
Abstract

Polycystic ovary syndrome (PCOS) is an endocrinological condition affecting up to 18% of reproductive-age women. 1 Diagnosis requires two or more of the following: (a) menstrual irregularity; (b) hyperandrogenism (excess male hormones); and (c) polycystic ovaries. 1 In addition, women with PCOS have higher rates of cardiovascular disease (CVD) risk factors and, potentially, CVD events. 1 Given that some PCOS symptoms are specifically premenopausal, it is important to understand the CVD risk associated with PCOS across the lifespan. To address this, we conducted a nationwide registry study.
We identified women from 1994 to 2015 using the Danish National assisted reproductive technology (ART)-Couple II Cohort, linked to the National Patient Register, the Civil Registration System and the Medical Birth Register. Women with CVD at baseline were excluded (n = 2325), resulting in a total of 60,574 women. Women with PCOS were identified using the International Classification of Diseases (ICD-10) code E28.2 from 2006 onwards. Before 2006 the register-specific code ‘ovulation defect’ was used to indicate PCOS. As 90–95% of anovulatory women presenting to fertility clinics have PCOS, ovulation defect is an appropriate proxy. 1
Incident CVD was identified through the National Patient Register using ICD-10 codes (G45–G46, I10–I28, I42–I51, I60–I72, I74–I79, I81, I82). The study was approved by the Danish Data Protection Agency and Health Data Authority. Patient informed consent and ethics committee approval were not required.
Women were followed from their initial ART treatment and censored at the first of the following: (a) CVD presentation; (b) death; (c) emigration; (d) designated ‘missing’ in the Civil Registration System; or (e) 31 December 2015 (end of follow-up). Hazard ratios (HRs) and 95% confidence intervals (CIs) were estimated using Cox proportional hazards models with age as the underlying time scale. To obtain HR estimates for CVD at different ages, analyses was stratified by age: less than 30, 30–34, 35–39, 40–49 and 50 years and over. Two models were constructed: model 1 (age) and model 2 (age, year of first ART treatment, baseline parity, gestational diabetes, relationship status and education). Body mass index (BMI), smoking and alcohol data were available from 2006 onwards. A sensitivity analysis also adjusting for these factors was conducted. As data from 2006 onwards were only included, no risk estimates were calculated for women over 50 years of age, as none had reached that age.
Of the 60,574 women, 6149 (10.2%) had PCOS. Median follow-up was 8.9 years (interquartile range 4.2–14.8), and 2925 (4.8%) women developed CVD. Baseline characteristics are displayed in Table 1. Women with PCOS were younger, more likely to develop gestational diabetes and less likely to be single. Women with PCOS were at greater CVD risk (age-adjusted HR 1.20, 95% CI 1.08–1.34), which remained after adjustment for covariates (adjusted HR 1.19, 95% CI 1.07–1.33). After stratifying by age, there was no evidence of a higher CVD risk for women with PCOS after the age of 50 years (Figure 1).
Characteristics of women receiving ART treatment by polycystic ovary syndrome diagnosis, Denmark, 1994–2015.
