
Abstract
Background:
An increasing number of breast cancer patients are using statins concomitantly. However, there are relatively few safety studies on the association between statins and adverse events (AEs) during breast cancer treatment.
Objective:
This study aims to systematically evaluate the disproportionality signals associated with statin use and the reporting of AEs across different system organ classes (SOCs) in breast cancer patients.
Design:
This is a pharmacovigilance disproportionality analysis based on the U.S. Food and Drug Administration’s (FDA) Adverse Event Reporting System database.
Methods:
All AE reports related to breast cancer from the 2004 Q1 to 2024 Q3 were extracted. Disproportionality analysis was performed using reporting odds ratios (RORs) to detect potential safety signals associated with statin use. Multivariate logistic regression model was used as a secondary analysis to adjust for potential confounders, including age, gender, and therapeutic drugs.
Results:
A total of 237,868 breast cancer-related AE reports were identified, of which 8,223 involved concomitant statin use. Statin use was associated with lower RORs of hepatobiliary (ROR: 0.60, 95% CI: 0.52–0.68), and blood and lymphatic system disorders (ROR: 0.62, 95% CI: 0.57–0.67). In contrast, higher RORs were observed for skin and subcutaneous tissue (ROR: 1.75, 95% CI: 1.67–1.84), psychiatric (ROR: 1.95, 95% CI: 1.82–2.08), renal and urinary (ROR: 2.03, 95% CI: 1.85–2.22), musculoskeletal and connective tissue (ROR: 1.48, 95% CI: 1.40–1.58), infections and infestations (ROR: 1.25, 95% CI: 1.18–1.34), metabolism and nutrition (ROR: 1.25, 95% CI: 1.16–1.35), gastrointestinal (ROR: 1.10, 95% CI: 1.05–1.16), vascular (ROR: 1.26, 95% CI: 1.16–1.37), nervous system (ROR: 1.20, 95% CI: 1.13–1.27), respiratory, thoracic and mediastinal disorders (ROR: 1.07, 95% CI: 1.00–1.14).
Conclusion:
In breast cancer patients receiving statins concomitantly, specific disproportionality signals were observed across multiple SOCs. These findings highlight the need for individualized monitoring strategies and further mechanistic studies to clarify the underlying pathways and optimize clinical risk management.
Plain language summary
Why was this study done? Statins are medicines commonly used to lower cholesterol and protect the heart. Many people with breast cancer also take statins because of age or other health problems. However, it is not clear whether statins change the risk of side effects caused by cancer treatment. Understanding this relationship could help doctors and patients make safer medication choices. What did the researchers do? Researchers analyzed safety reports from the U.S. Food and Drug Administration’s Adverse Event Reporting System (FAERS). These reports describe possible side effects that patients or healthcare professionals have observed. The team looked at more than 230,000 reports related to breast cancer between 2004 and 2024, and compared those involving statin use with those that did not. They used statistical analysis to see whether taking statins was linked to more or fewer side effects in different body systems. What did the study find? Among all reports, about 8,223 involved statin use. The results showed that statin use was associated with lower reporting odds ratios of hepatobiliary and blood and lymphatic disorders, whereas higher reporting odds ratios were observed for renal and urinary, musculoskeletal and connective tissue, infections and infestations, metabolism and nutrition, gastrointestinal, vascular, nervous system, and respiratory, thoracic and mediastinal disorders. What do the findings mean? For people with breast cancer who also take statins, it is important to monitor for specific types of side effects and adjust treatments when needed. Doctors may consider closer follow-up for mood changes, skin reactions, or kidney problems. More studies are needed to understand how statins interact with cancer treatments and to guide safer, more personalized care.
Introduction
According to data from GLOBOCAN 2020, female breast cancer has surpassed lung cancer to become the most common cancer globally, accounting for 11.7% of all new cancer cases and resulting in over 2 million cases and 684,996 deaths. 1 Currently, the treatment regimens for breast cancer mainly include surgery, radiotherapy, chemotherapy, endocrine therapy, targeted therapy, and immunotherapy. 2 These treatments have significantly improved the survival rate of breast cancer patients; however, attention should be paid to treatment-related adverse events (AEs). Severe AEs may lead to treatment interruption or reduced compliance, thereby affecting therapeutic outcomes and survival time. With the extension of the survival period of breast cancer patients, the management of treatment-related long-term sequelae and the focus on patients’ quality of life have become increasingly important. 3
Some studies have shown that approximately 32%–42% of breast cancer patients had comorbidities at the time of diagnosis. 4 The most common ones are hypertension, followed by other cardiovascular diseases and type 2 diabetes. Therefore, most breast cancer patients need to use other medications concomitantly during treatment, including statins. Statins are currently widely used for the prevention and management of cardiovascular diseases. Some studies have suggested that statins may enhance the efficacy of certain anti-tumor therapies, such as immune checkpoint inhibitors, 5 and statin use is associated with reduced breast cancer-specific mortality and improved overall survival rates,6,7 although this association remains controversial.8,9 Nevertheless, there are relatively few safety studies on the association between statins and AEs during breast cancer treatment. In the large population of breast cancer patients who have received statins, the impact of these drugs on AEs remains unclear.
