
Abstract
Background:
The causes of cardiovascular disease are complex, with hyperlipidemia being a major factor in its development. The connection between peptic ulcer disease (PUD) and hyperlipidemia is unclear, and there have been no thorough studies on the effect of anti-PUD medications on the risk of hyperlipidemia, particularly in Asian populations. This study aimed to explore the relationship among PUD, anti-PUD medications, and the risk of developing hyperlipidemia.
Objectives:
Utilizing a population-based cohort study conducted in Taiwan, we investigated the association between PUD, the administration of anti-PUD medications, and the subsequent risk of developing hyperlipidemia.
Design:
Retrospective study.
Methods:
Using data from the Taiwan National Health Insurance Research Database, we conducted a 21-year follow-up study on patients diagnosed with PUD between 2000 and 2021. The Cox proportional hazards regression model was used to analyze the risk of developing hyperlipidemia in relation to PUD and the use of anti-PUD medications.
Results:
According to the multivariable Cox proportional hazards regression analysis, patients with PUD had a higher overall incidence of hyperlipidemia (80.7 vs 53.6 per 1000 person-years) than those without PUD. The adjusted hazard ratio was 1.64 (95% confidence interval = 1.62–1.67). Both men and women, as well as different age groups, showed a higher risk of hyperlipidemia among patients with PUD. Patients with PUD who undergo surgery have a higher risk of developing hyperlipidemia than those who do not. The use of anti-PUD medications, such as H2 receptor antagonists, proton pump inhibitors, antibiotics, prostaglandin analogs, anticholinergics, antacids, and carbenoxolone, but not bismuth salts, was associated with a lower risk of developing hyperlipidemia than non-use.
Conclusion:
Patients with PUD were more likely to develop hyperlipidemia. However, patients receiving anti-PUD medications had a lower incidence of hyperlipidemia.
Introduction
Peptic ulcer disease (PUD) primarily occurs in two forms: gastric ulcers, which develop in the stomach, and duodenal ulcers, which develop in the upper portion of the small intestine. PUD is believed to result from an imbalance between protective factors, such as mucin, bicarbonate, and prostaglandins, and harmful factors, such as Helicobacter pylori (H. pylori), nonsteroidal anti-inflammatory drugs (NSAIDs), and stomach acid, which together weaken the lining of the digestive tract. 1 Common causes of PUD include drug-related ulcers (particularly those caused by NSAIDs), ulcers triggered by stress, conditions such as the Zollinger-Ellison syndrome, and chronic ulcers of the stomach or duodenum. 1 Several factors contribute to the development of ulcers, including lifestyle habits such as smoking, excessive alcohol intake, and consuming spicy foods. 1 Helicobacter pylori, a spiral-shaped bacterium, is notorious for infecting the stomach lining, with approximately 30%–40% of Americans and nearly half of the global population carrying the infection. 2 Helicobacter pylori infection is responsible for 90% of duodenal ulcers and 80% of gastric ulcers 3 and can lead to chronic gastritis, which can alter serum lipid levels and increase the risk of cardiovascular diseases (CVD).4,5 Globally, PUD affects approximately 4% of the population, with about 10% of individuals developing an ulcer at some point in their lives. 1 The prevalence of PUD in Taiwan was 38.74 per 100,000 population in 2001 and 47.89 per 100,000 population in 2019. 6 Recent years have seen a significant decline in prevalence because of improved hygiene, reducing H. pylori infection rates. 7 However, in areas with high rates of antibiotic overuse, H. pylori remains a major contributor to PUD due to increased antibiotic resistance, which complicates eradication efforts. 8 In addition, with an aging population, the use of antiplatelet agents is increasing, contributing to an aging trend in PUD cases. 9
PUD is primarily managed with a variety of medications, including H2 receptor antagonists (H2RAs), proton pump inhibitors (PPIs), regimens aimed at eradicating H. pylori, bismuth salts, prostaglandin analogs, anticholinergics, and antacids. The lifetime prevalence of PUD in the general population is estimated to be approximately 5%–10%, with an annual incidence of 0%–3%. 9 Since the 1950s, the prevalence of PUD has declined significantly, with annual estimates ranging from 0.12% to 1.5%. 9 This decline is reflected in reduced complication rates associated with the disease. 1 In the U.S., hospitalizations related to PUD decreased by 25.8% between 2005 and 2014, and in-hospital mortality decreased by 2.4% during the same period. 1 The age-standardized prevalence rate of PUD dropped from 143.4 in 1990 to 99.4 per 100,000 people in 2019, a trend that mirrors the reductions in mortality and disability-adjusted life-years. 1 However, even as H. pylori infections decline, the increase in PUD cases associated with long-term NSAID use has become more pronounced. Chronic NSAID users develop gastric ulcers in 10%–30% of cases, with 2%–4% experiencing complications. In addition, idiopathic ulcers account for approximately 20% of PUD cases in regions with declining H. pylori infection rates. 1
