
Abstract
Background
Iron deficiency is the most common nutritional deficiency in infants, with varying prevalence across countries.
Objective
The objectives of this study were firstly to compare hematological, biochemical, and dietary parameters between iron-deficient (ID) and non-iron-deficient (NID) infants; and secondly to identify dietary components associated with iron deficiency.
Methods
Infants (n = 130, Girls/Boys 59/71) aged 18 to 24 months, were recruited from pediatric center in Oran. Fresh blood count, plasma ferritin, and soluble receptors of transferrin (RsTf) were measured. Dietary consumption by the 24-h recall followed by 3 days record was evaluated.
Results
Among the 130 infants recruited, 71 had iron deficiency, representing a prevalence of 54.6%. Hemoglobin, mean corpuscular volume (MCV), and ferritin levels lowered in ID compared to NID group (p < 0.05), while RsTf levels increased by 10%, confirming iron-deficient erythropoiesis. Despite comparable total energy and macronutrient intakes between the both groups, animal proteins consumption was 1.41-fold lower and vegetable proteins was 1.34-fold higher in ID group compared to NID (p < 0.001). Micronutrient analysis revealed significant low dietary iron, retinol (vitamin A), zinc, and vitamin B1 in ID group (p < 0.05). Notably, growth milk consumption was reduced by 64% in ID infants suggesting a potential link between fortified milk intake and iron status.
Conclusion
This study highlights key differences in hematological, biochemical, and dietary parameters between ID and NID groups, thus underscoring the importance of dietary quality, particularly bioavailable iron, and animal protein sources, to prevent iron deficiency, and to reinforce the role of fortified foods in pediatric nutrition.
Introduction
Iron is an essential micronutrient that plays a critical role in numerous physiological processes, including the synthesis of hemoglobin, myoglobin, cytochrome enzymes, and other key proteins and enzymes. However, certain populations, such as newborns, children, adolescents, and pregnant women, exhibit elevated dietary iron requirements, rendering them more vulnerable to iron deficiency which represents the most prevalent micronutrient deficiency globally, affecting an estimated 2 billion individuals.1,2
This deficiency may result from inadequate dietary iron intake or impaired gastrointestinal absorption. Iron absorption depends on body's iron status, rate of erythropoiesis, amount and form of iron in diet, heme iron (Fe2+) or inorganic iron (Fe3+), and presence of absorption enhancers and inhibitors in diet.3–5 Young infants seem to have a lower capacity to regulate iron homeostasis.6,7
Consequently, a prolonged deficit in bioavailable iron, coupled with depleted iron stores, progresses to iron deficiency, and may ultimately lead to iron deficiency anemia. 8
The etiology of iron deficiency primarily involves three pathways: inadequate dietary intake (the predominant etiology), elevated physiological iron demands, and blood loss. Among these, insufficient dietary intake remains the leading cause of iron deficiency in children worldwide. Epidemiological studies demonstrate higher incidence among infants, preschool-aged children, and female adolescents.9,10
The first 1000 days arguably represents the period of lifewith the greatest risk of iron deficiency, can result in long-lasting, irreversible disorder in cognition, motor function and behavior. 11 Moreover, infants and toddlers have high nutritional requirements relative to body size but consume small amounts of food, and therefore need nutrient-dense complementary foods. 12
Dietary iron intake (DII) determination is considered as the only available marker to assess the risk of iron deficiency. The DII is estimated from food consumption surveys.6–13 The influence of DII on body iron status is modulated by iron bioavailability, which refers to the fraction of ingested iron that is effectively absorbed. Iron absorption is governed by three key factors: the individual's iron status (with enhanced absorption during deficiency), the chemical form of dietary iron (heme vs non-heme), and the concurrent presence of dietary enhancers or inhibitors of iron uptake.4,14,13 Bioavailability assessment must consider meal-level interactions between enhancers (ascorbic acid, heme iron, fermented vegetables), and inhibitors (phytates, polyphenols, but also calcium, zinc, copper).14,13 Thus, iron content in diet must then be taken into account by integrating these concepts.