Therefore, this study utilized the database records from the U.S. Food and Drug Administration’s (FDA) Adverse Event Reporting System (FAERS) to examine the reporting patterns of AEs associated with statin co-use in breast cancer patients receiving different therapeutic regimens, including chemotherapy, endocrine therapy, targeted therapy, and immunotherapy. The FAERS is a publicly accessible, voluntary reporting database and serves as an important resource for drug safety monitoring, enabling large-scale analysis of adverse drug reactions in real-world clinical settings. 10 This study aimed to systematically characterize the disproportionality signals related to statin use in breast cancer, thereby providing evidence that may assist clinicians in the evaluation and monitoring of concomitant medication safety.
Methods
Data source
This study is a pharmacovigilance disproportionality analysis based on the FAERS database, which is an open-access resource managed by the FDA. The study design and reporting adhered to the READUS-PV guidelines to ensure methodological transparency and reproducibility. 11 We extracted cases from FAERS spanning from the first quarter of 2004 to the third quarter of 2024, where any “drug indication” included the terms “breast cancer” or “breast carcinoma”. We downloaded the original data and constructed a cohort of breast cancer patients (accessed on December 20, 2024). All relevant original data were obtained through the FAERS official website and were then organized into an analyzable dataset according to a standardized protocol.
Data processing procedure
First, duplicate reports obtained from the FAERS database were removed. The detailed screening process is shown in Figure 1. The duplicate values were removed by applying case identification number (CASEID). Additionally, reports with the same values for parameters such as gender, age, country, date of AE, adverse reaction, drug, and indication were also identified as duplicate reports. Subsequently, reports lacking crucial information, such as missing descriptions of AEs or records with incomplete suspected drug information, were excluded. We refined and standardized the “generic name” field, unified the naming of drugs, and excluded reports that did not contain any breast cancer treatment drugs (Supplemental Table 1) in either the suspected drugs or concomitant medications. Breast cancer treatment drugs are classified into four major categories based on their therapeutic mechanisms: chemotherapy drugs, endocrine therapy drugs, targeted therapy drugs, and immunotherapy drugs. For subgroup analyses stratified by anticancer therapy type, reports were categorized based on the presence of specific drug classes. Patients who received multiple types of anticancer therapies (e.g., concomitant chemotherapy and targeted therapy) were assigned to all corresponding treatment groups. This non-mutually exclusive approach ensures that each therapy type subgroup captures all reports involving that class of drugs, reflecting the complexity of real-world treatment regimens where combination therapies are common. Consequently, the same report may contribute to multiple subgroup analyses. Statin exposure was defined based on the presence of statins (including atorvastatin, rosuvastatin, simvastatin, lovastatin, pravastatin, fluvastatin, and pitavastatin) recorded as concomitant or suspect drugs in FAERS reports. Reports containing any of these statins were classified as the statin group, while those without any recorded statin use were assigned to the non-statin group, regardless of whether other lipid-lowering agents were present. We uniformly encoded the AEs mentioned in the report according to the Medical Dictionary for Regulatory Activities (MedDRA; version 25.1; MedDRA Maintenance and Support Services Organization, MSSO). MedDRA employs a five-level hierarchical structure, with the basic unit being “Preferred Terms” (PTs), which are used to describe a single medical event or diagnosis. Based on the PTs, further classification can be made into “high-level terms” and “high-level group terms,” and ultimately categorized under the top-level “system organ classes” (SOCs). SOCs are used to summarize and classify AEs according to the cause, location or functional system, to support subsequent systematic analysis.

The flow chart of screening AEs for patients with breast cancer from 2004Q1 to 2024Q3 in the FAERS database.
Statistical analysis
Given the spontaneous nature of the FAERS database, the primary statistical approach in this study was disproportionality analysis using the reporting odds ratio (ROR), which is the standard method for signal detection in spontaneous reporting systems. For each SOC, a 2 × 2 contingency table was constructed comparing the number of reports of a specific AE between statin users and non-statin users. The formulas and thresholds are provided in Table 1. To evaluate the potential impact of competition bias on disproportionality signals, a sensitivity analysis was conducted by excluding reports containing statin-related high-frequency AEs. Specifically, reports with PTs including myopathy, rhabdomyolysis, myalgia, blood creatine phosphokinase increased were identified and removed from the dataset. After exclusion, disproportionality analyses were repeated using RORs for each SOC.
