
Abstract
Hard Metal Lung Disease (HMLD) is a form of Interstitial Lung Disease that occurs due to occupational exposure to hard metals. It is clinically a hypersensitivity pneumonitis with typical radiological and histopathological findings including giant cell interstitial pneumonitis. Very rarely, it occurs due to non-occupational exposure and here we present the case of a 49 years old woman who presented with progressive breathlessness and was found to have typical features on histopathology of HMLD.
Introduction
Hard Metal Lung Disease (HMLD) is a form of Interstitial Lung Disease (ILD) that occurs due to occupational exposure to sintered tungsten carbide and cobalt which are widely used in industry because they are extremely ‘hard’ and resistant to corrosion. 1 Occasionally, exposure to other metals including titanium, chromium, tantalum, chromium, or nickel may cause HMLD. 2 Clinically, HMLD is a hypersensitivity pneumonitis, with both subacute presentations as well as possible progression to pulmonary fibrosis in the event of sustained exposure. 2
HMLD can also rarely occur as a result of non-occupational exposure, especially as a result of living in close proximity to industries involving the offending metals or due to exposure through other means such as handling contaminated clothes. 1 Here we present the case of a 49 years old woman who was a homemaker and had no occupational exposure, who presented with gradually worsening breathlessness and was found to have HMLD on radiology and histopathology.
