
Abstract
Background:
Hepatitis B virus (HBV) infection remains a major public health problem in sub-Saharan Africa, including Ethiopia, where adult vaccination uptake is limited. While quantitative studies have assessed knowledge and attitudes, little is known about how culturally embedded beliefs shape community perceptions of HBV transmission and vaccination.
Objectives:
This study explored adult community perspectives on HBV transmission and vaccination in Northwest Ethiopia.
Design:
A qualitative study using conventional content analysis.
Methods:
The study was conducted in Debre Tabor between December 2025 and February 2026. Data were collected through 20 in-depth interviews and six focus group discussions involving 68 adults selected through purposive sampling. Interviews were conducted in Amharic, audio-recorded, transcribed verbatim, translated into English, and analyzed inductively using Open Code software. Trustworthiness was ensured through independent coding, member checking, and reflexive documentation.
Results:
Three major themes emerged: (1) fragmented knowledge and moral framing of risk, (2) coexistence of biomedical and cultural explanatory models, and (3) the vaccine paradox-acknowledged benefits amid persistent barriers. A dominant culturally embedded belief attributed HBV to bat exposure (“wof zura”), often reducing the perceived relevance of vaccination. Although participants recognized disease severity, perceived personal susceptibility was low and frequently linked to moral behavior. Structural barriers including limited awareness of adult vaccination, cost concerns, and uncertainty about service availability further constrained uptake. Healthcare provider recommendation and community-based health education were identified as key facilitators.
Conclusion:
HBV vaccination decisions among adults are shaped by culturally grounded explanatory beliefs, low perceived susceptibility, and structural barriers. Context-sensitive health education and strengthened provider-initiated recommendations are critical for improving adult HBV vaccine uptake, thereby contributing to the global goal of eliminating viral hepatitis as a public health threat by 2030.
Plain language summary
Hepatitis B is a serious liver infection that can cause long-term illness and death, but it can be prevented with vaccination. Despite this, many adults in Ethiopia are not vaccinated. We conducted interviews and group discussions with adults in Debre Tabor, Northwest Ethiopia, to understand their views. Although most participants had heard of hepatitis B, knowledge was often limited. Many believed the disease is caused by exposure to bats (“wof zura”) rather than by a virus spread through blood or sexual contact. This belief reduced the perceived importance of vaccination. Some people also felt they were not at risk because they associated infection with “immoral behavior.” While vaccination was generally viewed positively, barriers such as low awareness of adult services, cost concerns, and lack of provider recommendation limited uptake. Clear health education and stronger provider advice may improve adult vaccination coverage
Keywords
Introduction
Hepatitis B virus (HBV) infection is a major global public health concern, affecting an estimate 296 million people worldwide and causing approximately 820,000 deaths annually due to cirrhosis, liver failure, and hepatocellular carcinoma.1,2 The disease burden is disproportionately high in low-and middle-income countries, particularly in sub-Saharan Africa and East Asia, where HBV prevalence remains intermediate to high. 3 In Ethiopia, the national prevalence of chronic HBV infection ranges between 6% and 8%, with considerable regional variation. Northwest Ethiopia, like other parts of the country, continues to experience a substantial burden of HBV infection, which contributes to preventable morbidity and mortality among adults.4,5
HBV is primarily transmitted through exposure to infected blood and body fluids, unsafe medical injections, sexual contact, and vertical transmission from mother to child.1,6 Despite the existence of an effective and safe vaccine, vaccination coverage remains suboptimal in many communities, partly due to low awareness, sociocultural beliefs, limited healthcare access, and misinformation.7,8 In addition to vaccination, strategies such as safe injection practices, screening of blood products, and health education are crucial components of HBV prevention and control. Understanding community perceptions of HBV transmission and vaccination is critical for the design and implementation of effective public health interventions.8,9 Community beliefs, attitudes, and behaviors directly influence vaccine uptake, adherence to preventive measures, and acceptance of healthcare interventions.10–12
In Ethiopia, previous research has largely focused on quantitative assessments of knowledge, attitudes, and practices (KAP) among specific populations, including healthcare workers, school-aged children, and pregnant women.13–15 While these studies provide useful information on general awareness levels, they often fail to capture the deeper sociocultural factors, lived experiences, and contextual realities that shape health-related behaviors in diverse communities.
Qualitative research methods, including in-depth interviews and focus group discussions, allow for the exploration of the complex social, cultural, and behavioral factors influencing health practices.16,17 Such qualitative methods enable researchers to uncover community narratives, beliefs, misconceptions, and barriers related to HBV transmission and vaccination, which cannot be adequately captured through quantitative surveys alone. 18 Despite the high burden of HBV and the public health significance of vaccination, there is limited qualitative evidence exploring adult community perspectives on HBV in Ethiopia, particularly in the northwest region. Existing Ethiopian studies largely rely on quantitative assessments among specific subgroups, leaving the perspectives of the broader adult community underexplored. To our knowledge, no prior qualitative study has explored adult community perspectives on HBV transmission and vaccination in Northwest Ethiopia. Understanding these perceptions is critical, as adults influence household health decisions and vaccine uptake. Context-specific insights are essential to design culturally responsive and effective HBV prevention strategies.
