
Abstract
Purpose
To systematically evaluate the impact of the COVID-19 pandemic, particularly lockdown (LD) periods, on the incidence, clinical presentations, surgical management, and outcomes of rhegmatogenous retinal detachment (RRD).
Methods
A systematic literature search was conducted in PubMed, Embase, and Web of Science up to June 2025. Observational studies comparing RRD patients during COVID-19 LDs or pandemic periods with pre-pandemic controls were included. Outcomes assessed included RRD incidence, baseline clinical characteristics, intervals from symptom onset to first visit and surgery, surgical interventions, and anatomical and visual outcomes. Meta-analyses were performed for comparable outcomes using random- or fixed-effects models based on heterogeneity.
Results
Twenty-nine observational studies involving more than 116,000 eyes were included. COVID-19–related restrictions were associated with a significant reduction in RRD surgical volume (rate ratio 0.71; 95% CI: 0.60–0.84), although marked regional heterogeneity was observed. Marked heterogeneity across studies appeared to be partly related to differences in LD severity, duration, and regional healthcare system burden. Patients presenting during LD periods were significantly less likely to have macula-on RRD (OR = 0.61; 95% CI: 0.46–0.83) and more likely to exhibit moderate-to-severe proliferative vitreoretinopathy (PVR) (OR = 2.58; 95% CI: 1.37–4.87) compared with pre-LD periods. Time from symptom onset to surgery increased during LD periods, while presentation-to-surgery intervals decreased. Surgical practice shifted toward greater use of pars plana vitrectomy (PPV), often combined with longer-acting gas tamponades or silicone oil. Despite increased disease severity, single-surgery retinal attachment rates and postoperative visual outcomes remained largely unchanged across periods.
Conclusions
The COVID-19 pandemic had substantial and region-specific effects on RRD management, influencing patient presentation patterns, disease severity, and surgical strategies. Nevertheless, adaptive healthcare responses helped preserve overall anatomical and visual outcomes.
Keywords
Introduction
The COVID-19 pandemic, declared by the World Health Organization (WHO) in March 2020, significantly disrupted healthcare delivery worldwide, notably affecting ophthalmology services.1,2 Rhegmatogenous retinal detachment (RRD) constitutes a vision-threatening emergency requiring timely diagnosis and surgical intervention to prevent permanent vision loss. 3 The pandemic-induced lockdowns (LDs) resulted in marked reductions in healthcare access, elective surgeries, and patient encounters, altering patient behaviors and delaying urgent medical care. 4
Emerging data suggest heterogeneous impacts of the COVID-19 LDs on RRD incidence, clinical presentation, and management practices. While several studies across Europe and North America reported considerable declines in RRD cases and surgical interventions during peak LD periods (such as reductions of 41.6% in France 5 and 46% in the United Kingdom 6 ), other regions, including Canada, 7 Pakistan, 8 and Iran 9 documented stable or increased caseloads possibly due to altered referral pathways or continuous operation of specialized centers. In Switzerland, emergency pars plana vitrectomy (PPV) for RRD dropped to a minimum during the first LD, but increased later in 2020, compensating for the initial decline. 10
Additionally, many patients presented with more advanced stages of RRD during the pandemic, exhibiting a higher proportion of macula-off detachments, prolonged symptom duration, increased incidence of proliferative vitreoretinopathy (PVR), and poorer visual acuity at presentation.7,11–13 Factors contributing to delayed presentations included fear of virus exposure, transportation difficulties, and restricted access to primary eye care.4,12,14–16 Surgical management also shifted during this period, favoring procedures such as PPV with silicone oil or longer-acting gas tamponades to manage complex cases and reduce re-intervention risks.15,17–19 Despite these alterations, the majority of studies reported final anatomical and visual outcomes comparable to pre-pandemic standards.7,9,15,20
Given the variability and occasional contradictions observed across different studies, this systematic review aims to comprehensively evaluate and meta-analyze evidence regarding the impact of COVID-19 LDs on RRD incidence, clinical characteristics, management strategies, and surgical outcomes. Clarifying these impacts will provide insights for developing resilient care pathways and inform preparedness strategies for managing retinal emergencies during future public health crises.
Methods
Design
This systematic review and meta-analysis were conducted following the Joanna Briggs Institute (JBI) guidelines for evidence synthesis and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement.21,22 To enhance methodological transparency and reproducibility, the protocol was prospectively registered with the PROSPERO database (registration number CRD420251061961).
Search strategy
A comprehensive literature search was conducted in June 2025 across the following databases: PubMed, Embase, and Web of Science. Keywords included “rhegmatogenous retinal detachment,” “retinal detachment,” “COVID-19,” “SARS-CoV-2,” and “lockdown,” alongside relevant synonyms and medical subject headings. In this review, the term “LD” was operationally defined as any period of government- or institution-mandated restrictions associated with the COVID-19 pandemic that resulted in reduced mobility, suspension of elective medical services, or limited access to ophthalmic care. Additionally, reference lists of included articles were manually reviewed, citations of relevant articles were screened (snowballing), and related articles were identified using PubMed’s “related articles” function. A monthly PubMed alert was established to capture ongoing publications. The detailed search strategies for each database are available in Supplemental Materials, Table S1-3.
