
Abstract
Objectives
Functional mitral regurgitation (FMR) remains challenging to repair surgically, as highlighted by the Cardiothoracic Surgical Trials Network (CTSN) trial, which showed limited durability of mitral annuloplasty. We previously demonstrated in vivo and experimentally that papillary muscle approximation (PMA) can improve mitral valve (MV) function, with or without annuloplasty. In this study, we assessed valve biomechanics after PMA, mitral annuloplasty, and their combination in imaging-derived computational models.
Methods
3D echo images were obtained in three pigs with heart failure, dilated ventricles, and FMR. Each echo dataset was segmented, and a subject-specific computational model of the MV was created. Virtual FMR repair was performed on each valve using PMA, annuloplasty with true-sized (40 mm) and downsized (38 mm and 36 mm) rings, and a combination of both techniques. For each repair strategy, leaflet closure was simulated, and MV geometry and biomechanics at peak systole were evaluated.
Results
Isolated PMA improved valve coaptation, reduced leaflet stresses and chordal tension forces, but failed to completely eliminate FMR. Isolated mitral annuloplasty also improved coaptation, but overall provided only limited geometric and biomechanical benefits. Combining annuloplasty and PMA resulted in the most favorable outcomes, eliminating FMR, increasing coaptation length (up to 97.7%), and reducing leaflet stresses (up to 43.7%) and chordal forces (up to 43.0%).
Conclusions
While both PMA and annuloplasty independently improved MV function, neither technique fully resolved FMR on its own. Their combination yielded the most favorable repair outcomes, eliminating FMR and significantly improving valve geometry and biomechanics without the need for excessive annular downsizing.
Keywords
Introduction
Functional mitral regurgitation (FMR) is a heart valve lesion that is often seen in patients with heart failure, wherein the left ventricle (LV) is dilated and dysfunctional. 1 The diseased LV perturbs the native mitral valve (MV) geometry resulting in inadequate systolic closure and backward leakage of blood through the valve (Figure 1A). Such regurgitation of blood into the left atrium elevates and congests pulmonary venous system and causes shortness of breath, dyspnea, etc., that worsen patient's quality of life and functional capacity. Furthermore, this regurgitant volume combined with the constant right ventricular output increases the total blood inflow to the LV in each heartbeat and imposes pathological volume overload on the LV causing its further dysfunction and progression of heart failure. Wall stresses become elevated, and ventricular dysfunction ensues, altogether accelerating heart failure hospitalizations and doubling mortality. 2
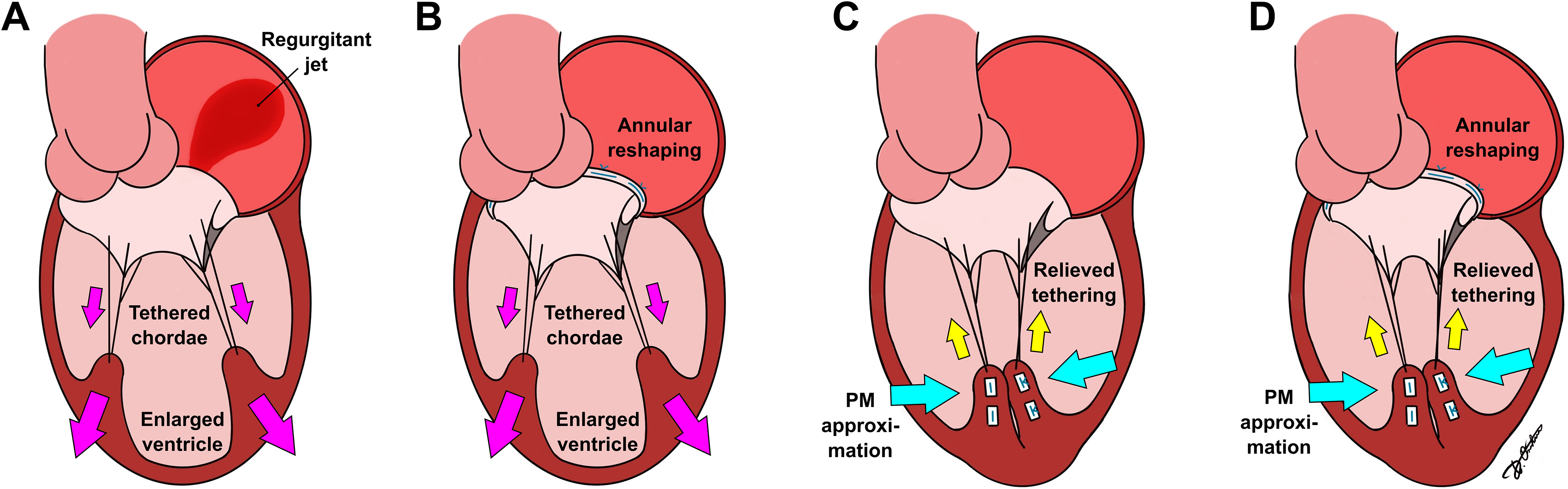
Schematic of FMR (A), mitral annuloplasty (B), PMA (C), and combination of PMA and annuloplasty ring (D).
Currently, FMR treatment strategies depend on the clinical presentation of patients. If the patient presents with FMR alone, they are likely to be referred for transcatheter mitral intervention with MitraClip, despite the data showing a relatively high rate of long-term FMR recurrence after such repair, especially in patients with dilated LVs.3,4 Meanwhile, if the patient has FMR but also requires coronary revascularization, surgery is the preferred option. In surgery, the MV is often replaced, as the only existing repair—undersizing mitral annuloplasty (Figure 1B)—has failed to yield durable outcomes. The randomized clinical trial by the Cardiothoracic Surgical Trials Network (CTSN) comparing undersized mitral annuloplasty to MV replacement for FMR repair demonstrated that annuloplasty failed in nearly 59% of the patients within 2 years. 5 Further dissecting the data from this trial reveals that more than 30% of the patients receiving annuloplasty had moderate degree of FMR at 30 days, indicating an inadequate repair to begin with. However, the very same trial provides strong evidence that a good index repair can yield better survival and LV reverse remodeling than a valve replacement. Therefore, there is a clear need for therapies that can repair FMR adequately and durably.
While undersizing mitral annuloplasty effectively reduces the dilated mitral annulus, it does not address the alterations in the subvalvular apparatus characteristic of FMR, such as increased interpapillary distance or restricted papillary muscle (PM) mobility, both of which contribute to persistent leaflet tethering and restricted MV closure in systole. Papillary muscle approximation (PMA) is a surgical technique that aims to restore the function of the subvalvular apparatus and repair FMR by drawing the PMs laterally and fixing them together (Figure 1C). 6
Our recently reported findings suggest that this technique might be an effective therapy to improve the outcomes in heart failure patients with FMR. A large animal study by King et al. 7 showed that PMA reduces the effective regurgitant orifice area of the MV and increases its systolic coaptation. Additionally, an ex vivo study by Zhan-Moodie et al. 8 demonstrated a significant reduction in leaflet tethering and improvement in leaflet mobility after PMA, leading to better valve coaptation. However, as PMA neither reduces present nor accounts for future annular dilation, the addition of an annuloplasty ring (Figure 1D) might be beneficial for patients with dilated LVs and FMR. Previous clinical studies have shown that combining mitral annuloplasty with PMA helps improve the MV function and reduce the recurrence rate of mitral regurgitation.6,9,10 Understanding the interaction between PMA and extent of annuloplasty would thus be relevant to clinical translation.