Addressing this gap is essential to inform context-specific, culturally sensitive, and effective public health strategies. By understanding how adults perceive HBV transmission, the benefits and risks of vaccination, and the social or cultural factors influencing health-seeking behavior, policymakers and healthcare providers can design interventions that are more acceptable, feasible, and sustainable. 19 Moreover, such evidence contributes to the global effort to reduce HBV-related morbidity and mortality, aligning with the World Health Organization’s goal of eliminating viral hepatitis as a major public health threat by 2030. 7
The study was conceptually informed by the health belief model (HBM), which posits that health-related behaviors are influenced by individuals’ perceptions of susceptibility to a disease, perceived severity of the condition, perceived benefits of preventive action, perceived barriers to action, cues to action, and self-efficacy. 20 Given that decisions regarding HBV vaccination are shaped by beliefs about infection risk, disease consequences, vaccine safety, and healthcare access, the HBM provides a useful lens to understand how adults interpret HBV transmission and prevention within their sociocultural context. Although the analysis remained inductive, the HBM informed the interpretation of findings related to perceived risk, vaccination attitudes, and behavioral intentions. 21
Therefore, this study aims to explore the perceptions, beliefs, and experiences of adults in Northwest Ethiopia regarding HBV transmission and vaccination using a qualitative approach. The findings are expected to provide in-depth insights into community understanding, identify barriers and facilitators to vaccine uptake, and inform evidence-based strategies for HBV prevention and control in similar low-resource settings. In this study, HBM will serve as a conceptual lens to interpret participants’ perceptions, beliefs, and experiences, guiding both the analysis and discussion of barriers and facilitators to preventive behavior.
Methods
Study design
A conventional qualitative content analysis approach was employed to explore community perceptions of HBV transmission and vaccination. This methodological orientation allows themes and categories to emerge inductively from participants’ narratives without imposing pre-existing theoretical frameworks. The approach was selected to generate an in-depth contextual understanding of beliefs, attitudes, and social norms influencing HBV-related behaviors. The study was designed and reported in accordance with the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines 17 to ensure methodological rigor and transparency.
Study setting and period
The study was conducted among adult residents of Debre Tabor city, Northwest Ethiopia, between December 2025 and February 06, 2026. The data collection phase, including in-depth interviews and focus group discussions, was conducted between December 07, 2025 and January 16, 2026, with data analysis conducted from January 24 to February 06, 2026. Debre Tabor is an urban center with a diverse socio-demographic composition, representing various age groups, educational backgrounds, and occupations. The city was selected as the study site because of the limited published data on community awareness, perceptions, and practices related to HBV transmission and vaccination. Conducting the study in this setting allowed for an in-depth exploration of local community perspectives within an urban Ethiopian context.
Study population
The study population consisted of adult residents of Debre Tabor city aged 18 years and above. Eligible participants were those who had lived in the city for at least 6 months, ensuring sufficient exposure to local social norms, health services, and community interactions relevant to HBV knowledge and vaccination practices. Participants were required to be able to communicate in Amharic, the primary language of the area, to facilitate effective interviews and discussions. Individuals were excluded if they were severely ill, mentally incapacitated, or otherwise unable to provide informed consent, as these conditions could affect their ability to participate fully in the interviews or focus group discussions. The study aimed to include a diverse range of participants, representing different ages, genders, educational levels, and occupations to capture heterogeneous perspectives and provide a comprehensive understanding of community beliefs, attitudes, and practices related to HBV transmission and vaccination. This approach ensured that the findings would reflect the breadth and complexity of community perceptions, enhancing the credibility and transferability of the results to similar urban Ethiopian settings.
In this study, community perspectives refer to the collective beliefs, attitudes, and experiences of adult residents regarding HBV transmission and vaccination. Perceptions of HBV transmission encompass participants’ beliefs about how HBV spreads, including scientifically recognized routes (e.g., blood and body fluids) as well as perceived or misconceived modes. Awareness of HBV indicates the extent to which participants have heard about HBV and possess general knowledge of its causes, transmission, prevention, and consequences. HBV vaccination was understood as the administration of the hepatitis B vaccine for prevention, and beliefs about vaccination-included participants’ views on its benefits, risks, safety, effectiveness, and necessity. Barriers to vaccine uptake were defined as factors perceived to hinder the acceptance or utilization of vaccination, such as misinformation, fear of side effects, cultural beliefs, access issues, cost, or trust in healthcare services.
Sampling and recruitment
Purposive sampling was used to recruit participants with diverse characteristics, including age, sex, education, occupation, and urban residence, to maximize the variability of perspectives. Recruitment continued until data saturation reached the point at which no new themes emerged during the analysis. Community leaders and health extension workers assisted in identifying eligible participants and facilitating contact. The involvement of health extension workers, who are trusted community members, facilitated rapport-building and encouraged participants to share their perspectives openly.
Data collection
Data were collected between December 07, 2025 and January 16, 2026, using semi-structured in-depth interviews (IDIs) and focus group discussions (FGDs) to capture both individual experiences and shared community perspectives regarding HBV transmission and vaccination. Focus group discussions were organized to ensure heterogeneity in perspectives while maintaining a comfortable discussion environment. Groups were composed to include participants of similar community status, with attention to gender balance, although strict stratification by age or gender was not applied. Participants in IDIs and FGDs were distinct and non-overlapping, allowing for both in-depth individual perspectives and broader community-level insights without duplication of responses. A semi-structured interview guide (Supplemental File) developed by the principal investigator focused on participants’ knowledge of hepatitis B and its modes of transmission, perceptions of susceptibility and disease severity, beliefs about vaccination and preventive practices, sources of health information and trust in healthcare providers, and barriers and facilitators to vaccine uptake. The guide was validated through content, face, and expert review and translated into Amharic to ensure clear communication with participants.
