
Abstract
People who believe they are invulnerable to infectious diseases often fail to protect themselves against the disease threats that others pose to them. The current paper hypothesizes that social pain—the experience of feeling interpersonally hurt or rejected—can sensitize the behavioral-immune system by giving people added reason to see others as worthy of protecting themselves against. We obtained four daily diary samples involving 2,794 participants who reported how hurt/rejected they felt by those they knew, how personally concerned they were about the spread of illness/COVID-19, and how vigilantly they engaged in self-protective behaviors to safeguard their health each day. An integrative data analysis revealed robust evidence that people who believed they were invulnerable to infectious disease engaged in more concerted efforts to protect themselves against the greater daily risk of contracting COVID-19 when being in acute social pain gave them added reason to see others as harmful to them.
Although humans are strongly motivated to connect to others (Baumeister & Leary, 1995), there are times when it makes sense to be wary of getting too close. Not only can other individuals reject and ostracize us (Leary & Baumeister, 2000), but the COVID-19 pandemic has also made it quite salient that they can also expose us to contagious diseases (Salathé et al., 2010). Fortunately, we have systems in place that identify when others pose each of these distinct social and physical risks and motivate appropriate self-protective behaviors (Miller & Maner, 2012; Murray et al., 2006). However, these risk-control systems are not impervious to other influences; despite these systems, we can too readily forgive a badly-behaving spouse or too blithely share handshakes with friends when COVID-19 infections are soaring.
Prior research examining these risk-control systems has almost exclusively focused on situations where either the motivation to avoid infection or the motivation to avoid rejection dominates. Indeed, experimental research invariably primes either infection or rejection risk, tacitly assuming that people only need to manage one risk at a time (Mortensen et al., 2010; Sacco et al., 2014). Nevertheless, in many settings, especially in the age of COVID-19, social interactions simultaneously present the risk of rejection and infection.
Recognizing this reality, the present research is the first to examine whether the systems that regulate infection and rejection risk can work in tandem. We argue that experiencing social pain—feeling acutely hurt or rejected by others—can sensitize or upregulate the behavioral-immune system by giving people added reason to see others as potentially selfish and worthy of protecting against. Accordingly, across four daily diary samples, we hypothesize that social pain can motivate people who would not normally worry about catching infectious diseases to take extra daily steps to physically protect themselves against the disease threat posed by COVID-19.
Regulating Infection Risk
People are equipped with behavioral-immune systems that help protect them against the risk of being physically infected by others (Murray & Schaller, 2016). The behavioral-immune system links visible cues to infection risk to the behavioral impulse to be vigilant and avoid others (Miller & Maner, 2012; Sacco et al., 2014; Tybur & Lieberman, 2016). For instance, participants primed with images of infectious disease are more likely to pull away from human faces (Mortensen et al., 2010), forego opportunities for romantic connection (Sawada et al., 2018), and distrust outgroups (Navarrete & Fessler, 2006), as compared with control participants.
Nevertheless, on its own, the behavioral-immune system may offer only partial protection against the risk of infection. First, while some disease threats are easily detected, others are not. Indeed, viral infections like COVID-19 cannot always be visually detected (Bai et al., 2020) or flagged by group membership (Ji et al., 2019; Kim et al., 2016; Oaten et al., 2011; O’Shea et al., 2020), which could compromise the protection the behavioral-immune system can offer. Second, while some infectious individuals are easily avoided, others are not. For example, everyone is a threat in the presence of highly contagious viruses like COVID-19, forcing people to choose between the safety of complete isolation and the strong desire to affiliate (Navarrete & Fessler, 2006; Qian et al., 2020). Third, and most relevant to the current research, people who are less sensitive to disgust (Aaroe et al., 2016; Kupfer & Tybur, 2017) or perceive themselves to have highly effective biological immune systems (Clay et al., 2012) even discount the infection risk potentially dangerous strangers pose (Neuberg et al., 2011), further limiting the protection the behavioral-immune system can offer. For example, experimentally priming disease repels people who feel highly susceptible to contagious diseases from approaching human faces, but it has no such effect on people who feel less susceptible (Mortensen et al., 2010).
For all of these reasons, we contend the behavioral-immune system could conceivably better protect people against the risk of physical infection if it had evolved to be sensitive to additional diagnostic aspects of experience that alert people to the harm others can pose to them. Social pain seems well-positioned to provide just such needed motivational reinforcement.
