
Abstract
Background:
In Côte d’Ivoire, pharmacovigilance is not a routine activity in most healthcare facilities and many healthcare professionals have limited knowledge of pharmacovigilance methods.
Objectives:
This study aimed to evaluate the quality of adverse event (AE) reports submitted to the central Pharmacovigilance Unit in Côte d’Ivoire and to perform causality assessments (CAs) on each report.
Design:
This was a descriptive, retrospective analysis of AE reports notified between January 2019 and February 2020 by healthcare providers in Côte d’Ivoire.
Methods:
We assessed 141 verified reports of suspected adverse reactions to medicines, of which 118 reports were eligible for inclusion in the analysis of report quality using a modified Beckmann method. CAs were performed using the World Health Organization-Uppsala Monitoring Center (WHO-UMC) method and French CA method.
Results:
Of 118 AE reports, 28 (23.7%) had very good/good quality, 74 (62.7%) were average, 12 (10.2%) had poor quality, and 4 (3.4%) contained insufficient information for assessment. CAs could be performed for all reports except the four with insufficient information (three had no information on patient or suspected drug; all four had no information on the AE), although the reliability of the CA for poor quality reports was questionable. There was no significant difference in distribution of causality ratings calculated by the WHO-UMC method (p = 0.42) or the French method (p = 0.91) by report quality.
Conclusion:
There is underreporting of AEs in Côte d’Ivoire and most AE reports had average quality. The reliability of the CA, irrespective of method used, was dependent on the quality of reporting. Further training and mentoring of healthcare providers are required to increase the number and completeness of AE reports submitted to the central Pharmacovigilance Unit, and thereby directly support more accurate CAs in Côte d’Ivoire.
Plain language summary
Keywords
Introduction
Pharmacovigilance (PV) is the science and activities relating to the detection, assessment, understanding, and prevention of adverse effects or any other medicine/vaccine-related problem. 1 The reliability and utility of PV conducted via the World Health Organization (WHO) global safety database, VigiBase, coordinated by the Uppsala Monitoring Centre (UMC), are dependent on the timeliness and completeness of individual case safety reports (ICSRs) received by national PV centers and entered into the database. 2 However, PV systems are nascent or nonoperational in many low- and middle-income countries (LMICs).3,4 Of all ICSRs entered into VigiBase, around two-thirds are from the United States and the European Union, 5 and LMICs contribute around 18%, despite making up over 70% of the membership of the WHO Program for International Drug Monitoring. 6
In Côte d’Ivoire, PV activities evolved from an academic to an institutional activity managed within a safety department that became the Vigilance Unit of the Ivorian Pharmaceutical Regulatory Authority (Autorité Ivoirienne de Régulation Pharmaceutique: AIRP). 7 AIRP is responsible for effective (postmarketing) safety surveillance of medicines and vaccines and for populating VigiBase with country-wide adverse event (AE) report data to contextualize national safety data with international data. 2 Although a member of the WHO Program for International Drug Monitoring since 2010, 8 Côte d’Ivoire does not have PV as a routine activity. 9 Up to 2015, only 28 ICSRs were submitted from Côte d’Ivoire to VigiBase 10 despite previous active PV investigations due to serious suspected adverse drug reactions (ADRs), such as blackwater fever and hepatonephritis associated with antimalarial drugs in the late 1990s and 2008–2012.11,12 One of the main reasons for underreporting was a lack of knowledge among healthcare professionals (HCPs) of the AE reporting procedure.9,11
Subsequent efforts by the WHO, government, and funding partners led to the establishment of the Vigilance Unit, designated PV focal points within healthcare facilities, and training and awareness campaigns on PV. This included the PV enhancement project, implemented in the Abidjan region of Côte d’Ivoire from September 2018 to February 2020 to improve routine reporting of AEs by training and mentoring HCPs.13,14 This pilot project was initiated via a partnership between GSK, the nongovernmental organization PATH, the Ministry of Health, the national health authority, and the Vigilance Unit.13,14 During the 18-month project, 1427 HCPs were trained and mentored and 361 AE reports were delivered nationwide, as opposed to 33 reports in the 8 months before implementation. 14 However, a basic assessment of quality showed only 69% of reports from Abidjan contained mandatory information on notifier, patient, event, and suspected product. Also, causality assessments (CAs) to determine the relationship between medicinal product and AE occurrence were conducted for few AEs (15%), 14 with implications for timely safety signal detection.