IDIs were conducted with 20 participants, focusing on personal experiences, beliefs, and perceptions of HBV. FGDs included eight participants per group, with six FGDs, allowing exploration of community norms and collective attitudes toward HBV and vaccination. All interviews and discussions were conducted face-to-face in private and convenient locations, lasting approximately 45–70 min per session. They were audio-recorded with participants’ verbal consent and supplemented by detailed field notes capturing non-verbal cues and contextual information. The interviewers, all holding a Master’s degree, had received in-house training in systematic review, meta-analysis, and qualitative research methods through their institute, though not formally certified. In addition, they had prior experience conducting qualitative studies and prior experience in qualitative research. They had no previous personal relationship with the participants, ensuring neutrality and minimizing bias. Data collection continued until thematic saturation was reached, defined as the point when no new themes or insights emerged from additional interviews or discussions. This approach allowed the research team to determine that further data collection was unlikely to yield additional meaningful information. There were no dropouts, and all planned interviews and discussions were successfully completed.
Data quality assurance
To ensure data quality, multiple assurance measures were implemented throughout the study. The data collection tool was pretested on a small sample of eligible patients at Debre Markos town to assess clarity, relevance, and consistency, and necessary modifications were made accordingly. Data collectors and supervisors received comprehensive training on the study objectives, ethical considerations, and standardized data collection procedures. During the data collection period, supervisors conducted daily reviews of completed tools to check for completeness and internal consistency, providing immediate feedback and corrective guidance when required. All interviews were audio-recorded with participants’ consent to enhance data accuracy, and verbatim transcriptions were cross-checked against the original recordings before data analysis.
Handling of missing data
To minimize missing data and ensure the completeness and credibility of the qualitative findings, rigorous data management procedures were implemented. These included comprehensive training of interviewers, pretesting of the interview guide, and systematic review of audio recordings and field notes. During data collection, unclear or incomplete responses were addressed through appropriate probing techniques and, when necessary, follow-up discussions with participants. All interview transcripts were carefully cross-checked against the original audio recordings to verify accuracy and completeness. Decisions related to handling incomplete or ambiguous data were thoroughly documented to enhance transparency, dependability, and analytical rigor.
Data analysis
All interviews were audio-recorded with participants’ consent, transcribed verbatim, and translated into English. The transcripts were cross-checked against the original audio recordings to ensure accuracy and completeness. Translation was performed by bilingual researchers familiar with both the local language and cultural context, with additional verification against audio data to maintain fidelity. Culturally specific terms and expressions (e.g., “wof zura”) were retained and explained to preserve their contextual meaning. Data were analyzed thematically using an inductive approach, allowing codes and themes to emerge directly from the data rather than being guided by a pre-existing coding framework. Initial coding was performed using Open Code software (version 4.03) to facilitate systematic data organization and management. Line-by-line coding was conducted based on participants’ narratives, with codes iteratively refined as the analysis progressed. To enhance analytical rigor and credibility, two researchers independently coded the transcripts. Discrepancies in coding were discussed and resolved through consensus, resulting in the development of a shared and coherent coding framework.
Rigor and trustworthiness
To ensure methodological rigor and enhance the trustworthiness of the findings, strategies were implemented throughout the research process in accordance with established qualitative criteria of credibility, dependability, confirmability, and transferability.
Credibility
Credibility was strengthened through prolonged engagement with participants and the use of multiple data collection methods, including in-depth interviews and focus group discussions, to capture both individual and collective perspectives. The interview guide was pretested to ensure clarity and cultural appropriateness, and probing techniques were used during interviews to obtain comprehensive and detailed responses. All interviews were audio-recorded with participants’ consent and transcribed verbatim. Transcripts were cross-checked against original recordings to ensure accuracy. Member checking was conducted by sharing preliminary findings with selected participants to verify that interpretations reflected their lived experiences.
Dependability
Dependability was enhanced through systematic documentation of all methodological decisions, including sampling procedures, data collection processes, and analytical steps. Two researchers independently coded the transcripts, and discrepancies were resolved through discussion and consensus, resulting in a refined and coherent coding framework. An audit trail was maintained to document analytical decisions and theme development.
Confirmability
To promote confirmability, reflexivity was actively practiced throughout the study. The researchers acknowledged potential biases and critically reflected on their roles in shaping data interpretation. Field notes were maintained to capture contextual observations and reflexive insights during data collection and analysis. Independent coding and peer debriefing were employed to ensure that findings remained grounded in participants’ narratives rather than researcher assumptions. The research team comprised clinical pharmacy professionals with training and experience in qualitative research. While this background facilitated an informed understanding of biomedical perspectives on HBV, it may also have influenced the interpretation of culturally grounded beliefs. To mitigate this, ongoing reflexive practices including critical self-reflection, independent coding by multiple researchers, and peer debriefing were consistently applied to minimize the influence of preconceptions.
Transferability
Transferability was supported through detailed descriptions of the study setting, participant characteristics, sampling strategy, and data collection procedures. Providing rich contextual information enables readers to assess the applicability of the findings to similar urban Ethiopian or comparable low-resource settings.
