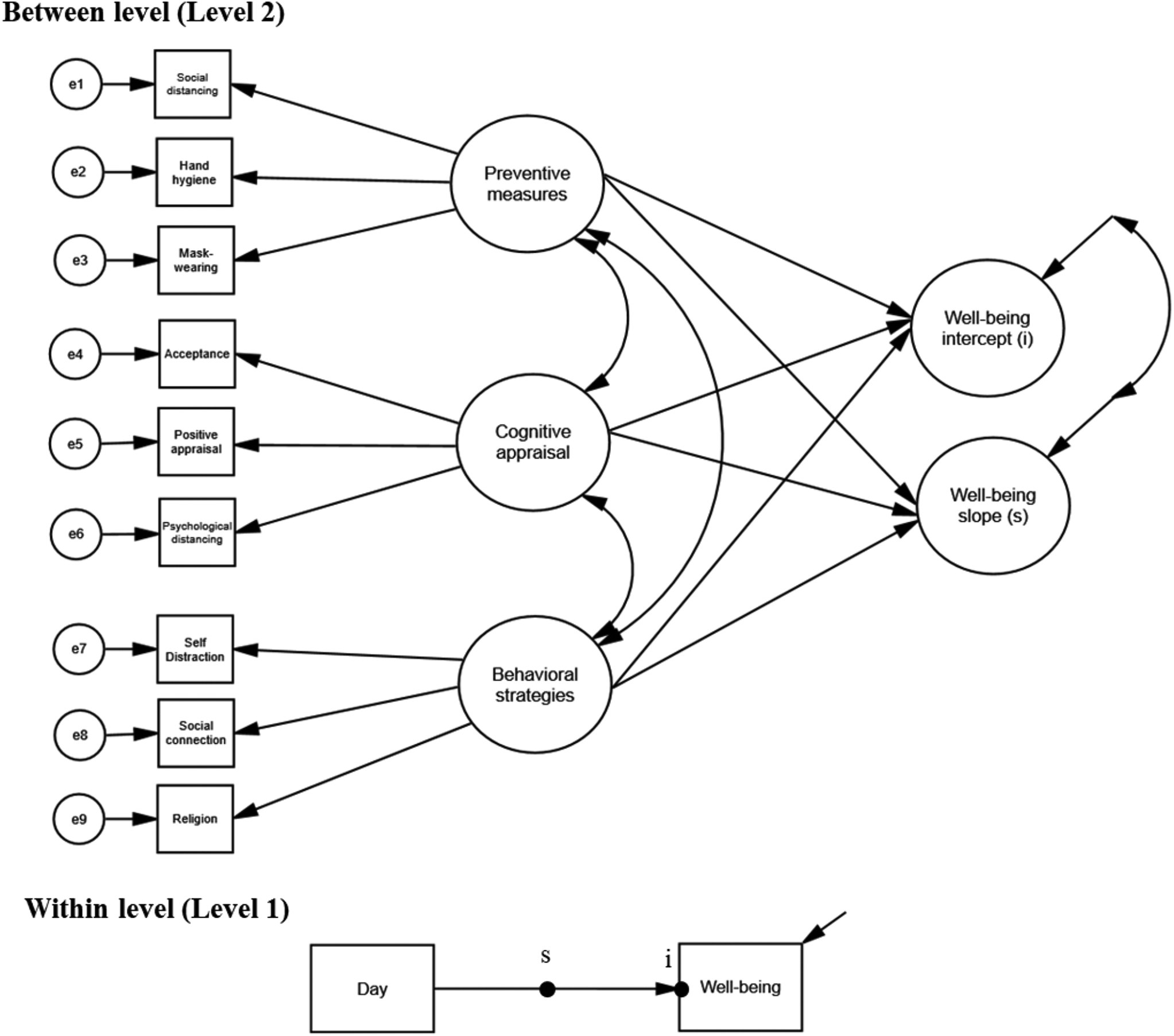
Conceptual model of the intercept and slope as outcome model (Model 3) Note. The filled circle at the end of the arrow from time to well-being represents a random intercept (i), and the filled circle on the arrow from time to well-being indicates a random slope (s). The line with a single arrowhead, oriented at a 45° angle, that points to outcome variables indicates residual variance in this model. The model includes covariates (i.e., gender and age) but, for model simplicity, these are not presented.