In this study, we sought to use computational models of the MV derived from swine with FMR to assess clinically relevant questions related to the translational potential of PMA. To the best of our knowledge, only a single simplified 2D computational study investigating PMA and its impact on the MV function has been published previously by Nappi et al. 11 This study used a highly idealized model of the MV; thus, the results were challenging to translate further. While several computational studies have used 3D geometries to investigate mitral annuloplasty,12–14 none have investigated the effects of sub-valvular PMA or the combination of PMA and annuloplasty. Therefore, the present study aims to address this gap. We recently published a conference paper assessing the benefit of adding differently sized annuloplasty rings to PMA in pigs with dilated ventricles. 15 In the present study, we expand this analysis by also evaluating mitral annuloplasty used independently and comparing it with PMA and the combination of both repair techniques. Additionally, we investigated the impact of ring sizing, both with and without PMA, on the effectiveness of FMR repair.
Materials and methods
Image-based MV model with FMR
Three distinct image-derived computational models of the MV were created from swine that were induced with a myocardial infarction and developed advanced heart failure and clinically significant FMR after 3 months. The details about the swine model were previously published by our team. 16 3D echo images of the left heart were obtained in these swine and used to create computational models of the MV. Specifically, MV annular geometry and its changes from end-diastole to peak systole, anterior and posterior leaflet geometries in diastole, and PM geometries, locations in the LV, and their motion from end-diastole to peak systole were segmented and derived from the imaging datasets. Since chordae are challenging to visualize from ultrasound images, a chordal distribution model reported in literature to best represent swine and human MVs was used, along with previously reported tissue material properties.
The animals received a myocardial infarction via percutaneous occlusion of the left circumflex artery (LCX) by injecting 200 proof (100%) ethanol into the LCX, which instantaneously coagulated blood and caused myocardial infarction. As a result, in a subsequent 3-month period, these swine developed ventricular dilation and FMR. Pigs were imaged at this 90-day endpoint, under general anesthesia, and by tunneling an ultrasound probe onto the roof of the left atrium via a sub-xyphoid incision. 3D full volume datasets were obtained using a Siemens Z6MS TEE probe on the ACUSON SC2000 Prime ultrasound system. The modeling workflow of this study (Figure 2) was based on the approach developed and validated previously 17 with the addition of subject-specific geometry of the PMs, thus allowing to create a computational model of the MV with a complete subvalvular apparatus included. Such a model can be used to test different FMR repair strategies and assess post-repair valve geometry and biomechanics.
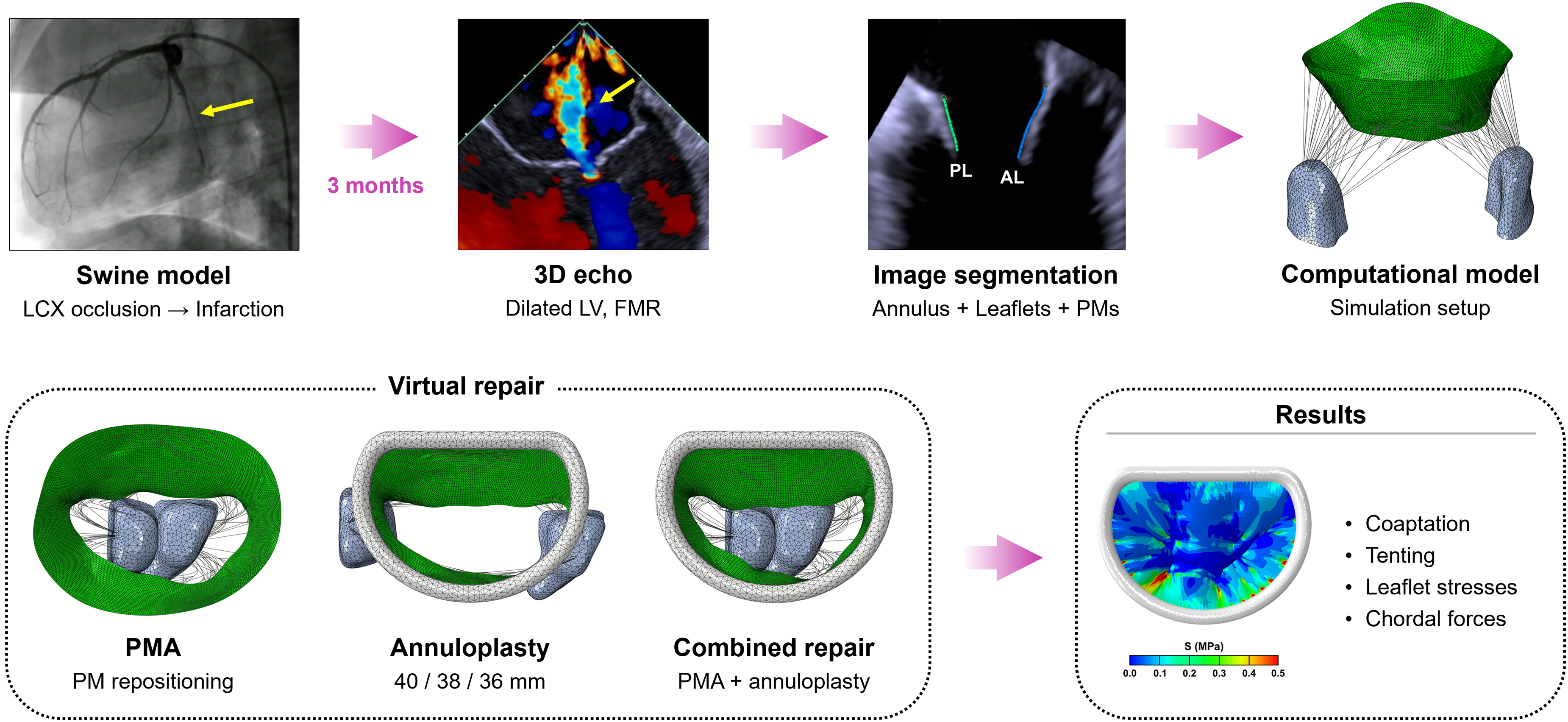
Schematic overview of the study workflow.
Briefly, for each 3D echo dataset, the geometries of the MV annulus and leaflets in diastole were semi-automatically reconstructed from echo images using proprietary software Siemens AutoValve and in-house written MATLAB code. Additionally, geometries of anteroposterior papillary muscle (APM) and posteromedial papillary muscle (PPM) were segmented manually in MATLAB, and realistic 3D models of both PMs were created. Each MV model was completed by adding a branched network of chordae, connecting the MV leaflets to the PMs. Since chordae are not visible on echo, an anatomically informed, literature-based chordal branching model developed according to ex vivo observations and prior studies12,18,19 was used. This chordal network was based on healthy hearts without any chordal tethering, thus chordae were pre-strained in the model to mimic the tethering forces that would be seen in FMR.
