
Abstract
Background:
Glucagon-like peptide-1 receptor agonists (GLP-1RAs) are widely used across the glycemic spectrum, yet their thyroid safety profile remains debated. Prior studies have shown inconsistent findings, and evidence across prediabetes, type 1 diabetes (T1D), and type 2 diabetes (T2D) is lacking.
Objectives:
To evaluate diabetes-type-specific associations between GLP-1RA therapy and thyroid outcomes, including thyroid dysfunction, autoimmune thyroiditis, nontoxic goiter, and thyroid cancer.
Design:
A real-world, retrospective target-trial emulation using electronic health records (EHR) from a large multicenter network.
Methods:
We used the TriNetX US Collaborative Network to identify adults with prediabetes, T1D, or T2D initiating GLP-1RAs. Active comparators included usual care and sodium–glucose cotransporter two inhibitors (SGLT2i). Propensity score matching with extensive covariate adjustment was applied. Participants were followed for incident thyroid outcomes for up to 5 years. Sensitivity and subgroup analyses were conducted to assess robustness.
Results:
Across glycemic states, GLP-1RA therapy demonstrated distinct thyroid safety patterns. In prediabetes and T1D, GLP-1RA use was associated with reduced risks of thyroid dysfunction and all-cause mortality, suggesting potential metabolic or immunomodulatory benefits. By contrast, among individuals with T2D, GLP-1RA exposure was linked to modest increases in autoimmune thyroiditis and nontoxic goiter, particularly among those with obesity or without hypertension. Importantly, no increased risk of thyroid cancer was observed in any glycemic state, providing reassuring evidence regarding long-term endocrine safety.
Conclusion:
In this large-scale target-trial emulation, GLP-1RAs showed favorable thyroid safety profiles in prediabetes and T1D, while modestly increasing selected nonmalignant thyroid outcomes in T2D. The absence of elevated thyroid cancer risk across glycemic states supports the overall endocrine safety of GLP-1RAs. These findings highlight the importance of individualized monitoring, particularly in metabolically high-risk T2D populations.
Keywords
Introduction
Diabetes mellitus, a chronic metabolic disorder characterized by persistent hyperglycemia, affects over 500 million individuals worldwide and remains a leading cause of morbidity and mortality.1,2 This disease encompasses several subtypes, including type 1 diabetes (T1D), type 2 diabetes (T2D), and prediabetes (PreD), each with distinct pathophysiological mechanisms and clinical presentations.3,4 The rising global prevalence of diabetes, particularly T2D, has driven the widespread adoption of novel pharmacotherapies designed to improve metabolic control and reduce long-term complications.2,5,6
Glucagon-like peptide-1 receptor agonists (GLP-1RAs) have emerged as a cornerstone of modern diabetes management. Beyond their potent glucose-lowering effects, these agents confer weight reduction and cardiometabolic benefits,7–10 making them increasingly prescribed across a broad glycemic spectrum, including PreD, 11 obesity, 12 and, in some cases, T1D.13–16 However, as their indications expand, concerns regarding potential adverse effects have also grown. The U.S. Food and Drug Administration has issued boxed warnings based on preclinical evidence suggesting C-cell hyperplasia and medullary thyroid carcinoma associated with GLP-1RA exposure,17–19 though human data remain inconsistent. While randomized controlled trials (RCTs) have largely supported their short-term safety,20,21 the limited duration and selective enrollment of such trials preclude robust conclusions about long-term thyroid risk.
Emerging real-world studies have provided conflicting evidence, with some reporting an increased incidence of thyroid disorders and others demonstrating no significant association.20–26 Importantly, prior investigations have primarily focused on patients with T2D, leaving a critical knowledge gap regarding how thyroid outcomes may differ across the continuum of glycemic states. Given that immune and metabolic factors vary substantially among individuals with PreD, T1D, and T2D, these differences may modulate thyroid vulnerability during GLP-1RA treatment.
This study aimed to evaluate the long-term thyroid safety of GLP-1RAs across PreD, T1D, and T2D using a large-scale real-world target-trial emulation. By leveraging data from over two million adults in the TriNetX US Collaborative Network, we sought to determine whether GLP-1RA-associated thyroid risks vary according to glycemic state, thereby informing individualized risk–benefit assessments and clinical monitoring strategies.
Research design and methods
Study design and cohort definition
Our study used a target trial emulation framework to compare thyroid-related health outcomes between GLP-1RAs users and GLP-1RA non-users across three distinct and mutually exclusive populations: PreD, T1D, and T2D, each independently defined to ensure cohort non-overlap. We analyzed data from the TriNetX US Collaborative Network (January 2015–February 2025) and used 1:1 propensity score matching (PSM) to balance treatment groups. The design mimicked RCTs while addressing potential biases in observational studies through methodological safeguards such as PSM and time-based exposure definitions (per-protocol (PP) analyses). Sensitivity analyses incorporated SGLT2 inhibitor (SGLT2i) users as an active comparator to evaluate robustness. Full details of the study protocol, bias mitigation strategies, and statistical approaches are provided in Table S1, and a schematic study design timeline is shown in Figure 1.