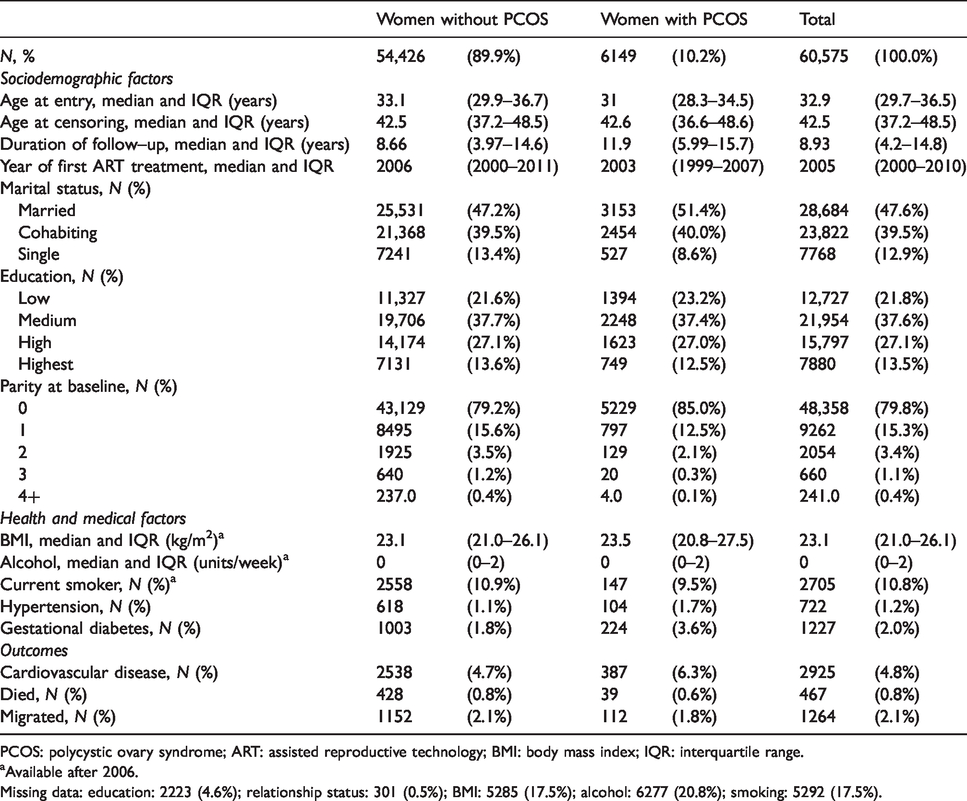
PCOS: polycystic ovary syndrome; ART: assisted reproductive technology; BMI: body mass index; IQR: interquartile range.
aAvailable after 2006.
Missing data: education: 2223 (4.6%); relationship status: 301 (0.5%); BMI: 5285 (17.5%); alcohol: 6277 (20.8%); smoking: 5292 (17.5%).
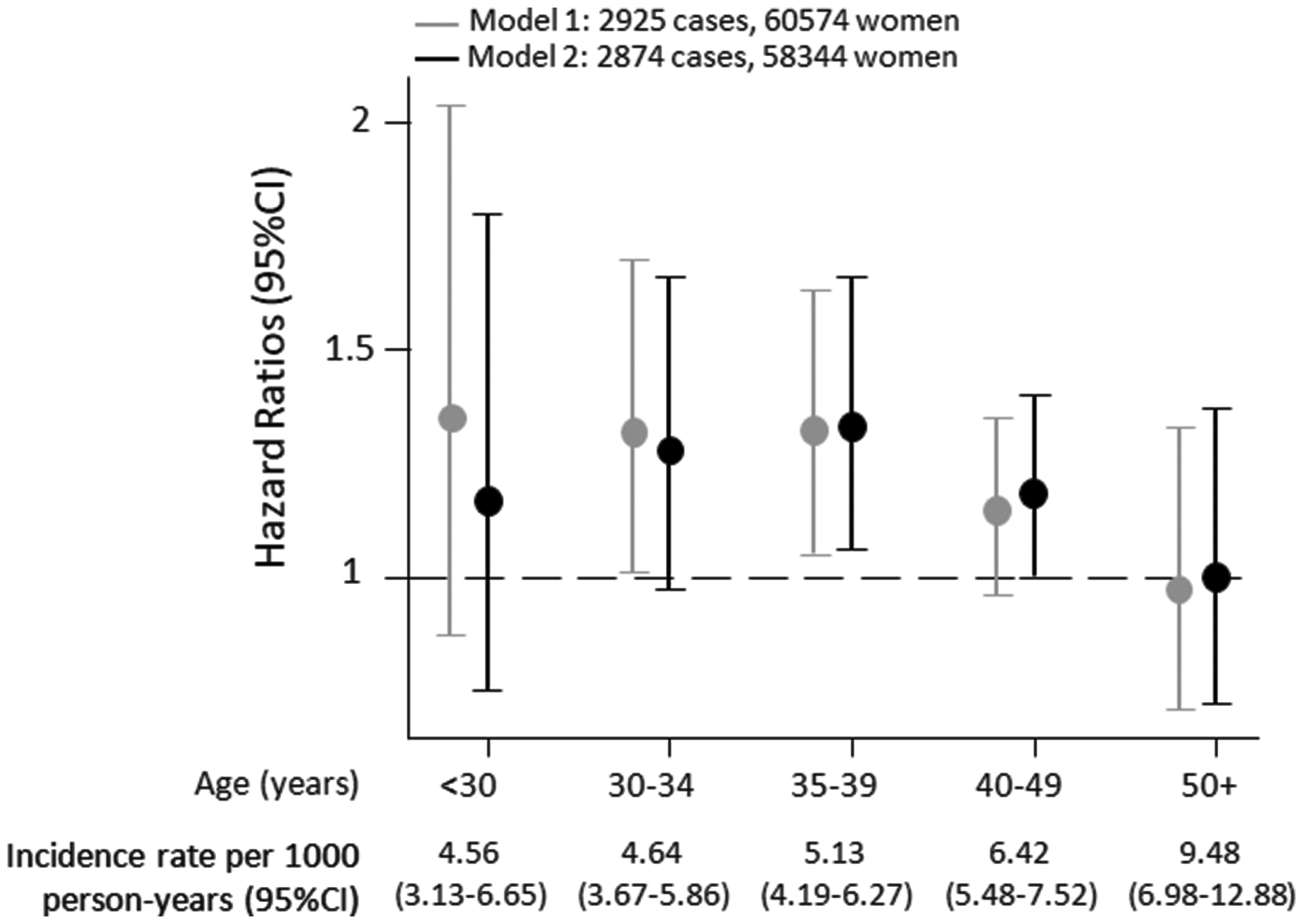
Incidence rates, hazard ratios and 95% confidence intervals (CIs) for the risk of incident cardiovascular disease by polycystic ovary syndrome status in the full cohort, and stratified by age group, Denmark, 1994–2015. Model 1: Age adjusted; Model 2: Age, year of first assisted reproductive technology treatment, baseline parity, gestational diabetes, relationship status, level of education.
In sensitivity analyses adjusting for BMI, smoking and alcohol, the greater CVD risk remained for women with PCOS overall (n = 21,631, HR 1.49, 95% CI 1.04–2.06). There was also evidence of a greater risk in younger women only: less than 30 years: HR 1.59, 95% CI 0.68–3.72; 30–34 years: HR 1.43, 95% CI 0.82–2.48; 35–39 years: HR 1.72, 95% CI 0.97–3.03 and 40–49 years: HR 0.93, 95% CI 0.29–3.01).
To our knowledge, this is the first study to assess whether the CVD risk associated with PCOS varies with age, although inconsistencies between previous publications may be partly explained by an age-related variation in risk. 3 The potential variation of risk with age may be due to differences in the CVD risk profile between women with and without PCOS. On average, women with PCOS have a worse CVD risk profile than women without PCOS, 1 but these differences may diminish with age. 2