The algorithm used in this study.
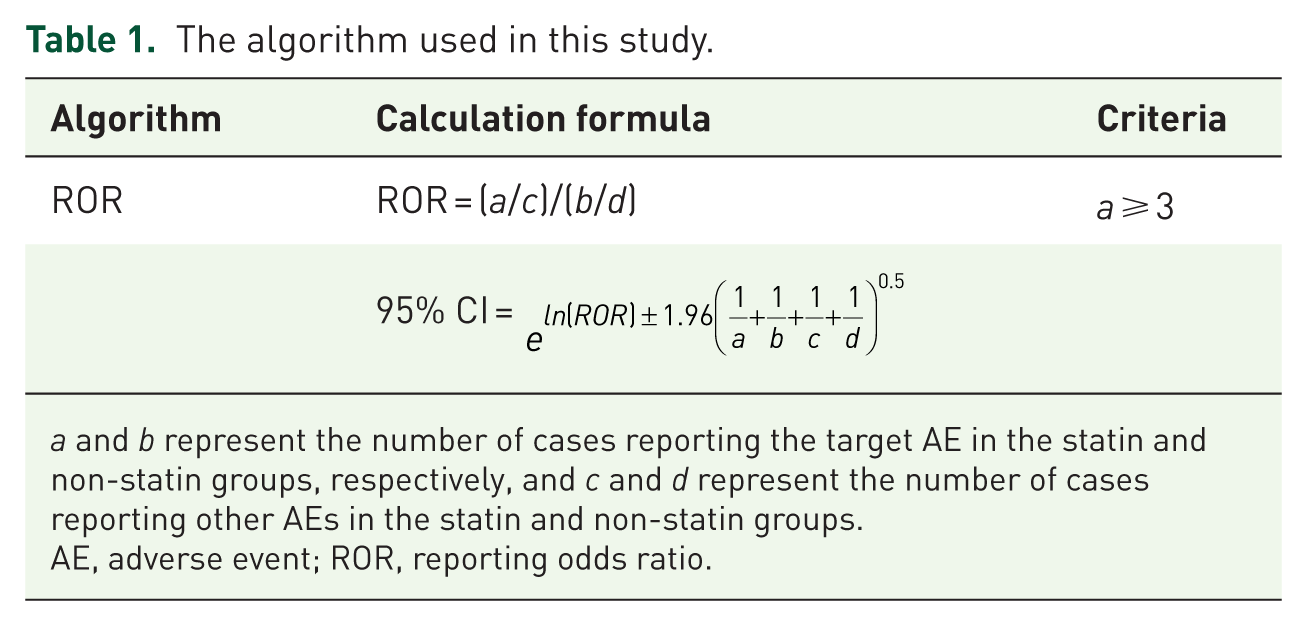
a and b represent the number of cases reporting the target AE in the statin and non-statin groups, respectively, and c and d represent the number of cases reporting other AEs in the statin and non-statin groups.
AE, adverse event; ROR, reporting odds ratio.
To further explore whether the disproportionality signals remained after adjusting for potential confounders, a multivariable logistic regression model was applied. The main outcome was the reporting of specific AEs (coded as SOC). The independent variable was concomitant statin use. Covariates included age, gender, and therapeutic drugs to control for confounding factors. To address the multiple comparison problem arising from repeated hypothesis testing of AEs classified by multiple SOC categories, Benjamini-Hochberg method to adjust the false discovery rate (FDR) for p-values in the regression analysis was applied to all subgroup analyses. Specifically, the p.adjust function provided by the stats package in R was used to adjust all the original p-values. The FDR-adjusted p-values were used to determine statistical significance. The FDR-adjusted p-value less than 0.05 (FDR p < 0.05) in a two-sided test was considered statistically significant. The analysis was conducted using R software version 4.4.3 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Report screening and patient characteristics
The report screening process is shown in Figure 1. During the period from Q1 2004 to Q3 2024 in the FAERS database, a total of 18,700,413 reports were collected. Among these, 269,845 reports containing “breast cancer” or “breast carcinoma” in any “drug indication” were selected. After removing duplicate reports, excluding reports lacking key information and reports whose drug information did not include any breast cancer treatment medications, 237,868 reports were finally retained. Among these, the medication information in 8,223 reports contained statins.