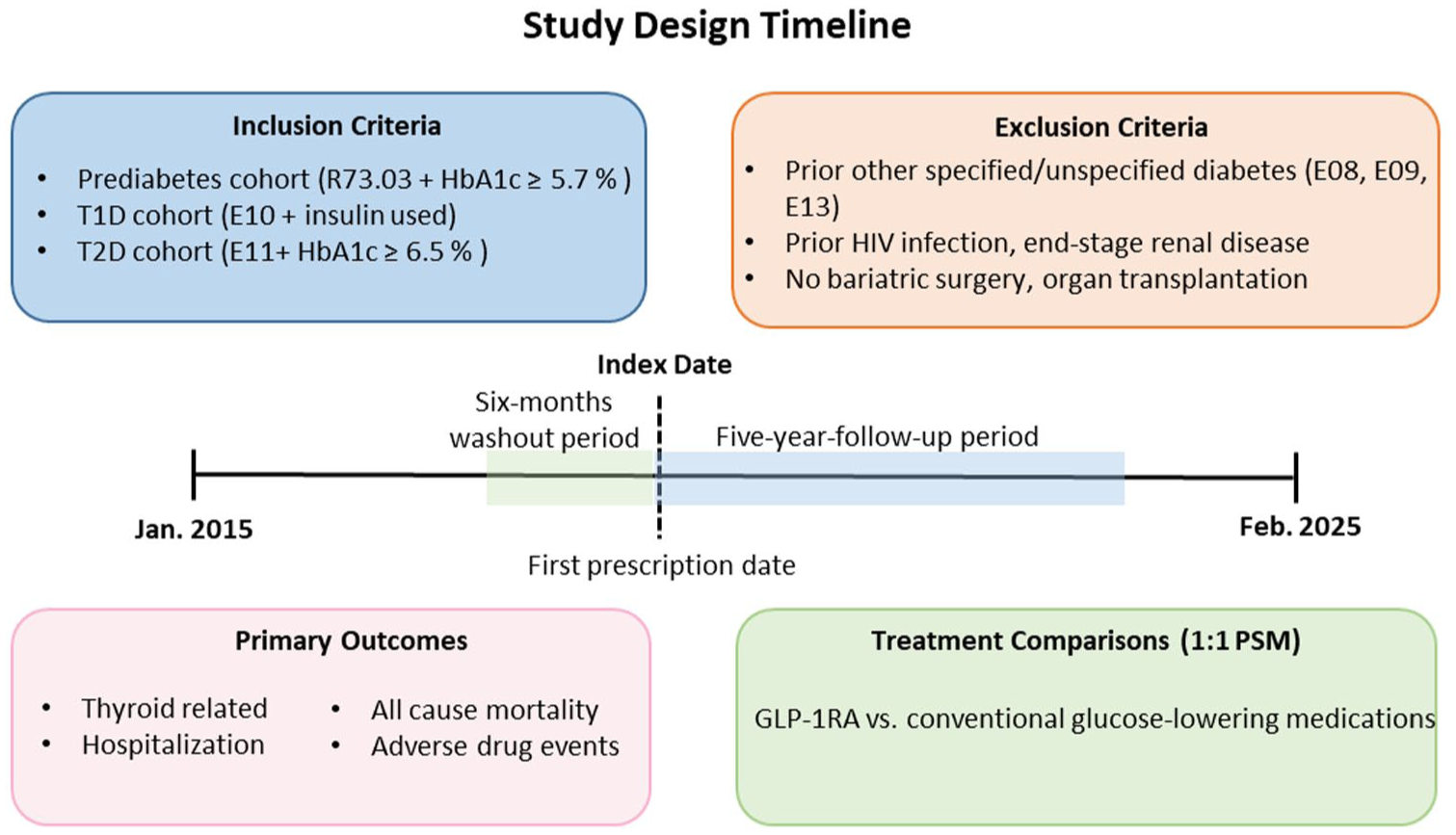
Study design timeline and key methodological components of the target trial emulation. This figure illustrates the temporal framework and core methodological elements of our target trial emulation study. The observation period extended from January 2015 to February 2025, with the index date defined as the first prescription date of the study medication. A 6-month washout period was applied prior to the index date to minimize potential carryover effects from prior treatments. Three distinct cohorts were included: prediabetes (PreD; ICD-10-CM: R73.03), type 1 diabetes (E10), and type 2 diabetes (E11). Additional inclusion criteria were as follows: HbA1c ⩾ 5.7% (TNX curated code: 9037) for the PreD cohort; insulin use for the type 1 diabetes cohort; and HbA1c ⩾ 6.5% for the type 2 diabetes cohort. Exclusion criteria included other specified/unspecified diabetes (E08, E09, and E13), prior bariatric surgery, organ transplantation, HIV infection, or end-stage renal disease. Primary outcomes included all-cause mortality, hospitalization, adverse drug events, and thyroid-related outcomes. Treatment comparisons were conducted using 1:1 PSM between GLP-1 receptor agonist users and non-users (comparators). A 5-year follow-up period was implemented to enable comprehensive assessment of long-term outcomes across all three cohorts.