Results
Participant characteristics
A total of 68 adults participated in the study, comprising 20 IDI participants and 48 FGD participants across six groups. Participants represented diverse sociodemographic backgrounds, including variations in age, sex, educational attainment, and occupation. Ages ranged from 18 to 65 years. Employed and unemployed individuals, merchants, government employees, daily laborers, and housewives were included to ensure heterogeneity of perspectives (Table 1).
Sociodemographic characteristics of the study participants (n = 68).

FGD, focus group discussions; IDIs, in-depth interviews.
Thematic areas
Community perspectives on HBV transmission and vaccination
Data analysis generated three major themes and nine subthemes reflecting community perspectives on HBV transmission and vaccination (Table 2). These themes capture participants’ knowledge, attitudes, beliefs, and practices related to HBV, providing insight into barriers and facilitators to prevention and vaccination uptake.
The themes and subthemes developed from the data on community perspectives on HBV transmission and vaccination among adults in Northwest Ethiopia.
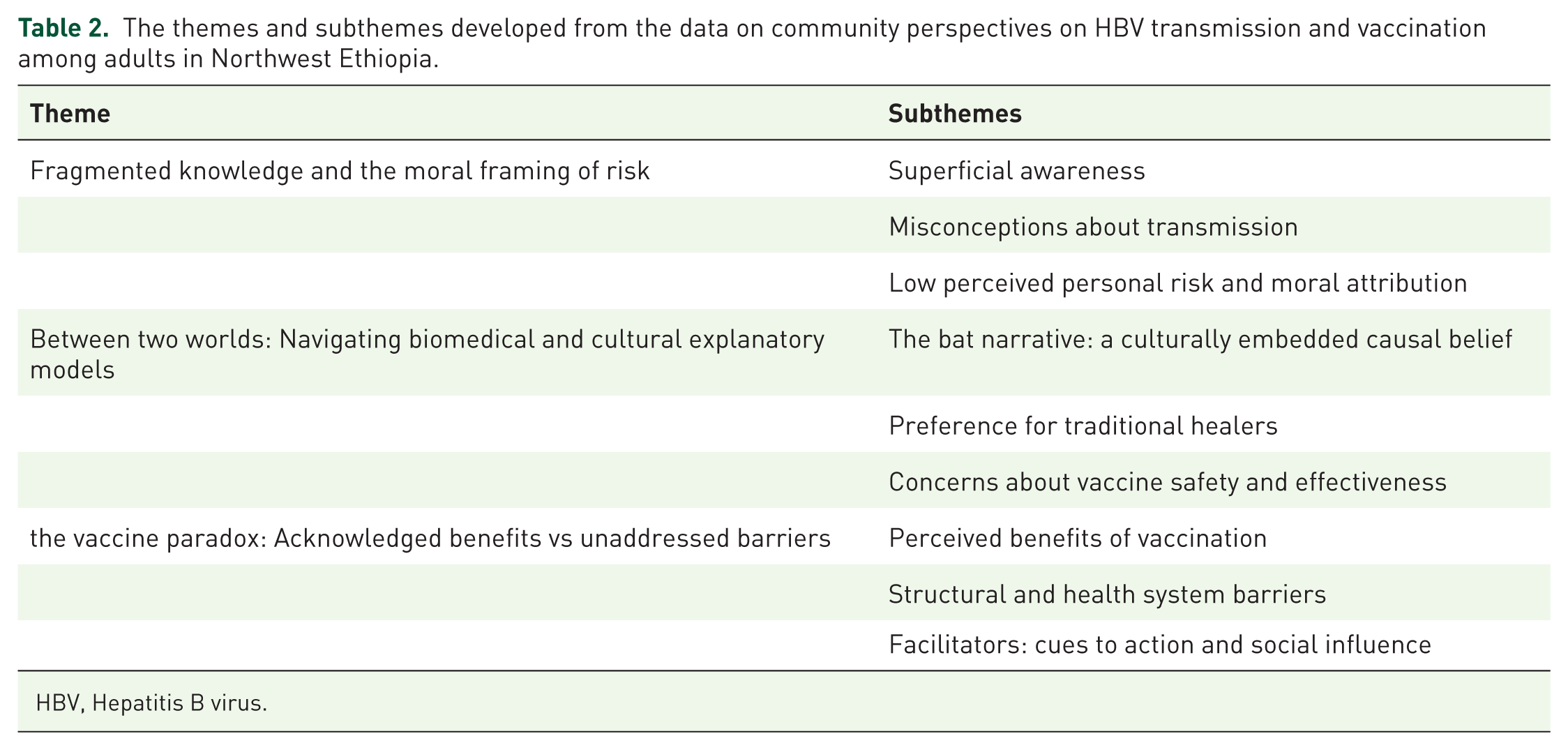
HBV, Hepatitis B virus.
Theme 1: Fragmented knowledge and the moral framing of risk
This theme primarily reflects low perceived susceptibility despite high perceived severity and captures the superficial and often inconsistent awareness participants held about HBV, along with the tendency to associate infection risk with morally questionable behavior. These factors combined to create a widespread perception of low personal vulnerability. Although participants widely recognized hepatitis B as a serious and potentially fatal disease affecting the liver, many did not perceive themselves to be personally at risk. This disconnect was largely driven by moral framing of disease transmission, whereby individuals associated infection with socially undesirable behaviors and consequently excluded themselves from vulnerability. As a result, high perceived severity alone was insufficient to motivate preventive action in the absence of perceived personal risk.