Globally, CVD is the leading cause of death and is responsible for approximately 17.9 million deaths annually. 10 The growing prevalence of risk factors such as smoking, high blood pressure, diabetes mellitus (DM), and hyperlipidemia continues to drive the increase in CVD cases worldwide. 10 Hyperlipidemia, a disorder of lipid metabolism, remains a significant public health concern. According to data from the National Health and Nutrition Examination Survey (2015–2018), approximately 11.4% of U.S. adults are affected. 11 According to Taiwan’s updated hyperlipidemia guidelines released in 2022, target low-density lipoprotein cholesterol (LDL-C) levels vary based on the individual’s comorbidity risk. 12
Helicobacter pylori infection has been widely associated with alterations in lipid metabolism, including elevated TG levels and reduced high-density lipoprotein cholesterol (HDL-C), both of which are known risk factors for coronary heart disease (CHD).4,13,14 Hashim et al. 15 showed that H. pylori infection led to increases in TC, TG, LDL-C, apolipoprotein B (Apo-B), and lipoprotein (a) and decreased HDL-C and apolipoprotein A1, thus promoting CVD and thrombogenesis. Chen et al. 4 observed that H. pylori-positive individuals experienced higher rates of gastric ulcers, dyslipidemia, and gastric mucosal erosion, indicating that this infection may increase the risk of atherosclerosis and CHD. Zapata-Colindres et al. 3 suggested that H. pylori and NSAID use together hastened PUD development, indicating a synergistic effect. Niemelä et al. 13 acknowledged elevated TG and lower HDL-C in H. pylori-positive individuals and concluded that H. pylori may act as an independent risk factor for CHD. In addition, research on PUD medications and blood lipids has revealed complex interactions. Emerging evidence suggests that acid-suppressive therapies such as PPIs and H2RAs, as well as antibiotics commonly used in PUD management, may exert diverse and sometimes contradictory effects on host metabolism beyond their antisecretory or antimicrobial actions. One well-described consequence of long-term PPIs and H2RAs use is alteration of the gut microbiota; PPIs in particular have been shown to significantly change microbial composition, leading to dysbiosis that may influence systemic metabolic pathways, including those related to glucose and lipid metabolism and inflammation. 16 Cimetidine, an H2RA, showed no significant effect on lipoproteins, although some trends were observed. 17 In addition, chronic acid suppression can reduce gastric acidity, impairing the absorption of micronutrients such as vitamin B12, which has been associated with metabolic changes, including dyslipidemia and insulin resistance in observational and pre-clinical studies. 18 These effects underscore that the net impact of these drugs on metabolic health is complex and context-dependent. While some studies highlight potential protective or neutral effects, other research has raised concerns about metabolic derangements with prolonged use.
Currently, there is a shortage of comprehensive studies examining the impact of PUD and its treatments on hyperlipidemia risk, particularly in Asian populations. To assess the risk of developing hyperlipidemia in patients with PUD with and without the use of anti-PUD medications, we conducted a retrospective study in a Taiwanese population to explore potential correlations.
Methods
Data source
This study was conducted using data from the Longitudinal Generation Tracking Database 2005 (LGTD2005), a subset of the Taiwan National Health Insurance Research Database (NHIRD). The NHIRD is a nationwide administrative database that contains registration files and original claims data for reimbursement under the National Health Insurance (NHI) program, which covers over 99% of Taiwan’s population (approximately 23.7 million individuals). The LGTD2005 consists of all medical claim records from 2,000,000 beneficiaries who were randomly sampled from the 2005 Registry for Beneficiaries of the NHIRD. These individuals were followed longitudinally, with complete claim data available from January 1, 2000, to December 31, 2021. The sampling method ensured that the LGTD2005 cohort is representative of the general Taiwanese population in terms of age, sex, and health care utilization, thereby enhancing the generalizability of the findings. Diagnoses and procedures were recorded according to the International Classification of Diseases, Ninth and Tenth Revision, Clinical Modification (ICD-9-CM and ICD-10-CM), which is the official system for assigning codes to diagnoses and procedures. This study was approved by the Institutional Review Board (IRB) of China Medical University Hospital Research Ethics Committee [CMUH112-REC1-117(CR-2)].
Study population
Patients with PUD (ICD-9-CM: 531-533 and ICD-10-CM: K25-27, K31.82, and K56.6) who were diagnosed between 2000 and 2021 were included in the peptic ulcer cohort. The index date was defined as the first date of PUD diagnosis in the PUD cohort. In contrast, individuals in the non-PUD cohort were chosen on a random basis, and the index date was a random date between 2000 and 2021. We excluded individuals with preexisting hyperlipidemia, those receiving lipid-modifying therapy at baseline, individuals aged <20 years, and those with missing information on age or sex to ensure a well-defined and eligible study population. We applied 1:1 propensity score matching (PSM) and standardized mean differences (SMDs) based on the following variables: age, sex, annual visits, comorbidities, medication history, and index year to construct a non-PUD cohort. This approach was intended to minimize baseline differences and reduce potential confounding effects related to clinical and treatment characteristics. A detailed flow chart (Figure 1) illustrates the participant selection process, including inclusion and exclusion criteria and the final matched cohort structure.