Eligibility criteria
Studies were eligible if they involved patients who underwent emergency surgery for RRD during COVID-19 LD periods. Included studies were required to compare these LD periods either inter-year (identical calendar days in pre-pandemic years) or intra-year (intervals immediately before or after LD within the same year). Eligible outcomes were RRD incidence or surgical volume, baseline clinical characteristics (macula status, detached quadrants, baseline visual acuity, PVR grade), intervals from symptom onset to first visit or surgery, and treatment outcomes (post-operative visual acuity and single-surgery retinal attachment rates). All visual acuity measurements were converted to LogMAR for pooling. Studies reporting on animal subjects, pediatric patients, mixed retinal detachments without clearly disaggregated RRD data, narrative reviews, or abstracts lacking comprehensive data were excluded.
Study selection, data extraction, and quality assessment
Retrieved studies were imported into EndNote 21 software, with duplicates removed electronically. Two independent reviewers screened the titles and abstracts for potential eligibility, followed by a detailed assessment of full-text articles against the defined inclusion criteria. Inter-rater reliability was quantified using Cohen’s κ, which indicated substantial agreement (κ = 0.90). Data extraction was independently conducted by two reviewers using a standardized form capturing study details (author, publication year, design, sample size), patient demographics (age, gender), clinical features (macula involvement, PVR grade), intervention specifics, and reported outcomes. Disagreements at each stage were resolved through consensus or arbitration by a third reviewer.
Studies were categorized into three groups based on the mean government Stringency Index (SI) during the study-specific observation period. Daily SI values were obtained from the Oxford COVID-19 Government Response Tracker (OxCGRT). 23 Borderline values were defined as a mean SI between 65 and 75. In these borderline cases, and in situations where the SI-derived estimate did not fully align with the epidemiological context of the country (particularly in several East Asian settings and China) the final classification was refined using the descriptions reported in the original studies regarding the nature, scope, and implementation of public health measures (e.g., nationwide lockdowns, mobility restrictions, school and workplace closures). To contextualize the severity of the pandemic across countries, excess mortality for the year 2020 was extracted from OxCGRT. 23 Countries were categorized into three levels of pandemic impact based on total excess deaths: high (≥1000 excess deaths), moderate-to-high (100–999 excess deaths), and low (<100 excess deaths). We assessed risk of bias in all included studies using the Joanna Briggs Institute (JBI) Critical Appraisal Tools (https://jbi.global/critical-appraisal-tools) for cohort studies. 24 The checklists cover domains that examine methodological quality, internal validity, and susceptibility to systematic bias.
For cohort studies, we evaluated 11 domains, including baseline comparability of groups, accuracy of exposure assessment, identification and management of confounders, completeness of follow-up, reliability of outcome measurement, and appropriateness of the statistical analyses. Each domain was judged as “Yes”, “No”, “Unclear”, or “Not Applicable” based on how well the study met the criterion.
Reporting quality was evaluated using an adapted version of the Downs and Black checklist, which included eight items assessing clarity of study aims, transparency of outcome definitions, completeness of patient and intervention descriptions, reporting of key confounders, presentation of main findings, and adequacy of statistical reporting (including measures of variability and exact p-values). 25 Two reviewers conducted the assessments independently, and any disagreements were resolved through discussion or by consulting a senior reviewer. (Supplemental Materials, Table S4).
Outcome measures and data synthesis
Data were quantitatively pooled when feasible; otherwise, narrative synthesis was performed. Outcomes were categorized into four domains 1 : incidence/surgical volume, 2 categorical clinical variables, 3 continuous clinical variables, and 4 surgical practice details. Incidence rates and risk ratios with 95% confidence intervals (CI) were reported. Meta-analyses were conducted where two or more comparable studies existed, utilizing fixed-effect or random-effects models based on Cochrane’s I2 statistic (random-effects model for I2 > 50%). Sensitivity analyses examined potential sources of heterogeneity.
To evaluate the impact of COVID-19–related restrictions on the number of RRD surgeries, rate ratios were calculated for each study based on the data reported and were entered into the meta-analysis. Subgroup analyses were conducted according to study setting, stringency category, excess mortality category, and the length of the exposure period (typically corresponding to the duration of the lockdown or the main pandemic wave) to identify potential sources of between-study heterogeneity. Categorical outcomes (macula status, presence of PVR, and anatomical success after a single surgery) were synthesized to yield odds ratios or risk ratios, with subgroup analyses whenever appropriate. Continuous outcomes were pooled as standardized mean differences with 95% CIs. Furthermore, in instances where data were presented as median and interquartile range (IQR), mean and standard deviation (SD) values were estimated by employing a validated, sample size-dependent transformation method introduced by Wan et al. 26 Additionally, quantitative data depicted graphically were extracted and digitized through PlotDigitizer, a web-based data extraction tool specifically designed for this purpose.
Details of surgical practices (procedure type, tamponade type, anesthesia, and single surgery success rates) were synthesized qualitatively. Publication bias was explored through funnel plots and Egger tests when at least ten studies were available. All statistical analyses and meta-analyses were executed using R statistical software (meta and metafor packages).