Subtheme 1.1: Superficial awareness
Most participants had heard of hepatitis B, often through media, health campaigns, or acquaintances. However, knowledge was generally superficial and lacked clarity regarding transmission mechanisms, prevention, and disease progression. Participants showed limited ability to differentiate types of hepatitis.
As one participant noted, “I have heard about hepatitis, but I do not clearly know the difference between the types. I just know it affects the liver.” (IDI, P12)
Participants with secondary or higher education demonstrated relatively better awareness of HBV as a viral infection affecting the liver, whereas those with no formal education often described it vaguely as a “liver disease” without distinguishing it from other conditions. Confusion between hepatitis B and HIV was common, particularly among participants with limited formal education. This conflation appeared to contribute to stigma and misinterpretation of risk.
Is it not like HIV? They say it spreads through blood and sex, so it must be the same. (FGD3)
Subtheme 1.2: Misconceptions about transmission
Although several participants correctly identified blood contact and sexual transmission as routes of infection, misconceptions were common. Some believed that HBV could spread through casual contact, shared food, or environmental exposure.
If someone with hepatitis eats with you using the same plate, you can get it. (FGD2)
These misconceptions were more pronounced among older participants and those with lower educational attainment. Fear of casual transmission contributed to social distancing behaviors and potential stigmatization of infected individuals.
Subtheme 1.3: Low perceived personal risk and moral attribution
Many participants did not perceive themselves as personally susceptible to HBV. Risk was frequently associated with what they considered “high-risk behaviors” or socially deviant practices, creating a moral framing that excluded those who viewed themselves as responsible community members.
I do not think I am at risk because I do not share needles or behave badly. I am married and live a good life. (IDI, P17)
Women, particularly housewives, commonly expressed lower perceived susceptibility, citing marital stability and domestic roles as protective factors. This overlooked potential risks, such as unsafe medical procedures, dental visits, or undiagnosed infection in their partners.
I stay home and take care of my children. How could I get such a disease? (FGD5)
Despite low personal risk perception, participants widely acknowledged that HBV could cause severe illness, including liver damage and death. However, this recognition of disease severity and, however, was insufficient to motivate preventive action in the absence of perceived personal vulnerability.
They say it can destroy your liver and you may die if it is not treated. But that is for people who expose themselves. (FGD4)
Theme 2: Between two worlds: Navigating biomedical and cultural explanatory models
This theme highlights how culturally embedded beliefs, particularly the bat-related explanatory narrative, influence perceived benefits of vaccination and introduce competing cues to action. When hepatitis B was understood as resulting from environmental exposure to bats, biomedical prevention strategies such as vaccination were often perceived as irrelevant or ineffective. At the same time, the preference for traditional healers functioned as an alternative cue to action, reinforcing non-biomedical pathways of care and further reducing engagement with vaccination services. Additionally, this theme represents the most striking finding of the study: the co-existence of and tension between biomedical understandings of HBV and deeply embedded cultural beliefs about disease causation. This duality profoundly influenced how participants interpreted prevention, particularly vaccination.
Subtheme 2.1: Bat narrative: Culturally embedded causal belief
A widespread and powerful belief across all participant groups was that hepatitis B is caused by exposure to bats, locally referred to as “wof zura.” This explanatory model was described in concrete terms, often linked to environmental contact with bat droppings or urine. To our knowledge, this bat-related explanatory belief has not been previously documented in Ethiopian HBV research.
Hepatitis comes from bats. If their waste falls on your food or into your water, you will get it. That is what people say, and we have seen it happen. (FGD1) In our area, we know that when bats are around, liver problems increase. The bats bring it. (IDI, P13)
This belief was not merely a peripheral myth but a central framework through which many participants understood the disease. It was transmitted through family and community networks and reinforced by experiential observations, such as the perceived clustering of liver disease in areas with bat populations. When disease causation was attributed to environmental exposure, biomedical prevention strategies like vaccination were often perceived as logically irrelevant. To our knowledge, this specific bat-related explanatory belief has not been previously documented.
If it comes from bats, how can a vaccine stop that? You would need to avoid bats, not go to the clinic. (FGD2)
Origins of the bat narrative
Participants frequently associated the belief that hepatitis B originates from bats to observable environmental experiences within their communities. “Many described the presence of bats in residential areas, particularly in roofs, old buildings, and fruit trees, as well as exposure to bat droppings contaminating food or water.” These recurring observations appeared to reinforce the perception that bats are directly associated with liver-related illnesses. In some accounts, participants connected the presence of bats with a perceived increase in cases of “liver disease” in their surroundings, suggesting that this explanatory model may be grounded in locally observed patterns rather than biomedical understanding. “The belief was commonly transmitted through family and community narratives, indicating its deep-rooted nature within shared social knowledge.”
Function of the bat narrative
Beyond its role as a causal explanation, the bat narrative appeared to serve important social and psychological functions. By attributing hepatitis B infection to environmental exposure rather than individual behavior, the belief externalizes the source of illness and reduces personal responsibility or moral judgment. As one participant explained, “We cannot control where bats live or where their droppings fall, so it is not our fault if someone gets sick” (IDI, P 16). This may help reduce stigma, particularly in a context where disease transmission is often associated with socially sensitive behaviors. However, this interpretation may also diminish the perceived relevance of preventive measures such as vaccination.
