
Abstract
Background:
Belimumab is a biologic agent used in the treatment of systemic lupus erythematosus (SLE). However, its safety profile during pregnancy has not been fully established, and real-world evidence regarding its association with adverse pregnancy outcomes remains limited.
Objectives:
To evaluate the safety of belimumab during pregnancy and explore its potential associations with maternal and fetal/neonatal adverse events.
Design:
Retrospective pharmacovigilance study.
Methods:
Disproportionality analysis of pregnancy-related individual case safety reports (ICSRs) from the FDA Adverse Event Reporting System (FAERS), Q2 2011–Q4 2024. Pregnancy-related cases were identified using Standardized MedDRA Queries. Belimumab was the primary suspected drug, with hydroxychloroquine and mycophenolate mofetil as negative and positive controls, respectively. Signal detection employed the reporting odds ratio (ROR); stratified analyses assessed potential confounding factors.
Results:
A total of 263,400 ICSRs was identified, including 537 belimumab, 1033 hydroxychloroquine, and 1039 mycophenolate mofetil. Most belimumab-related cases were reported from North America (78.40%), with SLE as the primary indication (71.88%). Disproportionality analysis revealed significant reporting of abortion (ROR 2.15, 95% confidence interval (CI) 1.76–2.63), hypertensive disorders of pregnancy (ROR 2.20, 95% CI 1.32–3.66), and pregnancy-related hemorrhagic complications (ROR 2.19, 95% CI 1.09–4.40), but not for stillbirth, preterm birth, or congenital malformations. A neonatal respiratory disorder signal was also observed (ROR 6.50, 95% CI 2.90–14.53). The hypertensive disorder signal was amplified with concomitant glucocorticoid use, suggesting confounding by disease severity. Mycophenolate mofetil, as a positive control, generated expected signals for adverse pregnancy outcomes and congenital anomalies, validating method sensitivity.
Conclusion:
Belimumab exposure during pregnancy is not associated with a significantly elevated risk of stillbirth, preterm birth, or overall congenital malformations. Conversely, disproportionality signals were detected for abortion, hypertensive disorders of pregnancy, hemorrhagic complications, and neonatal respiratory disorders. These signals warrant cautious interpretation, as they may partially reflect the elevated baseline risk intrinsic to the high-risk SLE patient population.
Plain language summary
Keywords
Introduction
Systemic lupus erythematosus (SLE) is a chronic autoimmune disorder that affects multiple organs and presents with a wide range of clinical manifestations. Recent data show that the global incidence and prevalence of SLE have reached 5.14 per 100,000 and 43.7 per 100,000, respectively, with notable variations based on gender and age. Studies have demonstrated that adult women are more susceptible to SLE. 1 Women with SLE face significant challenges during pregnancy. The disease is associated with adverse pregnancy outcomes and complications, including preterm birth, miscarriage, stillbirth, intrauterine growth restriction (IUGR), small-for-gestational-age (SGA) infants, and preeclampsia. Furthermore, pregnant women with SLE are at an increased risk of disease flare-ups during pregnancy. 2 In current clinical practice, standard SLE therapies, such as cyclophosphamide, methotrexate, and mycophenolate mofetil (MMF), have been linked to birth defects and miscarriage. The pregnancy medications recommended by existing guidelines, such as hydroxychloroquine and azathioprine, provide a balance between efficacy and safety, but remain insufficient for controlling moderate-to-severe active SLE in pregnant patients.3–5 This therapeutic gap has spurred interest in B lymphocyte-targeted therapies. Belimumab, the first approved B lymphocyte stimulator (BLyS) inhibitor, is increasingly being studied for its safety and efficacy during pregnancy.6,7
Belimumab selectively binds to soluble BLyS molecules, inhibiting their interaction with B cell surface receptors and thereby suppressing the survival and differentiation of autoreactive B cells. Phase III clinical trials have demonstrated that the drug reduces the risk of severe relapse in SLE patients by 46%–58%, with significant efficacy observed even in patients with inadequate responses to conventional treatments. 7 The updated 2024 EULAR guidelines endorse conditional use of belimumab during pregnancy for SLE management when clinically necessary to control maternal disease activity. 8 Notably, belimumab, an IgG1 monoclonal antibody, undergoes active placental transport, with transfer quantities increasing progressively with gestational age and reaching peak levels during the third trimester. 9 A case report has further substantiated the occurrence of placental transfer of belimumab in humans. Consequently, the characteristics of its transplacental passage and potential fetal implications warrant continued observation in clinical practice. 10 However, current clinical evidence has significant limitations, as pregnant women are typically excluded from pre-market trials for ethical reasons. Furthermore, available data on the use of belimumab in pregnant women are insufficient to establish its potential association with birth defects or adverse pregnancy outcomes. Therefore, the safety of this treatment during pregnancy warrants further investigation.
FAERS (FDA Adverse Event Reporting System) is the FDA’s spontaneous adverse event reporting system that supports post-marketing safety surveillance of drugs and biological products, serving as a crucial tool for assessing drug safety in clinical practice. 11 Due to the frequent exclusion of pregnant women from clinical trials, FAERS has become a key data source for evaluating medication safety during pregnancy. This retrospective pharmacovigilance study of the FAERS database aims to assess the association between maternal belimumab exposure during pregnancy and adverse maternal and fetal outcomes, thereby informing clinical risk assessment.