The reconstructed geometry of the MV with subvalvular apparatus was meshed, and material properties were prescribed. The MV leaflets were meshed using triangular shell elements (S3R in Abaqus), truss elements (T3D2) were used for the chordae, and for the PMs, tetrahedron solid elements (C3D4) were chosen, similar to previous studies on the MV modeling.12,20,21 To describe nonlinear and anisotropic mechanical behavior of the leaflets, we implemented the Fung-based anisotropic hyperelastic model proposed by Lee et al., 22 which effectively captures the stress–strain response of biological membranes and soft tissues. For nonlinear and isotropic mechanical behavior of the chordae, the third-order Ogden hyperelastic model was applied, following the approach of Caballero et al., 21 selected for its ability to represent the highly extensible nature of chordal tissue. Since in this study our primary focus was on the post-repair geometry and biomechanics of the MV leaflets and chordae only, the computational framework was simplified by assuming linear elastic and isotropic behavior of the PMs, with Young's modulus of 0.5 MPa and Poisson's ratio of 0.49; such values are characteristic to the LV myocardium.23,24 A schematic representation of the MV model development is shown in Figure 3.
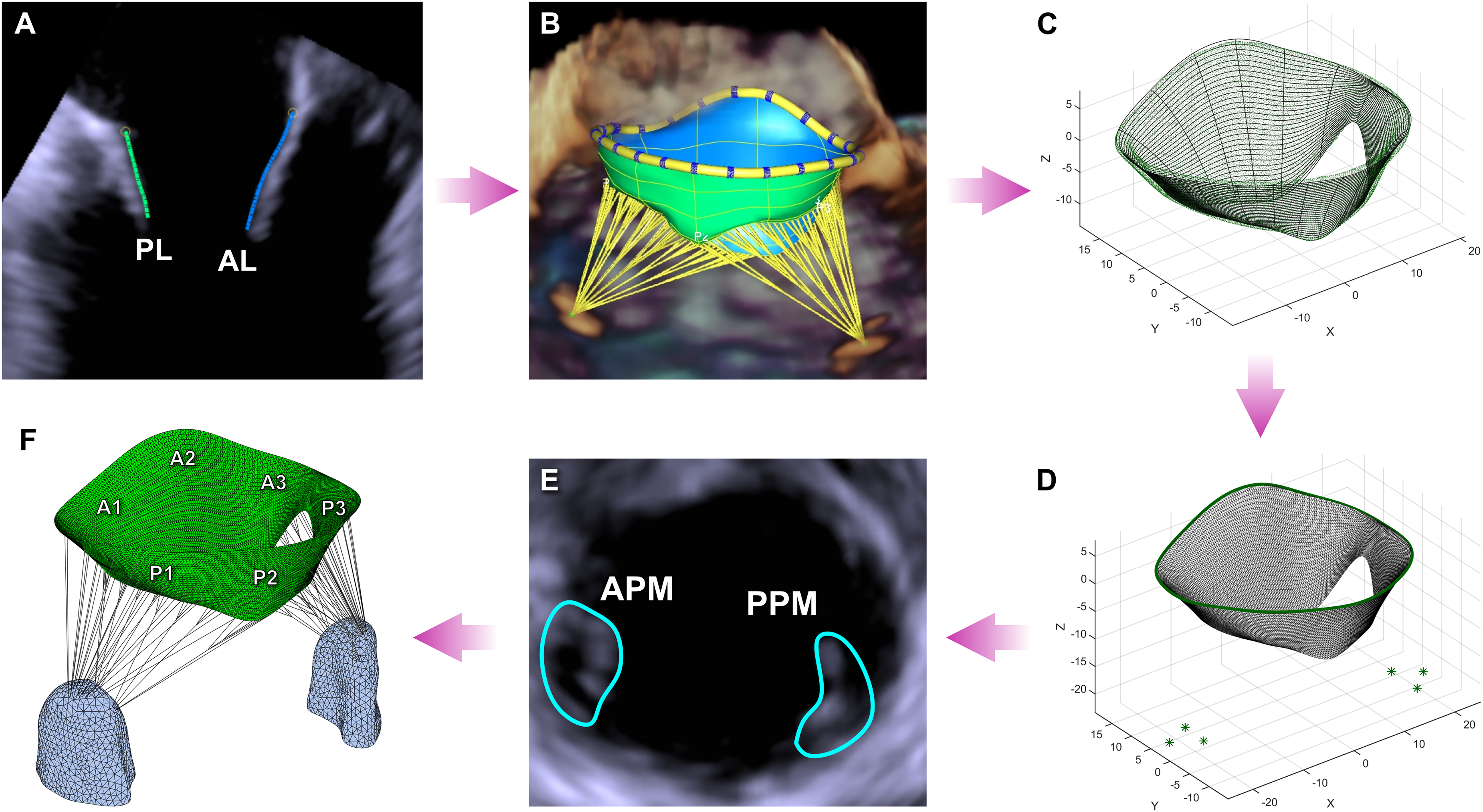
(A) Segmentation of the MV leaflets. (B) Visualization of the segmented geometry. (C) Approximation of leaflet profiles with splines. (D) Meshing of the segmented leaflet geometry. (E) Segmentation of the PMs. (F) Completed MV model in end-diastole.
The baseline configuration of each model used in this study represents anatomically accurate, subject-specific, image-derived FMR geometry in three swine. Chordal pre-straining, as done in the earlier studies,25–27 also accurately reproduced the tethered systolic valve configuration observed in FMR for each created computational model.
To simulate the MV closure before the repair, a physiological transvalvular pressure gradient with a peak value of 120 mmHg was applied to the leaflets. The motion of the annulus and the PMs was manually traced in echo images from end-diastole to peak systole, processed to reconstruct the field of time-varying displacements, and imposed on the mitral annulus and PMs as kinematic boundary conditions. A dynamic simulation in Abaqus/Explicit was performed, and the pre-repair peak systolic configuration of the MV was obtained in each investigated case. The explicit time integration scheme was chosen to avoid convergence issues common to implicit solvers in nonlinear contact problems. This approach is particularly well-suited for handling large deformations, complex contact interactions, and dynamic loading conditions, and has been widely used in previous computational studies on the MV biomechanics and repair techniques.12,20,21,25,27
The models were validated by comparing the computed systolic surfaces of the MV leaflets and the formation of the regurgitant gaps with echo data, as described in our previous work. 17 Good agreement was observed between the computational results and images, with a similar formation of regurgitant gaps across all models and echo data.
Computational modeling of FMR repair techniques
Papillary muscle approximation
The FMR repair modeling workflow used in this study is presented in Figure 4. PMA repair was simulated by prescribing displacements to the baseline APM and PPM positions in diastole to draw both muscles together until the bottom and tips of the two muscles approximated with each other. Systolic function of the MV was then simulated. To simulate valve closure, pressure was applied to the leaflets, and subject-specific annular contraction was prescribed as a kinematic boundary condition. The motion of the approximated PMs was determined by averaging the displacements of the APM and PPM and prescribing this computed displacement as a mutual boundary condition for both PMs. For each investigated case, a dynamic simulation of valve closure was performed, and the peak systolic configuration of the post-repair valve was obtained.