Case report
A 49 year old woman who was previously fit and well presented to the respiratory medicine clinic with gradual onset, worsening breathlessness for the past 10 months. At the time of presentation, she had grade 2 MMRC breathlessness with an associated dry cough. She was a homemaker who lived with her husband who was well. There were no respiratory diseases in her immediate family. She did not keep any pets. She was a non-smoker and was not on any regular medication.
On physical examination, general examination was unremarkable with no clubbing. Respiratory examination showed bilateral fine crackles with other systems being normal. Blood investigations showed a normal complete blood count, liver functions, and renal functions, and she had a normal ECG. A chest radiograph showed bilateral reticulonodular opacity. An HRCT thorax showed bilateral lung peri-lymphatic nodules with interlobular septal thickening and fibrosis along with enlarged mediastinal lymph nodes (Figure 1). HRCT thorax showing bilateral lung peri-lymphatic nodules with interlobular septal thickening and fibrosis.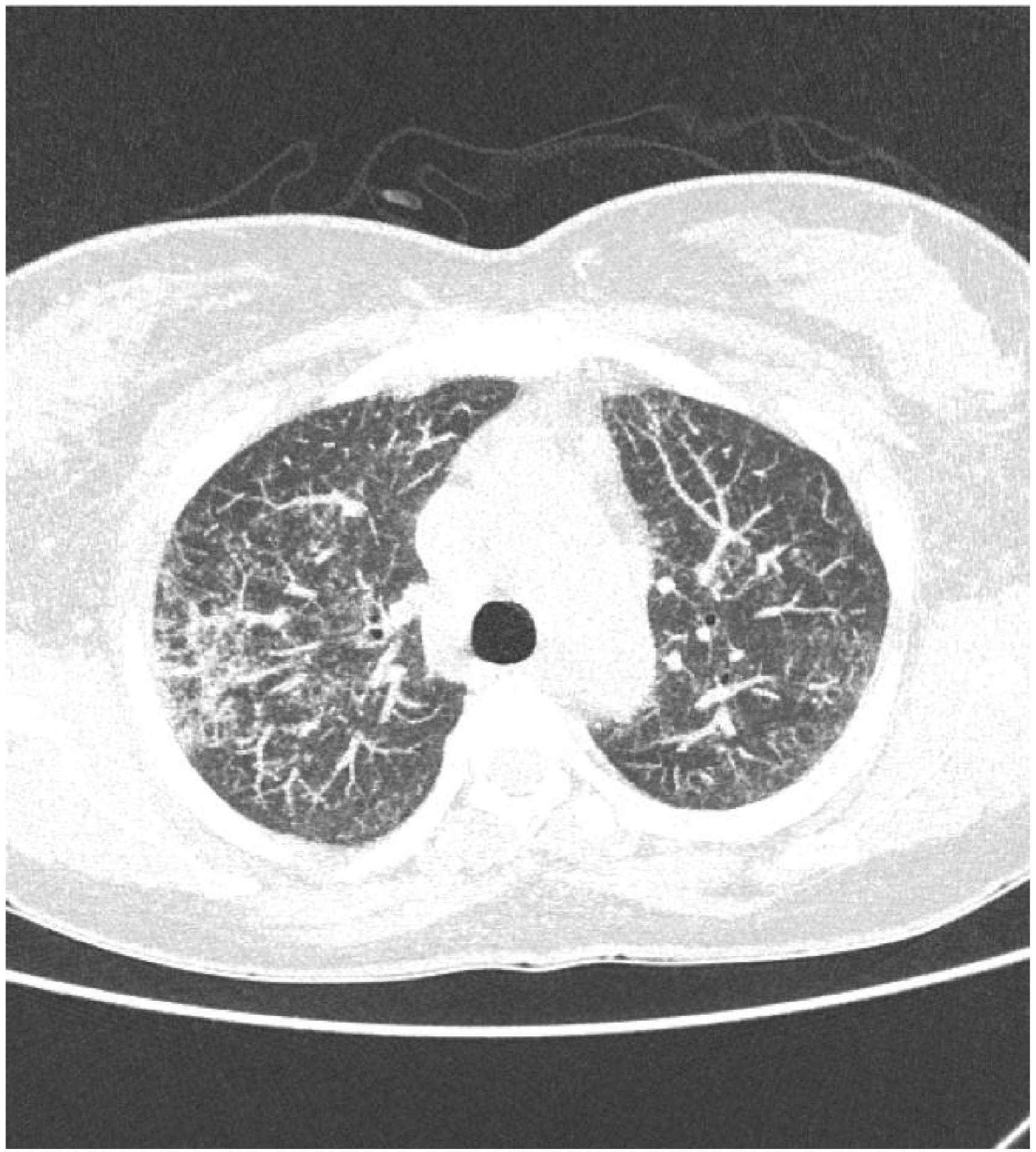
A differential diagnosis of an atypical infection including tuberculosis (TB) versus pulmonary sarcoidosis was considered. Serum ACE, serum and urinary calcium levels, ANA, and Rheumatoid factor were negative. She had a negative Mantoux test. Trans-thoracic echocardiography was unremarkable. A pulmonary function test (PFT) showed mild restriction. Bronchoscopy