For that, iron deficiency persists as a significant global public health challenge,
15
with an estimated worldwide prevalence of 17.95% (95% CI: 13.49–22.41). Up to 43% of all children younger than 5 years old, and approximately 60% in Africa are affected.
16
As the leading cause of anemia, iron deficiency contributes substantially to the burden of iron deficiency anemia
17
predominantly affecting low and middle income countries,
18
Significant burden of dietary iron deficiency is noticed across the Middle East and North Africa (MENA) region, with pronounced disparities by age, sex, and socioeconomic status. 1 However, few studies have focused on iron deficiency in Algeria, apart from some local studies.
The objectives of this study were to compare hematological, biochemical, and dietary parameters between iron-deficient (ID) and non-iron-deficient (NID) infants; and to identify dietary components associated with iron deficiency.
Population and methods
Study design and ethical considerations
In this analytical, cross-sectional, and observational study, 200 infants were recruited from January 18th 2021 to May 25th 2022, at three pediatric centers in Oran city (West Algeria). Mothers were interviewed during the pediatric consultation or for the vaccination of their infants.
Eligibility criteria were defined as follows: inclusion criteria were infants aged 18 to 24 months, term birth 37 weeks gestational age, singletons and birth weight ≥2500 g. Exclusion criteria concerned all infants with one of the following antecedents, born prematurely before 37 weeks of gestational age, with a small for gestation age, from multiple pregnancies, transfused, having received (or receiving) medicinal iron supplementation, major surgical intervention, severe infection, family history of hemoglobinopathy or chronic pathology.
This study was conducted, in accordance with the guidelines of the Helsinki Declaration, in the clinical and metabolic nutrition laboratory, and the pediatric department, in accordance with, the ethical guidelines and the laws governing the conduct of research in the country. This study was approved by the Ethics and Professional Conduct Committee of Oran1 Ahmed Ben Bella University (Ministerial decree N°991, December 10, 2020).
Of a total of 160 infants who met the inclusion criteria, only 130 (Girls/Boys 59/71) were included. Refusal was mostly due to mother's lack of interest or lack of time. Written informed consent was obtained from mothers prior to participation in the study. A specific identification card has been established for each infant with a code, to ensure confidentiality.
Characteristics of infants
A first questionnaire focused on the characteristics of infants, such as birth weight, type of birth (natural or cesarean section), date of birth, place of birth, sex, duration of sleep per night.
Anthropometric parameters were carried out according to WHO 19 standard method. Weight and height were measured using a device (ALPEC PESAGE) which is both a slider scale and a gauge calibrated to 0.5 cm. The cranial perimeter was measured by a tape measure calibrated in millimeters. Body mass index (BMI) was calculated as weight (kg)/height (m2) for each infant. Weight status was defined using IOTF (International Obesity Task Force) gender, and age-related cut-offs for BMI. 20 Children were classified into 4 groups: Normal-weight (NW), Overweight (OW), Obese (O), and Thin (T).
Biochemical analysis
Blood samples
Six mL of blood were taken from the vein of the elbow bend and were divided into 3 tubes: 2 mL on a EDTA tube for the realization of the blood count that was determined the same day. This same sample was recovered to undergo double centrifugation at 3000 rpm/min for 15 min. The resulting plasma was frozen at −18°C, for subsequent analyses.
Determination of blood count
Blood count was performed on fresh blood using a meter (Automat Actus Abacus) at the Laboratory of Biochemistry of the health center.
Determination of ferritinemia
The ferritin content was carried out by a tubidimetric method using a kit (Turbilatex ferritin, Spain).
Qualitative determination of C-reactive protein
Qualitative determination of CRP was done by agglutination method using a kit (PRC-Latex, Sprinreact, S.A.U-Ctra. Santa Coloma, 7-E-176SANTESTEVE DE BAS – Girona, Spain).
Determination of soluble transferrin receptors
The soluble transferrin receptors (RsTf) were determined by immunoenzymatic techniques (ELISA, immunoturbidimetry). Monoclonal antibodies specific to RsTf are used to capture and quantify their concentration in serum or plasma. These analyses were performed by CERBA laboratories.