The demographic and baseline characteristics of the patients are presented in Table 2. The average age of the overall population was 59.5 years; statin users were significantly older than non-users (66.2 years vs 59.2 years). In terms of gender distribution, the majority of patients were female, accounting for 92.3%; male patients accounted for 1.0%, and the remaining 6.7% had incomplete or missing gender information in the reports. Regarding the composition of therapeutic drugs, targeted therapy drugs were most frequently reported agents (67.4%), followed by chemotherapy drugs (37.1%) and endocrine therapy drugs (33.9%). Immunotherapy drugs were used in a relatively low proportion of reports, accounting for only 3.4%. In terms of regional distribution, the United States had the highest number of reports, accounting for 38.6% of all reports, followed by Germany, accounting for 5.1%, and reports from other regions were distributed across various locations. Regarding the years of adverse reaction reports, the period from 2016 to 2020 had the largest proportion of reports, accounting for 40.8%.
Clinical and treatment characteristics of breast cancer patients with reported adverse events.

Patients who received multiple types of anticancer therapies were counted in all applicable categories.
SOC distribution of AEs
Figure 2 presents the SOC distribution of AEs. Among breast cancer patients not receiving statin therapy, the gastrointestinal system was the most frequently implicated SOC in reported AEs, followed by the skin and subcutaneous tissue system, and the nervous system. Conversely, in patients on statin therapy, the skin and subcutaneous tissue system was the most frequently reported AE, followed by the gastrointestinal system and the nervous system, showing a slight difference in distribution compared to non-statin users. Regardless of statin use, the endocrine system was the least frequently implicated SOC.

Distribution of reported cases in the FAERS database by SOC and statin use.
Association between statin use and AEs reporting across SOCs in breast cancer patients
The RORs for AEs associated with statin co-use in breast cancer patients were calculated across all SOC categories (Table 3). Statin use showed elevated disproportionality signals for several SOCs, including skin and subcutaneous tissue, psychiatric, renal and urinary, musculoskeletal and connective tissue, infections and infestations, metabolism and nutrition, gastrointestinal, vascular, nervous system and respiratory, thoracic and mediastinal disorders. In contrast, statin co-use was associated with lower RORs for several SOCs, including blood and lymphatic system and hepatobiliary disorders. The results of a multivariate logistic regression analysis for total breast cancer patients after adjusting for age, gender, and treatment drugs showed that differences in AE reporting across several SOCs were observed between statin users and non-users (Supplemental Figure 1). Statin use was associated with lower RORs of AEs in hepatobiliary (aOR: 0.59, 95% CI: 0.50–0.68), blood and lymphatic system (aOR: 0.61, 95% CI: 0.56–0.67), immune system (aOR: 0.80, 95% CI: 0.67–0.97), eye (aOR: 0.82, 95% CI: 0.71–0.95) and cardiac disorders (aOR: 0.83, 95% CI: 0.75–0.93); while with higher RORs of AEs were observed in skin and subcutaneous tissue (aOR: 1.87, 95% CI: 1.77–1.98), psychiatric (aOR: 1.74, 95% CI: 1.61–1.87), renal and urinary (aOR: 1.69, 95% CI: 1.53–1.88), musculoskeletal and connective tissue (aOR: 1.13, 95% CI: 1.05–1.21), infections and infestations (aOR: 1.13, 95% CI: 1.05–1.21), metabolism and nutrition (aOR: 1.11, 95% CI: 1.02–1.21) and gastrointestinal disorders (aOR: 1.08, 95% CI: 1.02–1.15).
Disproportionality analysis of SOC-level AE reporting by statin use in breast cancer patients.

AE, adverse event; ROR, reporting odds ratio; SOC, system organ class.
To explore the impact of statins on AEs under various breast cancer treatment drugs, we conducted subgroup analyses based on the treatment medications. Table 4 showed the results in patients undergoing chemotherapy. Statin use elevated disproportionality signals for skin and subcutaneous tissue, psychiatric, renal and urinary, infections and infestations, and metabolism and nutrition disorders. In contrast, statin co-use was associated with lower RORs for respiratory, thoracic and mediastina, nervous system, cardiac, immune system, vascular, hepatobiliary, blood and lymphatic, and endocrine disorders. The results of a multivariate logistic regression analysis (Supplemental Figure 2) showed statin use was associated with higher RORs of AEs in the skin and subcutaneous tissue (aOR: 2.04, 95% CI: 1.86–2.24), psychiatric (aOR: 1.75, 95% CI: 1.56–1.96), and the renal and urinary disorders (aOR: 1.39, 95% CI: 1.12–1.72). However, statin use was significantly associated with lower RORs of AEs in 10 systems, including the endocrine (aOR: 0.31, 95% CI: 0.15–0.67), the blood and lymphatic (aOR: 0.48, 95% CI: 0.42–0.56), the hepatobiliary (aOR: 0.49, 95% CI: 0.36–0.67), the eye (aOR: 0.55, 95% CI: 0.39–0.76), the vascular (aOR: 0.63, 95% CI: 0.51–0.79), the immune system (aOR: 0.65, 95% CI: 0.44–0.96), the cardiac (aOR: 0.65, 95% CI: 0.53–0.79), the nervous system (aOR: 0.74, 95% CI: 0.64–0.83), the musculoskeletal and connective tissue (aOR: 0.76, 95% CI: 0.64–0.90), and the respiratory, thoracic and mediastinal disorders (aOR: 0.77, 95% CI: 0.67–0.89).