Results
Literature search and selection
An extensive and systematic literature search was executed across three major electronic databases (PubMed, Web of Science, and Embase), identifying a total of 611 records (131 from PubMed, 136 from Web of Science, and 344 from Embase). Subsequent to the removal of 230 duplicates, 381 unique records underwent initial screening based on titles and abstracts, resulting in the exclusion of 313 records. Consequently, 68 studies were considered potentially relevant and subjected to detailed full-text assessment. Upon rigorous evaluation, a further 39 studies were excluded due to insufficient quantitative data (n = 23), inappropriate publication formats such as reviews, comments, or conference abstracts (n = 8), overlapping patient populations (n = 3), absence of comparative control groups (n = 3), and publications not in English (n = 2). Ultimately, 29 studies fulfilled all established inclusion criteria and were incorporated into the final systematic review. The detailed selection workflow is visually represented in the accompanying PRISMA flow diagram (Figure 1). PRISMA 2020 flow diagram.
Study characteristics
Study and baseline patient characteristics*.

*Continuous variables are reported as mean ± SD, Median (IQR) or Median [Range].
Geographically, the included studies represent significant global diversity, spanning four continents. The United States contributed the highest number of studies (n = 6),11,20,27,32,36,37 followed by the United Kingdom4,6,17 and Japan12,29,31 (each n = 3). Additional studies originated from France5,34 and Italy13,14 (each n = 2), and one study each was reported from Canada, 7 Pakistan, 8 Poland, 28 Portugal, 15 China, 30 Austria, 33 Switzerland, 10 Germany, 19 Iran, 9 Korea, 38 Thailand, 18 Taiwan, 16 and Turkey. 35 The sample sizes varied substantially, ranging from 63 to 59,198 eyes or patients, collectively totaling more than 116,000 eyes.
Two principal comparator frameworks emerged for temporal analysis. Eighteen studies (62%) utilized an inter-year comparison, benchmarking data from LD periods against identical calendar intervals from pre-pandemic years. The remaining eleven studies (38%) employed an intra-year comparator, typically assessing data from months immediately preceding the confinement period (labeled as pre-COVID-19 or pre-LD depending on the precise temporal alignment). Among these, four studies also evaluated outcomes during the immediate post-LD (re-opening) phase, thus facilitating a preliminary assessment of healthcare service recovery.
Available demographic data indicated participant ages ranging from 11 to 93 years, with a study-level mean of approximately 56 years. Male patients constituted between 55% and 75% of the cohorts. Approximately two-thirds of the detachments occurred in phakic eyes, and trauma-related detachments represented fewer than 10% of cases. Median presenting visual acuity was generally poor, around 0.8–1.0 LogMAR (≈20/125 Snellen), reflecting the advanced severity of RRD at presentation.
Risk of bias assessment
Risk of bias within individual studies.
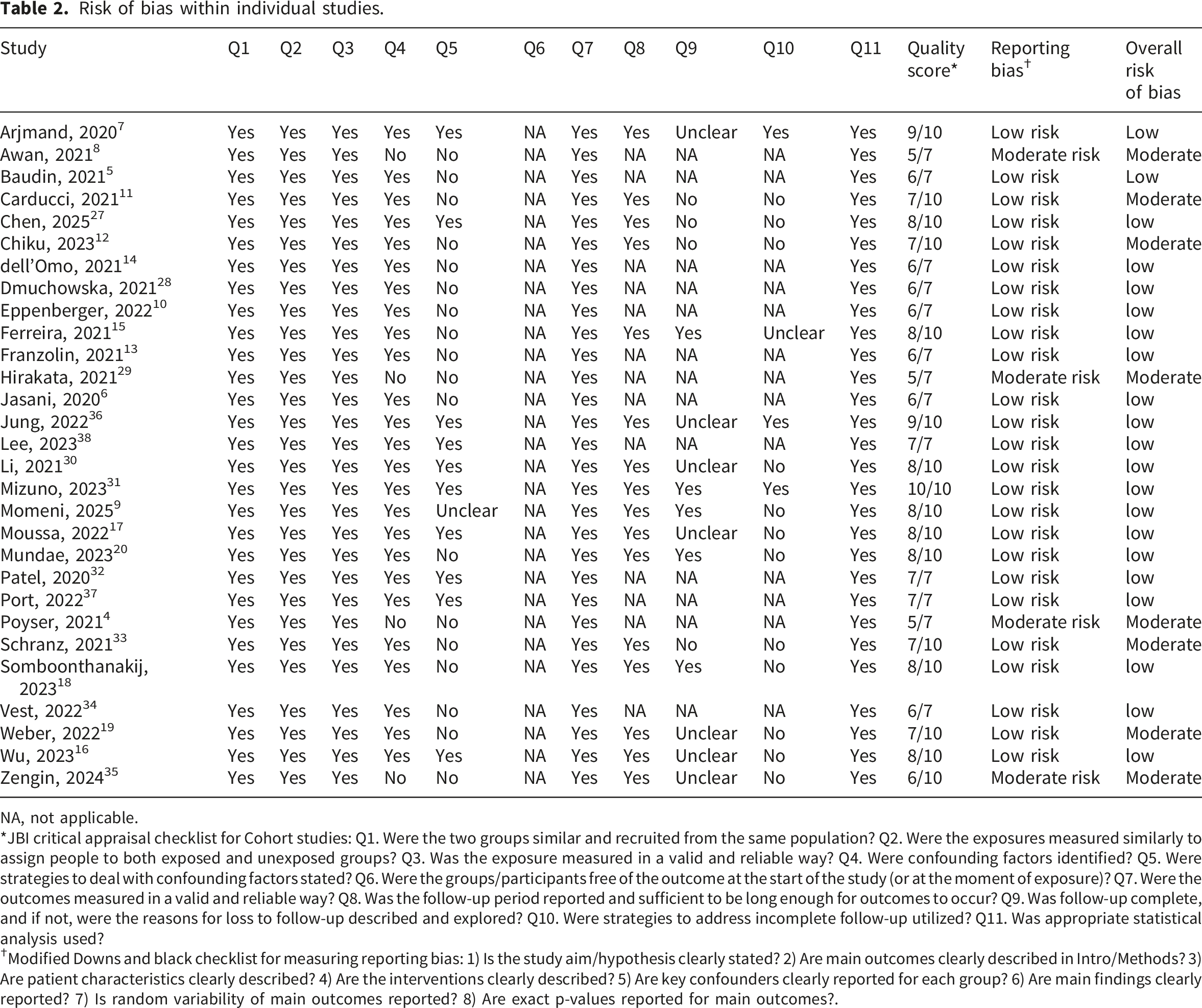
NA, not applicable.