The primary cohorts were defined using ICD-10 codes: PreD (R73.03), T1D (E10), and T2D (E11). To improve diagnostic specificity, additional inclusion criteria were applied for each cohort. Individuals in the PreD cohort were required to have a glycated hemoglobin (HbA1c) level ⩾5.7% (39 mmol/mol; TNX curated code: 9037). Those in the T1D cohort were required to have documented insulin use after diagnosis; however, autoimmune antibody data were not consistently available in the TriNetX database. To further improve diagnostic specificity, we ensured that individuals with other specified or secondary diabetes subtypes (E08, E09, and E13) were not included, although misclassification with insulin-treated T2D (E11) cannot be fully ruled out. Individuals in the T2D cohort were required to have HbA1c ⩾ 6.5% (48 mmol/mol) and to have received metformin following diagnosis. The index date was defined as the first prescription of the study medication after the diagnosis (index event). A 6-month washout period prior to the index date excluded individuals with any documented GLP-1RA use to prevent contamination from previous exposure. Additional exclusion criteria included other specified or unspecified diabetes (E08, E09, and E13), other types of diabetes, neoplasms, HIV infection, and end-stage renal disease before the index date, as well as any history of bariatric surgery or organ transplantation.
In each cohort, we identified two comparison groups: individuals who initiated GLP-1RAs (GLP-1RA users) and those who did not use (non-users). To ensure a clean comparison, both groups were required to have no exposure to SGLT2i at any time during the observation window. Because non-users may receive other glucose-lowering medications, PSM was applied to balance the distributions of all other antidiabetic drug classes—including metformin, biguanides, sulfonylureas, thiazolidinediones, dipeptidyl peptidase-4 inhibitors, and insulin—so that any differences in outcomes would more likely reflect GLP-1RA use rather than disparities in concomitant medication patterns.
Users of each medication were defined as individuals prescribed the medication after the index event, with at least one follow-up encounter within 5 years of treatment initiation. Matched GLP-1RA users and non-users were generated using 1:1 nearest-neighbor PSM without replacement. Matching covariates included demographic characteristics, lifestyle factors, comorbidities, medication use, and clinical parameters. Standardized mean differences (SMDs) <0.1 were considered indicative of adequate balance (Tables S2–S4). Detailed variable definitions and TriNetX codes are provided in the Supplemental Appendix.
After applying inclusion and exclusion criteria and completing PSM, the final analytic datasets included 43,167 individuals in each arm for the PreD cohort, 7428 individuals in each arm for the T1D cohort, and 137,952 individuals in each arm for the T2D cohort (detailed in Figure S1).
Outcomes
We investigated thyroid-related events as our primary outcome, including thyroid cancer, hypothyroidism, hyperthyroidism, autoimmune thyroiditis, nontoxic goiter, and other disorders of thyroid. Secondary outcomes were all-cause mortality and hospitalization occurring from the index event to a 5-year period (1825 days). Clinical biochemical profiles, including HbA1c, blood glucose, and body mass index (BMI), were investigated to confirm the clinical efficacy of GLP-1RAs and indicate satisfactory adherence to prescribed treatment protocols. Furthermore, exploratory outcomes such as adverse drug events (ADE) and negative control were also investigated. All outcomes were defined using ICD-10 codes or TNX curated codes (provided in Supplemental Material section (C)).
Covariates
We included a comprehensive set of covariates in our analysis. Demographic characteristics were as follows: age, sex, race, and ethnicity; lifestyle factors: nicotine dependence and problems related to lifestyle; comorbidities; Medication use: antidiabetic agents, heart medications, hypolipidemic agents, anticoagulants, and diuretics; and laboratory parameters: BMI, HbA1c, serum creatinine, lipid profiles (HDL, LDL, TG), CRP, and cardiac Troponin I. The presence of comorbidities was determined using their respective ICD-10 codes, and medication use was identified through prescription records. Laboratory values were extracted from structured data fields within the EHR. These covariates were incorporated into the PSM algorithm to minimize potential confounding factors and ensure a valid comparison of outcomes between the two groups. Detailed code lists and definitions are provided in the Supplemental Material section (C).
