
Abstract
Background
Spinal anesthesia is a widely preferred anesthetic technique for cesarean section but often leads to adverse effects such as nausea, vomiting, hypotension, bradycardia, and shivering, which are primarily attributed to increased intra-abdominal pressure. Since abdominal circumference correlates with intra-abdominal pressure in parturients, the objective is to investigate how abdominal circumference influences the spread of intrathecal heavy bupivacaine following spinal anesthesia during cesarean section.
Methodology
A total of 78 pregnant women with singleton gestation undergoing cesarean section under spinal anesthesia were enrolled in the study. Preoperative parturient abdominal circumference was measured. Lumbar puncture was performed at the L3-L4 interspinous space using a Quincke 25-gauge spinal needle with a midline approach in the sitting position, followed by the intrathecal administration of 2 mL of 0.5% heavy bupivacaine. The cephalic spread of local anesthetic was assessed by evaluating the dermatomal level of cold-sensation loss at 1, 3, 5, 10, and 15 minutes following spinal anesthesia. Kendall’s tau correlation analysis was used to assess the relationship between parturient abdominal circumference and the sensory block level at various time intervals.
Results
No correlation was found between parturient abdominal circumference and the level of loss of cold sensation at various time intervals. The incidence rates of adverse effects were as follows: hypotension (44.4%), bradycardia (4.2%), nausea (4.2%), vomiting (2.8%), and shivering (18.1%).
Conclusion
Our study found no correlation between parturient abdominal circumference and the intrathecal spread of heavy bupivacaine following spinal anesthesia during cesarean section.
Introduction
Spinal anesthesia (SA) is the preferred anesthetic technique for cesarean section (CS) among most anesthesiologists. A sensory block extending up to the fourth thoracic dermatomal level is recommended for CS to ensure adequate surgical anesthesia. 1 SA in parturients undergoing CS has been frequently associated with adverse effects such as nausea, vomiting, hypotension, bradycardia, and shivering. 2 These complications are primarily attributed to increased intra-abdominal pressure (IAP), which may contribute to aortocaval compression and an enhanced cephalic spread of local anesthetic (LA) during SA in parturients.3–5 The hypothesized mechanism for the increased cephalic spread of LA may be attributed to a reduction in cerebrospinal fluid (CSF) volume and dural sac capacity, potentially caused by either engorgement of the extradural venous plexus or inward displacement of soft tissue within the intervertebral foramina.3–5 Additionally, abdominal circumference (AC) in parturients can be correlated with IAP, which is influenced by factors such as fetal size, amniotic fluid volume, and uterine dimensions.6,7 Parturient AC may serve as a simple and convenient bedside measurement tool for assessing the compressive effects of increased intra-abdominal volume, particularly in resource-limited regions of Nepal. Several studies have reported that a larger AC is associated with higher sensory block levels during cesarean section. However, these findings have been inconsistent, and most prior studies were conducted exclusively in elective cases, used varying doses of local anesthetic, performed spinal anesthesia in the lateral position, or assessed block height using pinprick testing.8–11 Such methodological differences limit the generalizability of existing evidence, particularly in real-world obstetric settings where emergency CS predominates, and spinal anesthesia is commonly performed in the sitting position. Therefore, the objective of this study is to evaluate the effect of parturient AC on the spread of intrathecal heavy bupivacaine following SA during CS in real-world obstetric practice.