Our study has several strengths. These include nationwide data, adjustment for potential confounders and high validity of CVD diagnoses. 4 Furthermore, the sensitivity and specificity of a PCOS diagnosis is likely to be high, as women will have received a thorough gynaecological assessment. Study weaknesses include limited information about diabetes and hypercholesterolemia, and uncertain generalisability as women receiving ART treatment may differ from the general population. Prior to 2006, PCOS cases were identified through the registry-specific code ‘ovulation defect’, which could categorise women without PCOS as having PCOS. However, most women with an ovulation defect presenting in fertility clinics have PCOS. 1
In conclusion, women with PCOS are at greater CVD risk, with evidence of a higher risk for women in their 30s and 40s. Further investigation of how the association between PCOS and CVD varies with age is warranted within the general population.
Data sharing
On request, the analytical methods will be made available for other researchers for purposes of reproducing the results or procedures. The data are available through the Danish Data Protection Agency to approved researchers affiliated with a Danish institute.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the British Heart Foundation (RE/13/6/30180), a doctoral research grant to DV from the Faculty of Health and Medical Sciences, University of Copenhagen (Copenhagen, Denmark), a research fellowship to COW from Homerton College, University of Cambridge, a travel fellowship to COW from the European Society of Human Reproduction and Embryology and ReproUnion, and this article is part of the ReproUnion collaborative study, co-financed by the European Union, Intereg V Öresund-Kattegat-Skagerrak.