Methods
Data source
This study adhered to the Reporting of a Disproportionality Analysis for Drug Safety Signal Detection Using Individual Case Safety Reports in Pharmacovigilance (READUS-PV) guidelines. 12 This retrospective pharmacovigilance study uses the FAERS database as its data source. The study period was selected based on the availability of relevant drug and safety data. Belimumab received FDA approval for marketing in March 2011, and by the time of this study, only data up to the fourth quarter of 2024 had been released by the FDA. Individual case safety reports (ICSRs) were extracted from the FAERS database for the period between Q2 2011 and Q4 2024 to analyze maternal use of belimumab and its impact on pregnancy and fetal/neonatal outcomes. Duplicates were removed using the recommended method of FDA, retaining the report with the largest FDA_DT value for cases with identical CASEID. If both CASEID and FDA_DT were identical, the report with the highest PRIMARYID value was kept. Given the anonymized design of the FAERS database, this study was exempt from institutional review board approval.
Definition of the study population and target drug
Determination of the pregnant population
This study focuses on the pregnant population to minimize potential biases in analyzing the association between drugs and pregnancy outcomes, as most reports in databases come from nonpregnant women. Given that spontaneous reporting databases lack a specific field to identify reports from pregnant women, we adopted the method described by Sakai13,14 to identify pregnancy-related reports in FAERS, as shown in Figure 1. From 2011 Q2 to 2024, a total of 19,167,604 records were collected from FAERS, with duplicates excluded. To identify pregnancy-related reports, we included 88,569 records involving placental drug exposure and applied standard MedDRA queries (SMQs) based on adverse drug reactions and indications (the name of SMQ codes was shown in Table S1). This process initially identified 359,798 reports. This approach ensured that the reports included in the analysis were highly relevant and specific for drawing meaningful conclusions. Further screening defined cases with terms listed in Table S2 or those with placental drug exposure as explicitly pregnancy-related. After excluding explicitly pregnancy-related reports, 74,407 reports were removed due to treatment for pediatric diseases, gender and age mismatches, or paternal exposure. Ultimately, 263,400 reports were considered pregnancy-related and selected for final analysis.

Study flowchart. All reports were extracted from FAERS. n: the number of ICSRs. PTs*: maternal exposure during delivery (10071407), fetal exposure during delivery (10071409), maternal exposure before pregnancy (10071406), maternal exposure during pregnancy (10071408), fetal exposure during pregnancy (10071404), exposure during pregnancy (10073513), maternal exposure timing unspecified (10071415), fetal exposure timing unspecified (10071405), maternal drugs affecting fetus (10026923), drug exposure before pregnancy (10064998). PTs**: paternal drugs affecting the fetus (10050425), exposure via father (10071403), paternal exposure during pregnancy (10080091), paternal exposure timing unspecified (10080092), paternal exposure before pregnancy (10080093), and maternal exposure via partner during pregnancy (10084938).
Study drug
This study extracted all types of belimumab from the pregnant population. Data related to belimumab was obtained by querying drug names, brand names, and active pharmaceutical ingredients. This study only considered adverse reaction reports in which belimumab was listed as the primary suspect drug (PS). In this study, mycophenolate mofetil was used as a positive control, and hydroxychloroquine was selected as a negative control. Hydroxychloroquine is considered a safe option for the treatment of SLE during pregnancy, while mycophenolate mofetil should be avoided during pregnancy.5,15
Definition of maternal and fetal or newborn outcomes
Based on the MedDRA terms and hierarchy levels, this study identified perinatal and congenital abnormalities, categorizing them into six major types: stillbirth, abortions, premature birth, congenital malformations, pregnancy complications, and neonatal complications (Table 1).