Food consumption assessment
The methods of a 24-h recall followed by a 3-day recording were used. The infant mother was asked to report all the food, solid or liquid and all the drinks ingested by her child during the last 24 h, then had to note the 3 days following the food consumption of her child. The time and place of each food intake, the quantity proposed and the quantity actually consumed at each meal by the infant, the exact name of the product, with its brand name if applicable were noted. The method of preparation and detailed recipe for all home-prepared foods were specified.
The amount ingested of each food was specified using a manual-photo, to determine the amount actually consumed.
For breastfed children, WHO estimates of the mean quantity of breastmilk produced per day for developing countries21,22 were attributed to each child according to their age. USDA values 23 were used for breastmilk composition. Information on whether the participants had received micronutrient supplements was also collected. For each infant, total energy intake (TEI), macronutrients (proteins, fats and carbohydrates), fibre and micronutrients (vitamins and mineral salts) intakes were estimated using the Computerized Nutrition Survey Management software. 24
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics version 22. All values were expressed as mean ± SD. The Shapiro-Wilk test was used to verify whether variable distribution was normal. The student-t test was used to compare the means of different variables between ID and NID groups, and the Chi-square test was used to compare qualitative variables (expressed as percentages). A significance threshold of p < 0.05 was applied for all tests. Correlations between variables were calculated using Pearson's coefficient.
Results
Characteristics of the studied population
Iron deficiency was defined according to these two models: 22.1% of infants met model criteria of ferritin <12 µg/L in the absence of inflammation, 25 and 72.6% of infants with low ferritin or high RsTf.