*JBI critical appraisal checklist for Cohort studies: Q1. Were the two groups similar and recruited from the same population? Q2. Were the exposures measured similarly to assign people to both exposed and unexposed groups? Q3. Was the exposure measured in a valid and reliable way? Q4. Were confounding factors identified? Q5. Were strategies to deal with confounding factors stated? Q6. Were the groups/participants free of the outcome at the start of the study (or at the moment of exposure)? Q7. Were the outcomes measured in a valid and reliable way? Q8. Was the follow-up period reported and sufficient to be long enough for outcomes to occur? Q9. Was follow-up complete, and if not, were the reasons for loss to follow-up described and explored? Q10. Were strategies to address incomplete follow-up utilized? Q11. Was appropriate statistical analysis used?
✝Modified Downs and black checklist for measuring reporting bias: 1) Is the study aim/hypothesis clearly stated? 2) Are main outcomes clearly described in Intro/Methods? 3) Are patient characteristics clearly described? 4) Are the interventions clearly described? 5) Are key confounders clearly reported for each group? 6) Are main findings clearly reported? 7) Is random variability of main outcomes reported? 8) Are exact p-values reported for main outcomes?.
Overall, the included studies demonstrated reasonable methodological strength in several domains, including the comparability of study groups (Q1), the consistent and well-defined classification of exposure periods (Q2–Q3), the valid outcome measurement (Q7), and the use of statistically appropriate analytical methods (Q11). In studies that assessed postoperative outcomes, the duration of follow-up was generally sufficient (Q8); most provided roughly three months of postoperative observation or more, which is typically adequate to evaluate key early surgical endpoints such as initial anatomical success or short-term visual improvement. However, several recurrent methodological limitations were observed. 1) Confounder reporting (Q4) was variable, and strategies for confounder management (Q5) were limited. Most studies reported common baseline characteristics such as age, gender, lens status, or laterality. However, important potential confounders (such as referral patterns, travel distance to the treating center, socioeconomic status, insurance type, and prior ocular procedures) were reported only in a minority of studies. Furthermore, only a small number of studies implemented analytical methods to reduce confounding, such as multivariable regression or stratified analysis, leaving most analyses vulnerable to residual confounding. 2) Outcome-free status at baseline (Q6) was not applicable to the design of these studies. Because all included cohorts consisted of patients already diagnosed with RRD at presentation or at the time of surgery, this item does not align with the underlying structure of surgical or presentation-based cohort designs. 3) Completeness of follow-up and handling of missing data (Q9–Q10) were major weaknesses. While follow-up duration was usually adequate, most studies did not report the reasons for loss to follow-up or the characteristics of patients who were not retained. Additionally, most of the studies did not employ formal strategies (such as sensitivity analyses or imputation) to address missing outcome data.
Overall, most studies demonstrated a low risk of reporting bias, with study objectives, outcomes, interventions, and main results generally reported with adequate clarity and transparency. However, due to incomplete reporting of confounding factors, a number of studies were classified as having a moderate risk of reporting bias (Table 2 and Supplemental Table S4).
Incidence and surgical volume
Across 19 studies, COVID-19–related restrictions were associated with a significant reduction in the number of RRD surgeries (rate ratio 0.71, 95% CI 0.60–0.84; p=0.0004), with substantial heterogeneity between studies (I2=87.2%, p<0.0001) (Figure 2). Subgroup analyses based on excess mortality level, exposure duration, and restriction severity were statistically significant and accounted for part of the between-study heterogeneity (Table 3). Forest plot of studies comparing the RRD surgery volume during COVID-19 LD versus pre-LD periods. Subgroup analyses of changes in RRD surgical volume during COVID-19 lockdown periods.