Disproportionality analysis of SOC-level AE reporting by statin use in breast cancer patients undergoing chemotherapy.

AE, adverse event; ROR, reporting odds ratio; SOC, system organ class.
In patients receiving endocrine therapy (Table 5), statin use elevated disproportionality signals for renal and urinary, psychiatric, vascular, infections and infestations, gastrointestinal, metabolism and nutrition, nervous system, respiratory, thoracic and mediastinal, musculoskeletal and connective tissue, and skin and subcutaneous tissue disorders. In contrast, statin co-use was associated with lower RORs for hepatobiliary, and blood and lymphatic disorders. The results of multivariate logistic regression analysis (Supplemental Figure 3) showed that statin use was significantly associated with higher RORs of AEs in the psychiatric (aOR: 1.27, 95% CI: 1.15–1.41), skin and subcutaneous tissue (aOR: 1.36, 95% CI: 1.26–1.48), and renal and urinary disorders (aOR: 1.63, 95% CI: 1.43–1.86). However, statin use was associated with lower RORs of AEs in the blood and lymphatic (aOR: 0.60, 95% CI: 0.53–0.67), hepatobiliary (aOR: 0.60, 95% CI: 0.49–0.73), eye system (aOR: 0.80, 95% CI: 0.68–0.95), and cardiac disorders (aOR: 0.84, 95% CI: 0.73–0.97).
Disproportionality analysis of SOC-level AE reporting by statin use in breast cancer patients undergoing endocrine therapy.

AE, adverse event; ROR, reporting odds ratio; SOC, system organ class.
Breast cancer patients receiving targeted therapy were classified into four groups according to the treatment medications: human epidermal growth factor receptor-2 (HER-2)-targeted therapies, cyclin-dependent kinases (CDK) 4/6 inhibitors, anti-vascular endothelial growth factor (VEGF) monoclonal antibody, and PI3K/AKT/mTOR pathway inhibitors. Among patients receiving HER-2 targeted therapy (Table 6), statin use elevated disproportionality signals for psychiatric, skin and subcutaneous tissue, renal and urinary, gastrointestinal, infections and infestations, metabolism and nutrition, and musculoskeletal and connective tissue disorders. In contrast, statin co-use was associated with lower RORs for immune system, and blood and lymphatic disorders. In addition, the results of multivariate logistic regression analysis (Supplemental Figure 4(A)) showed that statin use was significantly associated with higher RORs of AEs in the infections and infestations (aOR: 1.41, 95% CI: 1.22–1.64), gastrointestinal (aOR: 1.43, 95% CI: 1.26–1.63), renal and urinary (aOR: 2.17, 95% CI: 1.71–2.75), skin and subcutaneous tissue (aOR: 2.69, 95% CI: 2.39–3.03), and psychiatric disorders (aOR: 2.75, 95% CI: 2.15–3.53). However, statin use was significantly associated with lower RORs of AEs in the blood and lymphatic (aOR: 0.54, 95% CI: 0.44–0.67), hepatobiliary (aOR: 0.65, 95% CI: 0.46–0.91), cardiac (aOR: 0.73, 95% CI: 0.59–0.90), vascular (aOR: 0.74, 95% CI: 0.56–0.96), and nervous disorders (aOR: 0.84, 95% CI: 0.71–0.99).
Disproportionality analysis of SOC-level AE reporting by statin use in breast cancer patients undergoing HER-2 targeted therapy.

AE, adverse event; HER-2, human epidermal growth factor receptor-2; ROR, reporting odds ratio; SOC, system organ class.