Variation in the bat narrative
Although widely shared, the strength and interpretation of the bat-related belief varied among participants. Younger individuals and those with higher levels of education were more likely to express uncertainty about the narrative, sometimes attempting to reconcile it with biomedical explanations of viral transmission. One younger participant stated, “I have heard people say bats cause hepatitis, but I also know the virus spreads through blood and body fluids, so I am not sure bats are the real cause” (IDI, P 6). In contrast, older participants and those with limited formal education tended to endorse the belief more strongly and describe it with greater certainty. This variation suggests that exposure to formal education and health information may influence how individuals interpret and negotiate between cultural and biomedical explanatory models.
Subtheme 2.2: Preference for traditional healing
Participants described traditional healers as trusted providers who offer both treatment and explanations for liver-related illnesses. Their herbal remedies, believed to “clean” or restore the liver, were often curative rather than preventive, emphasizing treatment over early prevention. Healers frequently attributed disease to environmental or spiritual causes, such as bat exposure, aligning with local cultural beliefs. Consequently, vaccination was rarely discussed or was seen as unnecessary, suggesting that traditional healing practices may indirectly compete with biomedical prevention by prioritizing cure and offering alternative causal explanations. Closely linked to the bat narrative was a strong preference for seeking care from traditional healers, particularly for symptoms perceived as liver-related. Traditional healers were described as accessible, culturally trusted, and knowledgeable about locally recognized illnesses.
If someone has a liver problem, we first go to the traditional healer. They have medicines from plants that work. The hospital is for other things. (IDI, P4)
This preference reflected a broader orientation toward treatment after symptom recognition rather than prevention before exposure. Participants described consulting healers for abdominal pain, yellow eyes, or other symptoms associated with liver disease, often delaying or foregoing biomedical care entirely. The influence of traditional healers was particularly strong among older participants and those with limited formal education.
The preference for traditional healers was not merely a fallback option but often described as a first-line choice for culturally recognized symptoms. Participants’ frequently framed traditional medicine as more effective for conditions perceived to have spiritual or environmental origins such as the “bat narrative.” As one participant noted: The doctors give you injections and tell you to take tablets for months. The traditional healer gives you one herbal remedy, and it cleans your liver completely. That is what our grandparents used. (IDI, P 9)
This suggests that traditional healers are perceived to offer a holistic and curative approach that aligns with local explanatory models, whereas biomedicine is sometimes viewed as palliative or symptom-focused.
Participants described traditional healers as “possessing specialized knowledge passed down through generations, which inspired greater trust than the impersonal care sometimes perceived in public health facilities.”
Subtheme 2.3: Concerns about vaccine safety and effectiveness
Even among participants who did not fully subscribe to the bat narrative, uncertainty and misinformation about vaccine safety were common. Rumors circulated through informal social networks, amplifying fears of side effects or long-term harm.
I heard vaccines can cause other problems in the body. Some people say they can make you sick instead of protecting you. (FGD6)
Lack of clear, consistent messaging from trusted health authorities exacerbated this uncertainty. When biomedical explanations conflicted with cultural causal models, participants often resolved the tension by questioning the vaccine’s relevance or safety.
The doctors say it is a virus, but we have our own understanding. If we are not sure what causes it, how can we be sure the vaccine works? (IDI, P19).
Theme 3: Vaccine paradox: Acknowledged benefits versus unaddressed barriers
This theme reflects the dynamic interplay between perceived benefits and perceived barriers. While participants generally recognized the protective value of vaccination, multiple structural and informational barriers, including limited awareness of adult vaccination, cost concerns, uncertainty about service availability, and fears about vaccine safety, hindered uptake. Within this context, cues to action, particularly healthcare provider recommendations and community-based health education, emerged as critical triggers that could shift intentions toward vaccination. Taken together, these findings illustrate that HBV vaccination behavior is shaped not by a single factor but by the interaction of low perceived susceptibility, culturally rooted interpretations of disease causation that weaken perceived benefits, substantial perceived barriers, and the presence or absence of effective cues to action. This integrated HBM perspective provides a comprehensive understanding of the behavioral dynamics underlying vaccine uptake in this setting. Despite the cultural and informational barriers described above, participants were not uniformly opposed to vaccination. This theme explores the paradox whereby the benefits of vaccination were often acknowledged, yet multiple unaddressed barriers prevented uptake.
Subtheme 3.1: Perceived benefits of vaccination
When participants understood the preventive purpose of the HBV vaccine, they generally viewed it positively. Prior positive experiences with childhood immunization programs appeared to build trust in vaccines more broadly.
If there is a vaccine that can prevent such a dangerous disease, it is good to take it. We take our children for vaccinations, so why not adults? (IDI, P8)
Some participants articulated the concept of collective protection, expressing a desire to protect their families. Education level appeared to influence acceptance, with participants who had higher education more likely to describe vaccination as a reasonable, scientific preventive measure.
Vaccination is like building a wall. It protects you so that the disease cannot enter. If we all build the wall, the community is safe. (FGD3)
Subtheme 3.2: Structural and health system barriers
Despite positive attitudes toward vaccination in principle, multiple barriers prevented participants from seeking or receiving the HBV vaccine. Limited awareness of adult vaccination was a primary barrier. Unlike childhood immunization, which was widely recognized and promoted, adult vaccination services were perceived as invisible.