Table 1 presents the characteristics of the both groups, with iron deficiency (ID), and without iron deficiency (NID). No significant differences were observed for sex ratio, age, birth weight, BMI, type of birth, and cranial parameter between the both groups. Anthropometric status of infants, according to IOTF classification, did not show any significant difference in distribution between the two groups. However, more than half of infants had a normal weight status (51% in ID vs 56% in NID group). Additionally, 13–14% of infants were underweight, while overweight accounted for 18 and 20% in the ID and NID groups respectively. Obesity was observed in 11% of ID group compared to 15% of NID group.
Characteristics of population.
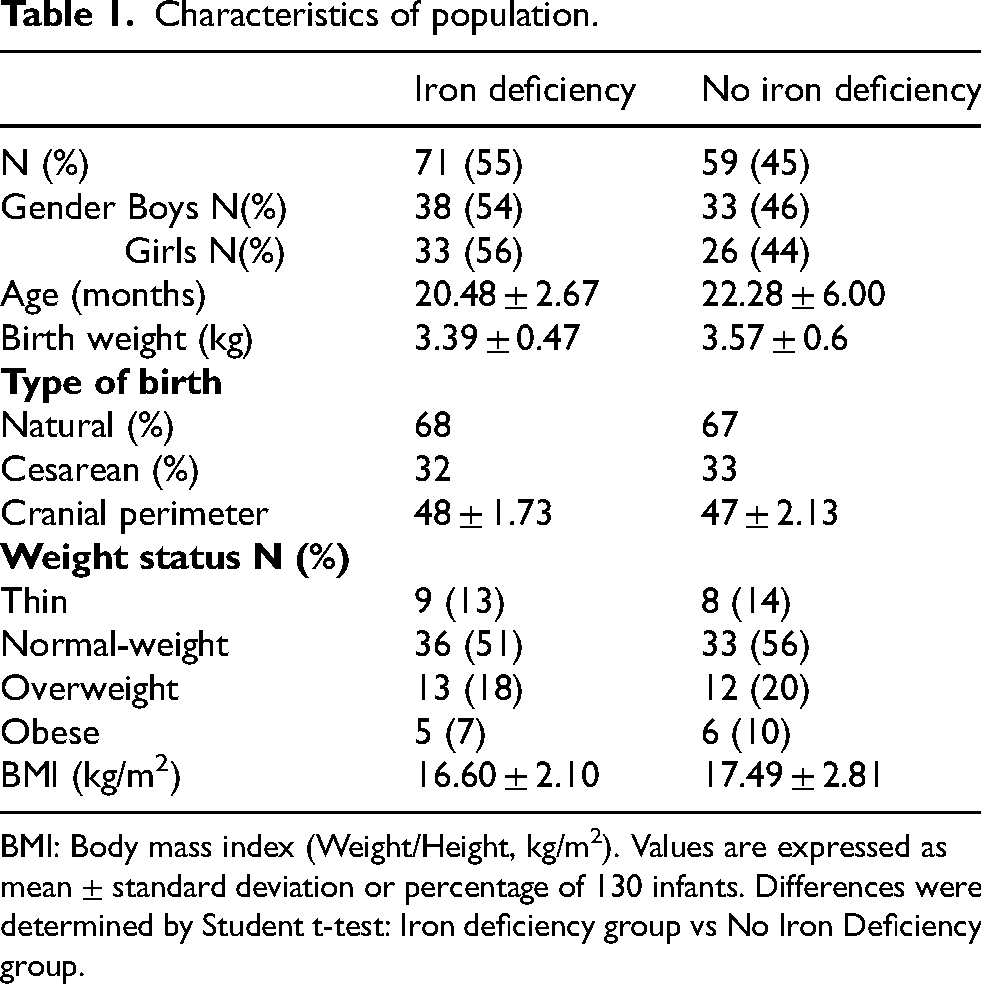
BMI: Body mass index (Weight/Height, kg/m2). Values are expressed as mean ± standard deviation or percentage of 130 infants. Differences were determined by Student t-test: Iron deficiency group vs No Iron Deficiency group.
Iron deficiency biomarkers
Table 2 shows serum markers of iron deficiency. In ID infants compared to NID group, decreased values were observed for hemoglobin (p < 0.05), MCV (p < 0.01), and ferritin (p < 0.05) (−5%,−6%, and-14%, respectively). Whereas, soluble transferrin receptor levels were enhanced by 10% in ID compared to NID group. CRP analysis was performed to rule out any inflammation.
Iron deficiency biomarkers.
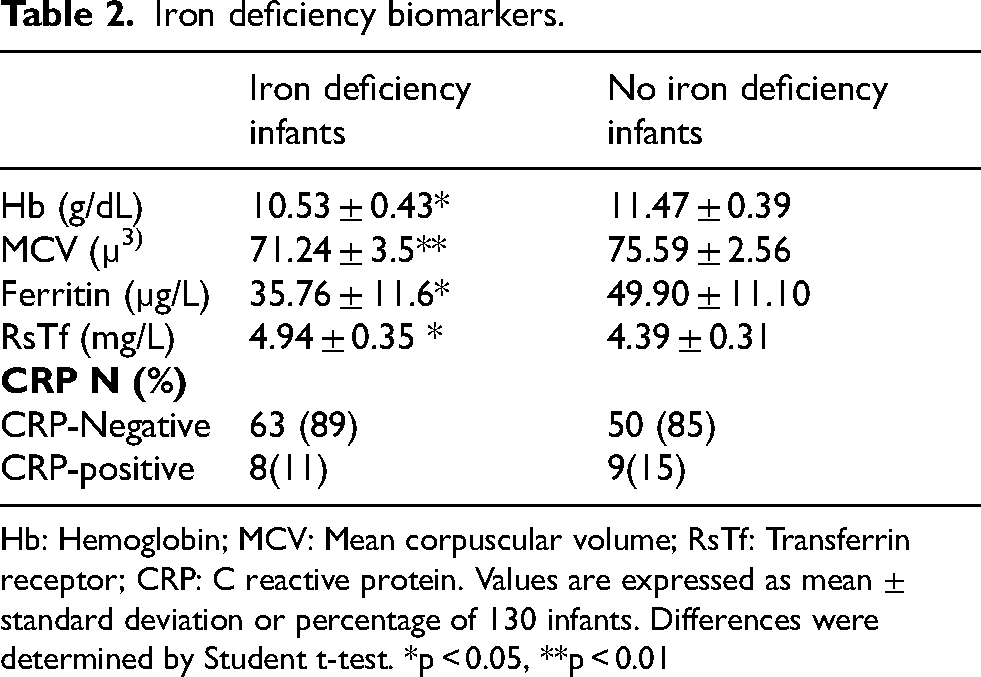
Hb: Hemoglobin; MCV: Mean corpuscular volume; RsTf: Transferrin receptor; CRP: C reactive protein. Values are expressed as mean ± standard deviation or percentage of 130 infants. Differences were determined by Student t-test. *p < 0.05, **p < 0.01
Dietary consumption
Qualitative distribution of total energy intake
Qualitative distribution of total energy intake (TEI) in ID group compared to NID group is presented in Table 3. No significant differences were observed in TEI, total proteins, carbohydrates, total lipids, or cholesterol, whether quantitatively or qualitatively. However, in ID group compared to NID group, qualitative distribution of proteins revealed that animal proteins were 1.41-fold lower, whereas, vegetable proteins intake was 1.34-fold higher (p < 0.001).