Assessment of AE report quality enables the identification of reports with the greatest potential to contribute to signal detection. This may be supported by computerized systems for data input 15 and systematic scoring methodologies, such as the vigiGrade completeness score, which was developed by the UMC as a quantitative method for measuring the completeness of clinically relevant information in ICSRs in VigiBase for CAs. 16 However, in countries without the expertise or resources to implement such methods, simpler qualitative methods have been used for manual review of AE report quality. This includes a system developed by Professor Jürgen Beckmann (previous member of WHO Expert Advisory Panel on Medicine Safety; Berlin, Germany), which considers report quality as a continuous variable, with (like vigiGrade) no cut-off for assessment, enabling CAs to be performed even when the quality is poor (Professor Jürgen Beckmann, personal communication). This provides a way forward for more detailed investigations by regulatory authorities if a safety signal is suspected.
We report the results of additional investigations into spontaneous AE reports received by the Côte d’Ivoire Vigilance Unit between January 2019 and February 2020. Report quality was assessed via the Beckmann system, modified in-house to include quality ratings, and in-depth CAs were conducted for each report, where possible.
Methods
AE reports included in the analysis
This descriptive, retrospective analysis was performed between November 2020 and April 2021 on AE reports received at the AIRP Vigilance Unit, Abidjan city, and notified between January 2019 and February 2020 during the PV enhancement project, 14 from HCPs mostly in the Abidjan region where the project was implemented but also other regions in Côte d’Ivoire. An AE reporting form was used to collect identifiable information on the notifier, patient, suspected drug, and AE, as well as other information, such as concomitant medication and medical history (see Supplemental File 1). The reports of suspected AEs routinely entered into the Côte d’Ivoire PV database were anonymized. Under local regulatory guidelines for retrospective analyses of routinely collected, de-identified data, 17 ethical approval and an Institutional Review Board consent waiver were not required. Informed consent was also not required for this database inquiry.
A total of 141 AE reports were received during the analysis period and verified. Of these, 118 were for suspected ADRs, 7 for AEs following immunization (AEFIs), and 16 for unspecified health products. The quality assessment method used was only suitable for ADRs. Therefore, the 118 suspected ADR reports were analyzed, in which 181 drugs were identified, including multiple drugs (63) in 35 reports; only the main incriminating drug was considered.
Quality assessment
AE report quality was assessed using a version of the method developed by Professor Beckmann, referred to hereafter as the Beckmann method, which was modified in-house to include quality ratings to avoid classification ambiguities. The information included in the AE reports was categorized as follows:
M: minimum necessary identifiable information on the notifier, patient, suspected drug, and AE, including at least the age and/or weight and sex of the patient, the name of the HCP/primary reporter, the name of the main suspected product, and type of AE (ADR/other);
C: chronology of drug treatment, that is, time to AE onset (date drug treatment started, date of AE onset), with complementary information on dechallenge upon drug withdrawal and/or date of rechallenge;
A: alternative causes, including at least one confounding factor, such as concomitant medications, underlying illness, or relevant medical history;
P: at least one plausible pharmacological mechanism of AE occurrence, such as drug mechanism, dosage, and plasma level, or results of etiological/biological examinations.
These categories were combined to provide four levels of quality plus an “insufficient” rating, taking into account relevance for the CA:
Very good quality. M, C, A, and P information are reported;
Good quality. At least M and C, and information on one other element (A or P) are reported;
Average quality. M and information on one other element (C, A, or P) are reported;
Poor quality. Only M information is reported, with limited relevant information. C, A, and P information is incomplete;
Insufficient. M information is incomplete (insufficient) or is irrelevant (for example, patient bed number).
Causality assessment
The widely used WHO-UMC system for CA18,19 and the official French CA method 20 were used for standardized case CA (see Supplemental Files 2 and 3 for further details on both methods).