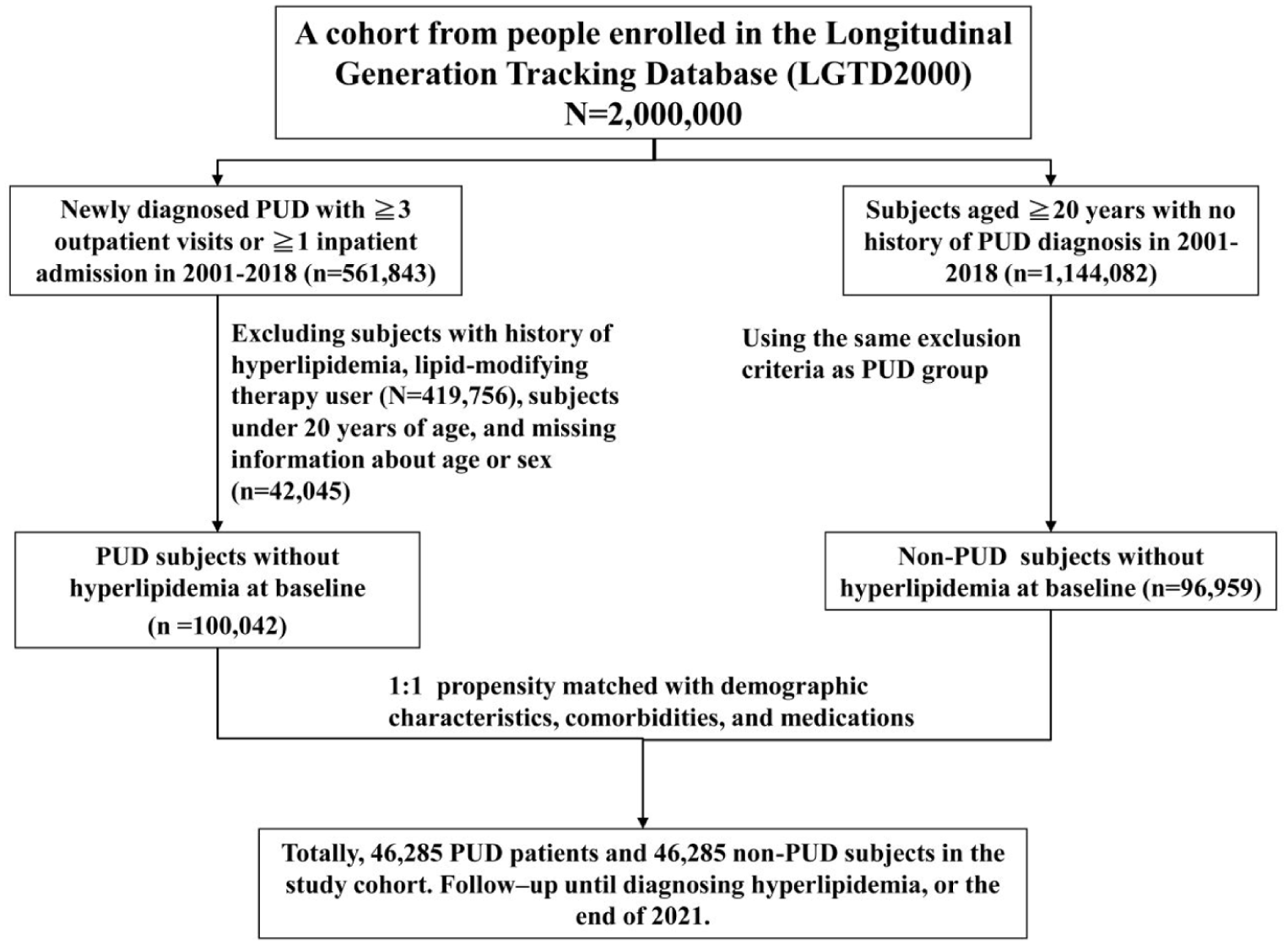
Flow chart showing the selection procedure of study participants.
Main outcome and comorbidities
We defined the outcome definition by requiring both a diagnosis of hyperlipidemia (ICD-9-CM: 272; ICD-10-CM: E78) and the use of lipid-lowering medications (ATC code: C10) between January 1, 2000, and December 31, 2021. The baseline comorbidities included type two diabetes mellitus (T2DM), CHD, hypertension, obesity, sleep disorder, chronic obstructive pulmonary disease (COPD), stroke, and heart failure (the details of ICD codes have been documented in Table S1). These variables were selected based on prior literature identifying them as either confounders or risk factors potentially associated with both PUD and hyperlipidemia.19–22 The anti-PUD medications that are available in Taiwan contain H2RAs (famotidine, cimetidine, nizatidine, ranitidine, and roxatidine), PPIs (esomeprazole, lansoprazole, pantoprazole, omeprazole, rabeprazole, and dexlansoprazole), antibiotics (clarithromycin, metronidazole, tetracycline, and amoxicillin), bismuth salts (bismuth subcitrate), prostaglandin analog (misoprostol), anticholinergics (dicyclomine and pirenzepine), antacids (aluminum hydroxide, magnesium hydroxide, calcium carbonate, and sodium bicarbonate), and other (carbenoxolone, CBX). In addition, we refined our case definition and conducted additional sensitivity analyses focusing on PUD with or without bleeding, identified using validated ICD-9-CM (531.x, 532.x, 533.x, 534.x, 578.x) and ICD-10-CM (K25.x, K26.x, K27.x) bleeding codes, underwent surgery, and those who did not. Comorbidities, use of anti-PUD medications, and surgical interventions (see Table S1 for surgery and bleeding codes for PUD) were identified from the index date to the study endpoints. In this study, a patient was classified as having “use” an anti-PUD medication if they had at least one prescription for that medication after the index date (i.e., the date of PUD diagnosis for the PUD group or the matched index date for the control group) and before the occurrence of the study endpoint (i.e., diagnosis of hyperlipidemia, death, or end of follow-up).