Reinforcing the Behavioral-Immune System Through Social Pain
Social pain refers to the hurt feelings people experience due to interpersonal rejection or loss (MacDonald & Jensen-Campbell, 2011; MacDonald & Leary, 2005). Rejecting experiences, like being criticized by spouses, ignored by friends, chastised by coworkers, or ostracized by acquaintances, elicit social pain or hurt feelings. Such social pain, in turn, serves to (a) alert people to the risks that others pose to them and (b) motivate them to take corrective action to foster greater interpersonal safety or security (Leary & Baumeister, 2000; Leary & Gabriel, 2021; MacDonald & Leary, 2005; Murray et al., 2006; Richman & Leary, 2009).
However, the corrective actions people take in response to social pain vary contextually, according to the risks and opportunities in ongoing situations (DeWall & Richman, 2011; Maxwell et al., 2013; Richman & Leary, 2009). Sensibly, social pain motivates people to self-protect and avoid social connections that have proven to be unsafe (Murray et al., 2006; Twenge, 2005). For instance, priming a rejecting close other automatically activates thoughts of distancing from that person (Cavallo et al., 2010; Gillath et al., 2006; Murray et al., 2008). Just as sensibly, social pain motivates people to set self-protection aside and approach social connections that promise the likelihood of being safe. For instance, people who have been rejected or excluded are quicker to detect sincere smiles (DeWall et al., 2009), pursue new friendships (Maner et al., 2007), and ingratiate themselves to impressionable acquaintances (Williams et al., 2000).
Because the motivating effects of social pain depend on the risks and opportunities apparent in ongoing situations, its capacity to sensitize the behavioral-immune system should vary according to the disease threat people perceive in specific situations. In situations where people are more concerned about COVID-19 than usual, other individuals should seem unsafe and worth avoiding. Indeed, people socially isolate individuals who possess markers of infectious disease (Oaten et al., 2011). In such a high-threat disease context, experiencing greater social pain should give people who are normally insensitive to disease threat added reason to see others as potentially harmful to them, thereby affording them necessary additional motivation to protect themselves against COVID-19. However, in situations where people are less concerned about COVID-19 than usual, other individuals should seem comparatively safe and worth approaching. In such low-threat disease contexts, experiencing greater social pain might instead give people who are normally insensitive to disease threat greater reason and motivation to relax their efforts to protect themselves against COVID-19.
The Present Research
This paper presents an integrative analysis of four daily diary samples (2,794 participants, 18,661 observations) across two countries (United States, United Kingdom) obtained in the first 6 months of the COVID-19 pandemic. Relative to analyzing samples individually, combining data sets into one affords increased statistical power and tests of generalizability (Curran & Hussong, 2009). 1
We measured three predictor variables: (a) individual differences in disease-sensitivity, captured through self-perceived vulnerability to contracting infectious disease (Duncan et al., 2009), (b) daily social pain, captured through feelings of being hurt/rejected by known others (MacDonald & Jensen-Campbell, 2011), and (c) daily disease threat, captured by personal concerns about the disease risk posed by COVID-19. We indexed the criterion variable—daily self-protective behavior—through (a) restriction of social and work behaviors due to health worries and (b) engagement in six behaviors that public health officials recommended to protect oneself and others against COVID-19 (Eikenberry et al., 2020; Lyu & Wehby, 2020).
We expected social pain to sensitize underactive behavioral-immune systems—motivating people who would not normally worry about infectious diseases to be more vigilant about protecting themselves when COVID-19 posed greater daily threat. That is, on days when people were more concerned about COVID-19 than usual, making social connection less safe, we expected experiencing greater social pain to provide added reason to avoid others, thereby motivating people low in disease-sensitivity to engage in more self-protective behavior. However, on days when people were less concerned about COVID-19 than usual, making social connection safer, we expected experiencing greater social pain to provide added reason to approach others, thereby motivating people low in disease-sensitivity to engage in less self-protective behavior. Unlike lows, people high on disease-sensitivity possess relatively overactive behavioral-immune systems, often protecting themselves against nebulous disease threats (Neuberg et al., 2011). Therefore, we did not expect people high in disease-sensitivity to need the incentive supplied by social pain to self-protect (Shook et al., 2020; Terrizzi et al., 2013).
Method
This research was approved by the University at Buffalo Institutional Review Board. We based the sample sizes of the funded studies on Monte Carlo power simulations to detect at least two-way cross-level interactions (Mathieu et al., 2012), using input parameters derived from tests of related questions in our prior diary research. These simulations suggested power to detect two-way interactions should approximate .90. 2 The Supplementary Online Material (SOM) provides greater detail about the samples and procedures/measures not relevant to the current report. Although not preregistered, the data are on OSF (https://osf.io/sfa25/?view_only=2c5dd8728f444b3cb9032d1d953526a2). Data from Sample 4 were included in two submitted manuscripts and one published paper (see SOM).