Qualitative distribution of daily energy intake.

SFAs: Saturated fatty acids; MUFAs: Monounsaturated fatty acids; PUFAs: Polyunsaturated fatty acids. Values are expressed as mean ± standard deviation or percentage of 130 infants. Differences were determined by Student t-test. ***p < 0.001
Dietary micronutrients related to iron deficiency
Table 4 presents dietary micronutrients related to iron deficiency. It was observed that dietary iron was lower 1.35-fold (p < 0.01), retinol (vitamin (Vit.) A) 1.38-fold (p < 0.01), zinc 1.15-fold (p < 0.05), and Vit. B1 1.23-fold (p < 0.05), in ID group than in NID group. However, no significant difference was found in Vit. D, calcium, Vit. E, Vit. B2, B3, B6, and B12 intakes in the both groups.
Micronutients linked to iron deficiency.
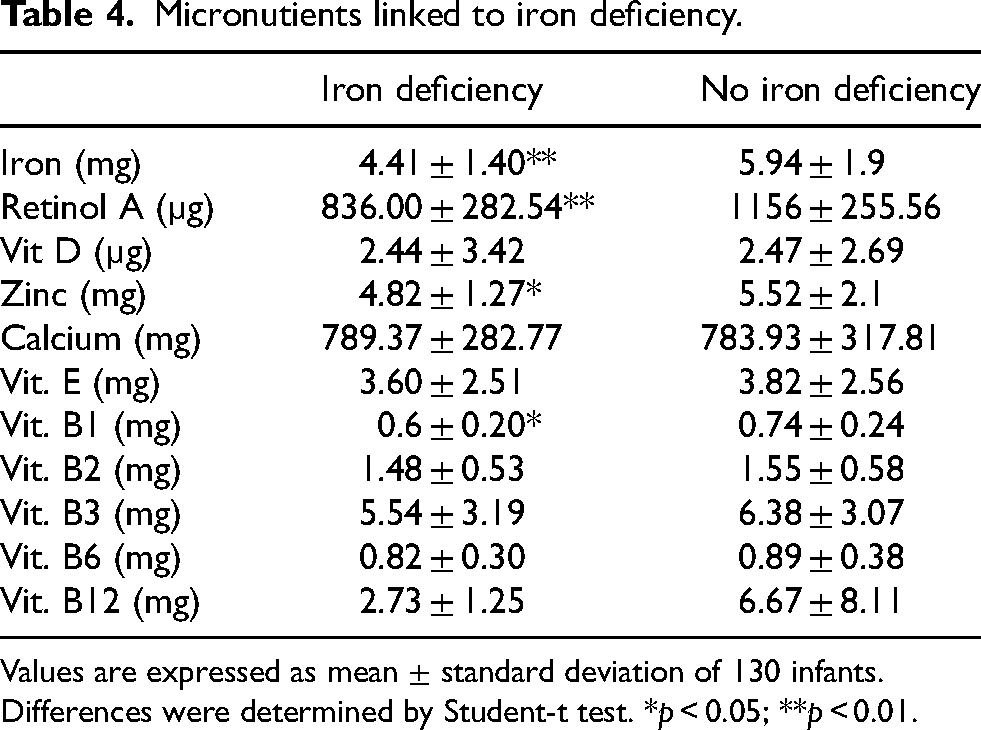
Values are expressed as mean ± standard deviation of 130 infants. Differences were determined by Student-t test. *p < 0.05; **p < 0.01.