Statistical analysis
The study was conducted using a retrospective cohort design. In this study, we included four different age groups: ⩽34, 35–49, 50–64, and ⩾65 years. The Chi-square test and two-sample t test were used to compare differences in categorical and continuous variables. We further analyzed anti-PUD medication use as a time-dependent covariate by quantifying participants’ anti-PUD medication exposure status for each 1-year interval during follow-up. Cox proportional hazards models with time-dependent exposure covariates were used to estimate hazard ratios (HR) and 95% confidence intervals (CI). Multivariate analysis included age, sex, annual visits, and comorbidities such as T2DM, CHD, hypertension, obesity, sleep disorder, COPD, stroke, and heart failure. We calculated and incorporated E-values for the primary association analysis. Kaplan–Meier (KM) plots were used to compare the cumulative incidence of hyperlipidemia between the two cohorts. To improve the interpretability of these survival curves, we have explicitly added the methods of the log-rank tests used to compare differences in cumulative incidence across medication groups. Thus, KM curves were also generated to visually compare the cumulative incidence of hyperlipidemia across different anti-PUD medication groups. All analyses were performed using the SAS version 9.4 and R software version 4.0 packages.
Results
As shown in Table 1, the PUD and non-PUD cohorts included 46,285 patients and 46,285 participants, respectively. Overall, Table 1 indicates no difference in sex group variables between the two cohorts. The average ages of the PUD and non-PUD cohorts were 49.78 ± 13.1 and 49.8 ± 13.2, respectively. All SMDs for baseline characteristics (sex, age, frequency of medical visits, comorbidities, and medications) were below 0.1, indicating adequate covariate balance between the PUD and non-PUD cohorts after PSM. The top three medications received in both cohorts were H2RAs, PPIs, and antibiotics.
Demographic characteristics, comorbidity, and medication in patients with and without PUD.

Chi-square test.
CHD, coronary heart disease; COPD, chronic obstructive pulmonary disease; H2RAs, H2-receptor antagonists; PPIs, proton pump inhibitors; PUD, peptic ulcer disease; SMD, standardized mean differences; T2DM, type 2 diabetes mellitus.
Table 2 presents a comparison of the incidence and HR of hyperlipidemia stratified by sex, age, and comorbidity between those with and without PUD. Patients with PUD had a higher risk of hyperlipidemia than patients without PUD (aHR = 1.64, 95% CI = 1.62–1.67). Females and males with PUD were 1.57 (95% CI = 1.54–1.61) and 1.70 (95% CI = 1.66–1.74) times, respectively. Patients with PUD aged ⩽34, 35–49, 50–64, and ⩾65 years were 1.40 (95% CI = 1.34–1.47), 1.54 (95% CI = 1.50–1.58), 1.72 (95% CI = 1.67–1.76), and 1.69 (95% CI = 1.62–1.77) times, respectively, more likely to suffer hyperlipidemia compared with same-aged patients without PUD. Patients with PUD with and without comorbidities were 1.67 (95% CI = 1.62–1.72) and 1.60 (95% CI = 1.57–1.63) times, respectively, more likely to contract hyperlipidemia than patients without PUD.
Comparison of incidence and HR of hyperlipidemia stratified by sex, age, and comorbidity between with and without PUD.

Adjusted HR: multivariable analysis including age, sex, annual visits, and comorbidities of T2DM, CHD, hypertension, obesity, sleep disorder, COPD, stroke, and heart failure.
Rate, incidence rate, per 1000 person-years.
Comorbidity: Patients with any one of the comorbidities T2DM, CHD, hypertension, obesity, sleep disorder, COPD, stroke, and heart failure were classified as the comorbidity group.
p < 0.001.
CHD, coronary heart disease; COPD, chronic obstructive pulmonary disease; crude HR, crude hazard ratio; PUD, peptic ulcer disease; T2DM, type 2 diabetes mellitus.
A sensitivity analysis was shown in Table 3, in which we excluded patients who were diagnosed with hyperlipidemia within 1 year after cohort entry (i.e., the index date). The results of the sensitivity analysis remained consistent with the main findings (aHR = 1.58; 95% CI = 1.56–1.61). For a visual picture of cumulative incidence, consider the graphic representation in Figure 2. The cumulative incidence of hyperlipidemia was significantly higher in patients with PUD compared to patients without PUD (log-rank test, p < 0.001).
Incidence, crude, and adjusted HR of hyperlipidemia compared among peptic ulcer disease patients compared to non-PUD controls by sensitivity analysis excluding patients diagnosed with hyperlipidemia within 1 year.

Rate, incidence rate, per 1000 person-years.
Adjusted HR: multivariable analysis including age, sex, annual visits, and comorbidities of T2DM, CHD, hypertension, obesity, sleep disorder, COPD, stroke, and heart failure.
p < 0.001.
CHD, coronary heart disease; COPD, chronic obstructive pulmonary disease; crude HR, crude hazard ratio; PUD, peptic ulcer disease; T2DM, type two diabetes mellitus.

Cummulative incidence of hyperlipidemia compared between those with and without peptic ulcer disease using the Kaplan–Meier method.
As shown in Table 4, compared with the non-PUD cohort, patients with PUD without surgery, PUD without bleeding but with surgery, and PUD with bleeding and surgery all had significantly higher risks of hyperlipidemia (aHR = 1.63, 95% CI = 1.60–1.66; aHR = 2.41, 95% CI = 2.12–2.75; and aHR = 2.65, 95% CI = 2.24–3.14, respectively). Moreover, PUD patients requiring surgery, regardless of bleeding status, exhibited significantly higher risks of hyperlipidemia compared with PUD patients who did not undergo surgery (with bleeding, aHR = 1.52, 95% CI = 1.28–1.80; and without bleeding, aHR = 1.41, 95% CI = 1.24–1.61, respectively).