Negative controls
To validate our analytical approach and detect potential unmeasured confounding, we employed two negative control outcomes, dog bites or ingrowing nail, which should have no plausible biological connection to the drug mechanism.
Statistical analysis
To assess the risk of outcomes between GLP-1RA users and comparators, we used Cox proportional hazards models, presenting results as hazard ratios (HRs) with 95% confidence intervals (CIs). Kaplan–Meier (K–M) curves were constructed to visualize cumulative incidence, and the log-rank test was used to evaluate group differences. To strengthen validity, we applied multiple approaches to reduce potential biases, including immortal time and selection bias. PSM (1:1 nearest neighbor) was performed to balance baseline covariates, with standardized mean differences <0.1 considered well balanced. Sensitivity analyses used PP definitions (⩾3 prescriptions during follow-up or within 45 days of initiation) to approximate sustained medication use. Subgroup analyses stratified by sex, eGFR (⩾45 or <45 mL/min/1.73 m²), BMI (<30 or ⩾30 kg/m²), presence of hypertension, and age (<60 or ⩾60 years) examined heterogeneity of associations. The consistency of results across these strategies supports the robustness of our findings. Statistical significance was set at two-sided p < 0.05, with Benjamini–Hochberg correction for multiple comparisons. For significant associations, we calculated E-values to quantify the strength of unmeasured confounding required to nullify results. Analyses were conducted on the TriNetX platform using Java 11.0.16 (Apache Commons Math 3.6.1), R 4.0.2 (Hmisc 1-1, Survival 3.2-3), and Python 3.7 (lifelines 0.22.4, matplotlib 3.5.1, numpy 1.21.5, pandas 1.3.5, scipy 1.7.3, and statsmodels 0.13.2).
Results
Baseline characteristics and cohorts
The study included three mutually exclusive matched cohorts: 43,167 individuals with PreD, 7428 with T1D, and 137,952 with T2D in each treatment arm. After matching, the mean age ranged from 53 to 59 years, and females accounted for 63.5%, 48.4%, and 50.9% of the PreD, T1D, and T2D cohorts, respectively. Baseline characteristics, including demographics (age, sex, race, ethnicity), comorbidities, medication used, and laboratory parameters, were well balanced between GLP-1RA users and non-users. This included comparable use of metformin, biguanides, sulfonylureas, thiazolidinediones, dipeptidyl peptidase 4 (DPP-4) inhibitors, and insulin, as well as similar proportions of individuals with HbA1c ⩾ 7%, and BMI ⩾ 30 kg/m2 (all SMD <0.1; Tables S2–S4; Figure S2).
Five-year risk of thyroid outcomes: GLP-1RA users versus non-users across prediabetes, type 1 diabetes, and type 2 diabetes
Our study investigated the 5-year risk of thyroid-related outcomes associated with GLP-1RA use versus non-use across PreD, T1D, and T2D cohorts (Figure 2, Tables S5–S7, and Figures S3–S5). Thyroid cancer incidence did not differ significantly between groups in any cohort. However, other thyroid-related outcomes demonstrated distinct glycemic-status-specific patterns. In the PreD cohort, GLP-1RA use was associated with significantly lower risks of hypothyroidism (HR 0.82, 95% CI 0.74–0.90), hyperthyroidism (HR 0.85, 95% CI 0.68–0.98), and other thyroid disorders (HR 0.77, 95% CI 0.67–0.90). Five-year cumulative incidences were 1.8%, 0.4%, and 0.7% with GLP1-RA use versus 3.6%, 0.8%, and 1.4% without GLP-1RA use, respectively (Figure 2(a); Table S5; Figure S3).
