
Abstract
Background
Gestational diabetes mellitus (GDM) is a common pregnancy complication with significant maternal and neonatal consequences.
Aim
To synthesise evidence on knowledge, awareness, and perception of men and women of reproductive age on GDM to enhance effective prevention and management of GDM.
Methods
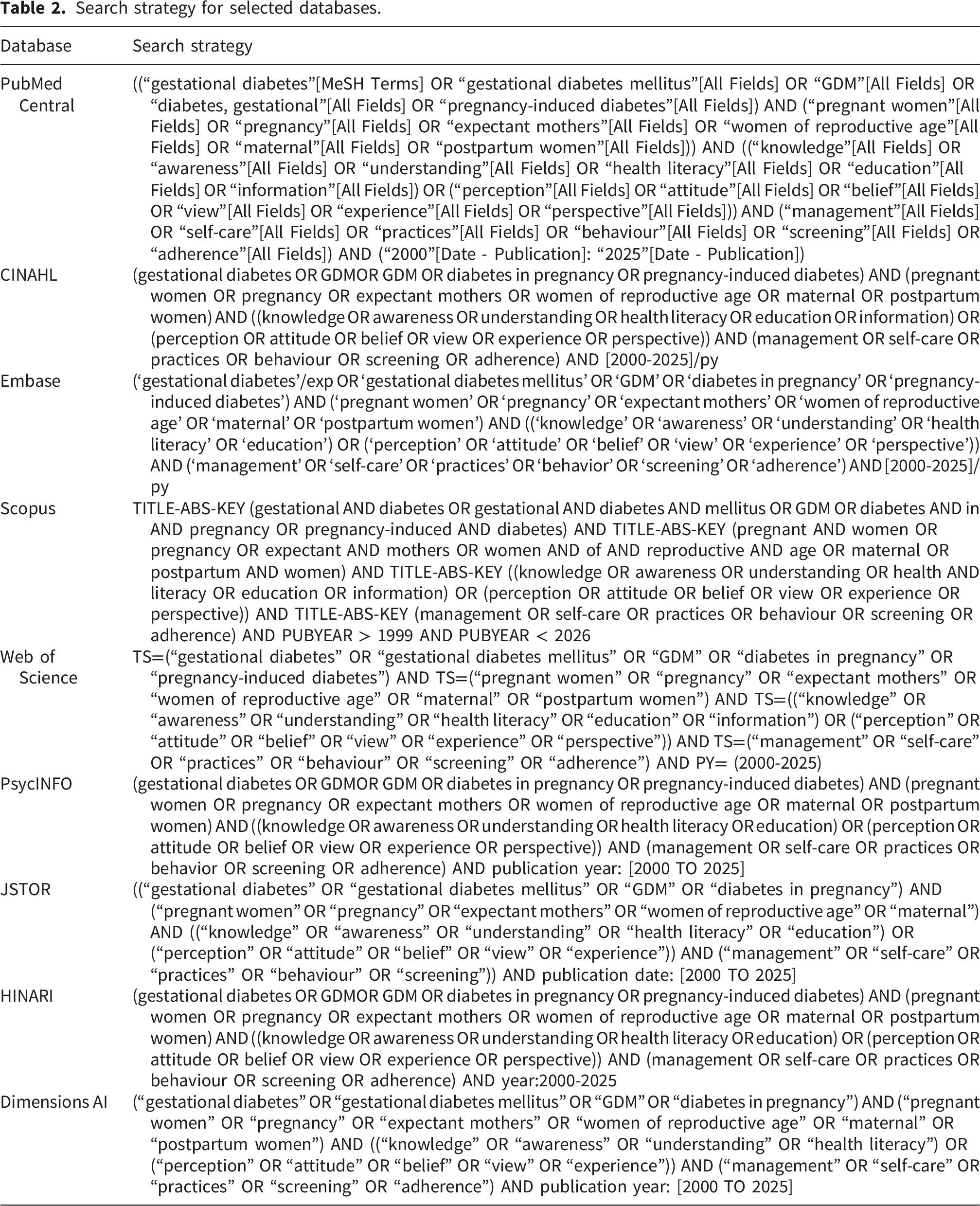
A systematic review was conducted following PRISMA guidelines across PubMed, CINAHL, Embase, Scopus, Web of Science, PsycINFO, JSTOR, Dimensions AI, and HINARI for studies published between 2000 and 2025. 50 studies, with a total sample size of 29,590 participants, assessing knowledge, awareness, attitudes, or perceptions of GDM among pregnant, postpartum, or reproductive-age women were included. Data were extracted, quality-appraised using JBI and MMAT tools, and synthesised thematically.