Food groups consumption and dietary iron intake
Table 5 presents food groups consumption and iron-rich foods. The most consumed food group, in both ID and NID infants, was milk and dairy products, with a significant difference observed between ID and NID group (422.88 ± 80.30 g vs 658.01 ± 90.72 g, p < 0.05). To determine which type of milk contributed most to this difference, specific milk consumption was analyzed. No significant variation was found for cow's milk or breast milk. However, young child formula intake in ID infants was 64% lower than in NID group. No significant differences were observed in other food groups consumed, including cereals and starchy foods, fruits and vegetables, sugars and sweet products, and fats and oils.
Consumption of food groups, and iron rich foods.

Values are expressed as mean ± standard deviation of 130 infants. Differences were determined by Student-t test. *p < 0.05; **p < 0.01.
Correlations between iron deficiency and biochemical and nutritional parameters
Negative relationships were noted between iron deficiency and Hb, ferritin, MCV, animal proteins, iron, meat, and growth milk. Inversely, strong correlations were found between iron deficiency and RsTf (Table 6).
Correlation between iron deficiency and biological and nutritional parameters.

Hb: Hemoglobine; RsTf : Transferrin receptor; CRP : C reactive protein; MCV : Mean corpuscular volume. Pearson's correlation coefficients between iron deficiency and biological and nutritional parameters studied. NS: Not Significant.
Discussion
The objectives of this study were firstly to compare hematological, biochemical, and dietary parameters between iron-deficient (ID) and non-iron-deficient (NID) infants aged 18–24 months; and secondly to identify dietary components associated with iron deficiency.
There are few studies on infants iron deficiency in Algeria, apart from some local studies, such as that of Smahi et al.,, 26 who found a prevalence of 53%, and Bouhajila, 27 who reported a prevalence of 51.9% in infants aged 7–12 months, and in children aged 13–60 months, with a prevalence of 42.3%. Our study showed that more half of infants were affected by iron deficiency. This is consistent with research conducted in the Middle East and North Africa (MENA) region, which found a very high prevalence of iron deficiency among children under the age of five years 1
Similar to findings of Nepesov & Say, 28 who found a prevalence of overweight of 55% in infants aged 6 to 12 months, our results revealed the coexistence of underweight and overweight/obesity in our population. Comparable results have been reported among older pediatric populations in Algeria. 29
A decrease in hemoglobin levels, and in mean corpuscular volume was observed in infants with iron deficiency. Previously, similar findings have been reported in other infant populations, such as in the study conducted in Nova Scotia, 30 and that realized in Turkey. 28
Iron deficiency in infants leads to decreased ferritin levels, indicating reduced iron stores.31,32 Our results are consistent with these findings, which showed a significantly lower ferritin level in ID group versus in NID group.
Infants with iron deficiency exhibited altered transferrin receptor dynamics, particularly the soluble transferrin receptor which serves as a reliable marker for assessing iron status. Data indicate that RsTf levels are less influenced by inflammation compared to traditional markers, making it a valuable tool in diagnosing ID in pediatric populations.33,15 Our study showed the same results.
The laboratory diagnosis of iron deficiency in infants should include serum ferritin and CRP levels to exclude the influence of infection. This approach allows for accurate detection of iron deficiency while accounting for potential confounding factors such as concurrent inflammatory conditions. 34 CRP was negative in most infants in both ID and NID groups, thereby preventing misclassification of iron status.
Nutritional deficiency due to a diet low in iron is the primary cause of ID. 28 Indeed, diet is a key determinant influencing iron status, 35 in particular, animal-derived foods, which serve as a valuable source of high-quality protein and heme iron, a form with superior bioavailability compared to non-heme iron. Therefore, their inclusion in diet is essential for optimizing iron status. 36
Our study revealed a significant decrease in animal proteins intake at the expense of plant-based proteins, in ID group compared to NID infants. These findings align with those reported in another study, which found that children consuming fewer animal proteins often exhibit lower iron levels due to the absence of heme iron, which has higher bioavailability than non-heme iron from plant sources. 37 Similarly, a high intake of plant-based proteins at the expense of animal proteins, as is the case in vegetarian children, is a risk factor for iron deficiency, 34 and plant foods and low in bioavailable iron are the most cause of ID in children. 15
Moreover, a study demonstrated that consumption of animal-source foods before the age of 3 years is associated with improved cranial growth (and thus likely brain development) among undernourished children in rural Nepal. 39 No significant difference in cranial perimeter was observed between the two groups of children.