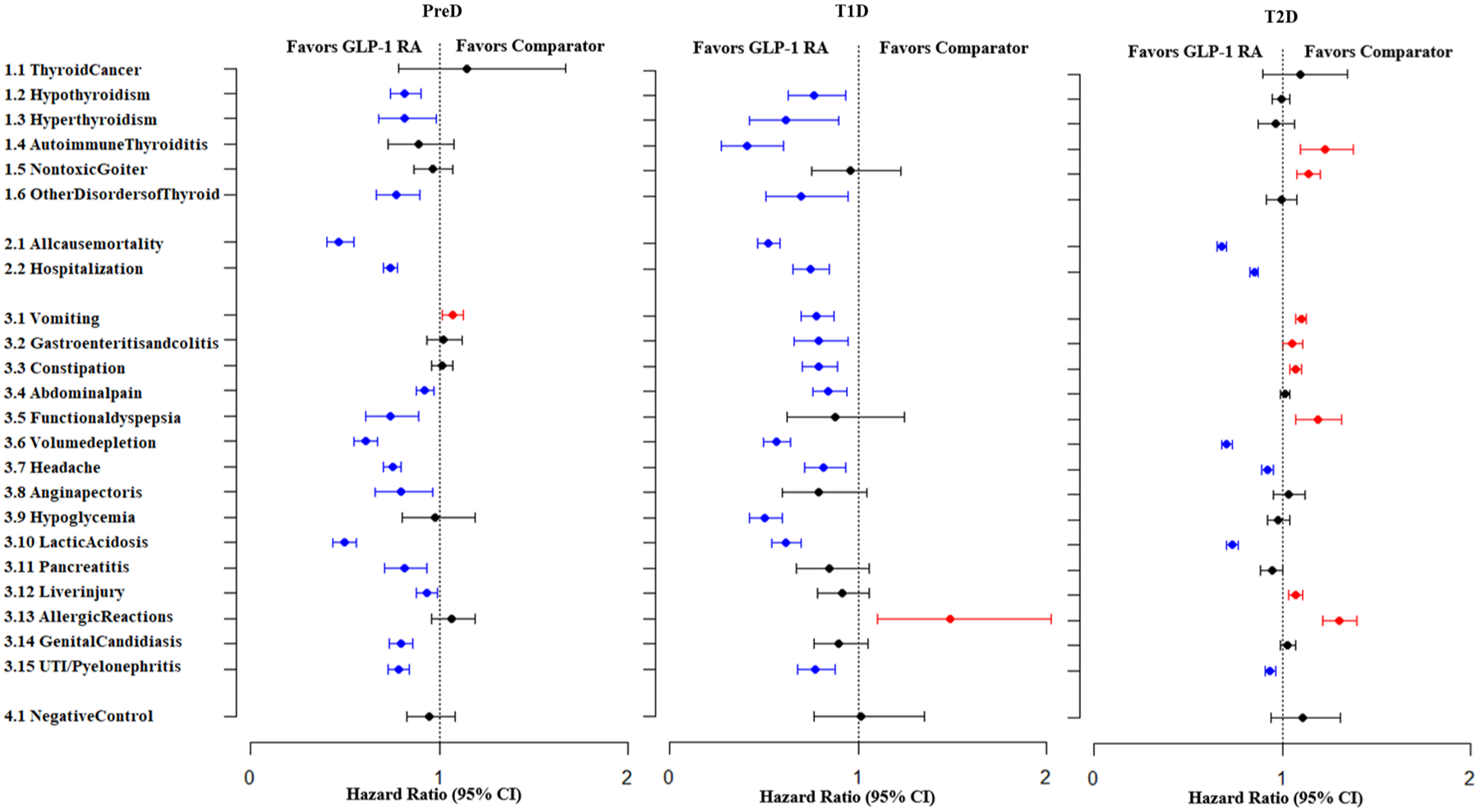
Forest plots of hazard ratios for all outcomes comparing GLP-1RA users with non-users across all cohorts. The plots present hazard ratios with 95% confidence intervals from ITT analyses in the (a) prediabetes, (b) type 1 diabetes, and (c) type 2 diabetes cohorts.
In the T1D cohort, GLP-1RA use was similarly associated with reduced risks of hypothyroidism (HR 0.77, 95% CI 0.63–0.94), hyperthyroidism (HR 0.61, 95% CI 0.42–0.90), autoimmune thyroiditis (HR 0.41, 95% CI 0.27–0.61), and other disorders of thyroid (HR 0.69, 95% CI 0.51–0.95). Five-year cumulative incidences were 2.8%, 0.6%, 0.5%, and 0.9% with GLP1-RA use versus 3.9%, 1.0%, 1.2%, and 1.4% without GLP1-RA use, respectively (Figure 2(b); Table S6; Figure S4).
By contrast, in the T2D cohort, GLP-1RA use was associated with an increased risk of autoimmune thyroiditis (HR 1.23, 95% CI 1.10–1.38) and nontoxic goiter (HR 1.14, 95% CI 1.08–1.20). Five-year cumulative incidences were 0.5% and 2% with GLP1-RA versus 0.4% and 1.9% with comparators, respectively (Figure 2(c); Table S7; Figure S5).
These patterns were generally consistent when compared with SGLT2i (Tables S8–S10). In the PreD cohort, GLP-1RA use was associated with reduced hypothyroidism risk (HR 0.78, 95% CI 0.64–0.94) but increased nontoxic goiter risk (HR 1.26, 95% CI 1.03–1.54) compared to SGLT2i use. No significant differences were observed in thyroid outcomes in the T1D cohort. In the T2D cohort, GLP-1RA use was associated with increased risks of autoimmune thyroiditis (HR 1.16, 95% CI 1.02–1.32) and nontoxic goiter (HR 1.06, 95% CI 1.00–1.13).