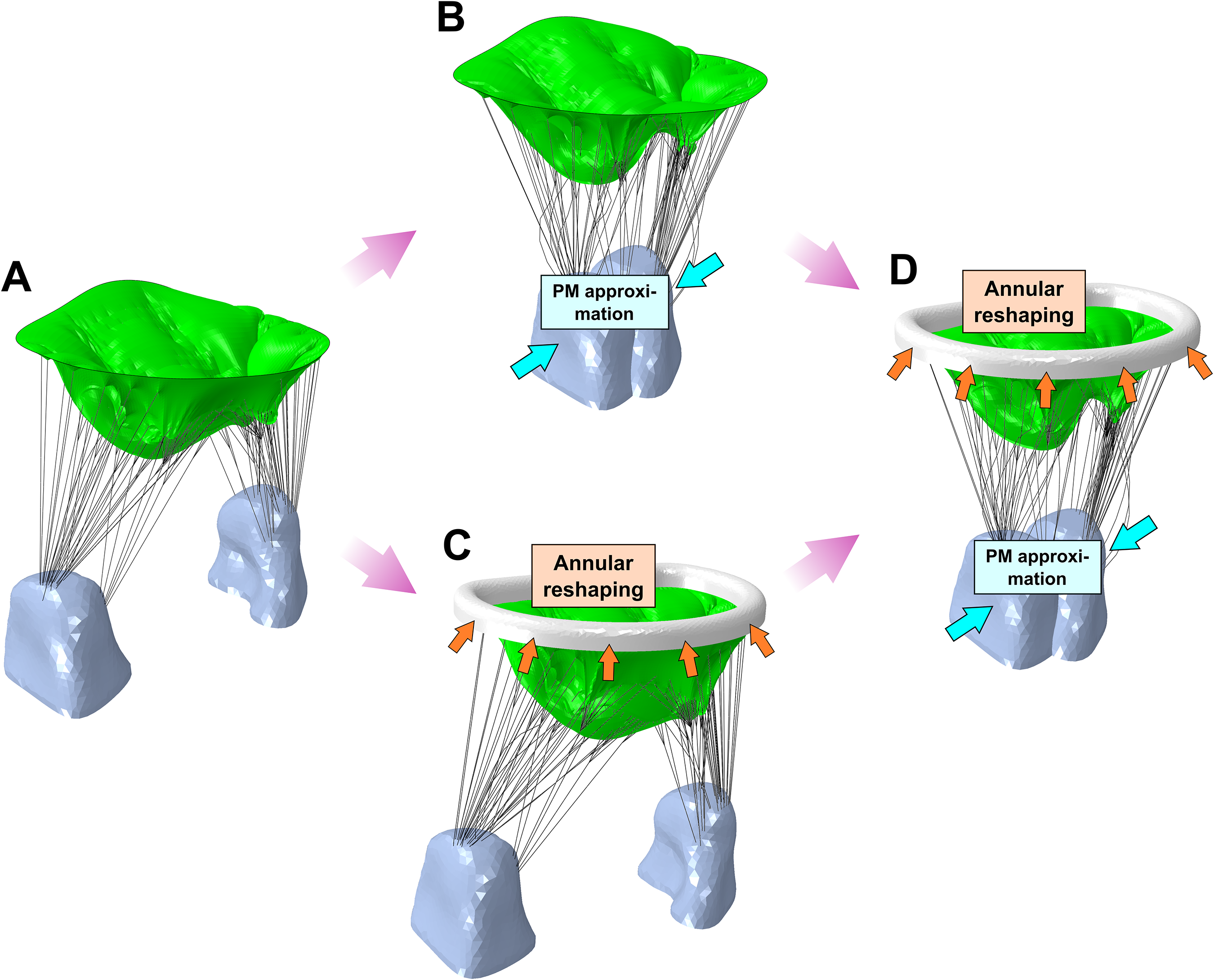
Modeling workflow for FMR repair: (A) pre-repair model with FMR, (B) PMA, (C) mitral annuloplasty, (D) combination of PMA and annuloplasty ring.
Mitral annuloplasty
Three annuloplasty ring models were created based on the shape and measurements of the Carpentier-Edwards Physio I ring. Given the similar annular dimensions among the investigated valves, a true-sized ring of 40 mm and two downsized rings of 38 mm and 36 mm were used in each case. For every valve model, all three rings were applied to reshape the mitral annulus in diastole, consistent with annular resizing performed on an arrested heart. Each annuloplasty ring was placed on the implied regions of the left and right fibrous trigones. The ring height was adjusted according to the positions of the MV commissures such that the intercommissural line of the mitral annulus and the XY-plane of the ring coincided. After the ring was positioned, the mitral annulus was deformed to match the ring's shape and size by prescribing the relevant displacements to the annular nodes.
Lastly, dynamic simulations were run for each model with different-sized rings. Physiological transvalvular pressure gradient was applied to the leaflets, and motion of the PMs was prescribed as a boundary condition. For the mitral annulus, a fixed boundary condition was applied to avoid deformation of the annulus or the ring during the MV closure. The systolic function of the MV after mitral annuloplasty was simulated, and the post-repair peak systolic configurations of the valves with the true-sized and downsized rings were obtained.
Combination of PMA and annuloplasty
The simulations of concomitant PMA and mitral annuloplasty were run after combining the steps described before. Firstly, PMA was performed by drawing the PMs and fixing them together as described in the earlier section. Afterward, the annuloplasty ring was positioned, and the mitral annulus was deformed to the ring configuration as described previously. To simulate valve closure, pressure was applied to the leaflets. The motion of the PMs was imposed as a boundary condition, while both mitral annulus and ring were fixed. For each investigated case, a true-sized ring of 40 mm and two downsized rings of 38 mm and 36 mm were used in combination with PMA. Peak systolic configuration of the post-repair valve was obtained in each model.
Data analysis
After each simulation—i.e., the pre-repair valve with FMR, isolated repair with PMA alone, isolated repair with mitral annuloplasty alone (three ring sizes), and the combination of PMA with the true-sized and downsized rings (three ring sizes)—the following parameters were calculated in systole: leaflet coaptation length at the A2-P2 region, coaptation area, tenting height and tenting area, excursion angles for the anterior leaflet (AL) and posterior leaflet (PL), stress distribution on the leaflets, and tension forces in the chordae. For all investigated cases, post-repair systolic results were compared with pre-repair values.
Results
Pre-repair valve model geometry and function
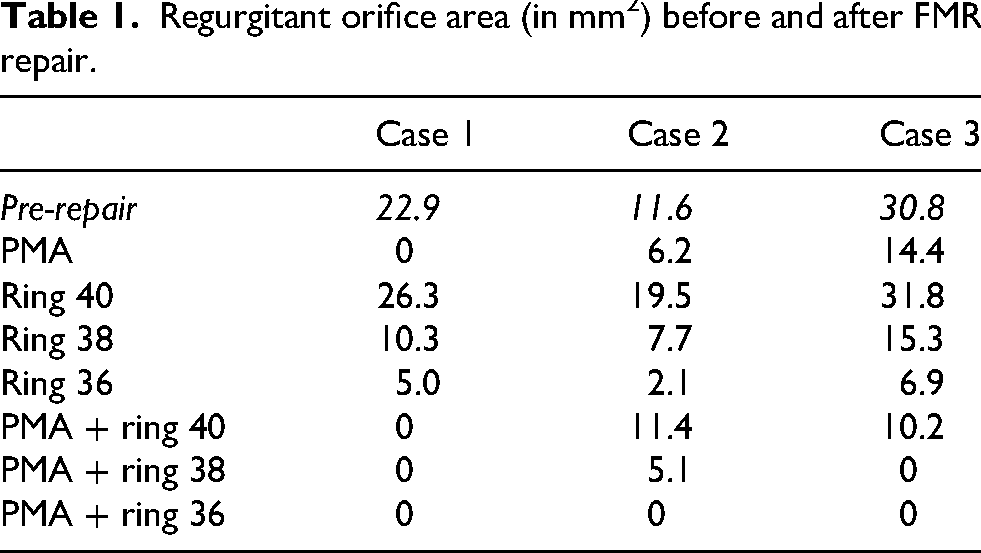
In diastole, all pre-repair MV models had a dilated mitral annulus, comparable to in vivo echocardiographic measurements on healthy porcine valves reported by us and others.28,29 On average, the MV annular area was 1120 ± 65 mm2, with anteroposterior (AP) diameter of 33.2 ± 1.0 mm and intercommissural (IC) diameter of 41.1 ± 1.3 mm. In systole, tethered valve geometry, lack of coaptation, and formation of regurgitant gaps were observed. The systolic annular area was 990 ± 64 mm2, AP diameter was 30.5 ± 1.4 mm, and IC diameter was 38.9 ± 1.2 mm. At 3 months in all the three swine, regurgitant orifices were observed at the transitional zones from A1-P1 to A2-P2 and A2-P2 to A3-P3. In cases 1 and 3, echocardiographic images showed a larger regurgitant jet at the A3-P3 region and a small jet at A1-P1. In case 2, a small jet was observed at A3-P3, while a larger jet was present at the A1-P1 region. Similar regurgitant gaps were observed in the pre-repair computational models, validating their use in this study. The regurgitant orifice area (ROA) measured in each model was 22.9 mm2 in case 1, 11.6 mm2 in case 2, and 30.8 mm2 in case 3.