Model comparisons were performed by moving from simple (Model 1) to more complex models (Models 2 and 3). A smaller value of the −2log likelihood ratio (deviance), Akaike information criterion, or Bayesian information criterion implies a better fit (Bliese, 2002; Luke, 2004). In addition, a smaller residual variance associated more with a complex model than with a simpler model supports the improvement of model fit.
Results
Measurement Model for Coping Strategies
First, an exploratory factor analysis was performed with the initial nine items to identify underlying constructs of coping strategies. 2 Results supported the three-factor model. The item on “religion,” which did not show sufficiently large factor loadings for any of the factors, was excluded from the model (Matsunaga, 2010; see Table S1 and Table S2 detailed results). Subsequently, in the measurement model (CFA), we labeled each factor as “preventive measures,” “cognitive appraisal,” and “behavioral strategies” with five correlations of error terms added to improve the model. According to the recommendation for good fit indices (Hu & Bentler, 1999), the final measurement model showed good fit with the data, χ2(12) = 303.236, p < .001, comparative fit index = .978, Tucker–Lewis index = .949, root mean square error of approximation = .048, standardized root mean residual = .025; SFigure 1), and it was used as Level 2 predictors in the following analyses. 3
Coping strategies Moderate Change in Well-Being
We investigated whether coping strategies predict the differences in the well-being slopes across individuals. As seen in Table 2, the average initial well-being score was 5.282 (SE = .023), and there was a general decline in well-being during the COVID-19 outbreak, b = –.391, SE = .026, p < .001. This finding was further supported by a regression discontinuity analysis and repeated measures analysis of variance, suggesting a decline in well-being before and after the intensive social distancing (see Table S3 and Figure S2). The comparison of model fit indices revealed that a complex model had a better fit to the data than a simpler model (i.e., Model 3 vs. Model 2 and Model 2 vs. Model 1). The results indicate that individuals’ well-being slopes are different, and coping strategies explained the substantial differences in individuals’ well-being growth rates.
Results of Multilevel Modeling Analysis for Well-Being Index.
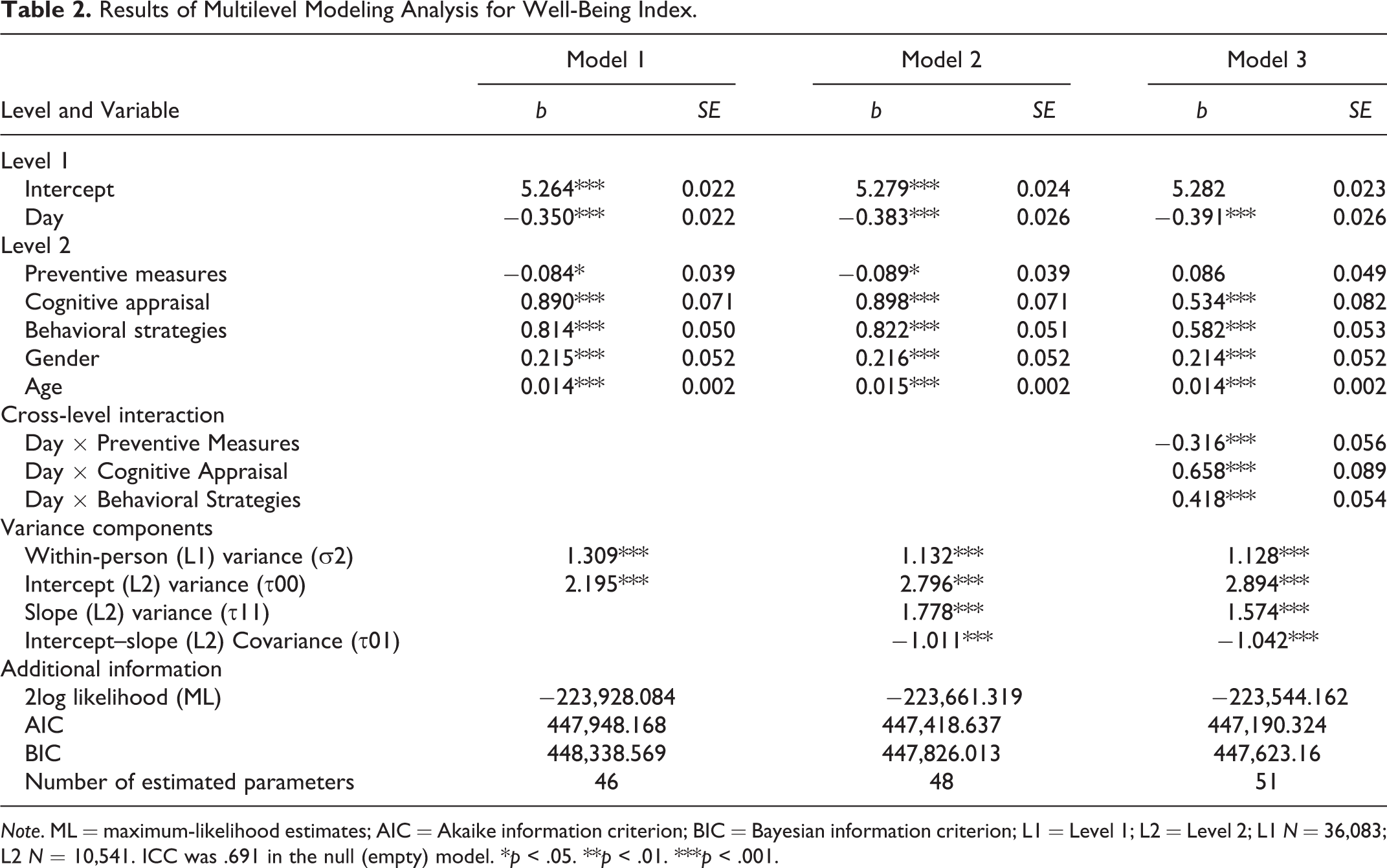
Note. ML = maximum-likelihood estimates; AIC = Akaike information criterion; BIC = Bayesian information criterion; L1 = Level 1; L2 = Level 2; L1 N = 36,083; L2 N = 10,541. ICC was .691 in the null (empty) model. *p < .05. **p < .01. ***p < .001.
In Model 3 (Figure 3), two coping strategies predicted differences in the initial well-being scores across participants, b = .659, SE = .089, p < .001 for cognitive appraisal and b = .419, SE = .534, p < .001 for behavioral strategies such that those who appraised the situation more positively and utilized behavioral strategies to a greater degree had higher initial well-being. More importantly, all three coping strategies significantly explained differences in the individual well-being slopes. Specifically, preventive measures negatively moderated the individual well-being slopes (b = –.316, SE = .056, p < .001) such that those who engaged in more preventive strategies (vs. less) experienced a greater decrease in well-being. For the ease of interpretation, we plotted the simple slopes using a composite score for each coping strategy.