Among patients receiving CDK 4/6 inhibitors therapy (Table 7), statin use elevated disproportionality signals for renal and urinary, musculoskeletal and connective tissue, infections and infestations, and metabolism and nutrition disorders. In contrast, statin co-use was associated with lower RORs for hepatobiliary, blood and lymphatic, endocrine and immune system disorders. The results of multivariate logistic regression analysis (Supplemental Figure 4(B)) showed that statin use was significantly associated with higher RORs of AEs in the infections and infestations (aOR: 1.19, 95% CI: 1.06–1.34), musculoskeletal and connective tissue (aOR: 1.27, 95% CI: 1.12–1.43), and renal and urinary disorders (aOR: 2.05, 95% CI: 1.72–2.43). However, statin use was associated with lower RORs of AEs in the immune system (aOR: 0.49, 95% CI: 0.33–0.71) and the blood and lymphatic disorders (aOR: 0.83, 95% CI: 0.73–0.94).
Disproportionality analysis of SOC-level AE reporting by statin use in breast cancer patients undergoing CDK 4/6 inhibitors therapy.

AE, adverse event; ROR, reporting odds ratio; SOC, system organ class.
Among patients receiving VEGF monoclonal antibody therapy (Table 8), statin use elevated disproportionality signals for psychiatric, renal and urinary, metabolism and nutrition, infections and infestations, and gastrointestinal disorders. The results of multivariate logistic regression analysis (Supplemental Figure 4(C)) showed that statin use was significantly associated with higher RORs of AEs in the gastrointestinal (aOR: 1.69, 95% CI: 1.10–2.60), the infections and infestations (aOR: 1.75, 95% CI: 1.10–2.79), metabolism and nutrition (aOR: 1.94, 95% CI: 1.07–3.52), renal and urinary (aOR: 2.44, 95% CI: 1.34–4.45), and the psychiatric disorders (aOR: 2.74, 95% CI: 1.30–5.77).
Disproportionality analysis of SOC-level AE reporting by statin use in breast cancer patients undergoing VEGF monoclonal antibody therapy.

AE, adverse event; ROR, reporting odds ratio; SOC, system organ class; VEGF, vascular endothelial growth factor.
Among patients treated with PI3K/AKT/mTOR pathway inhibitors (Table 9), statin use elevated disproportionality signals for infections and infestations, psychiatric, renal and urinary, respiratory, thoracic and mediastinal, vascular, nervous, musculoskeletal and connective tissue and gastrointestinal disorders. The results of multivariate logistic regression analysis (Supplemental Figure 4(D)) showed that statin use was significantly associated with higher RORs of AEs in the respiratory (aOR: 1.41, 95% CI: 1.09–1.81), renal and urinary (aOR: 1.58, 95% CI: 1.07–2.33), psychiatric (aOR: 2.74, 95% CI: 1.30–5.77), and infections and infestations disorders (aOR: 1.75, 95% CI: 1.10–2.79). Additionally, statin use was associated with lower RORs of AEs in eye system disorders (aOR: 0.23, 95% CI: 0.06–0.94).
Disproportionality analysis of SOC-level AE reporting by statin use in breast cancer patients undergoing PI3K/AKT/mTOR pathway inhibitors.

AE, adverse event; ROR, reporting odds ratio; SOC, system organ class.
In patients receiving immunotherapy (Table 10), statin use elevated disproportionality signals for eye system disorders. The results of multivariate logistic regression analysis (Supplemental Figure 5) showed that there was no significant difference in RORs of AEs across various systems associated with statin use.
Disproportionality analysis of SOC-level AE reporting by statin use in breast cancer patients undergoing immunotherapy.

AE, adverse event; ROR, reporting odds ratio; SOC, system organ class.
Sensitivity analysis
To evaluate the potential impact of competition bias on disproportionality signals, a sensitivity analysis was conducted by excluding reports containing statin-related high-frequency AEs (Supplemental Tables 2–9). Overall, the sensitivity analysis results were consistent with the trends observed in the primary analysis.
Discussion
Based on the FAERS database, this study characterized the differences in AEs reporting across multiple SOCs between statin users and non-users among breast cancer patients receiving various treatment regimens, including chemotherapy, endocrine therapy, targeted therapy, and immunotherapy. Statins are key medications commonly prescribed for hypercholesterolemia, atherosclerosis and primary or secondary prevention of cardiovascular diseases. Currently, they are also increasingly used in combination with other medications in cancer patients. However, potential drug interactions, organ toxicities, and adverse reactions that statins might cause when used in complex treatment regimens have not been fully clarified. This study carries substantial clinical importance for optimizing the safety management of breast cancer patients who are undergoing statin therapy.