The pre-repair leaflet coaptation length at the A2-P2 region was 2.3 ± 0.6 mm, which is substantially lower than the coaptation length measured in normal MVs.30,31 A small coaptation area of 84 ± 7 mm2 was noted as well. Compared to the reported in vivo data, 29 an increased tenting height of 10.9 ± 0.4 mm was observed, while the tenting area was 166 ± 2 mm2. Poor leaflet mobility was present, as reflected by the AL excursion angle of 24.7 ± 1.5° and PL excursion angle of 22.5 ± 2.8°. The areas of high leaflet stresses, exceeding the threshold value of 0.5 MPa, inherent to healthy valve,12,32,33 were found on both MV leaflets, near the insertion sites of the strut chordae, with the peak values reaching 1.48 ± 0.66 MPa. The elevated tension forces in the chordae, higher than the ones reported in the literature 8 and thus indicating the presence of the valve tethering, were calculated, with a total force of 24.8 ± 1.0 N.
The average results for the three pre-repair models are presented in Table 1.
Regurgitant orifice area (in mm2) before and after FMR repair.
Post-repair simulation results
Valve closure. In case 1, PMA eliminated both regurgitant gaps at the A1-P1 and A3-P3 regions. After annuloplasty alone, mitral regurgitation was corrected only at A1-P1, while the regurgitant gap at A3-P3 persisted both with the true-sized and downsized rings. The ROA of 26.3 mm2 was present with 40 mm, 10.3 mm2 with 38 mm, and 5.0 mm2 with 36 mm ring. Meanwhile, the combination of PMA and annuloplasty achieved complete correction of FMR regardless of the ring size.
In case 2, PMA reduced mitral regurgitation but was not able to completely eliminate the regurgitant gap at the A1-P1 region (ROA of 6.2 mm2). After mitral annuloplasty, regardless of the ring size, regurgitation at A1-P1 persisted as well (ROA of 19.5 mm2 with 40 mm, 7.7 mm2 with 38 mm, and 2.1 mm2 with 36 mm ring). The combination of PMA with the 40 mm and 38 mm rings reduced the gap at A1-P1, but regurgitation was still present (ROA of 11.4 mm2 with 40 mm and 5.1 mm2 with 38 mm ring). For this case, the complete elimination of FMR was achieved only when PMA was combined with the 36 mm annuloplasty ring.
In case 3, PMA eliminated regurgitation at A3-P3, but the gap at A1-P1, while reduced, remained present (ROA of 14.4 mm2). Mitral annuloplasty alone, regardless of the ring size, also resulted in residual FMR at the A1-P1 region (ROA of 31.8 mm2 with 40 mm, 15.3 mm2 with 38 mm, and 6.9 mm2 with 36 mm ring). After combining PMA with the true-sized ring, a gap at A1-P1 was still present (ROA of 10.2 mm2) and thus annular downsizing was needed. The addition of the 38 mm and 36 mm annuloplasty rings to PMA completely eliminated both regurgitant gaps in this model.
The changes in regurgitant orifice area following FMR repair across all cases and repair strategies are summarized in Table 1.
Leaflet coaptation. Compared to the pre-repair measurements, after PMA, the leaflet coaptation length at the A2-P2 region increased from 2.3 ± 0.6 mm to 3.5 ± 0.8 mm (increase by 56.1 ± 10.4%). Mitral annuloplasty with the true-sized ring increased coaptation to 2.8 ± 1.2 mm (increase by 18.4 ± 28%), while after annular downsizing, the coaptation length increased to 4.0 ± 0.6 mm with the 38 mm ring (increase by 79.7 ± 19.7%) and 4.8 ± 0.2 mm with the 36 mm ring (increase by 117.9 ± 45.4%). The combination of PMA and annuloplasty yielded similar outcomes: after PMA with the true-sized ring the coaptation length was 3.0 ± 0.8 mm (increase by 35.2 ± 42.8%), which increased to 4.0 ± 0.8 mm with the 38 mm ring (increase by 80.1 ± 38%) and 4.3 ± 0.2 mm with the 36 mm ring (increase by 97.7 ± 37.6%). However, a clinically adequate A2-P2 coaptation length, larger than 5 mm, was not achieved in any model. The comparison of the coaptation length before and after FMR repair for case 1 is shown in Figure 5.