Participants
Sample 1
Using the online platform Prolific Academic, we recruited 500 paid participants (250 U.S.; 250 U.K.) for a 10-day study, expecting 350 to complete 8/10 assessments. Participants had to be in monogamous, heterosexual live-in romantic relationships, U.S. or U.K. residents, native English speakers, and pass a research integrity check. Ultimately, 478 participants finished 9/10 assessments on average; 76% completed all 10. Participants (164 men) averaged 36.3 years in age (SD = 11.5); relationships averaged 11.0 (SD=10.4) years in length (152 dating, 44 engaged, 281 married); 255 had 1.9 children (SD = 0.9). Of the 344 employed participants, 36% were prioritized to work in person. U.S. participants lived across 41 states, with most from Florida (9%), Illinois (6.4%), New York (7.3%), North Carolina (5.6%), Ohio (6.4%), and Texas (6.4%); U.K. participants resided in England (87.3%), Scotland (7.8%), Wales (3.3%), and Northern Ireland (1.6%). Participants provided daily reports April 6 to 15, 2020. 3
Sample 2
Using the online platform ResearchMatch, we solicited 1,884 participants to attempt the first assessment of an 8-day study (for a chance to win 1/100 $10 Amazon gift cards). Participants had to be U.S. residents, native English speakers, and pass a research integrity check. We oversampled, expecting greater attrition and missing data in volunteers and decided a-priori to drop any participant who completed only the first, background assessment, leaving a total sample of 1,546. These participants finished 5.7/7 of the daily assessments on average; 51% completed all 7. They (275 men) averaged 45.3 years in age (SD = 17.1); 469 were single and 1,049 were in romantic relationships averaging 15.0 (SD = 14.9) years (56 casually dating, 292 exclusively dating, 57 engaged, 644 married); 673 participants had 2.2 children (SD = 1.1). Of the 904 employed participants, 37% were essential workers. Participants lived across 49 states, with the largest subsets in Oklahoma (9.8%), North Carolina (9%), and California (5%), and provided daily reports between April and May, 2020.
Sample 3
We recruited 215 undergraduates taking Introductory Psychology for a 10-day study for course credit in April–May, 2020. We enrolled as many participants as we could before the semester ended. Participants had to pass a research integrity check. Participants finished 5/9 daily assessments on average; 18% completed all 9. Participants (120 men) averaged 19.1 years in age (SD = 1.6); 135 were single and 80 were in romantic relationships averaging 1.3 (SD = 1.4) years in length (22 casually dating, 57 exclusively dating, 1 engaged).
Sample 4
We contracted the research firm Qualtrics to recruit 400 participants, so it oversampled, soliciting 716 to attempt the first assessment. Participants had to be U.S. citizens in monogamous, heterosexual live-in romantic relationships, native English speakers, and pass a research integrity check. Qualtrics did not recontact participants who failed to complete the second assessment, leaving 550 completing 9.6/11 assessments on average (with 348 completing all 11). Participants (268 men) averaged 42.6 years (SD = 11.7), 363 had 2.1 children (SD = 1.1), and relationships averaged 13.3 (SD = 10.2) years (130 dating, 36 engaged, 389 married). Of the 392 employed participants, 25.3% were essential workers. Participants lived across 41 states, with most from California (15.3%), North Carolina (11.9%), Indiana (10.5%), Vermont (5.9%), and Hawaii (5.4%). Participants were recruited in two 3-week cohorts in May and June, 2020.
Procedure
Each study was conducted online. On the first day, participants completed background surveys containing demographic and personality measures assessed once, including disease-sensitivity. In Samples 1 to 3, subsequent daily surveys were emailed to participants at 6:00 p.m. local time for the next 9 consecutive days in Samples 1 and 3 and 7 consecutive days in Sample 2. Participants had until 6:00 a.m. local time the next morning to complete the survey. In Sample 4, subsequent daily surveys were emailed to participants at 5:00 p.m. local time every other day for the next 3 weeks, resulting in 10 bi-daily assessments. Participants had until a specified (local) time the next morning (6:00–7:00 a.m.) to complete the survey. Samples 1 to 3 were nonexperimental; Sample 4 participants were randomly assigned to one of two experimental conditions (see SOM).