MedDRA terms and hierarchy levels used to identify maternal and fetal or newborn adverse outcomes.
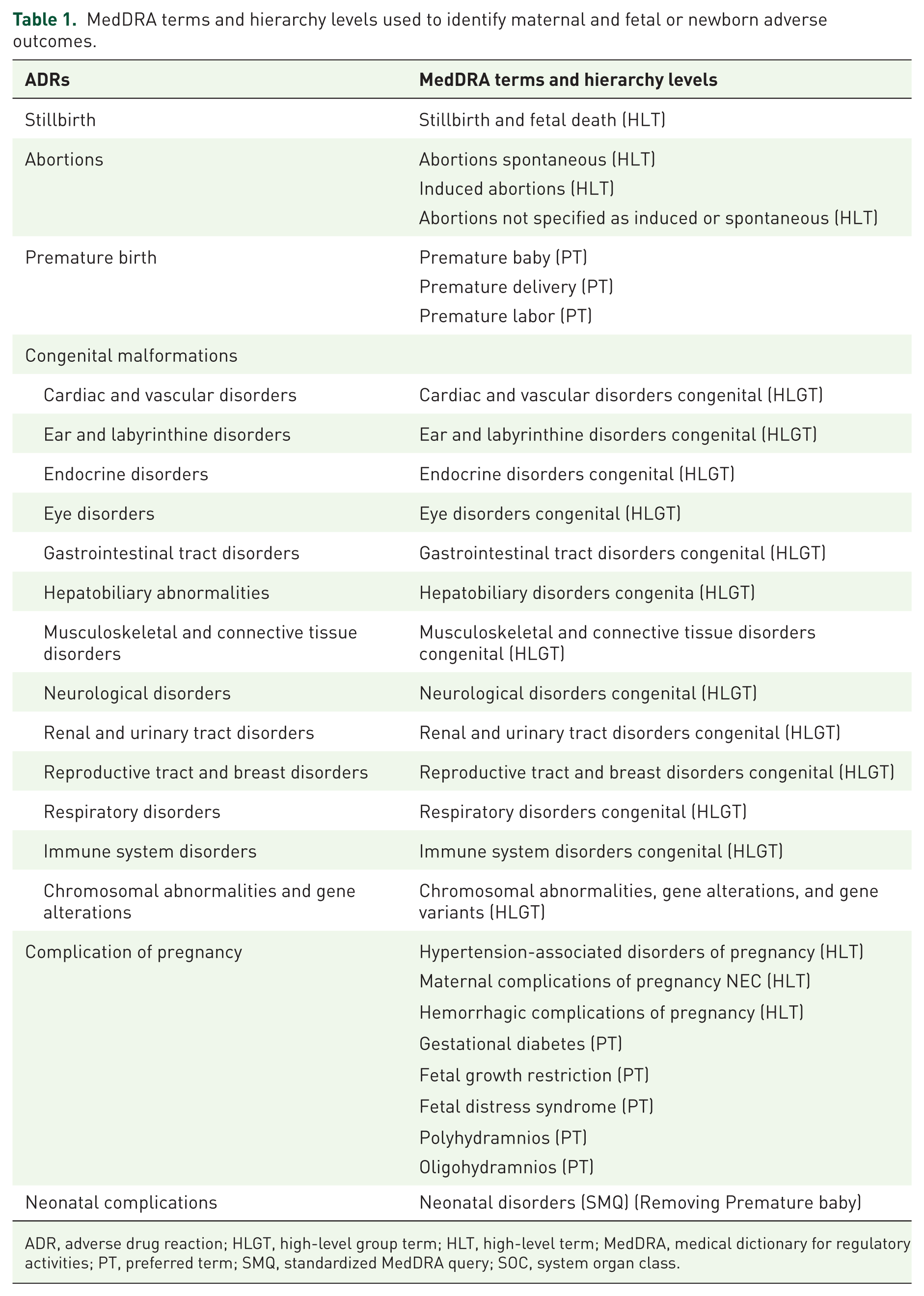
ADR, adverse drug reaction; HLGT, high-level group term; HLT, high-level term; MedDRA, medical dictionary for regulatory activities; PT, preferred term; SMQ, standardized MedDRA query; SOC, system organ class.
Statistical analysis
A descriptive analysis was performed on the reported clinical outcomes, which included factors such as age, indications, outcomes, reporters, and geographic origin, with frequencies (percentages) presented. For signal detection, this study employed the reporting odds ratio (ROR), a method commonly used in pharmacovigilance, to identify potential signals between drugs and adverse reactions.14,16 The ROR is calculated as follows: ROR = (a/c)/(b/d), where a represents the number of ADRs associated with the target drug, b represents the number of ADRs associated with other drugs of interest in the study population, c represents the number of ADRs unrelated to the target drug but associated with other drugs of interest, and d represents the number of ADRs unrelated to both the target drug and other drugs of interest in the study population. If the lower bound of the 95% confidence interval (CI) for the ROR is greater than one, it indicates that the reporting frequency of adverse reactions for the target drug is higher than that for all other drugs. ROR can only be interpreted when at least three ICSR reports have been submitted for a particular drug.
To assess the robustness of our findings and address potential confounding factors, we conducted sensitivity and stratified analyses. First, two sensitivity analyses were performed: (1) restricting the analysis to ICSRs submitted by healthcare professionals to minimize bias from nonprofessional reporters; and (2) analyzing ICSRs involving belimumab as the sole reported drug to evaluate the impact of concomitant medications. Second, to further enhance signal interpretation, we conducted a series of stratified disproportionality analyses based on key clinical and temporal variables. The overall dataset for belimumab was stratified according to primary indication (systemic lupus erythematosus (SLE) vs non-SLE indications), reported concomitant use of systemic glucocorticoids, reported concomitant use of anticoagulant/antiplatelet agents, and reporting time (reports up to and including 2022 vs reports from 2023 onwards).
All analyses were conducted using R software (version 3.6.3, R Foundation for Statistical Computing, Vienna, Austria) and Microsoft Excel 2019.
Results
Report characteristics
In the FAERS database from Q2 2011 to Q4 2024, a total of 263,400 ICSRs related to pregnancy were identified. Of these, 537 reports were associated with belimumab, 1033 with hydroxychloroquine, and 1039 with mycophenolate mofetil, all of which were included in the analysis. The characteristics of the study population are presented in Table 2.
Demographic characteristics of reports with belimumab, hydroxychloroquine, and mycophenolate mofetil for maternal and fetal or newborn adverse outcomes within the FAERS database.

Data are presented as N (%).
SLE were identified by narrow-scope PTs in the SMQ according to “INDI_PT” in INDI files.
Healthcare professionals including reporters such as physicians, pharmacists, and other health-professional; nonhealthcare professionals including reporters such as consumers and lawyers.
Since a case may experience different clinical outcomes during drug therapy, the outcome with the highest severity was selected for analysis.
MedDRA, medical dictionary for regulatory activities; PT, preferred term; SMQ, standardized MedDRA query.
Among the ICSRs related to belimumab, the majority (421 cases, 78.40%) were from North America. The most frequently reported age group was 18–35 years (16.76%). SLE was the primary indication for belimumab use in this population (71.88%). Furthermore, most reports were submitted by nonmedical personnel (62.01%). In terms of outcome severity, the most common category was “other serious outcomes” (24.95%), followed by “hospitalization” (15.64%). Over recent years, the number of belimumab-related reports has increased steadily, reaching its peak in 2024. The distribution of ICSRs by year is shown in Figure 2.