Five-year risk of all-cause mortality and hospitalizations: GLP-1RA users versus non-users across prediabetes, type 1 diabetes, and type 2 diabetes
Across all cohorts, GLP-1RA use was associated with significantly lower risks of all-cause mortality and hospitalization (Figure 2; Tables S5–S7). Mortality risk reductions were greatest in PreD (HR 0.47, 95% CI 0.40–0.55), followed by T1D (HR 0.52, 95% CI 0.47–0.58) and T2D (HR 0.68, 95% CI 0.66–0.71). Hospitalization risk displayed similar patterns. Compared with SGLT2i use, the lower all-cause mortality was observed among GLP-RA users in the PreD and T2D groups.
Five-year risk of ADEs: GLP-1RA users versus non-users across prediabetes, type 1 diabetes, and type 2 diabetes
Gastrointestinal adverse events varied across populations. Higher vomiting rates were observed among PreD (HR 1.07, 95% CI 1.02–1.13, p < 0.05) and T2D (HR 1.10, 95% CI 1.07–1.13, p < 0.05; Figure 2; Tables S5–S7). Gastroenteritis/colitis, constipation, and functional dyspepsia occurred more frequently in T2D, while no increased gastrointestinal risk in T1D.
Metabolic safety profiles also differed. GLP-1RA use was associated with higher rates of allergic reactions in both T1D (HR 1.49, 95% CI 1.10–2.03, p < 0.01) and T2D (HR 1.30, 95% CI 1.22–1.40, p < 0.001). An increased risk of liver injury was observed in T2D (HR 1.07, 95% CI 1.04, 1.11, p < 0.001). Compared to SGLT2i use in T2D, GLP-1RA therapy was associated with higher risks of hypoglycemia (HR 1.13, 95% CI 1.06–1.20, p < 0.001) and allergic reaction (HR 1.19, 95%CI 1.10–1.29, p < 0.001; Figure 2; Tables S5–S7).
Sensitivity analysis
Sensitivity analyses were conducted in two predefined subgroups to evaluate the robustness under stricter exposure definitions. Subgroup 1 included individuals meeting PP1 criteria (⩾3 prescriptions). Subgroup 2 applied the PP2 definition (⩾3 prescriptions plus follow-up encounter within 45 days after drug initiation). Findings were consistent with the main results (Figures S6–S7). Protective associations for hypothyroidism and other thyroid disorders persisted in PreD; reductions in hypothyroidism and autoimmune thyroiditis remained in T1D; and increased risks of autoimmune thyroiditis and nontoxic goiter continued to be observed in T2D under both definitions.
Subgroup analyses
Subgroup analyses stratified by sex, eGFR, BMI, hypertension status, and age showed results largely consistent with the primary findings. In the PreD cohort, protective effects for hypothyroidism and hyperthyroidism were largely preserved across subgroups (Figure 3; Tables S11–S15). In T1D, reduced risks of hypothyroidism, hyperthyroidism, and autoimmune thyroiditis were observed across most subgroups; however, subgroup analyses for thyroid cancer were not feasible due to limited events (Figure 3; Tables S16–S20). In T2D, the elevated risk of nontoxic goiter persisted across most subgroups but was not statistically significant among those with normal BMI or with hypertension. Increased risk of autoimmune thyroiditis was significant only in those with obesity or without hypertension (Figure 3; Tables S21–S25).
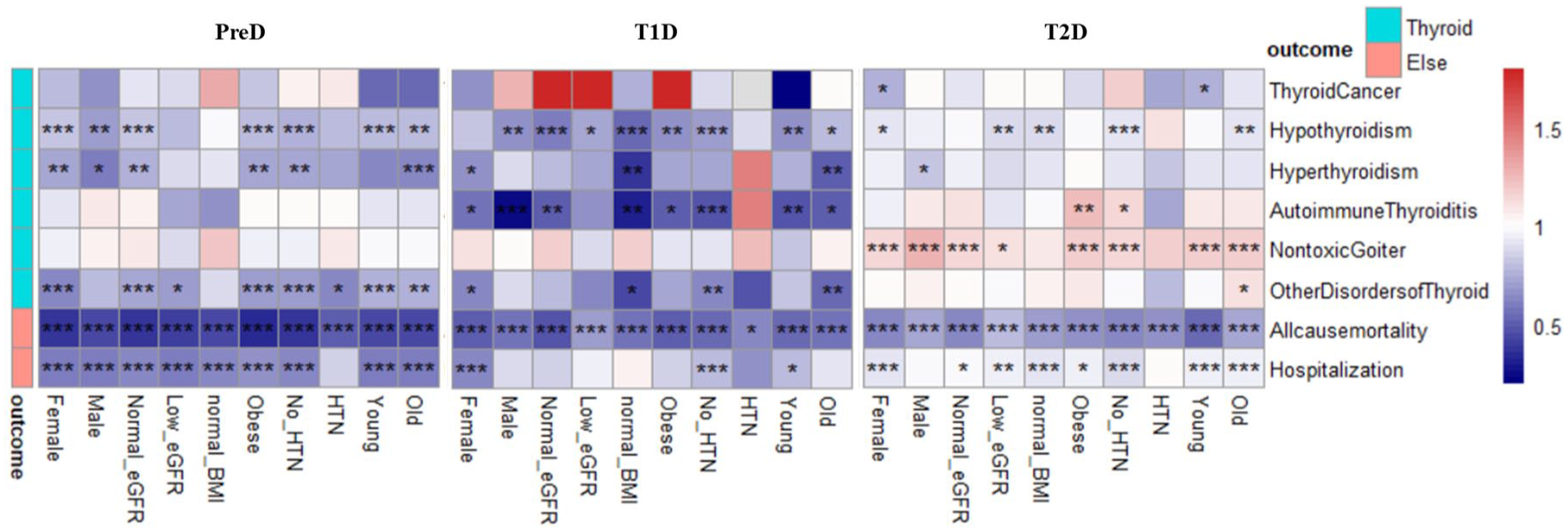
Heatmaps of HRs for all outcomes comparing GLP-1RA users with non-users across clinical subgroups. In the heatmaps, the x-axis represents different subgroups and the y-axis represents various outcomes in the prediabetes (left), type 1 diabetes (middle), and type 2 diabetes (right) cohorts. The color gradient reflects the magnitude of the HRs, with darker colors indicating larger effect sizes. Statistically significant results are marked with asterisks: *p < 0.05; **p < 0.01; ***p < 0.001.
Comparative analysis of clinical biochemical profiles