Measures
Disease-Sensitivity
Participants completed only the 6-item perceived infectability subscale of the Duncan et al. (2009) perceived vulnerability to disease scale (e.g., “In general, I am very susceptible to colds, flu, and other infectious diseases,” “If an illness is going around, I will get it,” reversed, 1 = strongly disagree, 6 = strongly agree). 4
Daily Social Pain
Participants reported on daily experiences of social pain by responding to the question, “Overall, how hurt or rejected did people you know make you feel today?,” 0 = not at all, 6 = a lot. Higher scores corresponded to greater social pain. 5
Daily Concerns About COVID-19
In Samples 1 to 3, participants rated their concern about “the spread of illness” and “COVID-19/Coronavirus” each day, 0 = not at all concerned, 4 = extremely concerned; we averaged these two items to index daily concern about the disease threat posed by COVID-19. In Sample 4, participants only rated their concern about “COVID-19/Coronavirus” each day, 0 = not at all concerned, 4 = extremely concerned.
Daily Health Worries Restricting Normal Activities
Each day participants rated how much time worries about their health (a) interfered with social activities and (b) made it difficult to perform work or other regular daily activities, 0 = none of the time, 4 = all of the time.
Daily Public Health–Recommended Behavior
Each day participants rated how much effort/energy they spent engaging in six behaviors: “washing my hands for at least 20 s,” “using hand sanitizer,” “keeping physical distance (at least 6 feet/2 meters) between myself and another person when in public,” “covering my coughs/sneezes,” “trying not to touch my face,” and “wearing a face mask.” In Samples 1 to 3, the response scale ranged from, 0 = no effort/energy at all, 4 = an extreme amount of effort/energy; in Sample 4, it ranged from 0 = not at all, 7 = a lot.
Daily Physical Pain
Each day participants rated their physical pain to allow us to compare the effects of social and physical pain, 0 = no pain at all, 10 = pain as bad as you can imagine, https://www.physiopedia.com/Numeric_Pain_Rating_Scale.
Results
In conducting the analyses, we wanted to capture self-protective behavior broadly (Diamantopoulos et al., 2008) because engaging in one type of self-protective behavior may reduce the need to engage in other types of behavior. For instance, someone who has completely restricted her interactions to her home has little need to mask or stand 6 feet apart from strangers. Therefore, to ensure we captured the substitutable ways that participants might self-protect, we z-scored and averaged daily reports of health worries restricting one’s activities and engaging in health-protective behavior into a composite index of self-protective behavior. 6
We also wanted to provide evidence consistent with the predicted direction of causality. By exposing people to manipulations intended to simulate real-world experiences, experiments provide the gold standard for establishing causality (Aronson et al., 1989). However, some real-life experiences cannot be easily or ethically simulated, as is the case with a pandemic health threat. In such cases, diary data can be used to shed light on how causal processes unfold within a person over time (Bolger et al., 2003; Neubauer & Schmiedek, 2020; Wickham & Knee, 2013). We used the over-time nature of our data to separate cause and effect temporally—using yesterday’s experiences to predict today’s behavior. In so doing, we assume that people greet each new day informed and influenced by previous experiences (Murray et al., 2003).
Model Specification
We modeled the data as a two-level nested structure using MLwiN (Goldstein et al., 1998) with time of assessment at Level 1 (within) and participant at Level 2 (between). We predicted today’s self-protective behavior from (a) a random intercept term, (b) the main effect of the prior day’s social pain (i.e., feeling hurt/rejected), a lagged within-person variable centered on the person’s daily mean, (c) the main effect of the prior day’s concern about COVID-19, a lagged within-person variable centered on the person’s daily mean, (d) disease-sensitivity, a between-person variable centered on the sample mean, and (e) the two- and three-way interactions between the prior day’s social pain, the prior day’s COVID-19 concerns, and disease-sensitivity. We modeled the focal within-person main effects as random. 7
We also included the (a) value of the outcome variable on the prior day to control for the autoregressive effects of time, (b) linear effect of time to control for collectively shared events on a given day or maturational changes in participants, (c) sample (dummy-coded, with three orthogonal contrasts), (d) main effects of participants’ mean daily social pain and mean daily concern about COVID-19 (both between-person variables), their two-way interaction, and their interactions with disease-sensitivity. Including the between-person means ensures daily-level effects are not confounded with between-person effects (Bolger & Laurenceau, 2013).
This model specification presents as close a naturalistic analogue to an experiment as nonexperimental data afford. First, person-centering the within-person variables treats participants as their own control. Importantly, this allows us to (a) gauge the “administration” of each independent variable by comparing days when people reported greater than usual social pain (or COVID-19 concern) to days when they reported less than usual social pain (or COVID-19 concern) and (b) rule out third-variable (i.e., individual difference) explanations for the daily effects. Second, examining the interactive effects of the prior day’s social pain and COVID-19 concern on today’s self-protective behavior temporally separates the naturalistic “administration” of the independent variables from the measurement of the dependent variable.