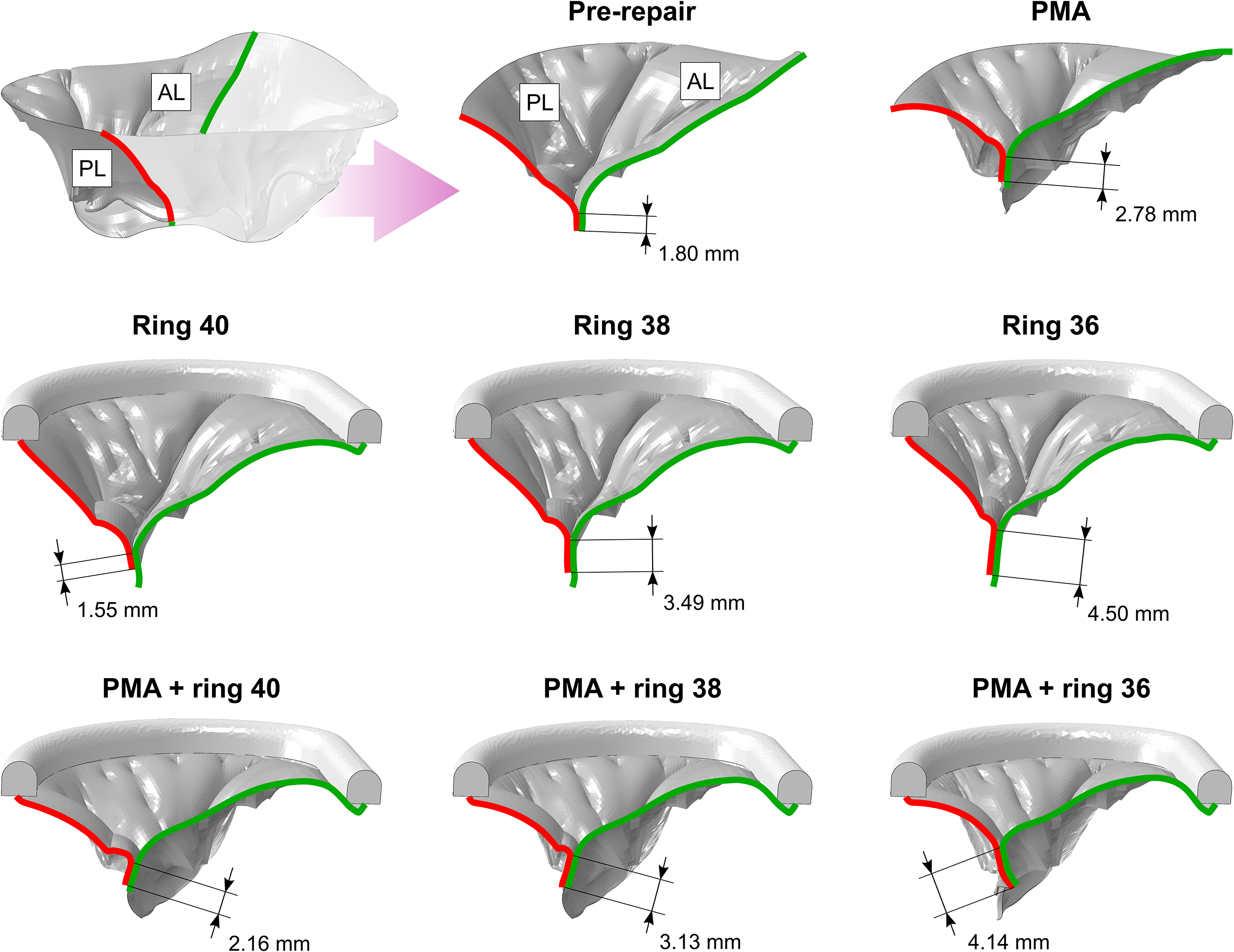
Coaptation length at A2-P2 before and after FMR repair (case 1).
In the pre-repair model, the leaflet coaptation area was measured at 84 ± 7 mm2. Following PMA, it increased to 110 ± 9 mm2 (increase by 30.6 ± 0.7%). Mitral annuloplasty alone resulted in the larger coaptation area, with smaller rings yielding greater increase: 136 ± 11 mm2 with the true-sized ring (increase by 62.1 ± 16.1%), 184 ± 12 mm2 with the 38 mm ring (increase by 120.1 ± 19.5%), and 233 ± 12 mm2 with the 36 mm ring (178.3 ± 16.5%). When PMA was combined with annuloplasty, the coaptation area increased to 155 ± 12 mm2 with the 40 mm ring (increase by 85.1 ± 24.8%), 199 ± 20 mm2 with the 38 mm ring (increase by 138.1 ± 36.6%), and 243 ± 15 mm2 with the smallest 36 mm ring (increase by 190.6 ± 37.6%).
Tenting height. All repair techniques used in this study reduced the tenting height of the MV, showing relieved valve tethering and improved leaflet mobility, but at different levels. After PMA, the tenting height was reduced from 10.9 ± 0.4 mm in the pre-repair model to 5.9 ± 0.9 mm (reduction by 45.8 ± 8.1%). Mitral annuloplasty showed less improvement, resulting in the tenting height of 8.2 ± 1.5 mm with the true-sized ring (reduction by 24.4 ± 16.4%), 7.3 ± 0.9 mm with the 38 mm ring (reduction by 32.7 ± 10.4%), and 6.7 ± 0.8 mm with the 36 mm ring (reduction by 38.0 ± 9.6%). Still, a clinically acceptable tenting height (less than 5 mm 34 ) was not achieved in any of the three models when only PMA or annuloplasty was performed. Meanwhile, combining both techniques allowed to achieve the targeted tenting height: 4.0 ± 1.7 mm with the 40 mm ring (reduction by 63.0 ± 16.5%), 3.5 ± 1.4 mm with the 38 mm ring (reduction by 67.8 ± 14%), and 2.9 ± 1.3 mm with the 36 mm ring (reduction by 72.8 ± 12.5%).
Similarly, all repair techniques led to a reduction in the MV tenting area. After PMA, the tenting area decreased from 166 ± 2 mm2 to 90 ± 14 mm2 (reduction by 45.8 ± 8.1%). After mitral annuloplasty alone, it was measured at 122.4 ± 22.4 mm2 with the true-sized ring (reduction by 26.3 ± 12.7%), 102.6 ± 12.6 mm2 with the 38 mm ring (reduction by 38.2 ± 6.9%), and 89.4 ± 10.9 mm2 with the 36 mm ring (reduction by 46.1 ± 6.0%). The concomitant PMA and annuloplasty yielded the smallest tenting area: 59.7 ± 25.4 mm2 with the 40 mm ring (reduction by 64.1 ± 15.0%), 48.9 ± 20.3 mm2 with the 38 mm ring (reduction by 70.6 ± 12.0%), and 39.1 ± 17.5 mm2 with the 36 mm ring (reduction by 76.5 ± 10.4%).
Leaflet mobility
To assess the leaflet mobility, the systolic and diastolic angles of both leaflets were measured. The excursion angles, representing the extent of leaflet motion, were then calculated as the difference between the systolic and diastolic angles. For the AL, PMA increased the excursion angle from 24.7 ± 1.5° to 41.3 ± 2.3° (increase by 68.2 ± 16.2%). After annuloplasty, the AL excursion angle increased to 36.6 ± 3.5° with the true-sized ring (increase by 49.2 ± 21.3%), 39.5 ± 2.7° with the 38 mm ring (increase by 61 ± 19.5%), and 41.1 ± 2.9° with the 36 mm ring (increase by 67.4 ± 21.2%). The concomitant PMA and annuloplasty achieved the best outcomes: 47.4 ± 4.0° with the 40 mm ring (increase by 92.8 ± 21.7%), 49.9 ± 3.9° with the 38 mm ring (increase by 103.0 ± 23.3%), and 52.3 ± 3.5° with the 36 mm ring (increase by 112.8 ± 21.6%).
The leaflet mobility of the PL increased in a manner similar to that of the AL. After PMA, the excursion angle increased from 22.5 ± 2.8° to 38.3 ± 3.4° (increase by 73.6 ± 38.7%). After annuloplasty, the excursion angle increase was minimal: 29.7 ± 2.2° with the 40 mm ring (increase by 34.1 ± 24.7%), 32.9 ± 1.0° with the 38 mm ring (increase by 47.9 ± 22.2%), and 36.3 ± 2.0° with the 36 mm ring (increase by 63.9 ± 30.2%). Again, the best repair outcomes were obtained after the combination of PMA and annuloplasty, increasing the PL excursion angle to 43.2 ± 5.8° with the true-sized ring (increase by 96.5 ± 53.2%), 49.0 ± 6.4° with the 38 mm ring (increase by 122.7 ± 60.2%), and 53.8 ± 7.2° with the 36 mm ring (increase by 144.7 ± 66.9%).