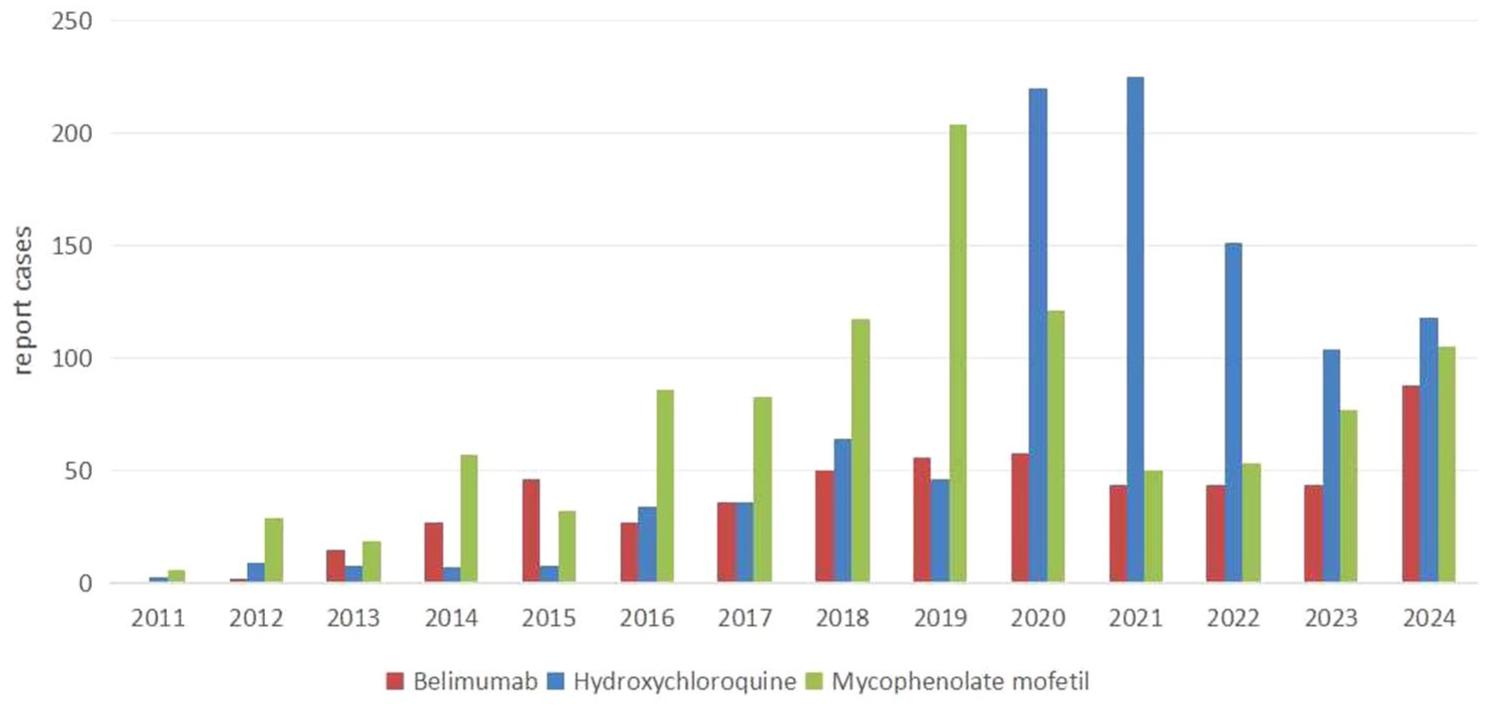
Annual distribution chart of ICSRs associated with belimumab, mycophenolate mofetil, and hydroxychloroquine in FAERS.
Disproportionality analysis
Initially, belimumab was compared with other medications used in the pregnancy population within the FAERS database. No significant overreporting was observed for adverse events such as stillbirth, preterm birth, or congenital malformations. However, significant overreporting was detected for abortion (including both spontaneous and induced abortion) (ROR 2.15, 95% CI 1.76–2.63), pregnancy-related hypertensive disorders (ROR 2.20, 95% CI 1.32–3.66), and pregnancy-related hemorrhagic complications (ROR 2.19, 95% CI 1.09–4.40). The detailed results were presented in Figure 3.