At the 5-year follow-up, GLP-1RA users in the PreD cohort showed greater reductions in BMI and HbA1c than non-users. In T1D and T2D, GLP-1RA use was associated with reductions in BMI, while HbA1c changes were comparable between groups. Full results are shown in Figure S8.
Discussion
In this large-scale, real-world target-trial emulation involving individuals with PreD, T1D, and T2D, GLP-1RA therapy revealed glycemic-state–dependent thyroid safety profiles. In both the PreD and T1D cohorts, GLP-1RA use was consistently associated with reduced risks of thyroid dysfunction and all-cause mortality. By contrast, among individuals with T2D, GLP-1RA exposure was linked to modestly increased risks of autoimmune thyroiditis and nontoxic goiter, particularly among those with obesity or without hypertension, suggesting a potential interaction between metabolic status and thyroid response. Importantly, no increased risk of thyroid cancer was observed across glycemic states, providing overall reassurance regarding endocrine safety. Together, these findings highlight that GLP-1RA safety is not uniform across metabolic conditions and underscore the need for individualized monitoring based on baseline glycemic and metabolic characteristics.
The relationship between GLP-1RAs and thyroid disease risk has long been debated, with inconsistent findings across clinical trials and observational studies. A French national case-control study suggested an increased incidence of thyroid cancers, 22 whereas cohort studies from Korea and Scandinavia, with shorter follow-up durations, reported null associations.23,24 A target-trial emulation observed transient risk elevations during the first treatment year, but these did not persist over time. 25 Conversely, a recent multisite cohort analysis encompassing six population-based databases found no association even at higher cumulative doses, supporting a generally favorable safety profile. 26 More recently, a large 2025 retrospective new-user active-comparator cohort study by Morales et al. involving over four million adults similarly reported no significant increase in either benign or malignant thyroid tumors with GLP-1RA therapy, further reinforcing the absence of carcinogenic risk in routine clinical practice. 27 Two meta-analyses of RCTs reported modest increases in thyroid disorders, particularly with liraglutide and dulaglutide, although these results were largely driven by short-duration studies and small event numbers.20,21 Taken together, evidence from contemporary large-scale cohorts—including the Morales et al. study and the present analysis—progressively supports the conclusion that GLP-1RA therapy does not elevate thyroid cancer risk, and that previously observed signals may reflect surveillance intensity, residual confounding, or insufficient follow-up in earlier studies. Therefore, the clinical significance of these associations should be interpreted with appropriate caution.
Compared with previous investigations, our study offers several advantages. To our knowledge, this is the first large-scale real-world analysis assessing GLP-1RA-related thyroid outcomes across PreD, T1D, and T2D. We leveraged a cohort of over two million adults with up to 5 years of follow-up, incorporated both usual care and SGLT2i as comparators, and adjusted for more than 60 clinical and demographic covariates. Multiple sensitivity and subgroup analyses further confirmed the robustness of our findings, minimizing the potential influence of confounding and bias inherent to observational data. By identifying glycemic-state–specific heterogeneity in nonmalignant thyroid outcomes while consistently demonstrating no increase in thyroid cancer, our results contribute a nuanced perspective that complements and extends prior literature.