I have heard about hepatitis, but I did not know that adults can take a vaccine for it. They only talk about vaccines for children. (IDI, P15)
Uncertainty about where and how to access the vaccine was nearly universal. Participants did not know whether the vaccine was available at public health facilities, whether it required payment, or how many doses were needed.
Even if I wanted to take it, I would not know where to go. Is it at the hospital? The health center? Do I need to pay? (IDI, P10)
Cost concerns were frequently mentioned, particularly by unemployed participants and daily laborers. The assumption that the vaccine would be expensive discourages proactive inquiry.
I think it must be expensive. Everything in the hospital costs money now. If I am not sick, why would I spend money on a vaccine? (IDI, P14)
Health system reliability also influenced perceptions. Participants noted medication stock-outs and inconsistent service quality as reasons for skepticism about the stability and sustainability of vaccination programs.
Sometimes you go to the clinic and they say there is no medicine. People lose trust in the system. If they cannot keep regular medicines, how can we trust that they will have the vaccine when we need it? (FGD5)
Subtheme 3.3: Facilitators: Cues to action and social influence
Despite the barriers, participants identified clear factors that would facilitate vaccine acceptance, providing actionable insights for intervention design.
Healthcare provider recommendation emerged as the most powerful potential cue to action. Participants consistently stated that they would accept vaccination if directly advised by a trusted clinician.
If a doctor tells me to take it, I will take it. They know what is best for our health. (IDI, P19) When we go to the clinic for other things, if the nurse or doctor said, “You should also get the hepatitis vaccine,” we would do it. (IDI, P 20)
Health education and community awareness campaigns were also emphasized. Participants expressed a desire for clear, accessible information delivered by trained health professionals rather than through informal channels.
If health workers come to our community and teach us clearly how it spreads and how vaccination helps, more people will accept it. We need to understand. (FGD4)
Social influence and family decision-making played a significant role. Adult participants, particularly men, described their authority in household health decisions, while women highlighted collaborative discussion processes. This suggests that improving adult awareness could have ripple effects on family-level vaccination uptake.
In our home, I decide about health matters. If I understand it, I will tell my wife and children to take it. (IDI, P10) We discuss together as a family. If we all understand, we will go together. (FGD6)
Discussion
This qualitative study explored adult community perspectives on HBV transmission and vaccination in Northwest Ethiopia. The findings reveal a complex interplay of limited biomedical awareness, culturally embedded explanatory beliefs, structural barriers, and trust dynamics that collectively shape vaccination attitudes and preventive behaviors. While participants widely acknowledged the severity of HBV, misconceptions regarding its causes, particularly attribution to bat exposure and preference for traditional healing practices, emerged as central determinants of vaccine hesitancy.
Cultural explanatory beliefs and competing health paradigms
One of the most striking findings was the widespread belief that HBV is caused by bats (called locally “wof zura”). This culturally grounded explanatory model overshadowed biomedical understandings of viral transmission through blood and body fluids. 22 Participants described bat exposure as the primary cause of infection, reflecting a locally constructed narrative that appears deeply embedded within community discourse. Such beliefs align with anthropological perspectives on illness representation, where communities develop culturally coherent explanations for disease causation based on environmental, social, and experiential knowledge. 23 In this context, HBV was conceptualized as an environmentally acquired condition rather than a viral infection transmitted through specific behavioral or medical risk factors. This interpretation directly influenced prevention behaviors. When disease causation is attributed to environmental exposure, biomedical prevention strategies, such as vaccination, may be employed, perceived as irrelevant or ineffective. 24
Traditional healers and hepatitis B
Traditional healers strongly shape community perceptions and behaviors regarding hepatitis B. 25 Trusted for their curative herbal remedies, often said to “clean” or restore the liver, they frequently attribute disease to environmental or spiritual causes, such as bat exposure. 26 This reinforces a treatment- focused approach and can reduce the perceived need for vaccination. 27 While medical pluralism allows traditional and biomedical systems to coexist, healer explanations may compete with biomedical prevention, leading individuals to prioritize cure over prevention. 28 Many participants expressed a preference for seeking traditional healers after disease onset rather than engaging in preventive vaccination. This reflects a pattern of medical pluralism, in which traditional and biomedical systems coexist but are differentially utilized depending on perceived disease origin and treatment expectations. 18 Traditional healers were described as accessible, culturally trusted, and experienced in managing liver-related illnesses. 29 The communities orientation toward treatment after symptom recognition, rather than prevention before exposure, substantially reduced perceived urgency for hepatitis B vaccination. 30 However, traditional healers’ social influence offers an opportunity for public health engagement. Culturally sensitive collaboration, including education on hepatitis B transmission and prevention, can align local beliefs with biomedical knowledge. Involving trusted community figures healers, religious leaders, and healthcare providers can strengthen health communication, improve vaccine acceptance, and promote sustainable preventive behaviors.