Leaflet stresses. After PMA, the leaflet stresses were reduced in all models, with the peak stress decreasing from 1.48 ± 0.66 MPa to 1.08 ± 0.51 MPa (reduction by 26.9 ± 3.9%). After mitral annuloplasty with the 40 mm and 38 mm rings, the peak leaflet stress increased to 1.97 ± 0.96 MPa (increase by 30.0 ± 15.0%) and 1.58 ± 0.71 (increase by 6.0 ± 2.8%), respectively. Only the smallest ring of 36 mm allowed to reduce the peak stress to 1.2 ± 0.39 MPa (reduction by 15.5 ± 12.9%). The combination of both techniques resulted in better repair outcomes than PMA or annuloplasty alone. In case 1, adding the true-sized ring to PMA increased the peak leaflet stress, while in cases 2 and 3, the stress reduction was observed after the addition of the true-sized annuloplasty. On average, the addition of the true-sized ring reduced the peak stress on the P2 cusp to 1.33 ± 0.72 MPa (reduction by 10.7 ± 16.4%). Adding smaller rings to PMA further reduced stresses, with the peak value decreasing to 1.03 ± 0.43 MPa (38 mm ring; reduction by 29.9 ± 2.2%) and 0.80 ± 0.26 MPa (36 mm ring; reduction by 43.7 ± 8.8%). The pre- and post-repair leaflet stress distribution for case 1 is shown in Figure 6.
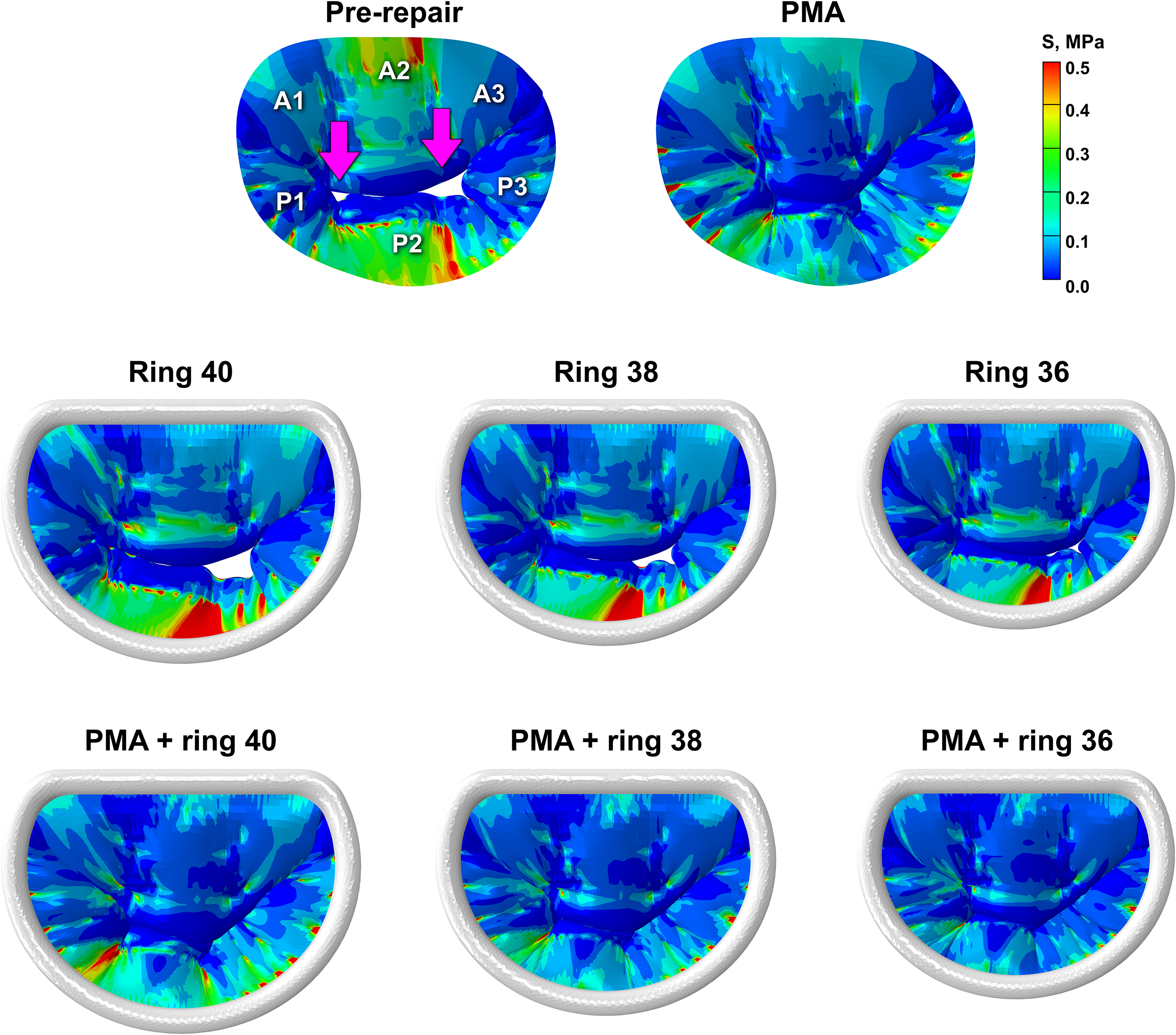
Leaflet stress distribution in peak systole (case 1).
Chordal tension forces. On average, after PMA alone, the total chordal tension force was reduced from 24.8 ± 1.0 N to 19.9 ± 0.8 N (reduction by 19.8 ± 1.2%). After mitral annuloplasty with the true-sized ring, the force increased to 27.6 ± 2.3 N, which was observed (increase by 10.1 ± 14.4%). The smaller rings allowed to reduce the total force to 22.8 ± 1.6 N (38 mm ring; reduction by 7.8 ± 10.1%) and 20.0 ± 0.7 N (36 mm ring; reduction by 19.1 ± 6.0%). Adding the true-sized ring to PMA reduced the force to 20.7 ± 0.6 N (reduction by 16.4 ± 5.7%). Using the smaller rings in combination with PMA reduced the total chordal force to 17.0 ± 0.3 N (38 mm ring; reduction by 31.2 ± 3.6%) and 14.1 ± 0.1 N (36 mm ring; reduction by 43.0 ± 2.2%).
The average post-repair simulation results are shown in Table 2.
The impact of FMR repair techniques on valve geometry and biomechanics.

Worst repair outcome.
Best repair outcome.
Discussion
In this study, we used computational modeling to investigate the impact of sub-valvular PMA, mitral annuloplasty, and a combination of both techniques for the repair of FMR in dilated ventricles. The approach we used allows us to test different FMR repair strategies in a patient-specific anatomical framework, providing insights into post-repair MV biomechanics and the overall effectiveness of the repair. While the present study is based on a limited number of subject-specific models (N = 3), consistent trends were observed across all cases and repair strategies. Our simulation results suggest that isolated PMA alone reduces the regurgitant gaps but might not repair FMR completely. Of the three cases investigated in this study, after PMA, the regurgitant gaps were still present in two models (cases 2 and 3), and therefore annular reshaping was needed. Isolated mitral annuloplasty alone fared worse, with persistent FMR in all the models regardless of the ring size used (40 mm, 38 mm, or 36 mm). As we showed in our previous study, 35 using mitral annuloplasty alone, an excessive annular downsizing might be needed to eliminate regurgitation, which comes at the expense of mitral stenosis and LV dysfunction. For the models used in the current study, downsizing to 36 mm was not sufficient and thus smaller rings might be needed. Meanwhile, the combination of PMA and annuloplasty yielded better outcomes even without an excessive annular downsizing. A complete elimination of the regurgitant gaps was achieved with the true-sized ring in case 1, the 36 mm ring in case 2, and the 38 mm ring in case 3. These results suggest that neither PMA nor mitral annuloplasty alone is consistently sufficient in the dilated ventricles, and that a combined approach with the true-sized ring or slight annular downsizing is needed to achieve FMR repair.