Methodology
Following approval from the Nepal Health Research Council (Reference No.: 338) and Sindhuli Hospital (Reference No.: 610), a prospective, observational study was conducted from September 2024 to March 2025. The study enrolled 78 pregnant women with singleton gestation undergoing CS under SA. Exclusion criteria included CS performed under general anesthesia, failed SA, a history of spinal deformities or surgeries, gestational disorders such as pre-eclampsia and diabetes, and any contraindications to neuraxial anesthesia. Preoperatively, a relevant patient assessment was conducted, followed by obtaining written informed consent from each participant after a detailed explanation of the study’s nature and the technique used to measure sensory block levels. Intravenous (IV) administration of 500 mL Ringer’s Lactate was initiated through an 18-G IV catheter. Premedication was administered gradually, consisting of metoclopramide (10 mg IV), ranitidine (50 mg IV), and ceftriaxone (1 g IV). The second co-author, who was experienced in maternity care and specifically trained in the standardized technique for AC measurement, measured each parturient’s AC at the level of the umbilicus at the end of expiration in the supine position using a standardized measuring tape. The recorded measurement was not shown to the anesthesiologist performing the SA. Subsequently, the patient was transferred to the operating theatre, where all necessary monitors were attached, and baseline heart rate (HR) and blood pressure (BP) were recorded. Lumbar puncture was performed at the L3-L4 interspinous space using a Quincke 25-gauge spinal needle with a midline approach in the sitting position. Following the confirmation of free CSF flow, 2 mL of 0.5% heavy bupivacaine was administered intrathecally without adjuncts, consistent with the standard practice for the majority of CS in our setting. The patient was then placed in the supine position with left uterine displacement. Immediately after the intrathecal administration of 0.5% heavy bupivacaine, the timer was started and recorded by the second co-author. The anesthesiologist then assessed the cephalic spread of the LA by evaluating the loss of cold sensation using an ice cube. The parturient was instructed to compare the cold stimulus to the forehead as a reference point. The stimulus was progressively advanced cephalad along the midclavicular line on both sides until the perception of cold sensation equaled that of the forehead. The dermatomal level inferior to this point was recorded as the level of sensory blockade. 10 The dermatomal level of cold-sensation loss was assessed at 1, 3, 5, 10, and 15 minutes following SA. Surgery commenced only after loss of cold sensation was achieved bilaterally up to the T4 dermatomal level. 1 Subsequent intraoperative and postoperative procedures proceeded as planned. The same anesthesiologist performed all SA and assessed the loss of cold sensation in each parturient. Failed SA was defined as the inability to achieve loss of cold sensation to the T4 dermatomal level within 15 minutes, necessitating repeated SA or administration of general anesthesia.12,13 Adverse effects related to SA were managed according to hospital protocol. Hypotension was defined as a systolic blood pressure (SBP) of less than 90 mmHg or a reduction of more than 30% from baseline. 14 Bradycardia was defined as a heart rate (HR) below 60 bpm. Any adverse effects, including hypotension, bradycardia, nausea, vomiting, and shivering, occurring within the study period were documented. The primary outcome was to assess the correlation between parturient AC and the level of sensory block at various time intervals. The secondary outcome was to assess the association between parturient AC and the incidence of hypotension, bradycardia, nausea, vomiting, and shivering.
Statistical analysis
Considering a two-tailed alpha level of 5%, a power of 80%, and an expected correlation coefficient of 0.5, the sample size was calculated based on the study by C.-H. Kuok et al., 10 resulting in an estimated 69 participants. Accounting for a 10% dropout rate, the final sample size was determined to be 78 participants. Quantitative variables were estimated and presented as mean ± standard deviation (SD) or median (interquartile range). Data normality was assessed using the Shapiro-Wilk test. Statistical analysis was conducted using the independent t-test or the non-parametric test, like the Mann-Whitney U test, as appropriate. Categorical variables were presented as proportions (%) and analyzed using Fisher’s exact test or the Chi-square test as appropriate. The correlation between parturient AC and the spread of SA was analyzed using Kendall’s tau-b correlation analysis. Statistical significance was established at a p-value of < 0.05. Data management and statistical analysis were performed using the Statistical Package for the Social Sciences.
Study flow chart

Results
Demographic variables.

Quantitative data as mean ± SD for normally distributed and median (interquartile range) for non-normally distributed; n (%) for categorical data. DBP: Diastolic Blood Pressure; BMI: Body Mass Index.
Level of sensory loss at 1, 3, 5, 10, and 15 minutes after SA.

Correlation between AC and right-sided level of sensory loss at different time intervals.

*Kendall’s tau-b correlation analysis (τ-b: correlation coefficient); CI: Confidence Interval.