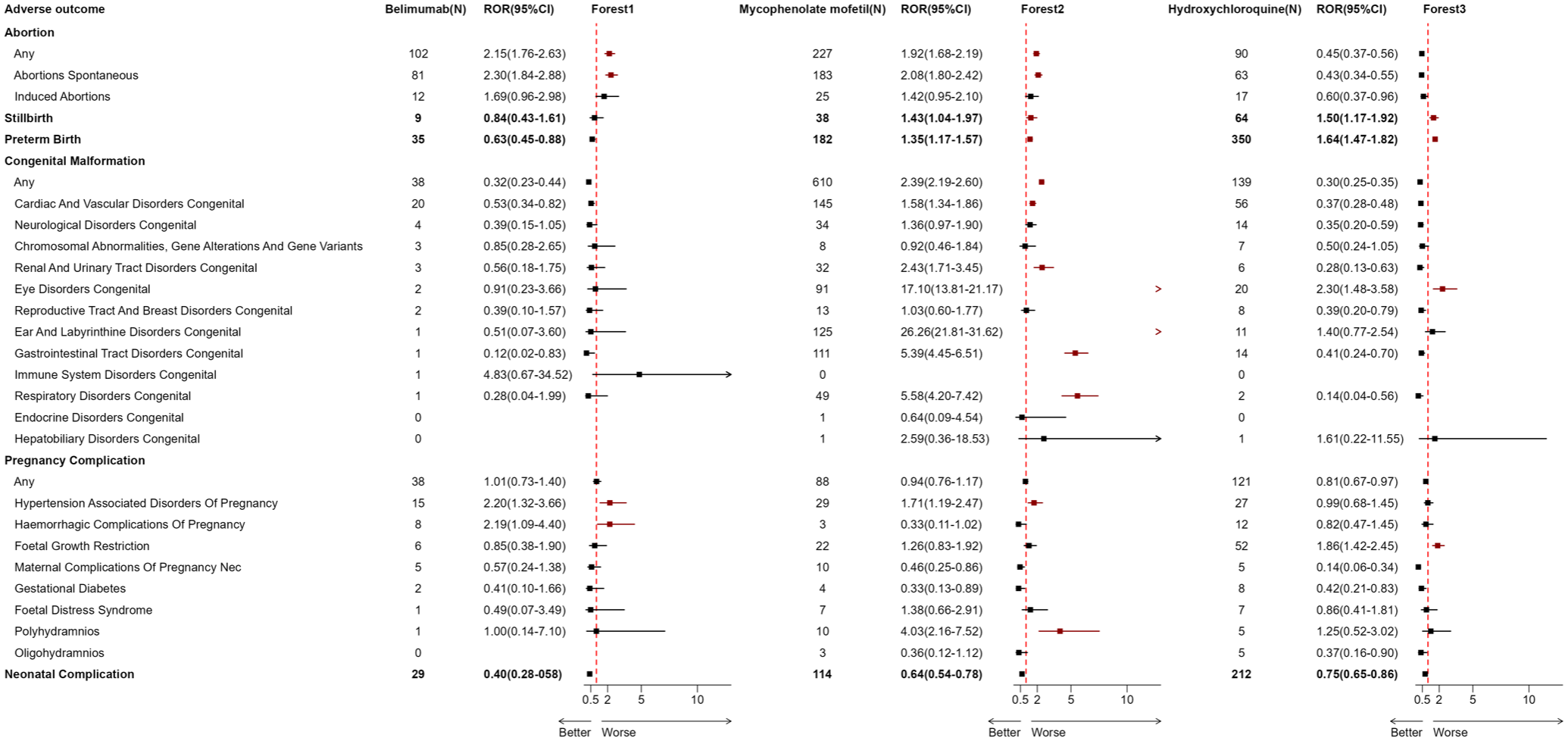
RORs of maternal and fetal or newborn outcomes with belimumab, mycophenolate mofetil, and hydroxychloroquine. N: number of drug–ADR pairs. Forest1: the forest plot of belimumab. Forest 2: the forest plot of mycophenolate mofetil. Forest 3: the forest plot of hydroxychloroquine. >: The range of ROR (95% CI) exceeds the x-coordinate of the forest plot. RORs in the figure are calculated by comparing the drug with all other drugs in pregnancy-related reports, excluding belimumab, hydroxychloroquine, and mycophenolate mofetil. When the lower bound of 95% CI for ROR > 1 and N > 3, a disproportionate reporting signal was detected.
As a negative control, reports involving hydroxychloroquine indicated positive signals for stillbirth, preterm birth, congenital eye disease, and fetal growth restriction. In contrast, reports involving mycophenolate mofetil exposure showed significantly positive signals for miscarriage (ROR 2.08, 95% CI 1.80–2.42), stillbirth (ROR 1.43, 95% CI 1.04–1.97), preterm birth (ROR 1.35, 95% CI 1.17–1.57), and congenital malformations (ROR 2.39, 95% CI 2.19–2.60). Within the congenital malformation subgroup, significant overreporting was observed for ear and labyrinth developmental abnormalities, congenital respiratory anomalies, urological defects, congenital digestive system abnormalities, cardiovascular malformations, and congenital eye defects in the mycophenolate mofetil reports. Additionally, pregnancy complications, including pregnancy-related hypertensive disorders and polyhydramnios, also exhibited significant positive signals. The detailed results are provided in Figure 3.
In reports related to neonatal complications, the overall ROR for all three medications was significantly below 1. For belimumab, the probability of neonatal respiratory distress increased (ROR 6.50, 95% CI 2.90–14.53). Detailed data are shown in Figure 4.

RORs of neonatal complications with belimumab in PT level. N: number of drug–ADR pairs. RORs in the figure are calculated by comparing the drug with all other drugs in pregnancy-related reports, excluding belimumab, hydroxychloroquine, and mycophenolate mofetil. When the lower bound of 95% CI for ROR > 1 and N > 3, a disproportionate reporting signal was detected.
Sensitivity and stratified analyses
To evaluate the robustness of the primary signals and investigate potential confounding factors, we conducted two prespecified sensitivity analyses and four stratified analyses.
In the sensitivity analyses, where the reporters were limited to health professionals, no significant differences that could have influenced the conclusions were observed (Figure S1). When the combination drug was excluded from the cases, only the signal of abortions was detected (Figure S2).
Stratified analyses were performed according to indication (SLE vs non-SLE), concomitant medication use (glucocorticoids, anticoagulants/antiplatelet agents), and reporting year. The significant signals of four stratified analyses are summarized in Table 3.