Iron deficiency is often resulting from decreased dietary iron intake. 15 Likewise, low dietary sources of iron are one of the prevalent causes of ID in children. 38 The same result was found in our study, as dietary iron was significantly reduced in ID group. It should be noted that none of the infants had received or were receiving iron supplementation. In the same way, low levels of retinol were found. Furthermore, anemia and iron deficiency were associated with low levels of serum retinol in children, and a positive correlation was found between serum retinol and serum ferritin and hemoglobin levels. 40
Our results are consistent with previous data reporting an association between iron deficiency and zinc deficiency in children. Indeed, as demonstrated in several studies,39,41,42 children with iron deficiency often have lower serum zinc concentrations. Furthermore, phytate, which is present in cereal- and legume-based diets widely consumed in low-income countries, is a potent inhibitor of iron and zinc absorption. 43 Thus, the co-occurrence of iron and zinc deficiencies observed in our population may be partly explained by the consumption of phytate-rich foods, as suggested in the literature. These micronutrient deficiencies during early childhood may also compromise brain growth, as observed in rural Nepalese children,39,44 in whom poor head circumference growth was associated with delayed cognitive development, underscoring the importance of adequate iron and zinc nutrition from the first months of life for optimal neurocognitive development.
The following variables were significantly associated with higher risk of ID: no cow's milk formula consumption, inadequate intake of fats, protein, calcium, Vit. D, iron, zinc, Vit. A, Vit. C, Vit. B6, and Vit. B12. Only cow's milk formula consumption and zinc intake were revealed as the determinant factors of anemia. 45 Nevertheless, the differential effects of various protein sources on growth, along with the underlying mechanisms driving these effects, remain insufficiently characterized. 36
Other risk factors for iron deficiency include low birth weight, periods of rapid growth such as infancy, early introduction of cow's milk and solid foods, breastfeeding beyond six months without iron supplementation, mother's low education level, and low socioeconomic status.10,46 Indeed, iron from human milk exhibits high bioavailability, whereas unmodified cow's milk impairs iron absorption. Iron supplementation is recommended starting at 4–6 months for healthy term infants and earlier for preterm infants, and ascorbic acid enhances iron absorption in term infants and children. 47
Recent evidence demonstrates that gut microbiota modulates iron absorption through several distinct mechanisms. In infants, prebiotic supplementation promotes beneficial bacteria, such as Lactobacillus spp., reduces pathogens and intestinal inflammation, thereby increasing iron absorption by 26% to 60%. 48 In pigs, phytase degrades phytic acid, releasing inositol and showing that enzymatic activity of gut microbiota can overcome barriers to iron absorption. 49 Furthermore, early introduction of cow's milk disrupts gut microbiota and impairs iron absorption, whereas breast milk, rich in natural prebiotics, supports a favorable microbial ecosystem. Thus, whether through prebiotic supplementation, degradation of antinutritional factors, or dietary choices, the gut microbiota emerges as a key modulator of iron absorption. 50
Iron deficiency in infants, particularly in relation to milk consumption, is a significant health concern. Research indicates that iron deficiency can adversely affect growth and cognitive development, requiring careful dietary management. Breast milk is shown to provide highly bioavailable iron, while cow's milk can inhibit iron absorption, highlighting the importance of appropriate feeding practices during infancy. 47
Our findings indicated that breastmilk was the most consumed milk in the both groups. These results are consistent with those of another study conducted in Algeria, which showed that breastmilk (exclusive breastfeeding or partial breastfeeding) remained the predominant milk source for infants aged 0–12 months. However, this trend declined after 12 months, with cow's milk gradually replacing breastmilk, showing that infants exhibited dietary iron deficiency breastmilk. 51 Breastfeeding protects against iron deficiency due to its high iron bioavailability in breastmilk. However, after the first months, increased iron demand surpasses breast milk's supply, requiring the introduction of iron-rich foods around 4–6 months to prevent deficiency. 52 Indeed, infants up to 6 months of age with ID who are not breastfed should receive iron-fortified formula, and infants over 6 months of age who are not breastfed should receive iron-fortified follow-on formulas. 53 Growth formulas specifically designed for children in this age group provide additional nutrients that may not always be met through daily food. 54