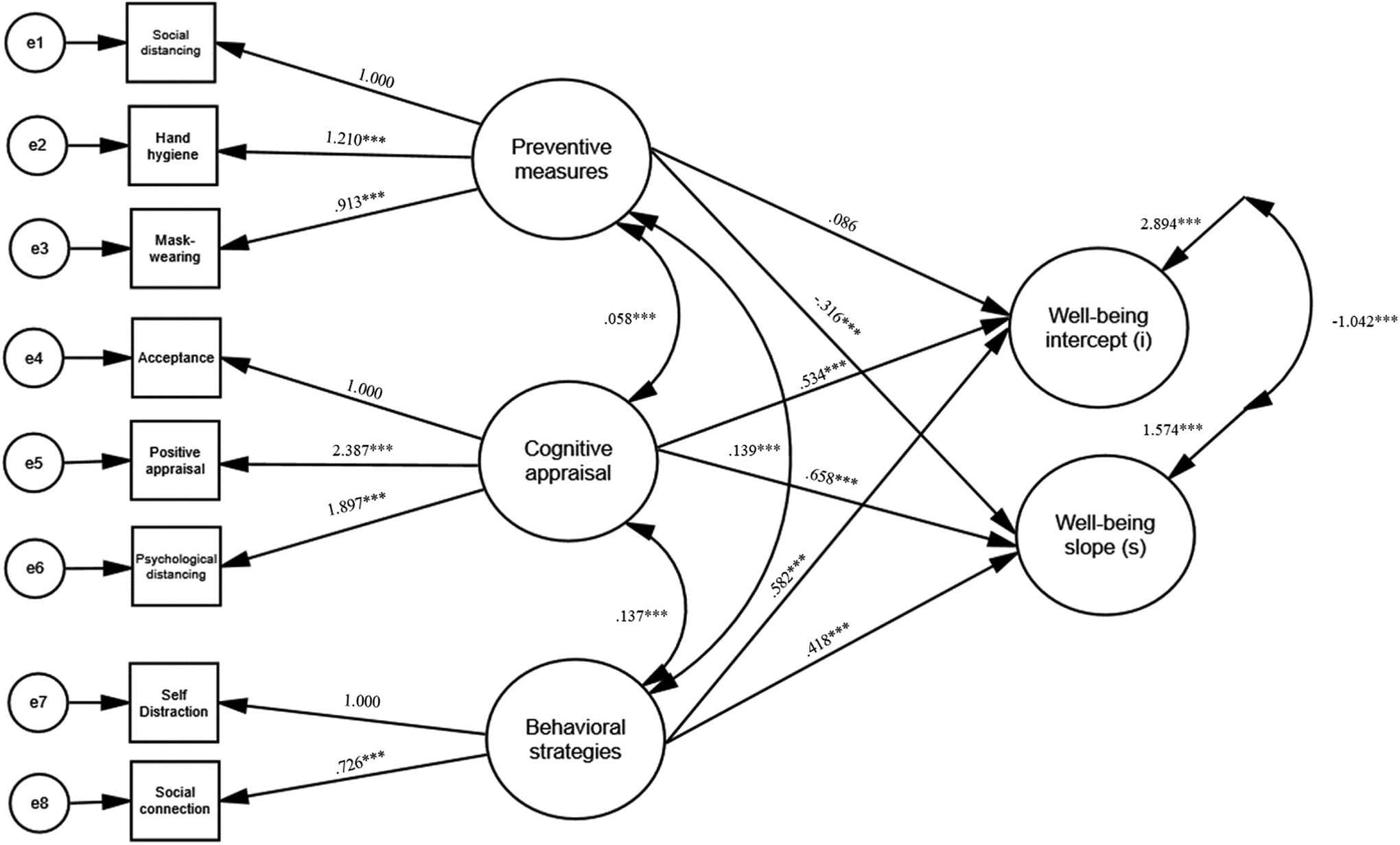
Latent coping strategies that moderate the well-being intercept and slope (Model 3). Note. Unstandardized coefficients are present. The correlations between measurement errors and covariates are drawn in the figure but not displayed for model simplicity. *p < .05. **p < .01. ***p < .001.
As shown in Figure 4, those who practiced preventive behaviors to a greater degree experienced a steeper decline in well-being (b = –.491, SE = .036, p < .001, at +1 SD) than those who engaged in fewer preventive behaviors (b = –.390, SE = .025, p < .001, at the mean; b = –.290, SE = .036, p < .001, at –1 SD).
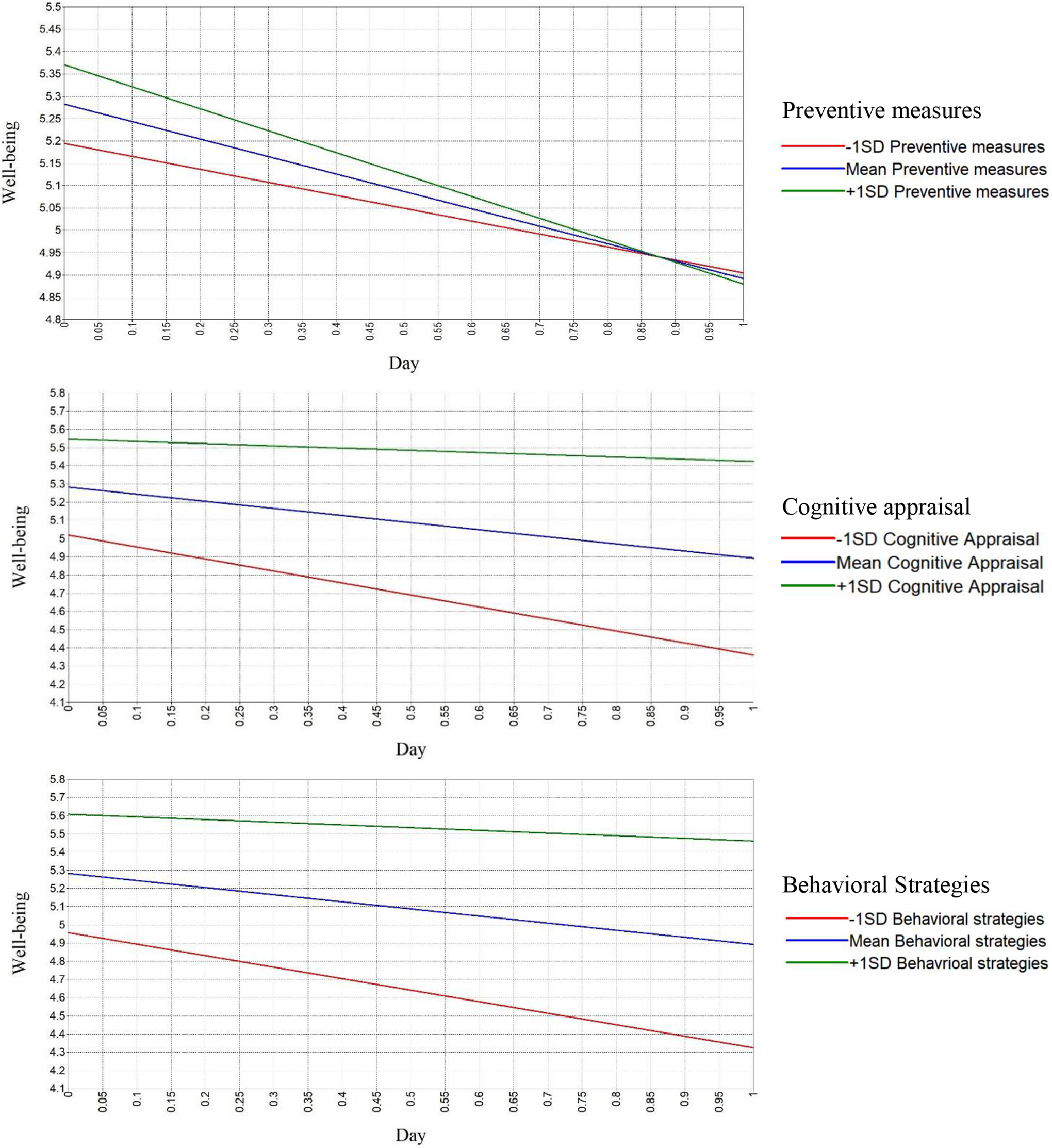
Prediction of changes in well-being by each coping strategy. Note. It depicts moderation effects of each coping strategy on well-being change over time using a pick-a-point approach. A composite score for each coping strategy was used to conduct simple slope analysis: α = .679 for preventive measures (three items), α = .637 for cognitive appraisal (three items), and α = .473 for behavioral strategies (two items)
In contrast, cognitive appraisal (b = .658, SE = .089, p < .001) and behavioral strategies (b = .418, SE = .054, p < .001) were found to attenuate the decrease in well-being. For cognitive appraisal, well-being showed a greater decline at a lower cognitive appraisal value (b = –.659, SE = .037, p < .001, at −1 SD). However, the well-being slope plateaued as the levels of cognitive appraisal increased and showed no significant decline (b = –.390, SE = .025, p < .001, at the mean; b = –.122, SE = .036, p < .01, at +1 SD). Likewise, higher levels of behavioral strategies were associated with steeper slopes (b = –.633, SE = .037, p < .001, at −1 SD; b = –.390, SE = .025, p < .001, at the mean; b = –.148, SE = .036, p < .01, at +1 SD). Further analyses using the Johnson–Neyman technique, which identified the continuous moderator-defined transition points (i.e., the boundaries of significance) at which interactions shift from being nonsignificant to significant, or vice versa (Hayes, 2015, 2017), are included in the Supplemental Materials (SFigure 3).
A series of robustness checks were conducted to test whether our main findings would hold for different subsamples who provided (1) only two well-being responses or (2) three or more responses. We also ran the analysis without the covariates (i.e., sex, age). Results revealed that the main findings that coping strategies significantly predicted the change in individuals’ well-being held across these robustness checks (see Table S4–S8).
Fear of Infection Predicts Changes in Well-Being Through Coping Strategies
Preventive measures were the only strategy found to accelerate a decline in well-being during the outbreak. In contrast, cognitive appraisal and behavioral strategies attenuated well-being decline. One possible explanation is that people with greater fear of infection may be more likely to implement preventive behaviors, which, in turn, may lead to a larger decrease in well-being. Thus, as an auxiliary analysis, we investigated whether fear of infection predicted the well-being slope (as a direct effect) and whether the direct path was significantly mediated by any of the three coping strategies (as indirect effects; see Figure 5). The significance of the indirect effects was confirmed using the Monte Carlo method (Preacher & Selig, 2012), by applying 20,000 random repetitions at a 95% confidence level.