Signals from stratified disproportionality analyses for belimumab.
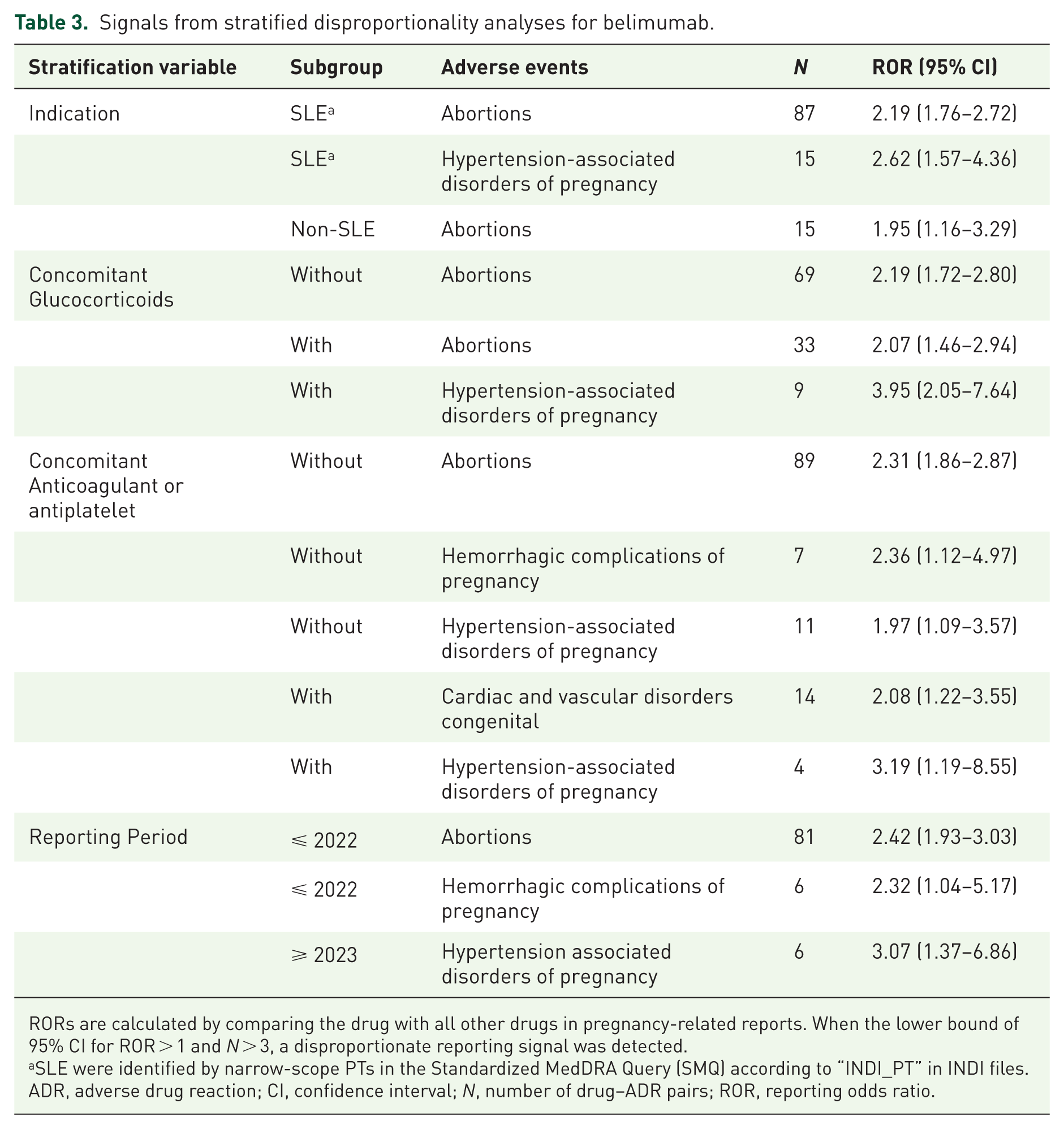
RORs are calculated by comparing the drug with all other drugs in pregnancy-related reports. When the lower bound of 95% CI for ROR > 1 and N > 3, a disproportionate reporting signal was detected.
SLE were identified by narrow-scope PTs in the Standardized MedDRA Query (SMQ) according to “INDI_PT” in INDI files.
ADR, adverse drug reaction; CI, confidence interval; N, number of drug–ADR pairs; ROR, reporting odds ratio.
Stratification by indication demonstrated that the signal for abortions remained significant both in reports with SLE indications (ROR 2.19, 95% CI 1.76–2.72) and in those with non-SLE indications (ROR 1.95, 95% CI 1.16–3.29). For hypertension-associated disorders of pregnancy, a significant signal was observed specifically in the SLE indication subgroup (ROR 2.62, 95% CI 1.57–4.36).
Stratification by concomitant glucocorticoid use revealed that the signal for hypertension-associated disorders of pregnancy was markedly stronger among reports mentioning glucocorticoid co-administration (ROR 3.95, 95% CI 2.05–7.64). In contrast, the signal for abortions remained consistent irrespective of glucocorticoid use, with comparable ROR values in both subgroups (with glucocorticoids: ROR 2.07, 95% CI 1.46–2.94; without glucocorticoids: ROR 2.19, 95% CI 1.72–2.79).