The WHO-UMC CA method is based on the chronological relationship between drug administration and AE, and with drug withdrawal and reintroduction, the medical or pharmacological probability of causation based on clinical signs and symptoms, laboratory tests, and pathological data, and the pharmacological mechanism of AE occurrence, and exclusion of another drug or non-drug cause. Combination of these criteria leads to six causality categories: certain, probable/likely, possible, unlikely, conditional/unclassified, and unassessable/unclassifiable. 18
The French CA method, which was updated in 2011 by Arimone et al., 20 is often used to complement the WHO-UMC method in French-speaking countries. This CA is based on three chronological (C) criteria (time relationship to drug intake; timing of response after drug withdrawal and to drug rechallenge) and four semiological (S) criteria (signs and symptoms suggestive of drug role; contributing factors [setting]; results of additional complementary investigations; results of investigations of nondrug etiology). These were used to calculate an intrinsic accountability score of I0–I6, corresponding to increasing levels of incrimination of the drug to the event (see Supplemental File 3).
Statistical analysis
The quality analyses and CAs were conducted during weekly meetings of national clinical PV experts involved in the establishment of surveillance policy and good PV practices in Côte d’Ivoire. The experts were from the Bouaké University Teaching Hospital (Centre Hospitalier Universitaire (CHU) de Bouaké) Pharmacology Department, Abidjan Heart Institute (Institut de Cardiologie d’Abidjan) Medical Unit, Cocody University Hospital (CHU de Cocody) Pharmacology Department, and AIRP Vigilance Unit. A consensus was reached when at least 80% of the expert panel members agreed on the quality rating and CA rating for each AE report.
An Excel spreadsheet was used for PV data entry, and this was analyzed using Epi Info version 7 software. The impact of report quality on the CA was assessed by Yates corrected Chi-square test.
We used the Standards for Reporting Qualitative Research guidelines 21 and checklist 22 to draft this manuscript (see Supplemental File 4 for the completed checklist).
Results
General description of AE reports
Of the 118 AE reports eligible for analysis, 104 (88.1%) were from Abidjan and 14 (11.9%) were from other regions in Côte d’Ivoire. Sixty-eight reports (57.6%) were made by medical doctors, 23 (19.5%) by nurses, 12 (10.2%) by midwives, and 3 (2.5%) by pharmacists; 12 (10.2%) reports did not specify the notifier’s profession. Almost two-thirds of AE reports (76; 64.4%) were for female patients and 83 (70.3%) were for patients aged 10 years or older.
Information on concomitant medicinal treatment was only included in 29.7% of reports, underlying illness in 24.6%, date of drug rechallenge in 14.4%, and outcome after drug rechallenge in 14.4% of reports (Table 1). Information on pharmacological mechanism and etiology, which was recorded in 28 (23.7%) and 27 (22.9%) reports, respectively (Table 1), was relevant to mechanism of action in only four and three of these reports, respectively.
Information included in the AE reports.

AE, adverse event; HCP, healthcare professional; N, total number of AE report forms; n (%), number (percentage) of AE report forms in category.
Quality assessment by modified Beckmann method
Report quality was assessed as very good for 5 (4.2%) reports, good for 23 (19.5%) reports, average for 74 (62.7%) reports, and poor for 12 (10.2%) reports (Figure 1; Table 2). The 28 very good/good quality reports contained information on all four minimum criteria (notifier, patient, suspected drug, and AE), and chronology information on drug start, AE onset, drug start, and drug withdrawal were included in at least 96.4% of reports, while the outcome after withdrawal, date of rechallenge, and outcome after rechallenge were included in 24 (85.7%), 16 (57.1%), and 16 (57.1%) reports, respectively (Table 2). Information on alternative causes was included in 18 (concomitant treatment; 64.3%) and 11 (underlying illness; 39.3%) very good/good quality reports (Table 2).

Quality of the 118 adverse event (AE) reports according to the modified Beckmann method.
Analysis of variables included in AE reports, according to quality category determined using the modified Beckmann method.