Results
Fifty studies were included, primarily cross-sectional (88%), with qualitative (8%) and mixed-methods (4%) designs. Women generally demonstrated limited understanding of GDM risk factors, screening procedures, and long-term implications. Cultural norms, emotional responses, and healthcare experiences shaped perceptions and attitudes, sometimes reducing engagement with preventive behaviours. Factors improving knowledge and adherence included structured education, prior exposure to diabetes, supportive healthcare interactions, and family involvement.
Conclusion
Awareness and understanding of GDM remain inadequate globally emphasizing major public health concern. Targeted educational interventions, culturally sensitive resources, and enhanced provider–patient engagement are essential to improve knowledge, attitudes, and health outcomes. Future research should prioritise interventional and longitudinal studies using standardised measures across diverse populations.
Background
Gestational diabetes mellitus (GDM) represents one of the most common metabolic disorders affecting pregnant women worldwide. The condition develops when pancreatic beta cells fail to compensate adequately for pregnancy-induced insulin resistance, resulting in hyperglycaemia during gestation. 1 Global prevalence estimates indicate that approximately one in seven pregnancies is affected by GDM, with regional variations ranging from 5.8% in Europe to 13% in Middle Eastern and North African populations. 1 Moreover, the incidence continues to rise, driven primarily by increasing maternal age, obesity rates, and sedentary lifestyles across diverse populations. 2 This burden presents substantial challenges for maternal and child health services globally. Furthermore, the consequences of GDM extend beyond immediate pregnancy outcomes. Women diagnosed with the condition face a threefold elevated risk of developing type 2 diabetes postpartum, whilst their offspring experience heightened vulnerability to childhood obesity and metabolic disorders. 1 Short-term maternal complications include pre-eclampsia, caesarean delivery, and labour induction, whereas foetal risks comprise macrosomia, neonatal hypoglycaemia, and shoulder dystocia. 2 Additionally, long-term evidence demonstrates that intrauterine exposure to maternal hyperglycaemia may contribute to neurodevelopmental alterations, including autistic spectrum disorder, and establishes intergenerational patterns of cardiometabolic disease. 2 These findings emphasise the importance of early identification and appropriate management strategies during pregnancy and beyond.
However, effective prevention and management of GDM depend substantially on women’s knowledge, awareness, and perceptions of the condition. Recent studies reveal concerning gaps in understanding among pregnant women across different geographical contexts. Studies have shown that in Kenya, 86.16% of pregnant women had never heard of GDM, whilst only 13.90% possessed adequate knowledge about the condition. 3 Similarly, investigations in China documented that although 70% of women demonstrated satisfactory knowledge scores, merely 45% exhibited positive attitudes, and 43% engaged in appropriate practices for diabetes management. 4 Furthermore, studies from India reported that only 17.5% of rural antenatal women possessed good knowledge about GDM, with substantial deficits in understanding screening protocols and potential complications.5,6 These findings show the persistent educational challenges that healthcare systems must address to improve pregnancy outcomes. Consequently, women’s perceptions and attitudes towards GDM influence their health-seeking behaviours and adherence to management protocols. Qualitative research has identified that women often experience psychosocial distress following diagnosis, characterised by feelings of shock, guilt, and anxiety about potential harm to their unborn children. 7 Additionally, many women perceive the diagnosis as overwhelming, particularly when confronted with dietary modifications, blood glucose monitoring, and frequent medical appointments during an already demanding period. 8 Studies examining postpartum screening adherence reveal that competing priorities, such as childcare responsibilities and lack of family support, serve as substantial barriers to attendance, with uptake rates falling below 55% in many settings.9,10 Moreover, healthcare system factors, including fragmented care pathways, ambiguous provider responsibilities, and inadequate patient education materials, further impede women’s engagement with both antenatal and postpartum diabetes services.10,11
Therefore, this systematic review aims to synthesise current evidence on knowledge, awareness, and perception of men and women of reproductive age on GDM to enhance effective prevention and management of GDM. By examining educational interventions, cultural influences, and healthcare delivery systems, this review seeks to identify effective strategies for improving men’s and women’s understanding and engagement with GDM prevention and management programmes. Such insights will inform the development of targeted interventions that address both individual-level knowledge deficits and systemic barriers within healthcare settings. Ultimately, enhanced awareness and appropriate perception of GDM may facilitate earlier diagnosis, improved glycaemic control during pregnancy, and greater participation in postpartum screening and diabetes prevention initiatives.