Incidence, crude, and adjusted HR of hyperlipidemia compared among peptic ulcer disease patients with and without surgery treatment compared to non-PUD controls.

Rate, incidence rate, per 1000 person-years.
Adjusted HR: multivariable analysis including age, sex, annual visits, and comorbidities of T2DM, CHD, hypertension, obesity, sleep disorder, COPD, stroke, and heart failure.
p < 0.001.
CHD, coronary heart disease; COPD, chronic obstructive pulmonary disease; crude HR, crude hazard ratio; PUD, peptic ulcer disease; T2DM, type two diabetes mellitus.
To analyze the anti-PUD medications, several findings are listed in Table 5. Patients receiving H2RAs (aHR = 0.61, 95% CI = 0.60–0.62), PPIs (aHR = 0.52, 95% CI = 0.51–0.53), antibiotics (aHR = 0.66, 95% CI = 0.64–0.67), prostaglandin analogs (aHR = 0.70, 95% CI = 0.60–0.81), anticholinergics (aHR = 0.68, 95% CI = 0.66–0.69), antacids (aHR = 0.67, 95% CI = 0.65–0.69), and other (aHR = 0.71, 95% CI = 0.69–0.73) had a lower risk of hyperlipidemia than non-use groups. However, patients receiving bismuth salts (aHR = 0.98, 95% CI = 0.86–1.12) did not show a significant risk of hyperlipidemia compared to the comparison group. KM curves (Figure 3) comparing the incidence of hyperlipidemia according to cumulative duration of use across different exposures. The results demonstrated a trend suggesting that longer durations of certain medications were associated with differing risks of hyperlipidemia, although not all trends reached statistical significance. We conducted additional subgroup analyses to evaluate the impact of anti-PUD medication frequency and combination therapy on the risk of developing hyperlipidemia. As shown in Table 6, we examined the association between the number of different anti-PUD medications used and the subsequent risk of hyperlipidemia. Our findings demonstrated a clear inverse trend, that is, the risk of hyperlipidemia decreased with the increasing number of anti-PUD medications prescribed.
Cox model with HRs and 95% confidence intervals of hyperlipidemia associated with anti-PUD medications among study population.

Rate, incidence rate, per 1000 person-years; crude HR represented relative HR.
Variable found to be statistically significant in the univariable model were further examined in the multivariable model (including age, sex, annual visits, comorbidities of T2DM, CHD, hypertension, obesity, sleep disorder, COPD, stroke, and heart failure). Adjusted HR represented adjusted hazard ratio.
CHD, coronary heart disease; COPD, chronic obstructive pulmonary disease; crude HR, crude hazard ratio; T2DM, type two diabetes mellitus.

Cumulative incidence of hyperlipidemia compared between the with and without anti-PUD medication subgroups using the Kaplan–Meier method. Log-rank tests were used to assess differences across groups.
Incidence, crude, and adjusted HR of hyperlipidemia compared among PUD patients compared to non-PUD controls by sensitivity analysis, excluding patients diagnosed with hyperlipidemia within 1 year.

Rate, incidence rate, per 1000 person-years.
Adjusted HR: multivariable analysis including age, sex, annual visits, and comorbidities of T2DM, CHD, hypertension, obesity, sleep disorder, COPD, stroke, and heart failure.
p < 0.001.
CHD, coronary heart disease; COPD, chronic obstructive pulmonary disease; crude HR, crude hazard ratio; PUD, peptic ulcer disease; T2DM, type two diabetes mellitus.
Discussion
This is the first retrospective cohort analysis to thoroughly evaluate the effect of anti-PUD medications on the risk of developing hyperlipidemia in individuals with PUD. Our findings indicate that patients with PUD have a higher risk of developing hyperlipidemia than those without PUD. However, we also observed that patients treated with most anti-PUD medications had a significantly lower risk of developing hyperlipidemia than those who did not receive these treatments. A sensitivity analysis in which we excluded patients who were diagnosed with hyperlipidemia within 1 year after cohort entry (i.e., the index date) to ensure that the observed association between PUD and the subsequent development of hyperlipidemia is not simply the result of preexisting but undiagnosed hyperlipidemia at baseline or shortly thereafter. The results of the sensitivity analysis remained consistent with the main findings, further supporting the robustness of our conclusions.
Chronic inflammation is a well-recognized consequence of PUD. Increased levels of pro-inflammatory cytokines (e.g., IL-6, TNFα, and CRP) can promote insulin resistance and hepatic lipid synthesis, leading to elevated serum lipid levels. Inflammatory responses may also impair lipid clearance, further contributing to dyslipidemia. 23 A study on the correlation between gastrointestinal inflammation and lipid levels found that higher white blood cell counts were associated with increased levels of LDL-C, VLDL-C, and TGs, while HDL-C levels decreased. 14 PUD can alter gut microbiota composition. Research has shown that conditions such as H. pylori infection can significantly affect the microbial balance in the gastrointestinal tract and can alter the microbiota by reducing the diversity of beneficial bacteria and promoting the growth of pathogenic species. 24 This imbalance may contribute to inflammation, mucosal damage, and disease progression. Additionally, chronic inflammation in PUD can damage the gastric mucosal barrier, increasing intestinal permeability and allowing bacterial endotoxins, such as lipopolysaccharide (LPS), to enter the bloodstream. LPS can trigger systemic inflammation by stimulating immune cells to release pro-inflammatory cytokines (e.g., IL-1β and TNFα), which may promote insulin resistance and hyperlipidemia. This disruption can also impair lipid digestion and absorption, contributing to lipid metabolism disorders. 25 Furthermore, oxidative stress resulting from mucosal injury may affect hepatic lipid metabolism. 25 Another study suggested that PUD disrupts the intestinal barrier, allowing bacteria and their metabolites into the bloodstream and triggering immune responses through the IL-1β pathway, thereby increasing the risk of CVD. 26 PUD is often linked to increased psychological stress and activation of the hypothalamic-pituitary-adrenal axis. Elevated cortisol levels can stimulate lipogenesis and impair lipid clearance, which may further contribute to hyperlipidemia. 27 In addition, PUD may reduce bile secretion, which affects nuclear receptors, such as FXR, LXR, PXR, and TGR5, all of which regulate lipid biosynthesis and metabolism, potentially contributing to hyperlipidemia and increasing the risk of CVD.28,29 Our results showed that patients with PUD had a 2.34-fold increased risk of hyperlipidemia compared with the control cohort, consistent with these previous findings.