Furthermore, eleven studies assessing extended periods (6–14 months) post-pandemic onset, irrespective of LD conditions, identified a median reduction of 8.1% in overall surgical volumes for RRD (mean: −5.4%; range: −35% to +86.0%). These findings suggest partial recovery of surgical activity but persistent deficits relative to pre-pandemic standards (Figure 3). Percentage change in overall RRD surgical volume during extended post-pandemic intervals (6–14 months) in 11 studies.
Clinical presentation
The meta-analysis revealed a significant decrease in the likelihood of presenting with macula-on RRD during COVID-19 LD periods (Figure 4). Analysis comparing LD periods to pre-LD periods across 15 studies demonstrated a statistically significant reduction in macula-on RRD presentations during LD (OR = 0.61; 95% CI: 0.46 – 0.83; I2 = 33.5%). Sensitivity analysis (leave-one-out approach) confirmed the robustness of these findings, indicating consistent results across studies (Supplemental Figure S1). Funnel plot asymmetry testing showed no significant evidence of publication bias (z = -0.5129, P-value = 0.6080), although the trim-and-fill method estimated two potentially missing studies on the right side (Supplemental Figure S2). Forest plot of studies comparing the likelihood of macula-on RRD at presentation during COVID-19 LD versus pre-LD periods.
When comparing COVID-19 periods to pre-COVID-19 eras, the meta-analysis of 9 studies showed no significant change in macula-on presentations (OR = 1.03; 95% CI: 0.91 – 1.18; I2 = 34.9%), indicating that the observed effect was specific to LD conditions rather than the broader COVID-19 era (Figure 5). Forest plot of studies comparing macula-on RRD presentations during COVID-19 versus pre-COVID-19 periods, showing no significant difference.
Furthermore, the comparison of LD periods with post-LD periods in 5 studies also yielded a significant decrease in macula-on cases during LD (OR = 0.65; 95% CI: 0.44 – 0.96; I2 = 0.0%) (Figure 6). Forest plot of studies comparing LD and post-LD periods, showing a significant decrease in macula-on RRD presentations during LD.
The meta-analysis investigating the extent of retinal detachment across the number of quadrants involved revealed no statistically significant differences in LD and pre-LD periods or between the broader COVID-19 era and pre-COVID-19 periods (Figure 7). Specifically, comparisons between LD and pre-LD periods involving 1 quadrant (OR = 0.89; 95% CI: 0.43 – 1.84; I2 = 0%), 2 quadrants (OR = 0.98; 95% CI: 0.63 – 1.52; I2 = 24.6%), 3 quadrants (OR = 1.47; 95% CI: 0.85 – 2.57; I2 = 0%), and 4 quadrants (OR = 1.40; 95% CI: 0.95 – 2.04; I2 = 13.4%) showed non-significant trends toward increased retinal involvement during LD periods. Similar trends were observed when comparing COVID-19 to pre-COVID-19 periods, with involvement of 1 quadrant (OR = 0.79; 95% CI: 0.53 – 1.18; I2 = 44.9%), 2 quadrants (OR = 0.92; 95% CI: 0.68 – 1.23; I2 = 0%), 3 quadrants (OR = 1.21; 95% CI: 0.85 – 1.71; I2 = 62.7%), and 4 quadrants (OR = 1.31; 95% CI: 0.89 – 1.95; I2 = 0%) all remaining statistically non-significant. Summary of odds ratios comparing the extent of retinal detachment.
The overall comparison of PVR incidence revealed a significantly higher risk during the LD period compared to Pre-LD (OR = 2.48; 95% CI: 1.74 – 3.53, I2 = 14.0%) (Figure 8). Subgroup analyses indicated a significantly increased odds for moderate to severe (Grade B-C) PVR during LD (OR = 2.58; 95% CI: 1.37 – 4.87, I2 = 0%). However, analysis of all-grade PVR demonstrated a nonsignificant elevation in odds (OR = 2.18; 95% CI: 0.61 – 7.75, I2 = 54.8%). PVR incidence before LD vs. during LD.
The overall incidence of primary PVR was significantly higher during the COVID-19 period compared to the pre-COVID-19 period, with considerable heterogeneity (OR = 1.88; 95% CI: 1.13 – 3.16, I2 = 76.5%). Subgroup analyses revealed no significant increase for all-grade PVR (OR = 1.24; 95% CI: 0.92 – 1.67, I2 = 15.7%), but significantly higher odds of grade B-C PVR during the COVID-19 period (OR = 3.19; 95% CI: 2.18 – 4.66, I2 = 0%) (Figure 9). PVR incidence before COVID-19 vs. during COVID-19.
Visual acuity analysis showed no statistically significant differences at baseline between the LD and Pre-LD periods (SMD = 0.169; 95% CI: 0.066 – 0.272; I2 = 36.6%), COVID-19 and pre-COVID-19 periods (SMD = 0.065; 95% CI: 0.001 – 0.129; I2 = 44.6%), or LD and post-LD periods (SMD = 0.088; 95% CI: -0.06 – 0.24; I2 = 0%). Similarly, postoperative visual acuity revealed no significant differences between LD vs. Pre-LD (SMD = 0.137; 95% CI: -0.001– 0.28; I2 = 3.3%), COVID-19 vs. Pre-COVID-19 (SMD = 0.194; 95% CI: -0.04 – 0.43; I2 = 86.4%), or LD vs. Post-LD comparisons (SMD = -0.152; 95% CI: -0.34 – 0.03; I2 = 0%) (Figure 10). Baseline and postoperative visual acuity comparisons across periods.