and BAL were performed with BAL fluid being negative on bacterial and mycobacterial cultures along with a negative TB GeneXpert. The BAL cytology showed lymphocyte-predominant white cells. A transbronchial needle aspiration (TBNA) did not demonstrate the presence of any granulomas or features of malignancy. A transbronchial forcep lung biopsy (TBLB) showed the presence of giant cells with histiocytes containing crystalline material of variable shape and size with evidence of submucosal fibrosis. Polaroid microscopy showed birefringent variable-shaped yellow-blue crystals suggestive of talc (Figure 2(A),(B),(C)). A second opinion was taken on the histopathology which was reported as giant cell interstitial pneumonia with crystalline material negative for iron suggestive of HMLD. (A): Bronchial mucosa (yellow asterisk) with underlying giant cell reaction (black arrow); (B): Giant cell containing slate grey foreign material (black arrow); (C): Refractile foreign material under polarised light.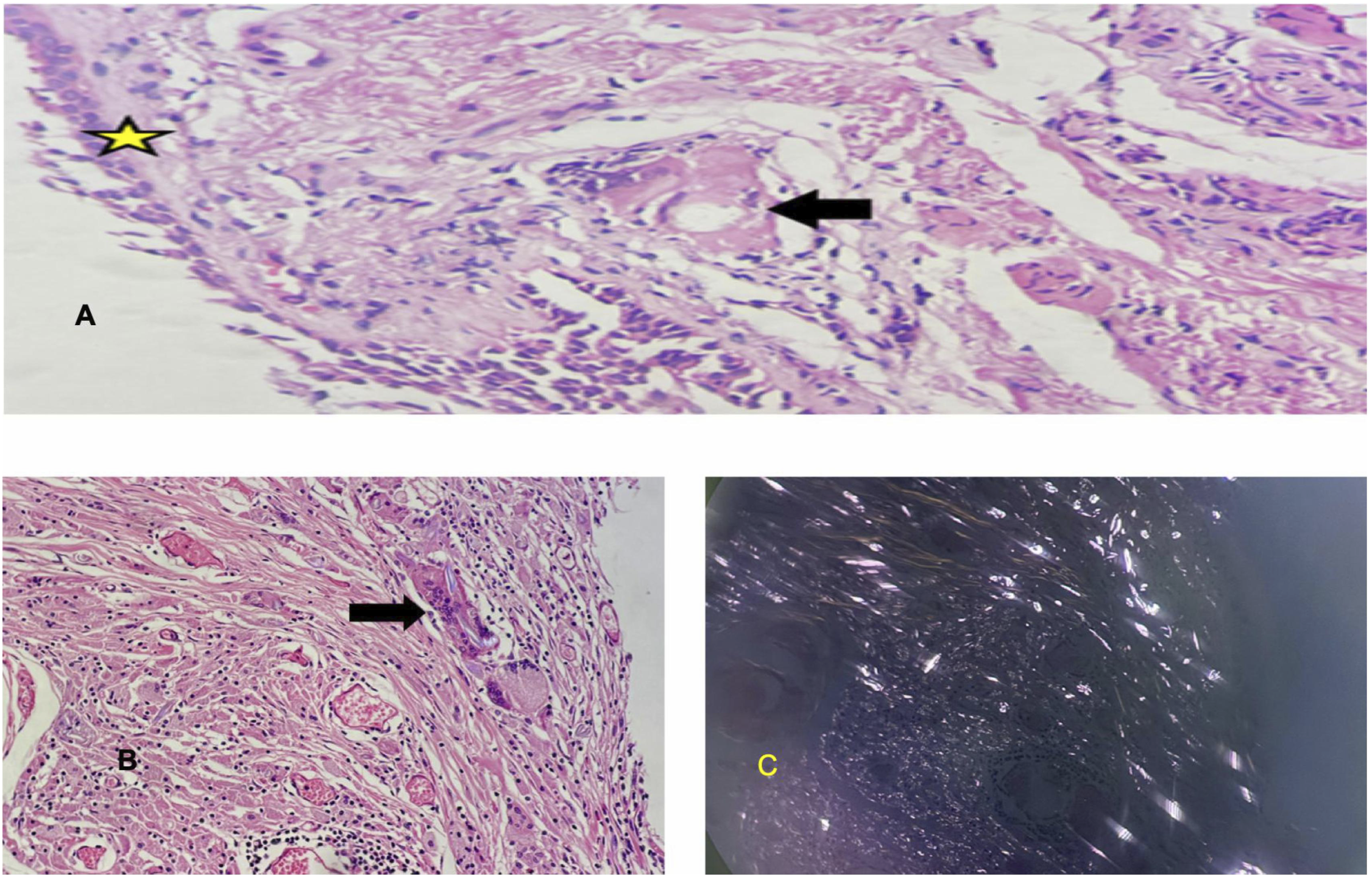
The history of the patient was revisited and it transpired that even though she was a homemaker, she lived in an industrial town in South India called Bellary where her house was situated near various factories and manufacturing units.
The diagnosis was explained to the patient and she was removed from the exposure. She was given pneumococcal and Influenza vaccines. She was then started on a weaning course of oral steroids along with pulmonary rehabilitation.