NSAIDs influence blood lipid profiles and eicosanoid production. Drugs such as aspirin, diclofenac, and celecoxib have shown hypolipidemic effects in hyperlipidemic rats and diabetic patients.30,31 Aspirin, in particular, reduced steatosis, atherosclerosis, and serum TC in mice. 32 However, some NSAIDs negatively affect lipid metabolism in normolipidemic individuals. 33 They also impact eicosanoid production by inhibiting cyclooxygenases and altering lipid body formation in leukocytes. 34 In addition, NSAIDs can change the lipid composition of intestinal membranes, potentially contributing to gastrointestinal side effects. 35 The effect of H. pylori on lipid metabolism is debated. A Finnish study found that H. pylori-infected individuals had higher TGs and TC, even after adjusting for confounders, suggesting an increased risk of atherosclerosis. 36 Conversely, studies from Northern Ireland and among blood donors and CVD patients found H. pylori was linked to lower HDL-C but not significantly to TC. 37 While studies suggest a link between PUD and lipid disorders, we further examined PUD, hyperlipidemia, and related medications.
Lansoprazole, a PPI, acts as an LXRα agonist, regulating lipid metabolism and biosynthesis, which leads to increased HDL-C and decreased LDL-C levels, making it an effective anti-atherosclerosis drug. This suggests that lansoprazole may have beneficial effects on atherosclerosis.18,38 PPIs modestly enhance LDL-C reduction in patients treated with statin, suggesting a potential interaction that benefits cholesterol management. 39 Although PPI use is associated with increased fasting LDL-C and Apo-B levels, it has no significant effects on other serum biomarkers of inflammation, insulin resistance, CVD risk, or renal function. 40 Al-Bachaji et al. 41 demonstrated that PPIs improve glycemic indices and lipid profiles in patients with T2DM. Thus, PPIs may have beneficial effects on lipid control, although their impact on broader metabolic and inflammatory markers remains unclear. Some studies have collectively indicated that cimetidine generally increases HDL-C and its subfractions, particularly HDL2, with significant increases reported by several studies.42–45 The mechanisms underlying these effects are not fully understood but are suggested to be unrelated to H2-receptor blockade45,46 and further studies are needed to clarify their clinical implications. In our study, we found that both H2RAs and PPIs decreased the risk of hyperlipidemia compared to the non-users, with the aHR of 0.61 and 0.52 (p < 0.001), respectively. We conducted an active-comparator analysis by directly comparing H2RA users with PPI users. The results showed that, relative to H2RA users, PPI users had a lower risk of developing hyperlipidemia (aHR = 0.58, 95% CI = 0.57–0.59, Table S3). This active-comparator design helps minimize confounding related to healthcare utilization and treatment-seeking behavior, as both groups consist of patients receiving prescribed pharmacologic therapy for similar clinical indications and are therefore more comparable in terms of healthcare engagement. The consistency of the observed association in this active-comparator analysis further supports the robustness of our results.
A study investigating the effects of triple therapy for H. pylori eradication on lipid levels found that a 14-day regimen of clarithromycin (1 g/day), amoxicillin (2 g/day), and omeprazole (40 mg/day) significantly increased HDL-C levels (p = 0.001) without notable effects on TC or LDL-C levels. 47 This leads to a reduction in the LDL/HDL ratio, which is an indicator of atherosclerosis, and consequently, reduced CVD risk. 47 Another study found that after H. pylori eradication using triple therapy, HDL-C levels significantly increased (p < 0.05), whereas TC and LDL-C levels significantly decreased. 48 We find significant changes of antibiotics user in aHR for hyperlipidemia risk in this study.
Currently, limited research has established a clear correlation between bismuth salt treatment and alterations in blood lipid levels. Bismuth salts, which are commonly used in the treatment of H. pylori infections and PUD, are more focused on gastrointestinal healing than on lipid metabolism. 2 However, the overall impact of bismuth on lipid levels may be minimal compared to the broader effects of related therapies, and more specific studies are needed to clarify this connection.