In our study, consumption of growth milk was significantly lower in ID group compared to NID group. These findings are consistent with another study demonstrating that infants consuming growing-up milk did not exhibit iron deficiency, 28 and infant formulas could help optimize the intake of certain key nutrients (iron) in this population. 51
Animal flesh foods are rich in bioavailable iron but infrequently consumed by young children. 55 Combined animal proteins and growth milk can help children to meet their daily nutritional needs required for optimal growth. These both sources of nutritional complement each other in providing a balanced intake, and preventing malnutrition. 54
Addressing iron deficiency requires a multifaceted approach combining nutritional interventions, education, and community engagement. Evidence shows that iron supplementation, fortified foods (e.g., infant cereals), and dietary diversification improve effectively iron status, though adherence depends on structured education and community involvement. 18 Cost constraints in low-resource settings may favor biofortification, while health policies should tailor mass or targeted strategies to local epidemiological and socioeconomic contexts. Given the persistent global burden of iron deficiency, particularly among children under five years, scaling up these interventions remains an urgent public health priority. 6
Future research should expand this study by including a larger cohort of infants across multiple municipalities, aiming for a comprehensive epidemiological assessment. Additionally, further parameters analysis is necessary to screen for potential deficiencies in other vitamins and minerals, including parameters that monitor growth rate over time and that detect socio-economic characteristics of the child's living context, such as the mother's educational level. Targeted nutritional education for prospective mothers could help prevent malnutrition both preconceptionally, and during pregnancy while also improving child health outcomes.
Conclusion
This study reveals that iron deficiency affects more than half of infants, and the coexistence of underweight and overweight/obesity. It highlights key differences in hematological, biochemical, and dietary parameters between ID and NID groups. Hemoglobin, MCV, and ferritin levels are significantly lower in ID group, while sTfR levels are higher. Although dietary intake shows comparable total energy and macronutrient intake between the both groups, animal protein consumption remains significantly lower in ID group, leading to reduced dietary iron, retinol, zinc, and Vit. B1 levels. Growth milk formula consumption is very low in ID group, suggesting a potential link between fortified milk intake and iron status. These findings underscore the importance of dietary quality, particularly bioavailable iron and animal protein sources, in preventing iron deficiency, while reinforcing the role of fortified foods in pediatric nutrition. Parents often instill poor dietary habits in their infants from an early age, leading to micronutrient deficiencies, particularly iron, iodine, and Vit. A. Promoting nutritional education for expectant mothers appears essential to ensure adequate feeding practices from birth, safeguarding infants long-term health.
Footnotes
Acknowledgments
The authors would like to thank the Master students (H. Saidani, A. Souali, S. Benadouda, A. Hadj Kadi, A. Hamous), and the health personnel of the pediatric departments for their assistance in collecting data, as well as, all the mothers and their infants involved for their contribution.
Authors contributions
The authors contribution to the paper was as follows: Study conception and design: M.B., K.B.N., M.C.E.S., I.B. Data collection: H.G.B., N.Dj. Analysis and interpretation of results: H.G.B., N.D., M.B., K.B.N. Statistical analysis: H.G.B., N.D., K.B.N. Draft manuscript preparation: H.G.B., M.B., K.B.N., I.B. All authors reviewed and approved the final version of the manuscript.
Funding
A part of this study was funded by the General Directory of Scientific Research and Technology Development (DGRS-DT) of the Ministry of Higher Education and Scientific Research. Another part was funded by Danone Nutricia Research in Algeria.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.