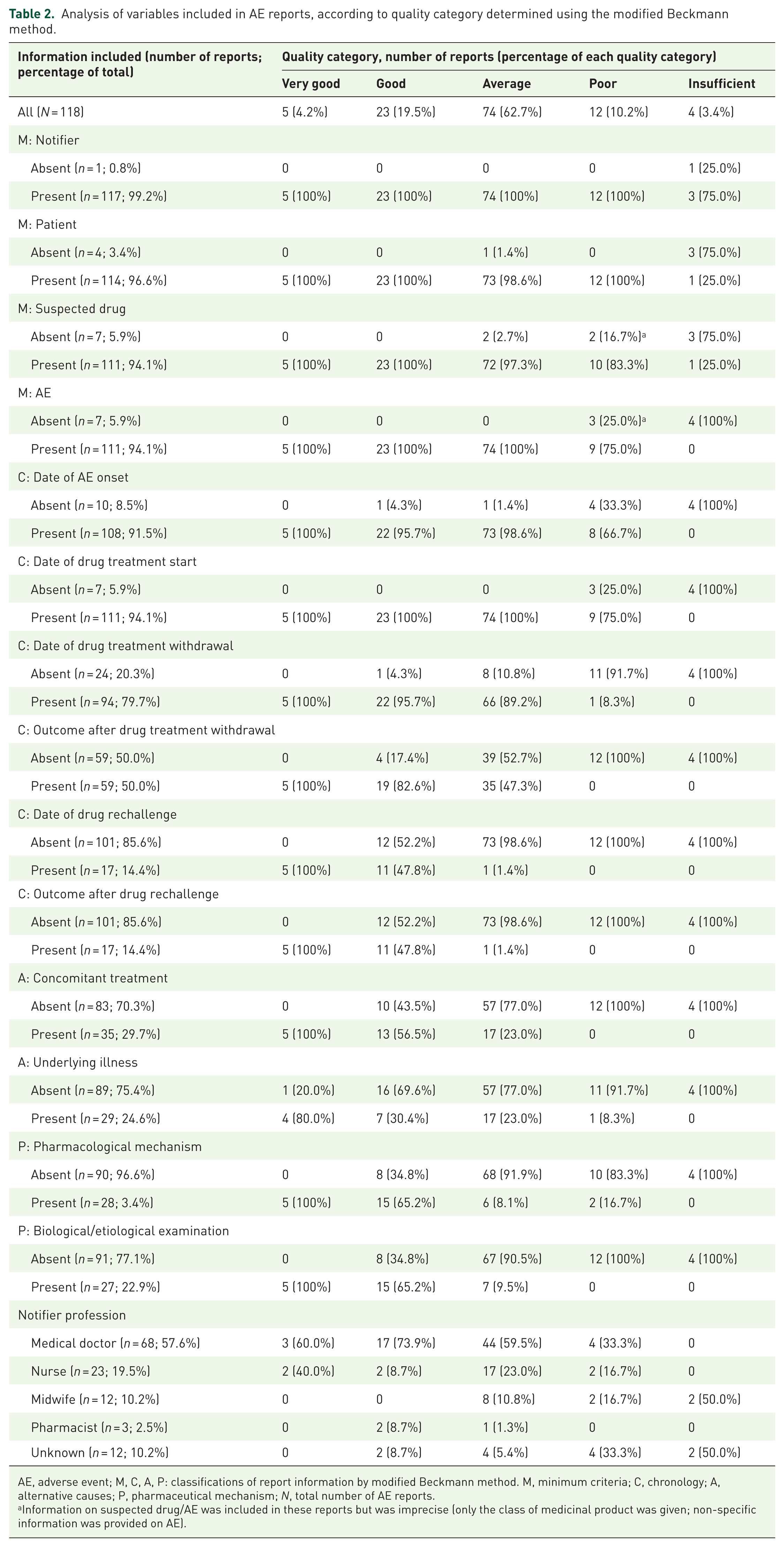
AE, adverse event; M, C, A, P: classifications of report information by modified Beckmann method. M, minimum criteria; C, chronology; A, alternative causes; P, pharmaceutical mechanism; N, total number of AE reports.
Information on suspected drug/AE was included in these reports but was imprecise (only the class of medicinal product was given; non-specific information was provided on AE).
Of the 68 reports made by doctors and 23 reports made by nurses, 20 (29.4%) and 4 (17.4%), respectively, were very good/good quality. Of three AE reports submitted by pharmacists, two were good and one had average quality and, of the 12 reports submitted by midwives, none were very good/good quality, 8 (66.7%) were average quality, and 4 (33.3%) had poor/insufficient quality (Table 2).