Prostaglandin analogs, particularly misoprostol and enprostil, affect lipid profiles and liver function. Specifically, misoprostol increases HDL-C, decreases TC and TG, and enhances liver enzyme activity. 49 Bilgiç and Ozgocmen 50 demonstrated that misoprostol mitigated doxorubicin-induced liver injury by increasing HDL-C and reducing oxidative stress, liver enzymes, and histopathological changes. Schwartz et al. 51 reported that enprostil significantly reduced TC, LDL-C, and Apo-B levels in patients with hypercholesterolemia, indicating its potential for treating hyperlipidemia. Together, these findings suggest that prostaglandin analogs have beneficial effects on lipid metabolism. Antacids are commonly used to neutralize stomach acids and relieve the symptoms of indigestion or heartburn. The impact of antacids on blood lipid levels is not well documented or a primary area of concern in clinical practice, as their primary function revolves around altering stomach pH rather than directly influencing lipid metabolism. 8 The available literature has not established a strong or clinically significant relationship between antacid use and blood lipid levels. Any potential influence of antacids on lipids is likely subtle and secondary to their primary action of neutralizing stomach acids.
Research has shown that CBX can affect lipid metabolism by inhibiting 11β-hydroxysteroid dehydrogenase (11β-HSD1), an enzyme that converts inactive cortisone into active cortisol in tissues. 52 This enzyme is linked to various metabolic processes, including fat storage and lipid metabolism. By inhibiting 11β-HSD1, carbenoxolone might influence lipid profiles, potentially lowering TGs and TC levels. In obese mice, CBX treatment significantly decreased the serum concentrations of TG, TC, and LDL-C, and increased HDL-C levels. 52 In obese Zucker rats, CBX increased HDL-C levels, although it did not affect plasma glucose levels or weight gain. 53 Additionally, in C57BL/6-Lep ob/ob mice, CBX prevented plasma TGs and free fatty acid accumulation. 54 In our studies, these categories of anti-PUD medications represent a significant reduction in hyperlipidemia risk in treated patients with PUD.
Recent literature also suggests that certain surgical procedures involving the gastrointestinal tract can lead to metabolic changes, including altered lipid absorption or hepatic lipid metabolism, which may contribute to hyperlipidemia in the long term.55,56 We acknowledge that gastrointestinal surgery, including partial gastrectomy, can induce long-term metabolic changes through mechanisms such as altered gastric acid secretion, reduced intestinal transit time, and impaired absorption of fats and fat-soluble vitamins. These changes may, paradoxically, result in either a reduction or elevation in lipid levels depending on individual metabolic responses and post-surgical nutritional intake. Some literature suggests that long-term adaptation after gastric surgery can lead to metabolic imbalances, including hyperlipidemia, especially in patients with altered dietary patterns or underlying metabolic conditions.57,58 Nonetheless, we acknowledge that postoperative nutritional status or body weight changes are clinically relevant, as gastrointestinal surgeries (such as partial gastrectomy) may lead to changes in digestion, absorption, and metabolic homeostasis that could influence lipid profiles over time. Although direct data were not available in our cohort, previous studies have reported conflicting findings regarding the metabolic consequences of upper gastrointestinal surgeries. Some reports suggest that postoperative weight loss and reduced fat absorption may lower lipid levels in the short term, whereas others note that long-term metabolic adaptations and changes in dietary patterns may predispose patients to hyperlipidemia.56,57 We found that surgery may alter patients with PUD by the increased risk of developing hyperlipidemia. Our findings suggest that patients with more severe or complicated PUD, as reflected by bleeding events or the need for surgical intervention, may have an even greater risk of developing hyperlipidemia. While the NHIRD does not provide direct clinical or endoscopic severity measures, our sensitivity and stratified analyses using bleeding and surgical status as severity proxies support the robustness and clinical relevance of the observed association.
Death represents a meaningful competing risk in long-term cohort studies, particularly among older individuals and patients with more severe disease, such as those requiring surgical intervention. We conducted an additional competing risk analysis using the Fine-Gray sub-distribution hazard model to evaluate the association between PUD and incident hyperlipidemia while treating death as a competing event (Table S2). The findings remained consistent in both direction and magnitude compared with the primary analysis, indicating that competing mortality did not materially alter the observed association between PUD and hyperlipidemia. In addition, we selected appendicitis as a negative control outcome, as it is not biologically expected to be influenced by PUD or anti-PUD medications. We conducted parallel analyses using the same cohort definitions, covariate adjustments, and modeling strategies as in the primary analysis, including time-dependent exposure modeling and multivariable Cox proportional hazards regression to ensure methodological consistency. As anticipated, no significant association was observed between PUD and the risk of appendicitis (Table S4). These findings provide additional reassurance that the primary association between PUD and hyperlipidemia is unlikely to be fully attributable to systematic bias or residual methodological artifacts.
This study had several strengths. First, data were sourced from the Taiwan NHIRD, a large population-based longitudinal cohort. This nationwide resource is particularly valuable for examining the relationship between anti-PUD medication use and the risk of developing hyperlipidemia. The cohort size provided strong statistical power for subgroup analyses and ensured that the findings could be broadly applied. The robustness of the study was further enhanced by the inclusion of a large population, allowing for a detailed subgroup analysis and long-term assessment of hyperlipidemia risk in patients with PUD who received various treatment approaches, coupled with a high follow-up rate and precise diagnosis. Second, the sample was restricted to individuals with PUD who had no history of hyperlipidemia and had experienced at least two consecutive episodes of PUD. The exclusion of individuals with ambiguous treatment histories helped enhance the diagnostic accuracy. Third, potential confounding factors for hyperlipidemia, including age, sex, T2DM, CHD, hypertension, obesity, sleep disorders, COPD, stroke, and heart failure, were thoroughly considered in the regression models. Fourth, the drug prescription data were highly accurate, as pharmacists were required to document prescriptions in detail for reimbursement, with legal consequences for inaccurate reporting. Finally, we further categorized anti-PUD medication users based on their treatment regimens, identifying correlations between specific anti-PUD medications and either a reduced or increased risk of hyperlipidemia.