Mechanistically, the thyroid effects of GLP-1RAs remain incompletely understood. Preclinical studies have proposed two opposing hypotheses: potential proliferative stimulation of thyroid C cells through GLP-1 receptor activation,17–19,28–30 and conversely, antitumor activity via modulation of macrophage and immune cell pathways. 31 GLP-1RAs may influence the hypothalamic–pituitary–thyroid axis and peripheral metabolism through weight reduction and improved insulin sensitivity. 32 The favorable thyroid outcomes observed in PreD and T1D may reflect the immunomodulatory effects33–35 and anti-inflammatory36–38 of GLP-1RAs, whereas the metabolic milieu in T2D, characterized by obesity, insulin resistance, and chronic low-grade inflammation, may modify these responses and contribute to differential thyroid outcomes. However, these mechanistic interpretations are speculative, as our study is based on observational EHR data without direct biological measurements. Further translational and experimental studies are required to elucidate the underlying mechanisms.
Limitations
Several limitations should be considered when interpreting these results. First, given the observational nature of the study, residual confounding cannot be completely ruled out, even with rigorous PSM and extensive covariate adjustment. Second, reliance on EHR data may have resulted in incomplete capture of certain medical conditions. In particular, outcome misclassification is possible due to reliance on diagnostic codes, especially for autoimmune thyroiditis and thyroid cancer, which may lead to non-differential misclassification bias. In addition, misclassification of diabetes subtypes is possible. Although T1D was defined using the ICD-10 code E10 with insulin use, this approach may not fully distinguish autoimmune T1D from insulin-treated T2D. Despite exclusion of other specified diabetes subtypes (E08, E09, and E13), misclassification with T2D (E11) may persist, particularly given the absence of autoantibody data (e.g., GAD or IA-2) and the relatively older age distribution of the T1D cohort. Furthermore, differential healthcare utilization may introduce detection bias, as patients receiving GLP-1RAs may undergo more frequent clinical follow-up or laboratory testing, potentially increasing the likelihood of thyroid disorder detection compared with non-users. These limitations may introduce heterogeneity in the observed associations and are inherent to large-scale EHR-based studies. Third, our analysis did not fully account for variations in medication dosage, treatment adherence, or lifestyle modifications, all of which could potentially influence clinical outcomes. This limitation also restricts our ability to assess potential dose- or time-dependent effects of GLP-1RA exposure. Future research incorporating detailed longitudinal data on dosage, adherence, and duration will be essential to clarify these temporal relationships. Fourth, although our study leveraged a large and diverse population from the TriNetX US Collaborative Network, the generalizability of these findings to non-U.S. or Asian populations may be limited due to differences in genetic background, healthcare systems, and treatment practices. Caution is warranted when extrapolating these results to other regions or ethnic groups. Finally, while the overall sample size was substantial, the number of outcome events in the T1D cohort, particularly for rare outcomes such as thyroid cancer, was relatively small. This issue was further exacerbated in subgroup analyses, potentially reducing statistical power and the precision of effect estimates.
Conclusion
Our findings provide real-world evidence supporting the overall thyroid safety of GLP-1 receptor agonists while underscoring the importance of individualized monitoring. In patients with T2D, particularly those who are obese, periodic thyroid function tests or ultrasonography may be warranted to detect early abnormalities. Conversely, the favorable profiles observed in PreD and T1D suggest that GLP-1RAs can be used more confidently in metabolic prevention and weight management contexts. Together, these data provide real-world evidence informing risk-benefit assessment and guide tailored surveillance strategies as GLP-1RAs are increasingly prescribed across the glycemic spectrum.
Supplemental Material
sj-docx-1-tae-10.1177_20420188261460619 – Supplemental material for Diabetes-type-specific thyroid safety of GLP-1 receptor agonists: evidence from a large real-world cohort
Supplemental material, sj-docx-1-tae-10.1177_20420188261460619 for Diabetes-type-specific thyroid safety of GLP-1 receptor agonists: evidence from a large real-world cohort by Hao-I Hsieh, Yu-Nan Huang, Ya-Wen Chang and Wen-Ling Liao in Therapeutic Advances in Endocrinology and Metabolism
Supplemental Material
sj-docx-2-tae-10.1177_20420188261460619 – Supplemental material for Diabetes-type-specific thyroid safety of GLP-1 receptor agonists: evidence from a large real-world cohort
Supplemental material, sj-docx-2-tae-10.1177_20420188261460619 for Diabetes-type-specific thyroid safety of GLP-1 receptor agonists: evidence from a large real-world cohort by Hao-I Hsieh, Yu-Nan Huang, Ya-Wen Chang and Wen-Ling Liao in Therapeutic Advances in Endocrinology and Metabolism
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.