Most average quality reports did not include information on rechallenge, alternative causes, pharmaceutical mechanism, or biological/etiological examinations (Table 2). All 12 poor quality reports contained minimum required information, although two lacked precise information on the suspected drug and three lacked precise information on the AE (Table 2). Nine poor quality reports had information on the date of drug treatment start and eight had information on date of AE onset.
WHO-UMC causality assessment by report quality
With the WHO-UMC method, the CA was certain for 16 (13.6%) AE reports, probable/likely for 49 (41.5%), possible for 45 (38.1%), and unlikely for 4 (3.4%) (Table 3). The time relationship to drug intake was plausible for 18 (15.2%) reports, reasonable for 92 (78.0%), improbable for 4 (3.4%), and unclassifiable or unassessable for 4 (3.4%) reports categorized as “insufficient quality.”
WHO-UMC CA ratings 18 according to AE report quality.

AE, adverse event; CA, causality assessment; N, total number of AE reports; WHO-UMC, World Health Organization-Uppsala Monitoring Center.
For the 114 reports for which a CA could be made, 5 (31.3%) of 16 with a certain WHO-UMC causality rating had good quality and 11 (68.8%) had average quality. Of the 94 reports with a probable/possible WHO-UMC causality rating, 17 (18.1%) had good quality and 63 (67.0%) had average quality. There was no significant difference in distribution of the certain/probable and possible/unlikely causality rating by report quality (very good/good, 13 vs 15; average, 45 vs 29; poor, 7 vs 5; p = 0.42).
French causality assessment by report quality
The chronology score for the 118 evaluable AE reports was C1 (doubtful) for 43 (36.4%), C2 (plausible) for 53 (44.9%), C3 (likely) for 15 (12.7%), and C0 (role of drug excluded) for 3 (2.5%) reports; 4 (3.4%) reports classified as “insufficient quality” were not assessable. The semiological score was S1 (doubtful) for 94 (79.7%), S2 (plausible) for 13 (11.0%), S3 (likely) for 6 (5.1%), and S0 (role of drug excluded) for 1 (0.8%) report.
Intrinsic causality was I0 (role of drug excluded) for 4 (3.4%) reports; two were good quality and two were poor quality (Table 4). The rating was I1/I2 (doubtful causality) for 82 (69.5%) reports, of which 55 (67.1%) were average quality. Twenty-eight reports (23.7%) were in the stronger causality categories (I3–I6), of which 19 (67.9%) had average quality (Table 4). There was no significant difference in distribution of causality scores ⩽I1 and scores I2–I6 by report quality (very good/good, 10 vs 18; average, 26 vs 48; poor/insufficient, 5 vs 7; p = 0.91).
French CA ratings 20 according to AE report quality.

I0 (role of drug excluded) to I6 (drug strongly incriminated), intrinsic causality rating.
AE, adverse event; CA, causality assessment; N, total number of AE reports.
Discussion
This was the first in-depth analysis of the quality of AE reports notified in a sub-Saharan country, Côte d’Ivoire, and the impact on the CA. Although the Côte d’Ivoire Vigilance Unit receives AE reports from all regions, 104 of the 118 reports notified between January 2019 and February 2020 were from Abidjan, suggesting underreporting from other parts of the country but also reflecting the positive impact of the PV enhancement project implemented in the Abidjan region during this period. 14 This indicates that the PV training and mentoring program should be extended to all parts of Côte d’Ivoire, along with broader strategies to strengthen national PV systems in a resource-limited country.4,23 -26
Most reports (57.6%) were made by medical doctors, 19.5% by nurses, and 10.2% by midwives, with only three reports (2.5%) made by pharmacists. This was broadly in line with the origin of reports during the complete PV enhancement project. 14 Of 28 very good/good quality reports, 20 were made by doctors, four by nurses, and two by pharmacists; no very good/good quality reports were submitted by midwives. Since most AE reports submitted by doctors, nurses, and midwives had average quality, it is clearly important to emphasize the need for good quality AE notifications among all HCPs, irrespective of profession.