Limitations
This study had a few limitations. The primary issue with this retrospective chart audit is that it only identified a statistical correlation between the increased risk of hyperlipidemia in patients with PUD and the effect of anti-PUD medications without establishing a causal link. Consequently, the analysis is largely based on documented intentions. First, the accuracy and reliability of the data may have been affected by the database used, which may have misclassified the cases of PUD and hyperlipidemia. However, given that Taiwan provides universal health insurance, experts have implemented peer-review processes to reduce the risk of false positives. 58 Second, we acknowledge that factors like physical activity, smoking status, and dietary patterns can influence lipid profiles. While our study utilized the Taiwan NHIRD, which provides extensive medical records, it lacks detailed information on patients’ lifestyle behaviors, dietary habits, such as fat intake, alcohol consumption, physical activity levels, BMI measurements, and other nutritional factors that are known to influence both PUD and lipid metabolism. The absence of this data may introduce residual confounding and limit the ability to fully account for dietary influences in our analysis. This limitation may introduce residual confounding. We calculated and incorporated E-values for the primary associations to estimate the minimum strength of association that an unmeasured confounder would need to have with both PUD and hyperlipidemia, independent of the measured covariates (Table 2). Larger E-values indicate that stronger unmeasured confounding would be required to negate the observed association, thereby supporting the robustness of our findings. The severity of PUD could potentially affect both the prescription of specific medications and the risk of hyperlipidemia. However, the NHIRD does not consistently document clinical parameters that accurately reflect disease severity, such as endoscopic findings or symptom scores. Consequently, our analysis could not adjust for PUD severity, which may confound the observed associations. In addition, some patients may have used over-the-counter drugs such as PPIs or H2RAs, which were not captured in the audited records, particularly given the high prevalence of gastroesophageal reflux and family history of the condition. In addition, individuals with better access to healthcare and higher socioeconomic status are more likely to receive regular medical care, including earlier diagnosis and management of both PUD and hyperlipidemia. This could lead to improved lipid profile monitoring and more effective treatment, thereby contributing to the observed lower risk of hyperlipidemia in the medicated PUD group. Conversely, individuals with limited access to healthcare may be underdiagnosed or undertreated, which could result in an underestimation of hyperlipidemia risk in certain subgroups. We performed sensitivity analyses excluding early events, specifically hyperlipidemia diagnoses occurring within the first year after the index date. This strategy minimizes the possibility that increased short-term clinical monitoring immediately following PUD diagnosis explains the observed association. However, the persistence and consistency of the association across multiple analyses, including adjusted models and sensitivity analyses, suggest that surveillance bias alone is unlikely to fully explain our findings. Third, because this claims database was initially established for billing purposes, we could not directly contact the patients or access their personal information because of data anonymization. Fourth, relevant clinical details, such as blood lipid levels, were unavailable, preventing us from assessing the severity of hyperlipidemia in patients with PUD. Hyperlipidemia diagnoses were inferred from the physicians’ medical records. Both PUD and hyperlipidemia were diagnosed based on standard clinical criteria. This approach may introduce diagnostic biases, as it relies on the accuracy and consistency of clinical documentation of ICD codes. Variations in diagnostic criteria, differences in healthcare providers’ practices, and the absence of standardized lipid panel testing can lead to misclassification or underdiagnosis of hyperlipidemia. According to the U.S. Preventive Services Task Force, lipid measurement is crucial for identifying individuals eligible for preventive therapy, and reliance solely on clinical records without standardized testing may compromise the accuracy of hyperlipidemia diagnosis. 59 To mitigate these biases, future studies should incorporate direct measurements of blood lipid levels using standardized lipid panels. To better evaluate the relationship between PUD, anti-PUD medications, and hyperlipidemia, a comprehensive prospective study or randomized controlled trial using data from diverse sources is recommended. While retrospective studies inherently carry biases, the high coverage rate of Taiwan’s NHI program and careful review of diagnoses ensure a level of reliability in these findings.
Conclusion
In conclusion, in the Taiwanese population, PUD was significantly associated with an elevated risk of developing hyperlipidemia. However, individuals taking most anti-PUD medications exhibited a greater reduction in the incidence of hyperlipidemia than those not using these medications. We suggest that our findings may highlight the potential value of considering blood lipid monitoring in patients with PUD, particularly in future research or clinical assessments. Further studies are needed to explore whether specific anti-PUD medications can be clinically utilized as novel treatments or preventive agents for hyperlipidemia.
Supplemental Material
sj-doc-1-tae-10.1177_20420188261442014 – Supplemental material for Impact of anti-peptic ulcer disease (PUD) medications on hyperlipidemia risk in patients with PUD: a population-based retrospective cohort study
Supplemental material, sj-doc-1-tae-10.1177_20420188261442014 for Impact of anti-peptic ulcer disease (PUD) medications on hyperlipidemia risk in patients with PUD: a population-based retrospective cohort study by Hui-Hsia Hsieh, Wan-Yi Lee, Cheng-Li Lin, Chi-Hua Chen, Fuu-Jen Tsai, Bang-Jau You, Ni Tien, Yi-Jen Fang and Yun-Ping Lim in Therapeutic Advances in Endocrinology and Metabolism
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.