Methods
This systematic review adhered to the methodological guidelines established by 12 and endorsed by the Joanna Briggs Institute (JBI). The guidelines consist of seven essential components: (1) formulation of explicit research objectives and questions, (2) specification of precise inclusion and exclusion parameters, (3) detailed search strategy, (4) rigorous quality appraisal of selected studies, (5) systematic analysis of extracted data, (6) coherent presentation and integration of results, and (7) clear documentation of methodological processes. Reporting of the search results of this review was guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
Research questions
1. What is the level of knowledge and awareness about GDM among pregnant women and women of reproductive age? 2. What are women’s perceptions and attitudes towards GDM diagnosis and management?
The research questions were formulated based on the Population–Concept–Context (PCC) framework, which is appropriate for systematic reviews that include qualitative, quantitative, and mixed-methods studies. This structured approach ensured that the review remained focused on synthesising evidence regarding knowledge, awareness, and perceptions of GDM among women whilst embracing different study designs and geographical contexts.
Inclusion and exclusion criteria

Search strategy
Search strategy for selected databases.
Study selection
All retrieved records were imported into Mendeley referencing software version 1.19.8 for bibliographic management. Duplicate entries were identified and removed through a combination of automated detection and manual verification. Following deduplication, the titles and abstracts of the remaining studies were screened against the predefined eligibility criteria presented in Table 1. This initial screening phase was conducted by two trained graduate students under the supervision of CA and DA to ensure consistency and compliance with the inclusion parameters. Subsequently, the reference lists of potentially eligible records were manually examined to identify additional relevant studies that may have been missed in the database searches. Corresponding authors of eligible studies without accessible full-text versions were contacted via email to request article copies. Full-text articles of all potentially relevant studies were then retrieved and independently assessed by two reviewers against the eligibility criteria. Any disagreements between the two reviewers during full-text screening were resolved through discussion, and where consensus could not be reached, a third reviewer was consulted for final arbitration. The study selection process was systematically documented using a PRISMA flow diagram, indicating the number of records identified, screened, excluded, and included at each stage.
Data extraction
A data extraction form was developed using Microsoft Word to systematically capture information from included studies. The form was piloted on five randomly selected studies to assess its reliability and effectiveness in capturing essential information. This pilot phase allowed for necessary refinements based on practical application. Key information extracted included author names, publication year, country of study, study purpose, research design, population characteristics, sample size, knowledge and awareness levels, perception and management practices, and study outcomes. The extracted data were reviewed by EJ and SEB and supervised by CA. Discrepancies identified during the review process were documented and discussed during regular team meetings. Where disagreements persisted, they were resolved by CA. See Appendix A for details of the extracted data.