Principal Analyses
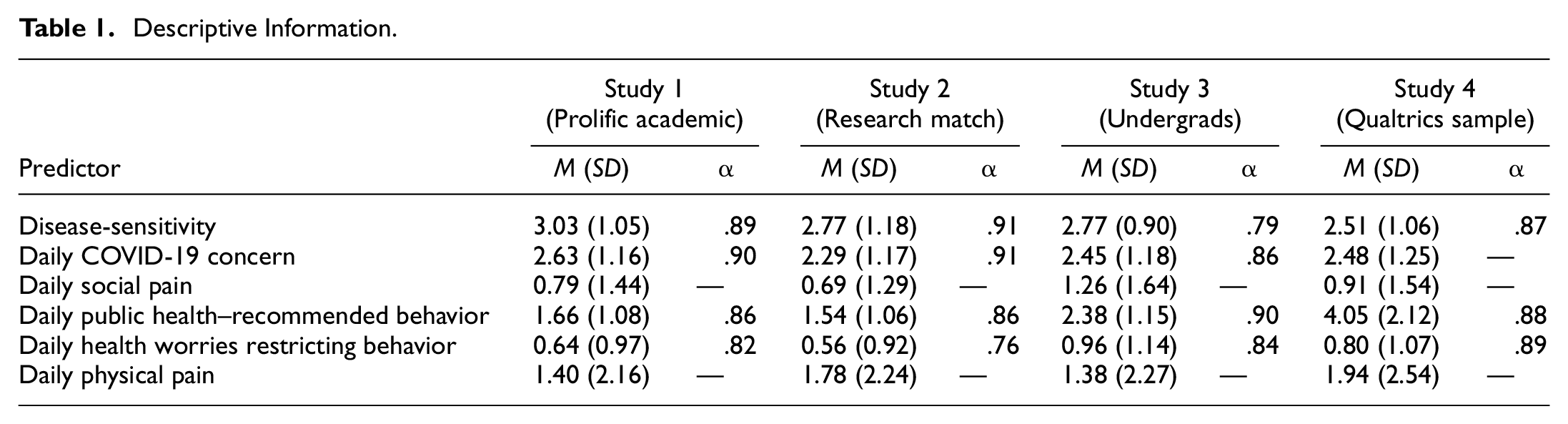
Tables 1 and 2 contain the descriptive information and intercorrelations, respectively.
Descriptive Information.
Intercorrelations Among the Primary Variables Used in the Integrative Data Analyses.
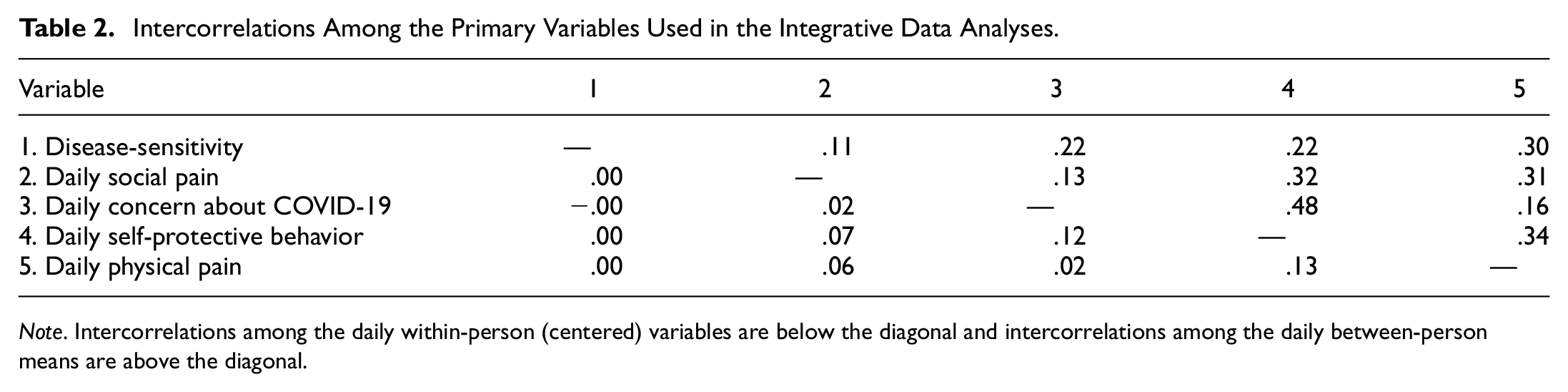
Note. Intercorrelations among the daily within-person (centered) variables are below the diagonal and intercorrelations among the daily between-person means are above the diagonal.