Review after 3 months showed significant improvement in symptoms with improvement to mMRC grade 1 breathlessness. Repeat PFT showed improvement in the restriction. A repeat HRCT showed regression of the mediastinal lymph nodes and lung nodularity (Figure 3). The need for a permanent change in residence was reinforced. The patient remained stable on follow-up over the next year without requiring any further treatment. However, she re-presented with worsening breathlessness and fibrosis when she revisited her native town which required treatment with nintedanib and another course of oral steroids following which she has remained relatively symptom-free for over a year. regression of the mediastinal lymph nodes and lung nodularity.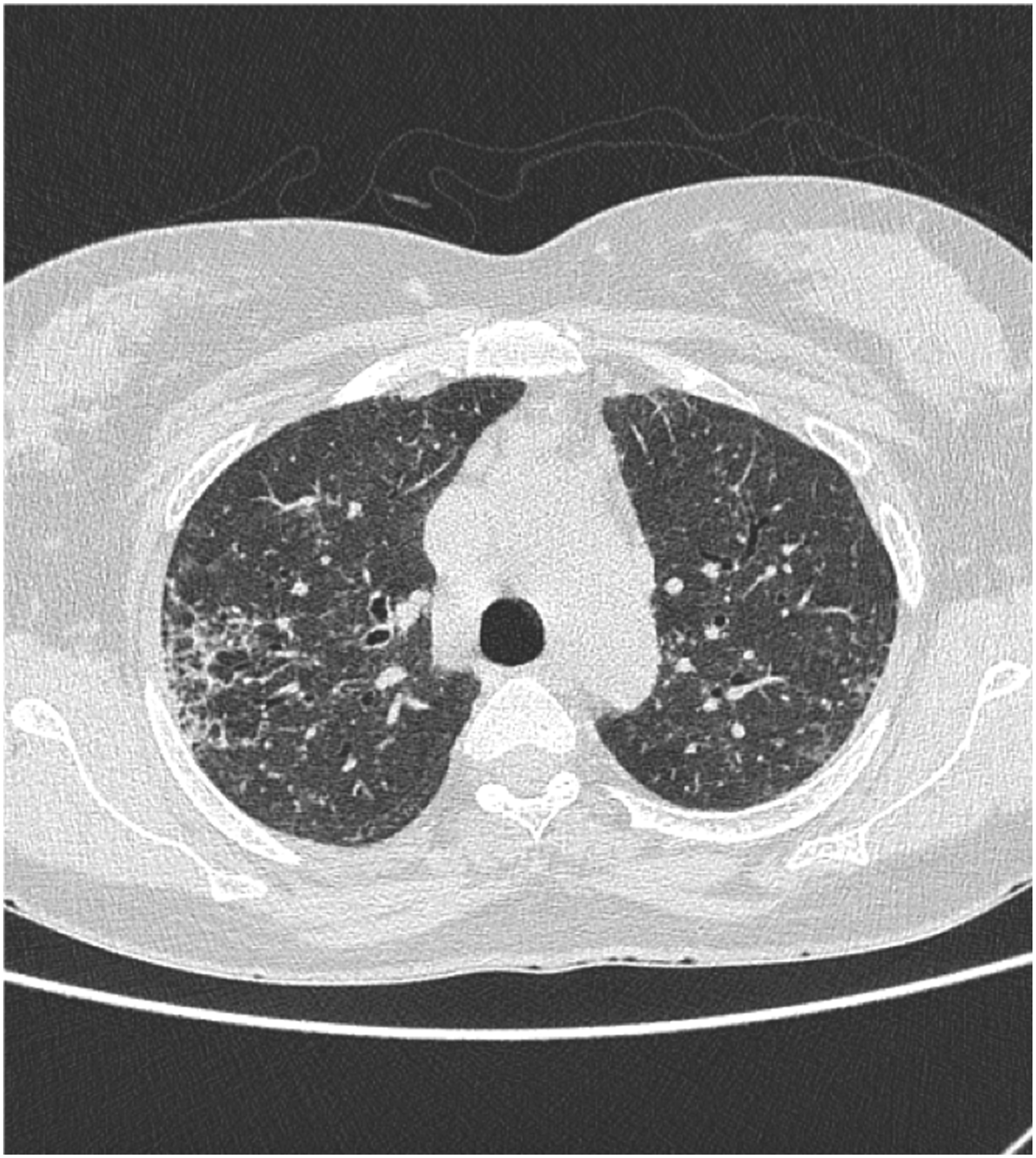
Discussion
Hard Metal Lung Disease (HMLD) is a relatively rare cause of ILD. In a case series of 320 patients with occupational lung diseases in Brazil, only 5 (1.5%) patients were found to have HMLD demonstrating the rarity of the condition even in people with possible sustained occupational exposure. 3 In two large studies among hard metal workers, Meyer-Bisch et al. 4 and Kusaka et al. 5 did not find any cases of HMLD in the 425 and 319 workers who had mean exposure durations of 9 and 14 years respectively. Sprince et al. found 1 patient (< 1%) among 290 hard metal production workers. 6 This highlights the sheer difficulty associated with making the diagnosis of HMLD in the absence of histopathology even in the presence of a compatible occupational history. In our patient, the lack of this history made the diagnosis of HMLD even more improbable with the need for a second histopathological opinion given the surprising findings.