In our analysis, AE reports were first evaluated via the identification of essential information on notifier, patient, suspected drug, and AE.27,28 One report did not include any notifier information and for 12 (10.2%) reports, the notifier’s profession was not given. This and the absence of patient information on age, sex, and weight (11.0%, 1.7%, and 7.6% of reports, respectively) and on the suspected drug (5.9% of reports) has implications for the utility of AE reports and prompt identification of safety signals.3,29 However, in LMICs such as Côte d’Ivoire, a pragmatic approach is often required toward incomplete report forms. For example, it may be feasible to infer notifier and patient profiling information from secondary data on the report form, such as the hospital name, which might suggest the likely notifier, or the patient’s occupation might help determine their likely age group and sex. This enables a proportion of incomplete reports to be put forward for further investigation, such as CA.
Assessment of AE report quality with the modified Beckmann method showed 23.7% had very good/good quality, 62.7% were average, and 10.2% had poor quality. Most average quality reports lacked information on rechallenge, concomitant treatment, underlying illness, and pharmacological and biological/etiological mechanisms. The latter was included in less than one-quarter of reports, and most of the information included did not enable the possible mechanism of action to be determined. This underlines the importance of sensitizing HCPs on the need to provide a sufficiently complete medical history for each case when reporting AEs, as well as verifiable information on potential mechanism, although the difficulty in obtaining this information, particularly in LMICs, 3 has to be acknowledged. Additionally, we admit that inclusion of the drug rechallenge category could be seen as problematic since rechallenge of a suspected medicine may not be applicable for ethical reasons. On the other hand, rechallenge data can help to fine-tune the CA, although these are usually absent from AE reports; in our analysis, only 14.4% of reports included rechallenge information.
For the CA, we used the WHO-UMC 18 and updated French 20 methods in which the assessment is conducted by clinical experts. 30 Ideally, these processes use good quality AE report information to enable confident CA and to avoid misunderstandings and disagreements among assessors. 31 In our analysis, CAs were performed for all reports except four with insufficient information (three had no information on patient or suspected drug; all four had no information on the AE). The reliability of the CA for the 12 poor quality reports was questionable since two had imprecise information on the suspected drug, three had imprecise AE information, none had information on concomitant treatment, and 11 had no information on underlying illness (Tables 2 and 3). However, it is worth noting that nine poor quality reports included the date of drug treatment start and eight included the date of AE onset, information that is important for the CA.18,20,32 In real-world situations, it is important to identify data that enables CAs to be performed with sufficient certitude; it may be feasible to perform CAs on an incomplete AE report, particularly if the available data indicate the likely timeframe of the AE. Therefore, even with a poor quality report, there may be enough relevant information to perform a CA as a first step in the signal detection process and complementary AE information may be obtained subsequently to confirm the CA rating. Moreover, most of the cases analyzed were in the ‘doubtful or possible’ causality categories, possibly because a lack of good quality reports prevented more definite CAs, but this cannot be confirmed. Overall, it can be assumed that the more complete an AE report is, the better the quality and the more credible (with a higher probability) the CA outcome. This is obviously important for reliable pharmacovigilance. Similar challenges in spontaneous reporting systems linked to reporting biases and differences in data sources have been shown to influence the analysis and interpretation of safety signals.3,33 -35
Limitations
This analysis of AE reports was limited partly because of logistical reasons associated with transmission and processing procedures that prevented the inclusion of more reports in the sample, and because AEFIs were excluded since the quality method used was not suitable for their analysis. Other limitations included absent, illegible, ambiguous, or imprecise report information on the AE and/or product, and the use of incomprehensible abbreviations. Also, the CA began 8 months after receiving the AE reports because of a lack of stable funding, impeding prompt follow-up. We also acknowledge that the use of different CA methods, as in this analysis, can lead to different results because of subjective variations. 36 Finally, most AE reports were submitted by HCPs in the Abidjan region who (as explained in the section “Methods”) were trained and mentored in AE reporting during the PV enhancement project, so the report quality may not be representative of AE reports from the whole country.
Conclusion
As in other LMICs, the infrastructure of the PV system in Côte d’Ivoire needs to be strengthened through various approaches. This analysis focused on the quality of AE reports received at the AIRP Vigilance Unit. Good quality AE reports are crucial for an accurate CA in PV, which can lead to signal detection, although enough relevant information may be available in reports of poorer quality for a preliminary CA. The results of this analysis highlight the need for further training and mentoring of HCPs in Côte d’Ivoire to, first, increase the number of notifications throughout the country and, second, to improve the quality and completeness of AE reports submitted to the central Vigilance Unit. Simplified methods of analyzing AE reports are required in LMICs that also help identify relevant information for reliable CAs.