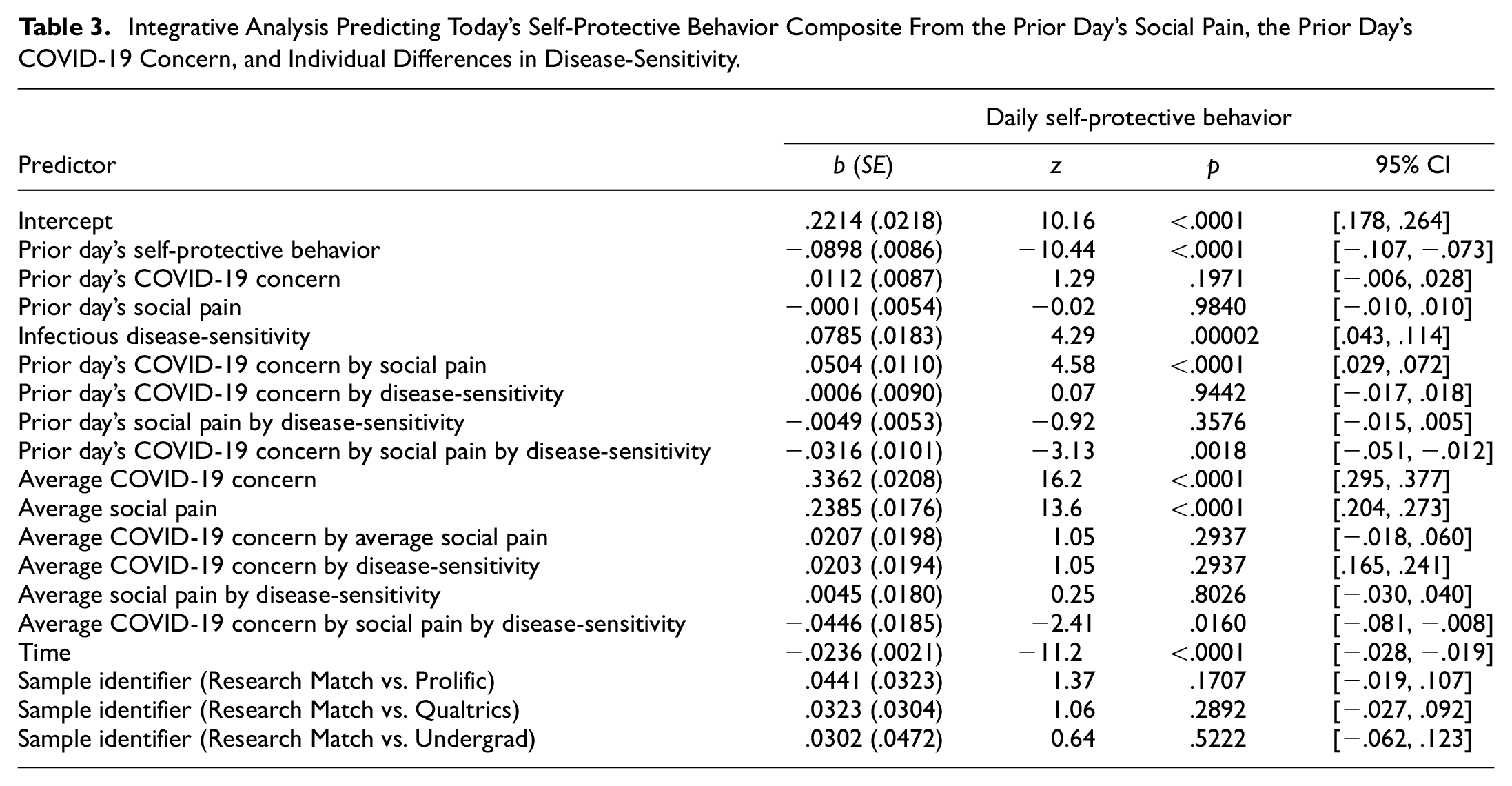
Table 3 presents the results of the multilevel analyses predicting the composite index of self-protective behavior. The predicted three-way interaction between the prior day’s social pain, the prior day’s COVID-19 concern, and disease-sensitivity was significant. 8 Figure 1 presents the predicted scores. Decomposing the three-way into its constituent lower-order effects revealed consistent evidence that social pain sensitized underactive behavioral-immune systems. 9
Integrative Analysis Predicting Today’s Self-Protective Behavior Composite From the Prior Day’s Social Pain, the Prior Day’s COVID-19 Concern, and Individual Differences in Disease-Sensitivity.