When analyzing “Time to Presentation (interval from symptom onset to medical visit),” results suggested a potential increase during the LD compared to Pre-LD, although this difference was not statistically significant (SMD = 0.196; 95% CI: -0.16 – 0.55; I2 = 79.2%). Similarly, comparisons between COVID-19 vs. pre-COVID-19 (SMD = 0.056; 95% CI: -0.14 – 0.25; I2 = 66.2%) and LD vs. post-LD periods also did not show significant differences (SMD = -0.14; 95% CI: -0.31 – 0.02; I2 = 32.1%). However, “Time to Surgery (interval from symptom onset to surgical intervention)” was significantly increased during the LD compared to Pre-LD period (SMD = 0.29; 95% CI: 0.12 – 0.46; I2 = 0%). “Presentation-to-Surgery Time (interval from first medical visit to surgical intervention)” decreased significantly during LD compared to Pre-LD (SMD = -0.25; 95% CI: -0.38 – -0.124; I2 = 19.1%), but showed no significant difference for COVID-19 vs. Pre-COVID-19 (SMD = 0.167; 95% CI: -0.62 – 0.956; I2 = 97.8%) and LD vs. Post-LD comparisons (SMD = -0.095; 95% CI: -0.266 – 0.074; I2 = 0%) (Figure 11). Time intervals in patient management: (A) Time to presentation (symptom onset to medical visit), (B) Time to surgery (symptom onset to surgery), and (C) Presentation-to-surgery time (first visit to surgery).
Surgical practice details
Surgery details and treatment outcomes*.

*Continuous variables are reported as mean ± SD or Median (IQR).
✝Time between the first presentation to surgery.
Tamponade selection varied notably across studies. Gas tamponade remained the preferred choice overall, but specific preferences differed significantly among centers (Table 4). During the COVID-19 LDs, a shift toward longer-acting gases such as C3F8 or silicone oil was observed in several studies.15–17,30,33
Reports on the use of general anesthesia were limited, yet two studies demonstrated an increased adoption of general anesthesia during the COVID-19 era.9,16 Conversely, one study reported a reduction in use of general anesthesia. 11
Comparing LD periods to pre-LD periods, single-surgery retinal attachment rates remained comparable (OR = 0.90; 95% CI: 0.57 – 1.41; I2 = 0%) (Figure 12). Single-surgery retinal attachment rates during LD vs. Pre-LD periods.
Similarly, the comparison between COVID-19 periods and pre-COVID-19 periods demonstrated no significant difference in single-surgery retinal attachment rates, despite notable heterogeneity among studies (OR = 0.57; 95% CI: 0.24 – 1.38; I2 = 84.5%) (Figure 13). Single-surgery retinal attachment rates during COVID-19 vs. pre-COVID-19 periods.
Sensitivity analysis and publication bias assessment
Summary of pooled effect sizes, sensitivity analyses, and publication bias for study outcomes.

1Significance flipped and heterogeneity disappeared upon removal of Wu et al. (2023) and Somboonthanakij et al. (2023).
2Significance flipped and heterogeneity disappeared upon removal of Vest et al. (2022).
3Significance flipped upon removal of any of the following studies: Patel et al. (2020), Li et al. (2021), Wu et al. (2023), Weber et al. (2022), Vest et al. (2022), or Carducci et al. (2021).
4Significance flipped and heterogeneity disappeared upon removal of Li et al. (2021).
5Significance flipped upon removal of Mundae et al. (2023) and Mizuno et al. (2023).
6Significance flipped and heterogeneity dropped upon removal of Mundae et al. (2023).
7Significance flipped and heterogeneity dropped upon removal of Mundae et al. (2023), Mizuno et al. (2023) and Arjmand et al. (2020).
8Significance flipped and heterogeneity dropped upon removal of Ferreira et al. (2021).
In the broader comparison between the COVID-19 and pre-COVID-19 eras, the statistically significant findings for PVR incidence, baseline visual acuity, and single-surgery attachment rates were not robust in the sensitivity analysis. Similarly, the non-significant finding for post-operative visual acuity was also not robust. The significance of these outcomes was dependent on the inclusion of specific studies, as noted in Table 5. The results for all other outcomes in this comparison were robust.
All findings from the comparison between the LD and post-LD periods were demonstrated to be robust in the leave-one-out sensitivity analysis.