Interpretation through the HBM
The findings can be meaningfully interpreted using the HBM. Although participants recognized HBV as a severe disease, perceived susceptibility was generally low. Risk was often associated with “immoral behavior” or socially stigmatized practices, leading many individuals to exclude themselves from perceived vulnerability. This moral framing of risk contributed to a false sense of protection, particularly among participants who considered themselves socially responsible. 18 Perceived severity, however, was consistently high. Participants frequently described HBV as life-threatening and capable of causing liver damage or death. In HBM terms, high-perceived severity alone was insufficient to motivate preventive action in the absence of perceived susceptibility and clear cues to action. 20 Perceived benefits of vaccination were acknowledged when participants understood its preventive function. 31 However, misinformation and uncertainty weakened confidence in vaccine effectiveness, particularly when biomedical explanations conflicted with cultural causal models. 31 This finding is supported by a participant’s statement (Lines 441–451), which illustrates how conflicting biomedical and cultural beliefs can undermine confidence in perceived benefits.” Perceived barriers included limited awareness of adult vaccination availability, cost concerns, health system reliability, and fear of side effects. Healthcare provider recommendation emerged as a strong cue to action. Participants repeatedly indicated that they would accept vaccination if directly advised by a trusted clinician. This highlights the importance of interpersonal trust and authoritative guidance in shaping preventive behavior. 30 Overall, the interaction of low perceived susceptibility, culturally framed causation beliefs, and structural access barriers appears to significantly constrain vaccine uptake intentions in this setting. 30
Implications for public health practice
The findings have important implications for HBV prevention strategies in similar low-resource settings. First, Educational interventions should respectfully engage with bat-related explanatory beliefs rather than dismiss them. For example, such beliefs can be used as a bridge in communication: “We know that bats are part of our environment and are often linked to illness in local understanding. Similarly, hepatitis B is an invisible infection that can affect health, but unlike many perceived threats, it can be prevented through a safe and effective vaccine.” This approach helps align local beliefs with biomedical explanations and may enhance acceptance of preventive measures. 22 Second, vaccination promotion strategies should explicitly emphasize adult susceptibility and clarify that HBV infection can occur through routine medical procedures, household exposure, and asymptomatic transmission. Increasing perceived susceptibility in a non-stigmatizing manner is critical for behavior change. 32 Third, healthcare providers represent a pivotal intervention point. Strengthening provider-initiated counseling and integrating HBV vaccination discussions into routine clinical encounters could serve as powerful cues to action. Fourth, collaboration with trusted community figures, including religious leaders and, where appropriate, traditional healers, may enhance credibility and improve vaccine acceptance. Engaging traditional healers and other community influencers in co-designed educational initiatives may enhance the acceptability of HBV prevention strategies and help reconcile biomedical approaches with existing cultural frameworks. 18 However, such engagement should be undertaken where ethically appropriate and with careful attention to the accuracy and consistency of the messages being conveyed. 18 Finally, improving the visibility and accessibility of adult vaccination services is essential. Clear information regarding vaccine availability, cost, and schedule should be widely disseminated to reduce structural uncertainty.
Strengths and limitations
This study provides in-depth qualitative insights into adult community perceptions of HBV transmission and vaccination in Northwest Ethiopia, a setting where limited qualitative evidence exists. The use of both in-depth interviews and focus group discussions enabled exploration of both individual experiences and shared community norms. Methodological rigor was strengthened through independent coding, member checking, reflexivity, and adherence to established qualitative reporting standards. However, some limitations should be acknowledged. The study was conducted in an urban setting, which may limit transferability to rural communities where cultural beliefs and access barriers may differ. Recruitment via community leaders and health extension workers may have introduced selection bias toward more health-engaged individuals, although their community integration supported diverse participation. Marginalized groups may still be underrepresented. Social desirability bias may have influenced responses, particularly regarding vaccination attitudes.
Conclusion
This study demonstrates that HBV vaccination decisions among adults in Northwest Ethiopia are shaped not only by knowledge gaps but also by culturally embedded beliefs and competing health paradigms. While perceived disease severity is high, low perceived susceptibility, attribution of disease causation to bats, and reliance on traditional healing practices substantially influence preventive behavior. Participants also identified structural and health system barriers, including limited awareness of adult vaccination, uncertainty about vaccine availability, cost concerns, and inconsistent service delivery. Although the study did not evaluate interventions or directly assess policy-level determinants, these findings suggest that future efforts aiming to improve HBV vaccine uptake may benefit from culturally sensitive approaches that engage with local belief systems alongside biomedical information. Implementation research is needed to explore the effectiveness of such strategies and to examine broader health system and policy-level factors affecting adult immunization in similar low-resource settings.
Supplemental Material
sj-docx-1-tai-10.1177_20499361261451362 – Supplemental material for Community perspectives on hepatitis B transmission and vaccination among adults in Northwest Ethiopia: a qualitative study
Supplemental material, sj-docx-1-tai-10.1177_20499361261451362 for Community perspectives on hepatitis B transmission and vaccination among adults in Northwest Ethiopia: a qualitative study by Desalegn Addis Mussie, Tigabu Eskeziya Zerihun, Samuel Berihun Dagnew, Abel Temeche Kassaw, Woretaw Sisay Zewdu, Tilaye Arega Moges, Fasil Bayafers Tamene, Samuel Agegnew Wondm, Getachew Yitayew Tarekegn and Teferi Bihonegn Melese in Therapeutic Advances in Infectious Disease
Footnotes
Acknowledgements
We would like to sincerely thank Debre Tabor University, College of Medicine and Health Sciences, Department of Clinical Pharmacy, for the support and opportunity to conduct this study. Our gratitude also goes to the Debre Tabor city community for their collaboration during data collection. We deeply appreciate the participants who participated in the qualitative interviews, as well as the data collectors and supervisors who contributed to the successful completion of the study.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.