Correlation between AC and left-sided level of sensory loss at different time intervals.

*Kendall’s tau-b correlation analysis (τ-b: correlation coefficient); CI: Confidence Interval.

Relationship between parturient AC and level of loss of cold sensation at 5 minutes after SA (all cases).
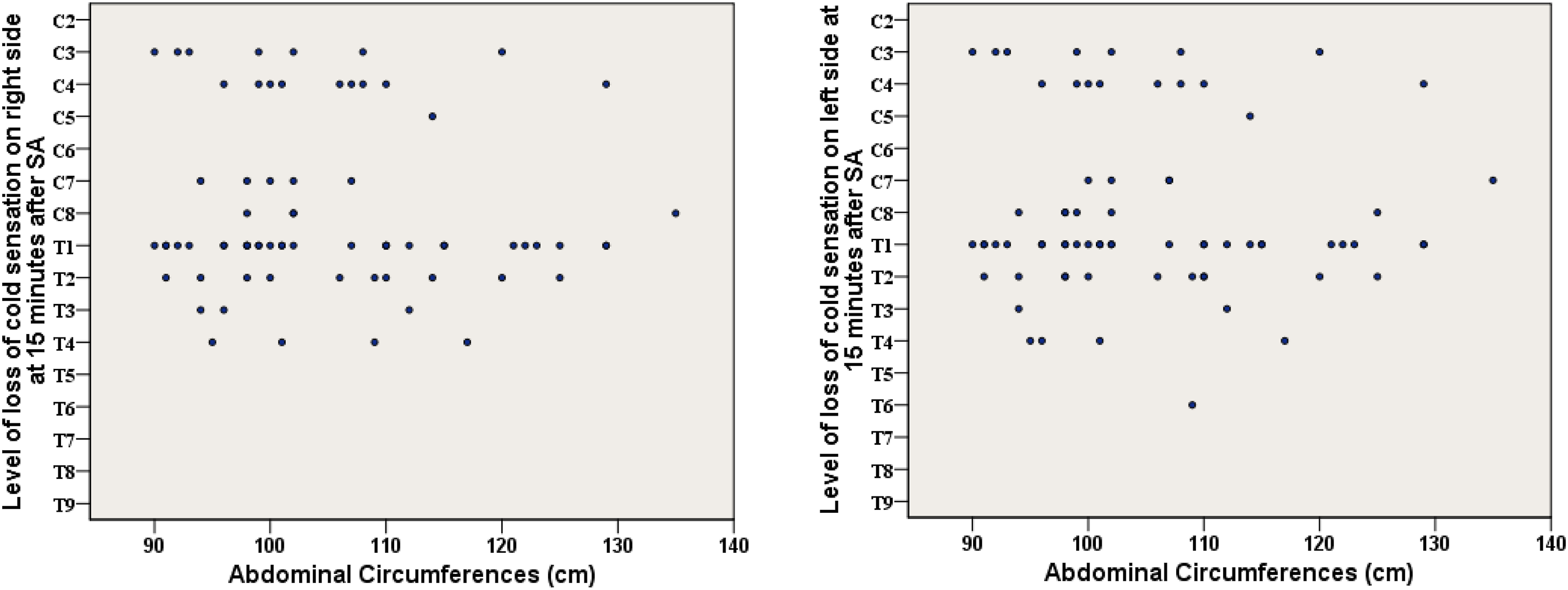
Relationship between parturient AC and level of loss of cold sensation at 15 minutes after SA (all cases).
Relationship between Parturient AC and the incidence of adverse effects.