Critical quality assessment
Quality appraisal of the included studies was performed in parallel with data extraction using the quality appraisal tools developed by the Joanna Briggs Institute (JBI). The goal was to ensure that study inclusion and interpretation of findings were informed by the extracted data. These tools comprise checklists for evaluating the quality of cross-sectional studies, qualitative studies, cohort studies, quasi-experimental studies, and mixed-methods studies. The scoring procedures adopted for JBI cross-sectional studies 13 were 1–4 (High risk of bias), 5–6 (Moderate risk of bias), and 7–8 (Low risk of bias). The scoring procedures adopted for JBI qualitative studies 14 were 1–5 (High risk of bias), 6–7 (Moderate risk of bias), and 8–10 (Low risk of bias). For Mixed Method Appraisal Tool (MMAT), 15 1–2 (High risk of bias), 3–4 (Moderate risk of bias), and 5 (Low risk of bias). Two independent reviewers (EJ and EB) conducted quality assessments, and disagreements were resolved through consensus discussions, with a third reviewer (CA) consulted where necessary. Studies were not excluded based on quality scores; however, quality ratings informed the interpretation of findings and the strength of evidence. Thus, all studies were included to ensure comprehensive evidence representation across diverse populations and settings, with quality appraisal serving an informative rather than exclusionary purpose. Low-risk studies were accorded greater interpretive weight during synthesis, whilst moderate-risk studies were interpreted cautiously with explicit acknowledgement of their methodological limitations in the discussion.
Data analysis and synthesis
Thematic analysis was first conducted to identify, organise, and interpret patterns across the data extracted from the included studies. This process began with familiarisation, involving repeated reading of the extracted data to gain a thorough understanding of the content related to knowledge, awareness, and perceptions of GDM. Initial codes were then generated to capture meaningful features of the data concerning knowledge gaps, awareness levels, perceptions, and attitudes in GDM care. These codes were subsequently grouped into potential themes based on conceptual similarities and alignment with the review objectives. Through an iterative process of review and discussion among the research team, themes were refined to ensure clarity, consistency, and relevance. A thematic framework was then developed to represent and organise the final themes and sub-themes visually. Quantitative data on knowledge scores, awareness prevalence, and perception measures were presented in summary tables and figures to complement the qualitative synthesis. Where appropriate and sufficient homogeneity existed across studies with similar populations, outcome measures, and study designs, descriptive statistical summaries were compiled. Statistical heterogeneity was assessed to determine the feasibility of quantitative integration.
Following thematic analysis, a convergent synthesis approach was employed to integrate findings from studies with varied methodological designs. This approach was chosen to accommodate the inclusion of both qualitative and quantitative evidence within a unified framework. Quantitative findings were transformed into qualitative descriptions through a process known as qualitisation, enabling their integration with qualitative data. This allowed for a unified interpretation of all study results across different research approaches. The synthesis involved systematically comparing and interpreting the developed themes across studies to identify areas of convergence and divergence. Key insights were drawn by analysing how knowledge, awareness, and perceptions of GDM were consistently or variably reported across different geographical settings, populations, healthcare contexts, and study types. Both descriptive themes summarising what participants reported and analytical themes generating new interpretations were developed. The synthesis process maintained analytical rigour and transparency throughout. This resulted in the identification of overarching themes that offered a detailed understanding of the factors influencing knowledge, awareness, and perception formation regarding GDM. The integrated perspective supported practical and policy-relevant implications for improving maternal health education, healthcare delivery systems, and pregnancy outcomes.
Results
Search results
The systematic search conducted across the main databases yielded a total of 41,505 records for this review. Additionally, 17,500 records were retrieved from supplementary sources. The studies that were retrieved were uploaded into the Mendeley referencing software version 1.19.8 for the removal of duplicates. Following the removal of duplicates using both automated (Mendeley referencing software) and manual screening methods, 148 records remained for further evaluation. These records underwent title and abstract screening by EJ and EB against the predefined eligibility criteria. Subsequently, 94 records were excluded at this stage due to irrelevance to the review objectives, leaving 54 records for full-text assessment. Furthermore, reference list examination of eligible studies identified 6 additional records, whilst consultation with a librarian and other experts yielded 2 more articles, making 62 in total. During full-text screening, 12 articles were excluded for specific reasons: three were not published in English, and nine did not report variables of interest related to knowledge, awareness, or perception of GDM. Consequently, 50 studies met all inclusion criteria and were included in the final synthesis. This rigorous and transparent selection process ensured that only relevant, high-quality studies contributed to the review findings. Figure 1 presents the complete PRISMA flow diagram illustrating the identification, screening, eligibility assessment, and final inclusion of studies at each stage of the selection process. PRISMA flow chart.