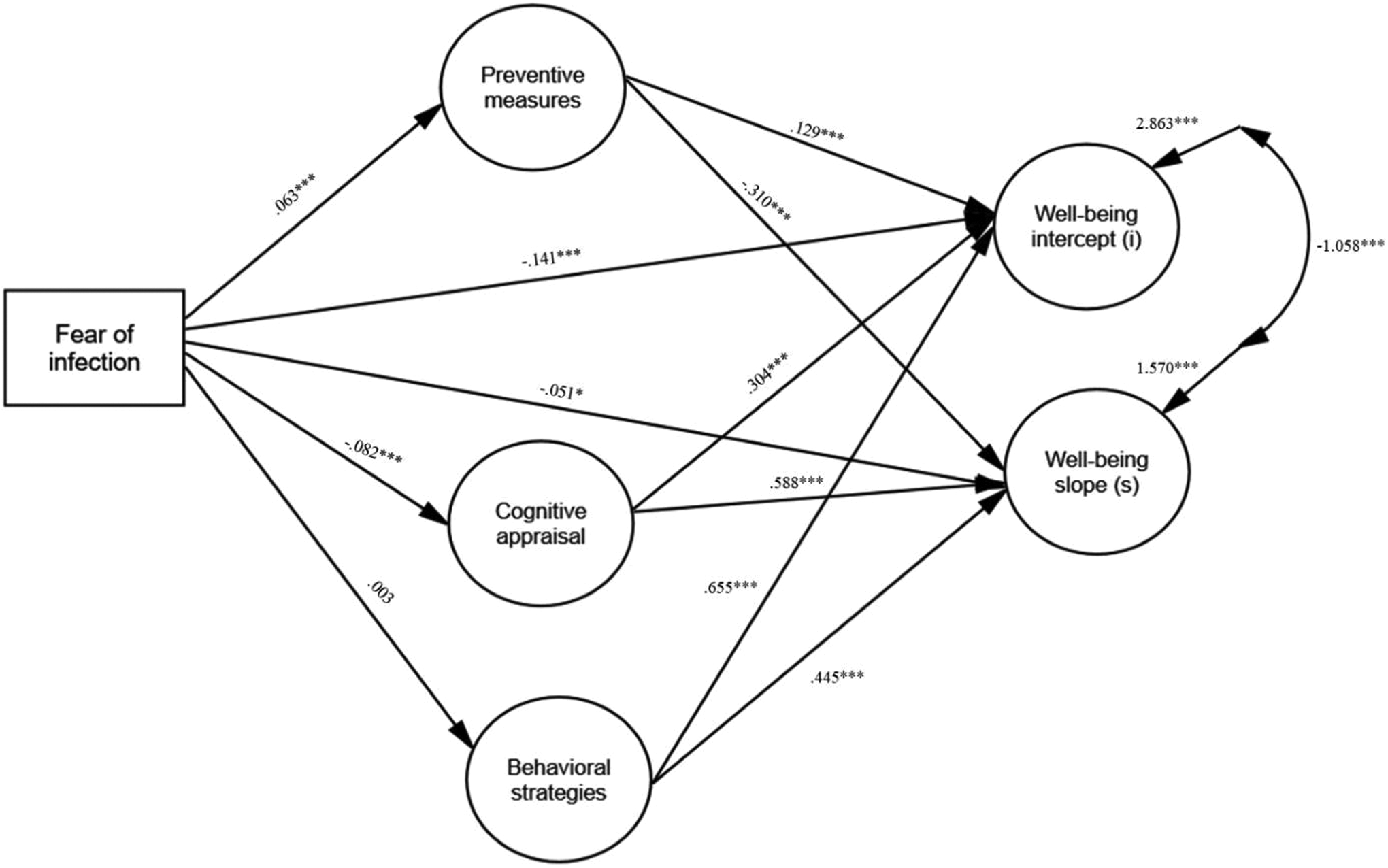
Indirect paths from fear of infection to well-being slopes, through coping strategies. Note. Deviance = −240480.921, AIC = 481085.842, BIC = 481612.035. Unstandardized coefficients are presented. The correlations between residual variances for coping strategies and between covariates are drawn in the figure but not displayed for model simplicity. The direct path from fear of infection to well-being slope was significant (b = – .051, SE = .022, p < .05, 95% CI [–.093, –.008]). In addition, the indirect effect from fear of infection on well-being slope was significant through preventive measures (b = – .020, SE = .004, p < .001, 95% CI [–.028, –.012] and cognitive appraisal (b = –.048, SE = .008, p < .001, 95% CI [–.064, –.033]). * p < .05, ** p < .01, *** p < .001.