Through the analysis of 237,868 AE reports related to breast cancer in the FAERS database, disproportionality analysis found that patients concomitantly using statin was associated with lower RORs of hepatobiliary, blood and lymphatic disorders. In contrast, higher RORs were observed for skin and subcutaneous tissue, psychiatric, renal and urinary, musculoskeletal and connective tissue, infections and infestations, metabolism and nutrition, gastrointestinal, vascular, nervous system, respiratory, thoracic and mediastinal disorders. In addition, the results of a multivariate logistic regression analysis after adjusting for age, gender, and treatment drugs showed that statin use was associated with lower RORs of AEs in hepatobiliary, blood and lymphatic, immune system and cardiac disorders; while higher RORs of AEs were observed in skin and subcutaneous tissue, psychiatric, renal and urinary, musculoskeletal and connective tissue, infections and infestations, metabolism and nutrition and gastrointestinal disorders.
In terms of consistency with known safety profiles, several of the observed signals align with established pharmacological characteristics of statins. Increased reporting of musculoskeletal and connective tissue disorders is consistent with well-recognized statin-associated AEs, such as myopathy and rhabdomyolysis.12,13 Similarly, elevated reporting in renal and urinary disorders may be linked to severe muscle injury leading to secondary renal impairment. 14 In addition, previous studies have demonstrated that statin-related musculoskeletal toxicity may be further amplified in the presence of drug-drug interactions. 15 Drugs used in breast cancer treatment such as Ribociclib and Everolimus may engage in competitive metabolism with statins, especially simvastatin and atorvastatin, which are metabolized by CYP3A4. This competitive interaction can lead to elevated plasma concentrations of statins, thereby increasing the risk of severe renal AEs.16,17
This study identified that statin use was associated with a higher ROR for respiratory, thoracic, and mediastinal disorders, a finding consistent with previously published pharmacovigilance signals. Tan et al. 18 similarly identified significant disproportionality signals linking several statins—including rosuvastatin and atorvastatin—to respiratory AEs. These findings suggest that statins may confer a risk of pulmonary adverse reactions in real-world settings. Notably, our subgroup analysis demonstrated that among breast cancer patients receiving chemotherapy, statin use was instead associated with a lower ROR for respiratory, thoracic, and mediastinal disorders—an inverse trend compared with the overall population. This finding suggests that the oncologic treatment context may substantially modify the relationship between statin exposure and pulmonary AEs. Several explanations may account for this pattern. First, certain chemotherapeutic regimens, such as taxanes and anthracyclines, inherently cause respiratory symptoms 19 ; statins’ anti-inflammatory and antioxidant properties may mitigate the underlying inflammatory milieu. Second, chemotherapy recipients typically undergo more intensive clinical monitoring, and respiratory symptoms may be more readily attributed to the malignancy or chemotherapy rather than to statins, influencing reporting behavior. These hypotheses warrant further investigation using real-world clinical data and mechanistic studies.
In this study, concomitant statin use was associated with lower RORs of hepatobiliary, blood, and lymphatic system disorders among breast cancer patients across multiple therapeutic contexts. Although FAERS data cannot establish causality, the consistent negative disproportionality signals suggest that statin use may be linked to a more favorable hematologic and hepatobiliary safety profile in this population. Clinical evidence also suggests a potential protective association between statin use and hematologic malignancies. A meta-analysis of 14 observational studies found that statin users had a lower overall risk of hematologic malignancies (RR 0.86; 95% CI: 0.77–0.96), including leukemia and non-Hodgkin lymphoma, with even stronger associations seen with long-term use (RR 0.78; 95% CI: −0.71, 0.87). 20 Our finding of reduced hepatobiliary AE reporting among statin users is likewise biologically consistent with evidence from clinical studies. The potential mechanism may involve the pleiotropic effects of statins, such as anti-inflammation and antioxidation, which help alleviate liver inflammation and fibrosis.21,22 Additionally, statins may also alleviate hepatic lipotoxicity by dissolving cholesterol crystals. 23 However, the “depletion of susceptibles” bias should be considered to explain these results. In the context of statins, patients with pre-existing hepatic dysfunction, abnormal liver enzymes, or hematologic instability may be intentionally excluded from statin therapy or from specific anticancer regimens known to exacerbate these abnormalities. Consequently, the statin-exposed group may represent a selectively healthier subset with greater hepatic and hematologic reserve. Thus, the findings should be interpreted cautiously.