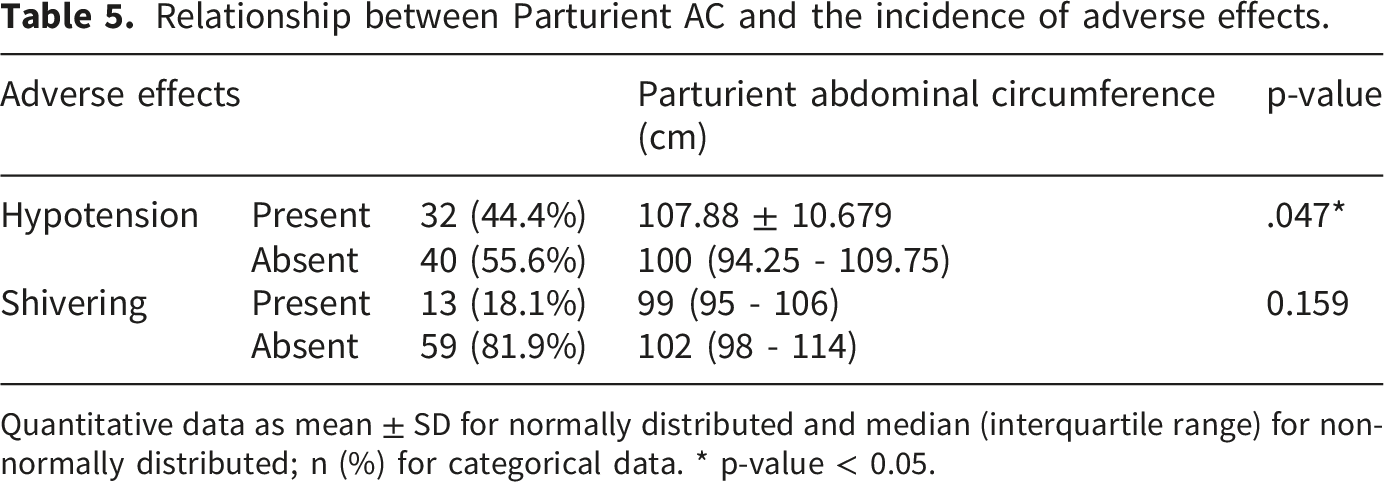
Quantitative data as mean ± SD for normally distributed and median (interquartile range) for non-normally distributed; n (%) for categorical data. * p-value < 0.05.
Multivariable binary logistic regression for predictors of hypotension.

*p-value < 0.05; OR: Odds Ratio; CI: Confidence Interval.
Discussion
The enhanced spinal block in parturients is believed to result from a relative decrease in CSF volume and dural sac capacity. 3 The probable mechanism involves increased IAP caused by an enlarged uterus, which may lead to dural sac compression through either engorgement of the extradural venous plexus or the inward displacement of soft tissue in the intervertebral foramina.3–5 Notably, the engorgement of the extradural venous plexus is positional, being more pronounced in the supine position compared to the left lateral position.4,15
A significant and strong positive correlation has been observed between IAP and abdominal girth in both pregnant and non-pregnant individuals.6,7 Therefore, parturient AC was utilized as a simple and convenient bedside measurement tool to assess its influence on the spread of intrathecal heavy bupivacaine following SA. Unlike studies that assess maximum sensory block height or the time required to reach maximum block height, we used fixed time-point measurements at 1, 3, 5, 10, and 15 minutes after SA. This approach allowed us to observe the effect of AC on the early, natural pattern of sensory block spread, a method also supported by prior studies.8,10 Additionally, waiting for each patient to reach maximum block height before incision was not feasible, especially in emergency CS, because the time required to reach maximum block height could potentially exceed our 15-minute observation period.
Contrary to popular belief, parturient AC in our study showed no correlation with sensory block level after intrathecal heavy bupivacaine. As emergency CS made up most of our cases, we further performed subgroup analyses to rule out any masking effect of case type. In all analyses: overall, emergency only, and routine only, AC remained unrelated to the level of loss of cold-sensation at any measured time point.