Discussion
The COVID-19 pandemic initiated a multifaceted and geographically varied impact on the presentation and management of RRD services.39,40 Our systematic review and meta-analysis revealed a significant overall reduction in RRD incidence during LD periods, although this decrease varied markedly among regions. Individual studies showed median surgical volume declines of 29.1% during LD periods, with reductions ranging from 85.4% 13 to paradoxical increases of 73.1%. 11 The observed disparities can be attributed to diverse local healthcare policies, variations in patient referral patterns, hospital resource allocation, and the operational status of ophthalmologic facilities during the pandemic.5,9
Several interrelated factors underpinned the observed decline in RRD presentations during LD. These factors included patient apprehension regarding COVID-19 exposure in healthcare settings, strict governmental movement restrictions and stay-at-home orders, widespread uncertainty about ophthalmic service availability, and disrupted transportation infrastructure. 7 Additionally, the general reduction in outdoor and contact sports due to LDs might have indirectly contributed to fewer incidences of retinal tears and subsequent RRDs, as such activities are known risk factors for RRD.6,13,37
Despite the decline in presentations, the reduced incidence was frequently associated with delayed patient presentations, characterized by prolonged symptom durations, more advanced stages of disease, a higher frequency of macula-off detachments, and increased severity, notably higher incidences of PVR.4,13,37,41 Our meta-analysis specifically highlighted that patients during LD periods were significantly less likely to present with macula-on RRD (OR = 0.61; 95% CI: 0.46 – 0.83; I2 = 33.5%) compared to pre-LD periods. Conversely, when comparing the broader COVID-19 periods to pre-COVID-19 eras, the meta-analysis revealed no significant change in macula-on presentations (OR = 1.03; 95% CI: 0.91 – 1.18; I2 = 34.9%), indicating that the observed delays were specifically attributable to LD measures rather than the pandemic itself. Additionally, patients during LD had higher odds of moderate to severe PVR (OR = 2.58; 95% CI: 1.37 – 4.87). These findings reinforce the clinical implications of delayed ophthalmic care directly associated with LD restrictions, as prolonged macular detachment and advanced PVR significantly impact visual prognosis.
Interestingly, several centers demonstrated notable resilience and adaptation to the crisis, maintaining stable or even increased surgical activity and ensuring relatively timely referrals and interventions. In some settings, the reduction in outpatient visits and elective activities during lockdown periods may have also contributed to improved operating room availability and shorter surgical waiting times. For example, a high-volume Iranian center reported not only an increase in the number of RRD surgeries but also significantly shorter referral times (44.97 vs. 76.76 days) and reduced surgical wait times (4.64 vs. 8.63 days). 9 This resilience was primarily attributed to the continuous full operation of specialized facilities and redirected patient referrals from temporarily closed institutions. 9 Similar adaptability was evident in centers in Taiwan and Turkey, where emergency ophthalmic services remained largely unaffected due to proactive contingency planning and robust emergency protocols.16,35 Additionally, a study in Poland found that while RRD referrals decreased initially, the impact lessened with successive waves of the pandemic, with no significant changes in patient demographics. 28 Furthermore, sustained observations over a longer period in the UK indicated that initial lower presentation rates and increased macula-off RRDs were not maintained or did not recur after the second LD, suggesting effective adaptations in patient behavior and healthcare services over time. 17
Our analysis also indicated significant shifts in surgical management practices during the pandemic. There was a marked increase in the utilization of PPV, often accompanied by the use of longer-acting gas tamponades (e.g., C3F8) or silicone oil, intended to minimize the need for reoperations because of limited healthcare resources and restricted access to operating theaters. Specifically, centers in Portugal, Pakistan, and the UK reported increased adoption of silicone oil and longer-acting gases to manage more complex presentations.8,15,17 Conversely, Taiwanese practices increasingly employed combined PPV and SB procedures, aiming to enhance surgical stability and minimize postoperative follow-up visits. 16
Even with these challenges and changes, the final anatomical outcomes after surgery were generally similar to those before the pandemic. Specifically, the single-surgery retinal attachment rates were stable across most studies. Our analysis showed no significant difference in single-surgery retinal attachment rates when comparing the LD periods to the periods before LD (OR = 0.90; 95% CI: 0.57 – 1.41; I2 = 0%). Similarly, when looking at the entire COVID-19 era compared to the period before COVID-19, single-surgery retinal attachment rates were also not significantly different, although there was high variability among studies (OR = 0.57; 95% CI: 0.24 – 1.38; I2 = 84.5%). However, some regions, particularly Japan, reported initial decreases in retinal attachment success, along with poorer visual outcomes in patients who delayed seeking treatment. 31 These findings emphasize how essential it is to maintain prompt access to ophthalmic care during major health crises to prevent long-term visual impairment.15,32,35,37
The additional subgroup analyses provided further insight into the substantial heterogeneity observed across studies. Variations in lockdown severity, duration of restrictions, and regional pandemic burden appeared to influence the magnitude of reductions in RRD surgical volume. In general, stricter lockdown measures were associated with greater declines in surgical activity, supporting the hypothesis that regional public health responses and healthcare system pressures played an important role in shaping access to emergency ophthalmic care during the pandemic.