In our study, statin use was associated with lower RORs of cardiac disorders in both the multivariate logistic regression analysis and subgroup analyses among breast cancer patients receiving chemotherapy. Several epidemiological studies have demonstrated similar associations. A meta-analysis that included six studies revealed that among breast cancer patients receiving chemotherapy, endocrine therapy, and HER2-targeted therapy, concomitant statin use significantly reduced the risk of AEs in the cardiac system; in cohort studies, statin users had a significantly lower risk of cardiotoxicity after exposure to anthracyclines and/or trastuzumab (RR = 0.46, 95% CI (0.27–0.78)). 24 Additionally, a retrospective cohort study showed that the 5-year cumulative incidence rate of cardiotoxicity after anthracycline treatment was 1.2% (95% CI, 0.5–2.6) in breast cancer women exposed to statins, compared to 2.9% (95% CI, 1.7–4.6) in those not exposed (p-value = 0.01). 25 Prospective real-world studies and translational research are needed to clarify whether statins exert protective effects on cardiac systems.
In the immunotherapy subgroup, statin use was associated with elevated disproportionality signals only for eye disorders, while no significant differences were observed in the multivariate logistic regression analysis. This largely null finding should be interpreted with caution, particularly given the limited sample size of this subgroup, in which statin-exposed reports accounted for only a small proportion of the overall dataset. Previous pharmacovigilance research26 based on FAERS has reported different findings. One study including a broader population of patients receiving immune checkpoint inhibitors found that statin use was associated with increased reporting of immune-related AEs in multivariable analyses, with stronger signals observed in patients with lung, pancreatic, and renal cancers. In contrast, our analysis was restricted to a breast cancer population, and the relatively small number of statin-exposed reports in the immunotherapy subgroup may have limited the ability to detect similar signals.
Limitations
This study conducted AE signal mining based on the FAERS database. Although it benefits from a large sample size and real-world representativeness, there are still some limitations. First, FAERS is a spontaneous reporting system, with data coming from patients, doctors, and other reporting parties. There is potential for reporting bias and incomplete information, making it difficult to obtain complete baseline characteristics and treatment background. Second, notoriety bias may have influenced the observed signals. Well-recognized statin-associated AEs, particularly musculoskeletal events (e.g., myopathy and rhabdomyolysis), are more likely to be reported due to increased clinical awareness and regulatory attention. This stimulated reporting may lead to overestimation of RORs for these events. Conversely, competition bias may reduce the reporting probability of other AEs within the same reports. Although sensitivity analyses were performed to mitigate this issue, the findings should still be interpreted with caution. Third, this database cannot provide causal relationship judgments. Thus, the findings of this study merely suggest possible safety signals that require further validation through prospective clinical studies. Fourth, reports of drug combinations often lack a clear temporal sequence, making it difficult to distinguish the sequence of drug administration. Fifth, the potential differential effects of statin subclasses on SOC-specific AE signals could not be fully evaluated in the present study limited sample size. Finally, breast cancer treatment regimens exhibit substantial individual variability. Despite our efforts to conduct subgroup analyses according to treatment types, we were unable to fully account for confounding interference.
Conclusion
In breast cancer patients receiving statins concomitantly, specific disproportionality signals were observed across multiple SOCs. These findings highlight the need for individualized monitoring strategies and further mechanistic studies to clarify the underlying pathways and optimize clinical risk management.
Supplemental Material
sj-docx-1-taw-10.1177_20420986261450026 – Supplemental material for Adverse events associated with statin co-use in breast cancer patients: a disproportionality analysis based on the FDA Adverse Event Reporting System
Supplemental material, sj-docx-1-taw-10.1177_20420986261450026 for Adverse events associated with statin co-use in breast cancer patients: a disproportionality analysis based on the FDA Adverse Event Reporting System by Yunnan Zhang, Wenxing Peng, Wei Yang, Yang Gao, Yannan Fan and Qianqian Guo in Therapeutic Advances in Drug Safety
Supplemental Material
sj-docx-2-taw-10.1177_20420986261450026 – Supplemental material for Adverse events associated with statin co-use in breast cancer patients: a disproportionality analysis based on the FDA Adverse Event Reporting System
Supplemental material, sj-docx-2-taw-10.1177_20420986261450026 for Adverse events associated with statin co-use in breast cancer patients: a disproportionality analysis based on the FDA Adverse Event Reporting System by Yunnan Zhang, Wenxing Peng, Wei Yang, Yang Gao, Yannan Fan and Qianqian Guo in Therapeutic Advances in Drug Safety
Supplemental Material
sj-docx-3-taw-10.1177_20420986261450026 – Supplemental material for Adverse events associated with statin co-use in breast cancer patients: a disproportionality analysis based on the FDA Adverse Event Reporting System
Supplemental material, sj-docx-3-taw-10.1177_20420986261450026 for Adverse events associated with statin co-use in breast cancer patients: a disproportionality analysis based on the FDA Adverse Event Reporting System by Yunnan Zhang, Wenxing Peng, Wei Yang, Yang Gao, Yannan Fan and Qianqian Guo in Therapeutic Advances in Drug Safety
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.