In contrast, several studies have reported a significant, albeit weak, positive correlation between parturient AC and sensory block level after SA.8–11,16 Unlike our study, previous studies were conducted exclusively in elective CS and involved comparatively older parturients (25 to 38 years). Most of them administered SA in the lateral position and used the pinprick method for sensory block assessment. In contrast, our study included 79.2% emergency cases, with a younger population (mean age 26.44 ± 5.09 years) and an average AC of 102 cm. We performed SA in the sitting position and assessed sensory block using loss of cold sensation. Patient positioning remains a crucial factor influencing the intrathecal spread of LA. 1 Studies have demonstrated that pinprick testing provides a more accurate assessment of sensory loss and usually registers a level approximately two dermatomes below that detected with cold-sensation testing.17,18 Additionally, earlier studies used a 10 to 15 degree operating table or patient tilt for left uterine displacement, whereas we used manual displacement. Although surgical incision was allowed only after achieving bilateral cold-sensation loss to T4, the emergency nature of most cases meant that draping and preparation often began before complete sensory loss was reached, with patients remaining supine. However, evidence from full-term singleton pregnancies suggests no significant difference in inferior vena cava compression between a 10 to 15 degree tilt and the supine position. 15 These methodological differences may partly explain the differing results observed in our study.
Similar to our findings, Seyhan et al. performed SA in the sitting position and assessed sensory block using loss of cold sensation. 19 Their study also found no significant association between maximum sensory block height and pre-incisional intra-abdominal pressure. However, their study consisted exclusively of elective cases and involved comparatively older parturients, with a mean age of 31.1 ± 4.8 years. Another study by Parthasarathy et al. also reported no significant correlation between maximum sensory block level and AC in a population similar in age to ours. 20 However, they administered SA in the lateral position, were conducted in elective CS, and did not clearly specify the method used to assess sensory block height.
Various adverse effects, such as hypotension, bradycardia, shivering, nausea, and vomiting, are commonly associated with the rapid cephalad spread of intrathecal LA during SA in CS.
2
Studies have reported varying incidence rates of hypotension, ranging from 34% to 85%.8–11 Hypotension (44.4%) and shivering (18.1%) were the most commonly observed adverse effects in our study. Since parturients with hypotension had significantly larger AC, but AC did not differ in those with or without shivering, we performed multivariable binary logistic regression to explore predictors of hypotension. Variables entered into the model were BMI, AC, emergency versus routine CS, baseline SBP, and baseline HR. Because all parturients in our study were term pregnancies between 20 and 30 years of age, age and gestational age were unlikely to contribute meaningful variation in hemodynamic responses to SA and were therefore not included. The regression analysis showed that higher BMI was independently associated with increased odds of hypotension after SA. In contrast, the literature reports mixed findings regarding the role of AC. Thomard et al
Despite these findings, our study has several important limitations. First, the same dose of LA was administered to all parturients, despite potential differences in individual characteristics such as age, height, weight, and race, which may influence intrathecal drug spread. Second, AC was used as a surrogate marker for IAP; however, we were unable to directly measure IAP, which may have provided a more accurate assessment. Third, there is a possibility of measurement bias. 1) Lack of objective assessment tools: Unable to employ more objective modalities, such as sensory evoked potentials, for assessing sensory block. 2) Single-observer measurements: a single investigator measured AC, and the same anesthesiologist performed all SA and assessed loss of cold sensation, without formal inter- or intra-observer reliability testing. 3) Subjective patient responses: Patient responses themselves may also have been subjective, delayed, or variable. Fourth, a large proportion of our sample consisted of emergency CS. Although we did not observe a significant difference in block spread between emergency and elective cases, separate adequately powered studies could better evaluate this distinction. Finally, this was a single-center study with a relatively small sample size, which may limit generalizability. Larger, multicenter studies are warranted to validate and extend these findings.
Conclusion
Although parturient AC was initially presumed to influence the spread of intrathecal LA. Our study found no correlation between AC and the intrathecal spread of heavy bupivacaine during CS in remote-area Nepali parturients. Larger studies involving more diverse populations, including balanced representation of emergency CS, are required to reach a definitive conclusion.
Footnotes
Ethical considerations
Approval from the Nepal Health Research Council (Reference No.: 338) and Sindhuli Hospital (Reference No.: 610). Written informed consent from each participant was obtained after a detailed explanation of the study’s nature and the technique.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
![]() .
22
.
22