HMLD includes Giant cell interstitial pneumonitis (GIP) and pulmonary fibrosis. Presence of bizzare, cannibalistic multinucleated giant cells is a typical pathological finding for HMLD and is also thought to be pathognomonic even though cases without GIP have been described.2,7 This, coupled with typical radiological features which include ground-glass changes, irregular linear opacities in the lung fields, consolidation, lung nodules, advanced disease, distortion of the parenchyma, traction bronchiectasis as well as honeycomb patterns, peri-lymphatic nodules and peri-bronchovascular consolidation have all been reported in HMLD.2,8 The diagnosis is made easier in the presence of a compatible occupational history but as our case highlights, even in the absence of such a history, the radiological and histopathological findings should lead to the diagnosis.
Our patient hailed from the industrial town of Bellary, a known hub of granite mines and factories. This was not considered a red flag initially when the history was taken. Tungsten is a component commonly found in granite mines and is one of the components of Hard metals.
In retrospect, an unexplained ILD from a resident of an industrial town should prompt the possibility of HMLD in addition to other conditions such as silicosis or pneumoconiosis. Bellary has in fact been featured in mainstream media recently as having a surge in respiratory illnesses which has been attributed to the rapid rise in industrialization of the area. 9 Our case should highlight the need for a very careful history of living conditions in patients presenting with an ILD even if no occupational or readily apparent exposure is found.
Finally with respect to management, avoiding further exposure to hard metals and metal dust is paramount in preventing further deterioration of established HMLD. Symptomatic and radiological improvements have been reported when exposure is ceased. 10 Our patient experienced symptomatic relief once the exposure stopped but initially needed steroids. Steroid therapy has been associated with improvement in symptoms in previous cases and case series, albeit anecdotal, in the absence of large-scale trials. 11 Similarly, nintedanib has also been used with successful outcomes in case series. 1 Our patient had an exacerbation of her symptoms and increased fibrosis a year down the line after her returning back to her native place and re exposure and for this, corticosteroid and nintedanib was used following which she improved significantly and remained symptom-free. This could add to the growing evidence that steroids and nintedanib may be useful therapeutic options in HMLD.
Conclusion
In conclusion, HMLD is a rare form of ILD that usually occurs secondary to occupational exposure to various hard metals, most commonly sintered tungsten carbide and cobalt but also titanium, chromium, tantalum, chromium, or nickel. This case is important as it highlights the importance of non occupational exposure in pathogenesis of HMLD. The diagnosis in the absence of typical exposure history relies on radiological and histopathological findings with the presence of GIPs being pathognomonic. Management involves limiting further exposure with a possible role for corticosteroids and anti-fibrotics like nintedanib.
Footnotes
Consent to participate
Written informed consent was obtained from the patient regarding publication of thiscase report.
Author contributions
All authors have contributed in the development, research and writing of this manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All clinical data and relevant information generated or analyzed during this study are includedwithin this case report. Any other datasets needed can be made availaible on request fromcorresponding author.