Results showed that the path from fear of infection to the well-being slope was partially mediated through preventive measures and cognitive appraisal. Fear of infection negatively predicted the well-being slope (b = – .051, SE = .022, p < .05, 95% CI [–.093, –.008]), indicating that higher fear of infection predicted greater well-being decline. Furthermore, the negative association between fear of infection and the well-being slope was significantly mediated by preventive measures (b = – .020, SE = .004, p < .001, 95% CI [–.028, –.012]) and cognitive appraisal (b = –.048, SE = .008, p < .001, 95% CI [–.064, –.033]). Fear of infection led to greater engagement in preventive measures (b = .063, SE = .005, p < .001), which, in turn, precipitated a decrease in well-being (b = –.310, SE = .058, p < .001). Additionally, fear of infection disrupted the use of cognitive appraisal (b = –.082, SE = .004, p < .001), which also resulted in a larger decrease in well-being (b = .588, SE = .092, p < .001).
Discussion
The current study examined individuals’ well-being changes over a 94-day period during the COVID-19 outbreak in South Korea and explored how the use of different coping strategies across individuals moderated these changes. Using an intensive longitudinal data set collected from a large South Korean sample, we found that overall, participants’ well-being significantly decreased during the COVID-19 outbreak. This pattern was observed even after controlling for the use of coping strategies and demographic variables and also considering individual variability. These findings are consistent with other recent findings showing the impact of COVID-19 on mental health in the general population in other countries such as China (Zhang & Ma, 2020), the United States (Fitzpatrick, Harris, & Drawve, 2020), Denmark (Sønderskov et al., 2020), and New Zealand (Sibley et al., 2020).
We also found that the use of coping strategies, preventive measures, cognitive appraisal, and behavioral strategies significantly moderated the rate of change in well-being across individuals. The results from the simple slope analyses further indicated that those with higher (vs. lower) adherence to preventive behaviors showed greater decreases in well-being, whereas those who utilized more cognitive appraisal and behavioral strategies maintained their well-being over time, compared with those who did not use these coping strategies. These results support a possible explanation that preventive measures, while effective for protecting one’s health, may negatively impact one’s well-being. The causal mechanism for this link is currently unknown; however, this may be due to discomfort and disruption in daily routine (Avni-Babad, 2011) and lack of social interactions (Sandstrom & Dunn, 2014). As speculated earlier, the externally motivated aspect of these behaviors may have further diminished people’s well-being through thwarted autonomy (Ryan & Deci, 2000). Instead, making sense of a difficult situation by focusing on the positive aspects (i.e., positive reappraisal) and psychologically distancing oneself from the threat, actively connecting with others, and engaging in other activities appeared to be more beneficial to well-being during the pandemic. In situations of low controllability, dealing with the threat through cognitive coping appears to result in better well-being than other coping strategies (Folkman, 1984). In addition, during lockdowns, when people are deprived of face-to-face contact and activities, connecting with others online or diverting one’s attention through other indoor activities may also be beneficial.
Further mediational analysis revealed insights regarding the possible effects of fear of COVID-19 infection on the use of different coping strategies, which, in turn, predicted changes in well-being. The results showed that a stronger fear of infection was associated with the increased engagement in preventive behaviors and the reduced utilization of cognitive appraisal, which further accelerated the decline in well-being. The tendency to engage in more preventive behaviors when the perception of threat is higher is consistent with other recent studies examining the responses to COVID-19 (Bashirian et al., 2020; Jang et al., 2020). When individuals are in a high arousal state, such as fear, they are more likely to resort to behavioral coping techniques to manage the problem; however, cognitive appraisal may be more challenging to implement, as it requires a greater cognitive effort. It is also possible that people with greater fear engage more in preventive behaviors as a way to manage their fear; yet, this strategy appears to backfire as shown in the moderation analysis.