A key contributor to the substantial heterogeneity observed in the pooled analyses (particularly for RRD incidence and surgical volume) likely relates to structural differences across healthcare systems and regional pandemic responses. Importantly, although “lockdown” was operationally defined in this review, its real-world implementation varied considerably across countries and even within regions in terms of timing, duration, and strictness. Variability in the strictness and duration of lockdown measures, differences in public health messaging, and regional healthcare policies governing elective and emergency services may have markedly influenced patient access and referral pathways. These differences in lockdown implementation may have directly affected both patient healthcare-seeking behavior and institutional surgical strategies, thereby contributing to the observed variability in clinical presentations and management approaches. In many settings, referral patterns were altered due to the temporary closure of peripheral clinics, redistribution of emergency services, or the designation of specific centers as COVID-19 facilities. Consequently, tertiary referral centers may have experienced either pronounced declines in caseload due to reduced mobility and patient hesitancy, or paradoxical increases owing to the centralization of urgent ophthalmic care. Furthermore, registry-based national studies inherently capture broader population-level trends, whereas single-center analyses reflect local operational dynamics, resource allocation, and institutional resilience. These structural and policy-related differences likely represent major drivers of the heterogeneity observed across studies and should be considered when interpreting pooled estimates.
This systematic review and meta-analysis have several inherent limitations. First, the retrospective design of all included studies introduces potential biases, including selection, recall, and reporting biases, leading to variability in data quality and completeness. Additionally, the overall quality and methodological variability of the included studies may have influenced the pooled estimates and should be considered when interpreting the findings. Secondly, considerable heterogeneity existed in LD measures, healthcare system capacities, regional healthcare policies, and patient demographics, which complicated direct comparisons across studies and limited the generalizability of certain findings. Thirdly, the absence of detailed demographic and socioeconomic data across studies restricted our ability to fully explore underlying factors influencing patient behavior and healthcare accessibility. In addition, important contextual variables (such as center representativeness, healthcare access pathways, and regional COVID-19 burden and lockdown characteristics) were inconsistently or not reported across studies, precluding more detailed subgroup analyses. Additionally, variability in definitions and grading criteria for clinical outcomes, such as PVR and visual acuity measurements, introduced further challenges in standardizing data synthesis. Finally, most included studies had relatively short and heterogeneous follow-up durations, which limits the evaluation of long-term anatomical and functional outcomes. Moreover, variations in follow-up length across studies, particularly during the pandemic period, may have influenced the comparability of reported postoperative visual outcomes.
Conclusions
The COVID-19 pandemic had substantial, region-specific impacts on RRD management, significantly influencing patient presentation patterns, disease severity, and surgical management practices. The considerable variability in responses and outcomes observed across different regions highlights the critical need for adaptable ophthalmic emergency services capable of ensuring timely patient access under varying healthcare conditions. Continued public education emphasizing the urgency of visual symptoms, combined with proactive contingency planning and resilient healthcare strategies, are vital for minimizing negative outcomes and safeguarding vision during future global health crises.
Supplemental material
Supplemental material - Impact of COVID-19 pandemic on surgical volume, clinical presentations, and management of rhegmatogenous retinal detachment: A systematic review and meta-analysis
Supplemental material for Impact of COVID-19 pandemic on surgical volume, clinical presentations, and management of rhegmatogenous retinal detachment: A systematic review and meta-analysis by Hassan Asadigandomani, Ali Tahmasebi, Mahan Jalilzadeh, Melika Arab Bafrani, Fatemeh Mahmoudi, Kimia Daneshvar, Sara Kamali Zonouzi, Hamid Riazi-Esfahani and Elias Khalili Pour in Sage Open Medicine.
Supplemental material
Supplemental material - Impact of COVID-19 pandemic on surgical volume, clinical presentations, and management of rhegmatogenous retinal detachment: A systematic review and meta-analysis
Supplemental material for Impact of COVID-19 pandemic on surgical volume, clinical presentations, and management of rhegmatogenous retinal detachment: A systematic review and meta-analysis by Hassan Asadigandomani, Ali Tahmasebi, Mahan Jalilzadeh, Melika Arab Bafrani, Fatemeh Mahmoudi, Kimia Daneshvar, Sara Kamali Zonouzi, Hamid Riazi-Esfahani and Elias Khalili Pour in Sage Open Medicine.
Supplemental material
Supplemental material - Impact of COVID-19 pandemic on surgical volume, clinical presentations, and management of rhegmatogenous retinal detachment: A systematic review and meta-analysis
Supplemental material for Impact of COVID-19 pandemic on surgical volume, clinical presentations, and management of rhegmatogenous retinal detachment: A systematic review and meta-analysis by Hassan Asadigandomani, Ali Tahmasebi, Mahan Jalilzadeh, Melika Arab Bafrani, Fatemeh Mahmoudi, Kimia Daneshvar, Sara Kamali Zonouzi, Hamid Riazi-Esfahani and Elias Khalili Pour in Sage Open Medicine.
Footnotes
Ethical considerations
This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Author contributions
H.A conceived and supervised the study. A.T contributed to database searching, screening, data extraction, formal analysis, visualization, and manuscript drafting. M.J prepared the proposal, participated in screening, data extraction, risk of bias assessment, and manuscript preparation for submission. M.A assisted in data analysis and interpretation. F.M, K.D, and S.K contributed to data collection, reference management, and manuscript revision. H.R and E.K provided critical supervision, methodological guidance, and final approval of the manuscript. All authors reviewed and approved the final version.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of generative AI
For this research, the authors employed ChatGPT to enhance the clarity and readability of the language. After utilizing this tool, they meticulously examined and adjusted the material as needed, taking complete responsibility for the published work.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.