Stratification by concomitant anticoagulant/antiplatelet use identified a signal for cardiac and vascular disorders congenital in the subgroup reporting such therapy (ROR 2.08, 95% CI 1.22–3.55; n = 14). Importantly, the signal for abortions (ROR 2.31, 95% CI 1.86–2.87) and hemorrhagic complications of pregnancy (ROR 2.36, 95% CI 1.12–4.97) remained significant in the subgroup not reporting anticoagulant/antiplatelet use.
Stratification by reporting year (using 2022 as the cutoff) showed that the signal for abortions was more pronounced in reports prior to 2022 (ROR 2.42, 95% CI 1.93–3.02). The signal for hypertension-associated disorders of pregnancy became more prominent in reports from 2023 onwards (ROR 3.07, 95% CI 1.37–6.86), while the signal for hemorrhagic complications of pregnancy was primarily observed in reports up to 2022 (ROR 2.32, 95% CI 1.04–5.17).
Discussion
This study systematically reviewed pregnancy outcomes in women using belimumab during pregnancy, utilizing the FAERS database from Q2 2011 to Q4 2024. The analysis revealed no significant signals for stillbirth, preterm birth, or congenital malformations associated with belimumab. However, significant overreporting was observed for abortions (including both spontaneous and induced abortion), pregnancy-related hypertensive disorders, pregnancy hemorrhagic complications, and neonatal respiratory diseases. In comparator analyses, mycophenolate mofetil, as a positive control, generated strong signals for multiple congenital malformations across cardiovascular, urinary, gastrointestinal, and ocular systems, and for adverse pregnancy outcomes, supporting the sensitivity and specificity of the analytical approach.
Hydroxychloroquine—generally considered a first-line, pregnancy-safe therapy in SLE—also yielded positive signals for a few outcomes in this analysis (e.g., stillbirth and fetal growth restriction), likely reflecting the contribution of SLE itself to adverse pregnancy outcomes rather than a direct drug effect. SLE significantly increases the risk of adverse pregnancy outcomes, including preeclampsia, fetal growth restriction, preterm birth, and stillbirth, through immune-inflammatory-mediated placental vascular lesions, complement activation, and coagulation-vascular pathway disturbances. 17 Disease activity represents the foremost independent risk factor for adverse pregnancy outcomes in SLE.18–20 The 2024 EULAR guidelines recommend continuation of hydroxychloroquine (⩽400 mg/d) throughout pregnancy as foundational therapy for SLE to reduce disease activity risk and preeclampsia incidence; for patients with inadequate response to conventional therapy, non-TNF inhibitor biologics such as belimumab may be continued during pregnancy following individualized risk–benefit assessment, achieving further disease activity control through targeted B-cell pathway modulation and thereby improving maternal-fetal outcomes. 8
Le Hai et al. 21 reported a system-level disproportionality signal for belimumab within the system organ class of “pregnancy, puerperium, and the perinatal period” using FAERS database. The present study narrows this broad association through three methodological refinements: strict case ascertainment of pregnancy-related reports, active comparator control with hydroxychloroquine and mycophenolate mofetil, and stratified outcome analyses. This granular approach transforms an undifferentiated system-level signal into specific, quantifiable risks for distinct pregnancy outcomes.
Among the pregnancy-related adverse outcomes, the strongest association was between belimumab and abortions (ROR = 2.15, 95% CI 1.76–2.63). In the sensitivity analysis restricted to ICSRs where belimumab was the reported drug (excluding all reports with concomitant medications), abortion remained the only signal. Stratified analyses demonstrated that this signal persisted across multiple subgroups, including those with SLE and non-SLE indications, with and without concomitant glucocorticoid use, and irrespective of anticoagulant therapy. This consistency suggests a relatively independent drug-effect association.
Although existing studies have not clearly established the link between belimumab and pregnancy loss, an analysis of the EudraVigilance database showed no significant difference in fetal death risk between continued medication and early discontinuation. 22 A comprehensive analysis of clinical trials, pregnancy registries (BPR), and postmarketing reports revealed considerable variability in miscarriage rates across data sources: 31.8% in clinical trials, 4.2% in the prospective cohort of the BPR, and 31.4% in postmarketing reports. 7 These discrepancies are difficult to interpret due to the lack of control groups matched for disease activity, as SLE itself is a high-risk factor for pregnancy loss. The low miscarriage rate in the prospective cohort of the BPR may be influenced by the extremely small sample size.
Belimumab demonstrated an elevated ROR for pregnancy-specific complications, including hypertensive disorders of pregnancy and preeclampsia (ROR 2.20, 95% CI 1.32-3.66). However, stratified analysis revealed important confounding effects. The signal was markedly stronger in the subgroup reporting concomitant glucocorticoid use, strongly suggesting an association with disease severity. Glucocorticoids are typically administered to control active or more severe SLE, and disease activity itself is a major risk factor for complications such as preeclampsia. Therefore, the observed signal likely reflects the clinical profile of high-risk patients requiring intensive therapy rather than a direct pharmacological effect of belimumab. The increased signal for hemorrhagic pregnancy complications (ROR = 2.19) may reflect maternal coagulopathy, thrombocytopenia, and immune-mediated vascular injury, which are more prevalent in the SLE population.23,24 Notably, reports of this signal were concentrated prior to 2022, possibly reflecting evolving clinical practices or reporting patterns. Additionally, stratified analysis identified a signal for congenital cardiovascular system disorders only in the subgroup reporting concomitant anticoagulant or antiplatelet therapy. This most likely points to a specific high-risk population with comorbid conditions such as antiphospholipid syndrome rather than a general drug effect. These observations indicate that interpretation of belimumab-related signals in FAERS must account for the underlying disease, the burden of complications, and concomitant medications.