Supplemental Material
sj-docx-1-taw-10.1177_20420986261446480 – Supplemental material for A descriptive, retrospective analysis of the quality of spontaneous adverse event reporting to the Côte d’Ivoire Pharmaceutical and Regulatory Authority and its impact on the causality assessment
Supplemental material, sj-docx-1-taw-10.1177_20420986261446480 for A descriptive, retrospective analysis of the quality of spontaneous adverse event reporting to the Côte d’Ivoire Pharmaceutical and Regulatory Authority and its impact on the causality assessment by Mamadou Kamagaté, Viviane Jusot, Diaby Mory, Amadou Barry, Félix Adou, Martha Kirabo, Teodora Perger and Yolanda Guerra Mendoza in Therapeutic Advances in Drug Safety
Supplemental Material
sj-docx-2-taw-10.1177_20420986261446480 – Supplemental material for A descriptive, retrospective analysis of the quality of spontaneous adverse event reporting to the Côte d’Ivoire Pharmaceutical and Regulatory Authority and its impact on the causality assessment
Supplemental material, sj-docx-2-taw-10.1177_20420986261446480 for A descriptive, retrospective analysis of the quality of spontaneous adverse event reporting to the Côte d’Ivoire Pharmaceutical and Regulatory Authority and its impact on the causality assessment by Mamadou Kamagaté, Viviane Jusot, Diaby Mory, Amadou Barry, Félix Adou, Martha Kirabo, Teodora Perger and Yolanda Guerra Mendoza in Therapeutic Advances in Drug Safety
Supplemental Material
sj-docx-3-taw-10.1177_20420986261446480 – Supplemental material for A descriptive, retrospective analysis of the quality of spontaneous adverse event reporting to the Côte d’Ivoire Pharmaceutical and Regulatory Authority and its impact on the causality assessment
Supplemental material, sj-docx-3-taw-10.1177_20420986261446480 for A descriptive, retrospective analysis of the quality of spontaneous adverse event reporting to the Côte d’Ivoire Pharmaceutical and Regulatory Authority and its impact on the causality assessment by Mamadou Kamagaté, Viviane Jusot, Diaby Mory, Amadou Barry, Félix Adou, Martha Kirabo, Teodora Perger and Yolanda Guerra Mendoza in Therapeutic Advances in Drug Safety
Supplemental Material
sj-docx-4-taw-10.1177_20420986261446480 – Supplemental material for A descriptive, retrospective analysis of the quality of spontaneous adverse event reporting to the Côte d’Ivoire Pharmaceutical and Regulatory Authority and its impact on the causality assessment
Supplemental material, sj-docx-4-taw-10.1177_20420986261446480 for A descriptive, retrospective analysis of the quality of spontaneous adverse event reporting to the Côte d’Ivoire Pharmaceutical and Regulatory Authority and its impact on the causality assessment by Mamadou Kamagaté, Viviane Jusot, Diaby Mory, Amadou Barry, Félix Adou, Martha Kirabo, Teodora Perger and Yolanda Guerra Mendoza in Therapeutic Advances in Drug Safety
Footnotes
Acknowledgements
The authors would like to thank the pharmacovigilance focal points in the district of Abidjan, Autorité Ivoirienne de Régulation Pharmaceutique (AIRP) and its Director, Dr Coulibaly Assane, who facilitated the access to data and financing of this analysis, and GSK and PATH for financing and technical support. We also thank Professor Jürgen Beckmann, pharmacologist (Berlin, Germany), for permission to use his quality assessment method and his additional explanations, and the Institut de Cardiologie d’Abidjan (ICA) and its Director, Professor Kramoh Euloge, for the analysis of cases by its pharmacovigilance team, particularly Professor Djénamba Bamba-Kamagaté. The authors thank Akkodis Belgium for editorial assistance, manuscript coordination, and design support on behalf of GSK. Joanne Knowles (independent medical writer) provided medical writing support.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.