The improvement in the leaflet coaptation and reduction in tenting were evident after isolated PMA, as the A2-P2 coaptation length and coaptation area increased, while tenting height and tenting area were reduced. However, the restored coaptation fell short of the clinically adequate threshold of 5 mm, and the acceptable tenting height of less than 5 mm was not reached. Despite PMA relieving the tethering forces and enabling better leaflet mobility and thus improving leaflet coaptation, persistent annular dilation may impose peak systolic tethering forces that might resist restoration of optimal valve closure. After mitral annuloplasty with the true-sized ring, the A2-P2 coaptation length was less than that achieved with PMA. Both downsized rings showed improvements in the leaflet coaptation, but none of the models reached a clinically acceptable 5 mm coaptation length. Furthermore, the increased tenting height observed in all pre-repair models was not reduced enough to meet the 5 mm target. The inability of mitral annuloplasty to restore physiological valve closing geometry is a known fact, as drawing the posterior annulus inwards into the mitral orifice results in increased tethering forces on the posterior marginal and strut chordae. Often, this results in immobilization of the PL after annuloplasty, which does not yield optimal hemodynamic outcomes. The combination of the true-sized annuloplasty ring and PMA further improved the tenting parameters but was less successful in improving the coaptation length than PMA alone. Meanwhile, the addition of the downsized rings to PMA improved both leaflet tenting and coaptation. A clinically acceptable tenting height was achieved in all simulations; however, none of the models attained the target coaptation length of 5 mm. These results indicate that achieving the optimal coaptation length remains a significant challenge, requiring further refinement in FMR repair strategies.
In all pre-repair models, both leaflets had reduced the excursion angles, reflecting restricted mobility caused by the leaflet tethering. PMA led to a noticeable increase in the excursion angles for both leaflets, indicating reduced tethering as a result of the papillary muscle repositioning. Mitral annuloplasty, even with the 36 mm ring, resulted in smaller excursion angles compared to PMA, suggesting that annuloplasty alone may be insufficient to effectively relieve the leaflet tethering. In contrast, the combination of PMA with annuloplasty led to the most substantial improvement in the leaflet mobility, both with the true-sized and downsized rings. These results suggest that while PMA effectively addresses tethering, combining it with mitral annuloplasty further enhances leaflet mobility, enabling improved valve function after FMR repair without requiring excessive annular downsizing.
From a biomechanical perspective, PMA reduced leaflet stresses and chordal tension forces, once again indicating the relief of leaflet tethering. In addition, more uniform stress distribution across the whole surface of the leaflets was achieved, as shown in Figure 6, and more uniform force distribution across the entire chordal network was observed as well. In contrast, mitral annuloplasty with the true-sized ring resulted in an increase in leaflet stresses and chordal forces compared to the pre-repair. With the downsized rings, chordal forces were reduced but remained slightly higher than after PMA. Meanwhile, leaflet stresses still increased with the 38 mm ring and were reduced only with the 36 mm ring. However, even with this smallest ring, leaflet stress distribution remained uneven, with the high stress concentration on the P2 cusp, which was not present after PMA. These findings indicate that annuloplasty alone was less effective in relieving tethering-related biomechanical loading, as PMA achieved not only better stress reduction but also more uniform stress distribution across the surface of the leaflets. Meanwhile, adding different annuloplasty ring sizes to PMA consistently reduced leaflet tethering, with the 36 mm ring achieving the lowest stresses and forces. This suggests that PMA combined with mitral annuloplasty may potentially improve long-term durability of the repair, as reduced tethering lowers the likelihood of structural damage to the valve and FMR recurrence.
Although smaller annuloplasty rings, such as 36 mm size, seem to be the most beneficial when applied in combination with PMA, their use in the dilated ventricles is not without potential drawbacks. In certain cases, excessive downsizing can lead to restricted leaflet mobility and increased leaflet stresses, 36 increasing the likelihood of leaflet perforation or chordal rupture over time. Moreover, overly aggressive downsizing may distort the native annular geometry, leading to non-physiological valve dynamics and potentially impairing LV filling. 37 In addition, reduced valve opening may contribute to mitral stenosis. Therefore, careful consideration of ring size and individual patient anatomy is important to optimize repair outcomes and minimize post-repair complications.
To sum up, while PMA alone showed good outcomes, the addition of mitral annuloplasty was beneficial for FMR repair, confirming the findings reported in previous clinical studies.6,9,10 When used alone, mitral annuloplasty with the true-sized ring provided only limited improvements in valve geometry and biomechanics. Although the use of the downsized rings yielded more favorable outcomes, the complete FMR repair was not achieved with any ring size and most of the parameters calculated during simulations were inferior compared to those observed after PMA alone or the combination of PMA and annuloplasty. Notably, even the true-sized ring (40 mm) combined with PMA outperformed mitral annuloplasty with the smallest ring (36 mm), indicating more effective repair without the need for excessive annular downsizing. Overall, mitral annuloplasty added to PMA was the most beneficial for FMR repair, as it improved both MV geometry and biomechanics and thus yielded better repair outcomes.
The data from this study should be considered with some limitations in mind. First, diastolic analysis was limited to the characterization of annular geometry, while valve function in diastole was not assessed. In addition, the clinical application of FMR repair techniques requires consideration of procedural safety, reproducibility, and potential morbidity, which were not evaluated in this computational study. Moreover, in current clinical practice, surgical treatment of FMR is commonly performed in conjunction with coronary revascularization, and isolated surgical intervention is relatively uncommon. The present study evaluates repair strategies in an isolated setting and does not account for the effects of revascularization or subsequent ventricular remodeling.
While our work convincingly demonstrates that PMA can lead to improved leaflet stress distribution and coaptation, whether these favorable biomechanical changes translate into long-term durability of the repair can only be extrapolated. Therefore, the results should be viewed as providing mechanistic insights into repair strategies rather than direct predictors of clinical benefit or a recommendation to perform PMA in patients based solely on this study. Given that PMA is a relatively new technique, its long-term impact on valve function and geometry, including the risk of elevated MV gradients, warrants further investigation.
Footnotes
Authors’ contribution
G.G. conceived the computational study design, performed modeling and simulations, analyzed data, and drafted the manuscript. K.K. contributed to clinical interpretation and manuscript revision. M.P. contributed to study conception, experimental design, supervision, interpretation of results, and manuscript revision. All authors reviewed and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the National Heart, Lung, and Blood Institute through grants HL133667, HL135145, and HL140325 to M.P., and infrastructure support from the Carlyle Fraser Heart Center at Emory University Hospital Midtown. It was also funded by the American Heart Association through a postdoctoral fellowship grant 23POST1022468 to G.G.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M.P. discloses employment, stock ownership, and officer role in Nyra Medical, Inc., and receiving consulting fees from Heart Repair Technologies, Inc. None of these entities funded, reviewed, or approved this work. G.G. and K.K. have no financial relationships to disclose.