Implications and Strengths
The present study sought to understand how the use of different coping strategies impacted well-being over time during the COVID-19 pandemic. In addition, the present study extends the coping literature to self-regulation and adjustment processes in the context of infectious disease outbreaks. Although preventive measures for COVID-19 such as handwashing, wearing face masks, and social/physical distancing are strongly encouraged, worldwide, to protect people from the virus (World Health Organization, 2020), our study is among the first to provide evidence that these behaviors that reduce the risk of infection may come with a cost to well-being. These effects on well-being, however, should never be used to rationalize a lack of engagement in preventive behaviors, which could result in harmful consequences to health (Centers for Disease Control and Prevention COVID-19 Response Team, 2020). Instead, individuals must learn to engage in other coping strategies to buffer the negative effects of preventive measures on well-being during a pandemic, such as cognitive appraisal and self-distraction activities in addition to, and not in place of, preventive measures.
Our findings on the effects associated with increased fear of infection further suggest that the use of certain coping strategies can be detrimental and lead to greater decreases in well-being. Although cognitive appraisal has been shown to be an effective strategy that moderates a reduction in well-being over time, this strategy appears to be difficult to implement when fear of infection is high. Therefore, individuals must learn to manage their fear of infection effectively through other coping strategies such as emotion-focused coping (Lazarus & Folkman, 1984), which may allow them to access a wider variety of coping strategies.
Our study has several strengths that contribute to the literature. First, we used a multilevel, intensive longitudinal design, which considered existing variability in well-being and changes in well-being, across individuals. In addition, our study used momentary measures of well-being to overcome the limitations associated with retrospective measures (Stone & Shiffman, 2002). Finally, by using a latent model, we also addressed possible measurement error issues (B. O. Muthén, 2002), which further strengthens our findings.
Limitations and Future Directions
Our study, however, is not without limitations. First, participants may have self-selected themselves into the survey. Indeed, our results underrepresent the experiences of men in South Korea and may have limited generalizability. Future studies may consider using a stratified sampling strategy to better represent the proportion of gender in the general population. In addition, we examined changes in well-being over time using a linear growth curve to accommodate participants who had limited (three or fewer) data points. Nonlinear changes in well-being may have occurred among some individuals, which would provide additional information regarding patterns of changes in well-being and allow for further analysis of the possible causes underlying those fluctuations. Future studies should, thus, employ more sophisticated growth curve analyses with enough observations from individuals.
Additionally, because coping strategies and fear of infection were measured in only Phase 2, unlike well-being measures, our analysis was limited in its ability to test the within-person changes in these constructs over time or their causal effects. Regarding the moderation effect of coping strategies on changes of well-being, it should be noted that it is possible that differences in well-being change rates across individuals in Phase 1 may have led to differences in coping strategy use in Phase 2. In this study, however, we conceptualized coping strategies as a trait-like construct based on previous literature suggesting that people tend to have habitual coping strategies that are relatively stable across time (Carver & Connor-Smith, 2010). Still, the causal direction between fear of infection and coping strategies should be interpreted with caution as they were measured concurrently.
Finally, although our study tracked changes over 94 days in well-being among individuals, the long-term effects of coping strategies are currently unknown as the pandemic continues to be extended. Future work should examine the impacts of coping strategies in relation to the various stages of the pandemic as well as long-term changes in well-being. In addition, the underlying psychological mechanisms through which various coping strategies influence changes in well-being during the pandemic warrant future research.
Conclusion
As the current COVID-19 pandemic continues to impact the lives of people worldwide, it becomes essential for individuals to learn ways to adjust to the “new normal.” Our findings provide a hint for what types of coping strategies may be effective to maintain our well-being in a pandemic. We suggest that people continue to adhere to preventive behavior to protect and save their own lives and the lives of others but be aware of its potential negative impact on well-being. People should actively use other coping strategies such as finding positive meaning in the situation, keeping a healthy distance from COVID-related thoughts, reaching out to friends and family, and engaging in other interesting activities to survive through this pandemic without sacrificing well-being.
Supplemental Material
Supplemental Material, sj-pdf-1-spp-10.1177_1948550621990595 - The Role of Coping Strategies in Maintaining Well-Being During the COVID-19 Outbreak in South Korea
Supplemental Material, sj-pdf-1-spp-10.1177_1948550621990595 for The Role of Coping Strategies in Maintaining Well-Being During the COVID-19 Outbreak in South Korea by Joo Hyun Kim, Yerin Shim, Incheol Choi and Eunsoo Choi in Social Psychological and Personality Science
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present research was supported by Center for Happiness Studies at Seoul National University (Grant 0404-20200007).
Supplemental Material
The supplemental material is available in the online version of the article.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.