Today’s Predicted Self-Protective Behavior From the Prior Day’s COVID-19 Concern, the Prior Day’s Social Pain, and Individual Differences in Disease-Sensitivity.
First, and perhaps most importantly, the experiential coupling of social pain and disease threat on the prior day more strongly motivated participants with underactive than overactive behavioral-immune systems to self-protect. That is, consistent with predictions, the two-way prior day’s social pain by COVID-19 concern interaction predicting self-protective behavior was significantly positive for participants low on disease-sensitivity (1 SD below the mean), b = .0820, SE = .0153, z = 5.36, p < .00001, 95% confidence interval (CI) = [.052, .112], but not for those high on disease-sensitivity (1 SD above the mean), b = .0188, SE = .0145, z = 1.30, p = .1936, 95% CI = [−.010, .047].
Second, and also consistent with predictions, when daily disease threat was high on the prior day, simultaneously experiencing greater social pain more strongly motivated participants with underactive than overactive behavioral-immune systems to self-protect. That is, when disease threat was high, the two-way prior day’s social pain by disease-sensitivity interaction was significantly negative, b = −.0182, SE = .0066, z = −2.76, p = .00578, 95% CI = [−.031, −.005]. When participants were more concerned about COVID-19 on the prior day, those low in disease-sensitivity subsequently engaged in significantly more self-protective behavior when they experienced greater social pain, as compared to days they experienced less social pain. This simple effect of the prior day’s social pain was significantly positive, b = .0392, SE = .0098, z = 4.00, p = .000063, 95% CI = [.020, .058]. However, the simple effect of social pain was not significant for when participants high in disease-sensitivity experienced high disease threat on the prior day, b = .0029, SE = .0093, z = 0.31, p = .7566, 95% CI = [−.015, .021]. In contrast, when disease threat was low on the prior day, the two-way prior day’s social pain by disease-sensitivity interaction was not significant, b = .0084, SE = .0071, z = 1.18, p = .238, 95% CI = [−.006, .022], but the simple effect of the prior day’s social pain was significantly negative, b = −.0213, SE = .0072, z = −2.96, p = .003076, 95% CI = [−.035, −.007]. When participants were less concerned about COVID-19 on the prior day, those who also experienced greater social pain subsequently engaged in significantly less self-protective behavior, as compared with days they experienced less social pain.
Third, and also consistent with predictions, when daily social pain was high, participants with underactive behavioral-immune systems were more likely to protect themselves than participants with overactive behavioral-immune systems, although the contrasting conditional two ways just reached significance. That is, when participants experienced greater social pain than usual on the prior day, the prior day’s COVID-19 concern by disease–sensitivity interaction was significantly negative, b = −.02204, SE = .01127, z = −1.96, p = .049996, 95% CI = [−.044, .000]. When participants low on disease–sensitivity experienced greater social pain, they subsequently made more effort to protect themselves when they were more concerned about COVID-19 on the prior day, as compared with days they were less concerned about COVID-19, b = .0695, SE = .0160, z = 4.34, p = .000014, 95% CI = [.038, .101]. However, when participants high on disease–sensitivity experienced greater social pain, the prior day’s COVID-19 concern had no significant effect, b = .0254, SE = .0163, z = 1.56, p = .11876, 95% CI = [−.007, .057].
In contrast, when daily social pain was low, participants with underactive behavioral-immune systems were less likely to protect themselves in response to the daily disease threat posed by COVID-19 than participants with overactive behavioral-immune systems. That is, when participants experienced less social pain on the prior day, the prior day’s COVID-19 concern by disease–sensitivity interaction was significantly positive, b = .0233, SE = .01185, z = 1.97, p = .048838, 95% CI = [−.001, .047]. Specifically, when participants low on disease–sensitivity experienced less social pain on the prior day, they subsequently made less effort to protect themselves against the virus when they were more concerned about COVID-19 on the prior day, as compared with days were less concerned about the virus, b = −.0481, SE = .0169, z = −2.85, p = .004372, 95% CI = [−.081, −.015]. However, when participants high on disease–sensitivity experienced less social pain, the prior day’s COVID-19 concerns had no significant effect on self-protective behavior, b = −.0017, SE = .0166, z = −0.10, p = .92, 95% CI = [−.034, .031]. 10
Ruling In/Out Explanations
The findings thus far suggest that the experience of social pain can sensitize the behavioral-immune system for people who are normally less sensitive to disease threats. Admittedly, when participants experienced greater (vs. less) social pain, the two-way prior day’s COVID-19 concern by disease-sensitivity interactions just reached significance. However, the simple effects of the prior day’s COVID-19 concern underlying these interactions were clearly significant for people low on disease–sensitivity, but not for those high on disease-sensitivity. Nonetheless, social and physical pain often co-occur (MacDonald & Leary, 1995). To examine whether social pain played a unique moderating role, we added the main and moderating effects of daily physical pain to the models. The three-way involving social pain was still significant, b = −.0305, SE = .0102, z = −2.99, p = .0028, 95% CI = [−.050, −.011], but the three-way involving physical pain was not significant, b = .0041, SE = .0162, z = −0.25, p = .80, 95% CI = [−.028, .036].