Notably, a signal for neonatal respiratory disorders was found in this analysis (ROR = 6.50; 95% CI 2.90–14.53). One plausible mechanism is that pregnancy-associated immunosuppression increases maternal infection risk, which may adversely affect fetal lung development. Analyses of VigiBase data and a literature review likewise suggest that in utero exposure to belimumab may increase neonatal infection risk.9,25 This finding is consistent with belimumab’s B-cell–suppressing pharmacology and supports close infectious surveillance of infants exposed in utero.
Pharmacologically, belimumab binds and neutralizes soluble BLyS, attenuating excessive autoimmune activation. However, pregnancy-associated immune tolerance depends on specific B-cell subsets—particularly regulatory B cells that produce immunoregulatory cytokines such as interleukin-10 (IL-10). Suppression of these populations could perturb the trophoblastic immune microenvironment and increase the risk of embryonic loss. Moreover, immunosuppression may heighten maternal infection risk and promote placental inflammation, which could contribute to the observed association with neonatal respiratory disease. Placental transfer of IgG primarily occurs in late gestation via the neonatal Fc receptor; although transfer in early to mid-gestation is limited, maternal administration of belimumab in late pregnancy could result in fetal drug exposure and interfere with immune development. This mechanism warrants validation in higher-quality clinical and experimental studies.
Current evidence on belimumab safety in pregnancy is limited and largely comprised of case reports or small postmarketing series. Our analysis of a large real-world database supplements these data by identifying potential specific risk signals associated with belimumab use during pregnancy. The consistency of positive and negative control results supports the reasonable sensitivity and specificity of the ROR method employed, enhancing confidence in these findings.
Limitations
Several important limitations of this study warrant careful consideration when interpreting the findings. First, as a study based on a spontaneous reporting database, it is subject to inherent under-reporting, which precludes the calculation of absolute frequencies for specific adverse drug reactions. Furthermore, data for many key variables, such as pregnancy trimester, detailed dosing, gestational age, and duration of drug exposure, were missing or incomplete.
Second, although stratified analyses were conducted to address potential confounding by indication, concomitant medication use, and reporting period, residual confounding cannot be ruled out. The most critical limitation is the lack of quantitative assessment of disease activity. Given that SLE disease activity during pregnancy is a well-established risk factor for adverse outcomes and may influence treatment decisions (e.g., initiation of belimumab or glucocorticoids), the observed signals—particularly for hypertensive disorders and hemorrhagic complications—may be partly or wholly attributable to this unmeasured confounder rather than a direct effect of belimumab. Additionally, potential patient overlap between treatment groups (e.g., patients on belimumab likely using hydroxychloroquine as background therapy) and possible under-reporting of concomitant medications introduce further residual confounding.
Third, some subgroup analyses were based on small sample sizes (e.g., for hypertensive disorders or hemorrhagic complications in certain strata), resulting in less precise estimates (wide confidence intervals) and an increased risk of spurious findings.
Fourth, specific methodological data gaps exist. FAERS reports typically lack information on the precise timing of drug exposure during pregnancy (e.g., gestational week), preventing risk stratification by exposure timing (e.g., first vs. third trimester). Moreover, although we stratified by concomitant glucocorticoid use, dose information was severely missing, precluding reliable analysis based on clinically relevant dose thresholds and limiting our ability to adjust for confounding related to treatment intensity.
Finally, it must be emphasized that disproportionality analysis alone cannot establish causation. The signals detected in this study should be considered hypothesis-generating, indicating potential safety concerns that require prioritization for verification in prospective, well-designed studies.
Conclusion
This retrospective pharmacovigilance analysis of belimumab safety during pregnancy used data from the FAERS. The results indicated that significant overreporting was not observed for stillbirth, preterm birth, or congenital malformations, while abortions, pregnancy-related hypertensive disorders, and neonatal respiratory diseases showed increased reporting probability. These signals should be interpreted cautiously, as confounding by indication cannot be fully excluded, and they may partly reflect the baseline risk of the high-risk SLE patient population requiring belimumab therapy. In clinical decision-making, the use of belimumab in pregnant patients with SLE or those planning pregnancy requires a rigorous benefit–risk assessment, particularly when disease activity is high and conventional safe medications are inadequate. Prospective cohort or case–control studies are recommended to more definitively evaluate belimumab safety during pregnancy.
Supplemental Material
sj-doc-1-taw-10.1177_20420986261460168 – Supplemental material for Safety of belimumab during pregnancy: associations with maternal and fetal or newborn adverse outcomes based on FAERS data
Supplemental material, sj-doc-1-taw-10.1177_20420986261460168 for Safety of belimumab during pregnancy: associations with maternal and fetal or newborn adverse outcomes based on FAERS data by Yujie Lin and Jing Yao in Therapeutic Advances in Drug Safety
Supplemental Material
sj-docx-2-taw-10.1177_20420986261460168 – Supplemental material for Safety of belimumab during pregnancy: associations with maternal and fetal or newborn adverse outcomes based on FAERS data
Supplemental material, sj-docx-2-taw-10.1177_20420986261460168 for Safety of belimumab during pregnancy: associations with maternal and fetal or newborn adverse outcomes based on FAERS data by Yujie Lin and Jing Yao in Therapeutic Advances in Drug Safety
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.