Discussion
People are remarkably varied in how they respond to threats. Even at the height of the COVID-19 pandemic, participants high in disease–sensitivity engaged in markedly more self-protective behavior than participants low in disease–sensitivity across contexts (Shook et al., 2020). Yet, despite this individual difference in behavioral-immune system activation, we provided novel evidence that social pain had contextually-bound sensitizing (and desensitizing) effects.
When participants were more personally concerned about COVID-19 than usual, making social connection less safe, participants low in disease–sensitivity vigilantly engaged in more self-protective behavior when they felt more hurt/rejected, as compared with when they felt less hurt/rejected. In contrast, when participants were less personally concerned about COVID-19 than usual, making social connection safer, participants—regardless of disease-sensitivity—engaged in less self-protective behavior when they felt more hurt/rejected, as compared with days they felt less hurt/rejected. Furthermore, when participants low in disease–sensitivity felt more hurt/rejected (i.e., high social pain), they vigilantly engaged in more self-protective behavior when they were more personally concerned about COVID-19, as compared with when they were less concerned. However, when participants low in disease–sensitivity felt less hurt/rejected (i.e., low social pain), they engaged in less self-protective behavior when they were more concerned about COVID-19, as compared to days they were less concerned.
The present findings have strengths and limitations. On the plus side, the effects were robust across four daily diary samples utilizing large Ns, overlapping measures, and multiple assessments. The lagged analyses also separated hypothesized causes from effects. Furthermore, the predicted moderation effects were specific to social and not physical pain. Admittedly, the effects were small (see SOM), although that is expected given the multiplicity of factors likely to control self-protective behavior (Götz et al., 2021). On the negative side, the three-way interaction evident for the composite index of self-protection was significant for health worries restricting activities (Supplementary Table 1) but approached significance for public-health-recommended behavior (Supplementary Table 2), which happens even in the presence of a true effect (Lakens & Ets, 2017; Stanley & Spence, 2014). Nevertheless, meta-analyzing the samples revealed that the three-way interaction was significant for the composite index and its components (see SOM).
Human survival depends on social connection (Baumeister & Leary, 1995). Therefore, feeling hurt by others—aka feeling social pain—motivates people to take corrective action to keep themselves from being hurt again (Leary & Baumeister, 2000; Murray et al., 2006). However, to be most adaptive, such corrective actions should be context-dependent (Richman & Leary, 2009). The present findings provide the first evidence that social pain motivates people to be at times vigilant, and at times comparatively lax, about protecting themselves against COVID-19. Future research might examine whether social pain similarly motivates people who normally feel invulnerable to disease to engage in other forms of self-protection, such as outgroup avoidance. But, beyond this theoretical advance, the findings may have important practical implications. For instance, people are often unwilling to get preventive vaccinations because they feel personally invulnerable to disease. Reminding people of common everyday experiences of being hurt by others might help nudge the complacent to consider the wisdom of getting vaccinated by reminding them they cannot always count on others to protect them.
Conclusion
Social pain hurts to motivate people to take action to make social connection safer and less interpersonally risky. The present findings suggest that the acute experience of social pain motivates those who normally see little reason to self-protect against infectious disease to take steps to protect themselves, and others, from physical harm.
Supplemental Material
sj-docx-1-spp-10.1177_19485506221107741 – Supplemental material for Sensitizing the Behavioral-Immune System
Supplemental material, sj-docx-1-spp-10.1177_19485506221107741 for Sensitizing the Behavioral-Immune System by Sandra L. Murray, Ji Xia, Veronica M. Lamarche, Mark D. Seery, James McNulty, Deborah E. Ward, Dale W. Griffin and Lindsey Hicks in Social Psychological and Personality Science
Footnotes
Handling Editor: Veronika Job.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received a grant from the National Science Foundation (BCS-2028461) to support data collection for Sample 4.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.