Characteristics of the included studies
Extraction sheet for included studies.


Distribution of study designs.

Global distribution of the included studies.
Quality appraisal results of included studies
Appraisal of cross-sectional studies.

Appraisal of qualitative studies.

Appraisal of mixed-method studies.

All three qualitative studies scored 8 out of 10,37,56,58 indicating low risk of bias. The main limitations in these studies were related to researcher reflexivity and positionality (Q6 and Q7), which are essential considerations in qualitative research to ensure transparency and credibility. Without explicit reporting on how the researchers’ perspectives or prior experiences may have influenced data collection, analysis, and interpretation, the findings may be less fully contextualised. Both mixed-methods studies3,27 scored 5 out of 5, reflecting rigorous methodological quality and exemplary integration of qualitative and quantitative components. These studies demonstrated clear alignment between research questions, data collection methods, and analytical strategies, which enhances confidence in their findings.
Review findings
Knowledge and awareness levels about GDM among women
Across the included studies, knowledge and awareness of Gestational Diabetes Mellitus (GDM) were measured using structured questionnaires assessing understanding of the condition’s definition, risk factors, symptoms, diagnosis, management, and complications. Most studies calculated a total score by summing correct responses to multiple items, with score ranges varying across instruments (e.g., 0–8, 0–18, 0–19, or up to 0–88). Knowledge or awareness levels were then categorised using predefined cut-off points, most commonly as poor/low (<50% of the total score), moderate/fair (50–69%), and good/high (≥70%). Some studies also used scale-specific thresholds (e.g., ≤3 = poor, 4–5 = average, ≥6 = good on an 8-point scale). In addition to total scores, several studies reported mean scores and standard deviations to describe overall knowledge or awareness levels among participants.
Women’s knowledge and awareness of GDM were generally limited across the reviewed studies, with most demonstrating only a partial or superficial understanding of the condition. Numerous investigations reported that many pregnant women and women of reproductive age possessed insufficient awareness of GDM, and only a small proportion demonstrated adequate knowledge.3,5,26,30,33,59 Even in contexts where overall awareness appeared moderate, a substantial proportion of participants still lacked detailed or accurate knowledge.18,19,38,42 This broad pattern of limited understanding suggests that many women encounter gaps in health information related to GDM during pregnancy. Across studies, considerable variability in GDM knowledge levels was observed, with some groups showing basic awareness while others demonstrated substantial knowledge deficits.17,21,22,31,43,60 Despite this variability, most studies consistently identified similar knowledge gaps, particularly regarding risk factors, screening procedures, diagnostic criteria, and long-term health implications. Women commonly struggled to identify major risk factors such as obesity, advanced maternal age, and family history of diabetes.40,46,53 Many were also unfamiliar with recommended screening schedules, diagnostic processes, and key aspects of GDM management.32,39,47 A particularly notable finding was the limited understanding of long-term consequences, as many women were unaware that GDM increases the risk of type 2 diabetes mellitus later in life and heightens the likelihood of metabolic complications in offspring.37,45,53
The findings further indicated that healthcare facilities and healthcare providers constituted the primary sources of information about GDM. Women frequently relied on antenatal clinics, hospital visits, and consultations with nurses, midwives, and physicians to obtain information about the condition.23,27,46 Structured educational interventions delivered within these settings were consistently associated with higher knowledge levels compared to routine counselling alone, suggesting that active, intentional teaching strategies are more effective than passive information-sharing during consultations.5,16,30 Despite the central role of healthcare settings, significant barriers reduced the accessibility and effectiveness of GDM-related health information. Several studies reported limited availability of structured educational programmes, inconsistent delivery of antenatal health education, and limited use of community-based health promotion or public awareness campaigns.42,56 As a result, many women relied on informal information sources, such as family members, peers, or internet searches, sources that often provided incomplete, conflicting, or inaccurate information. 37 Women with limited literacy, language barriers, or restricted access to healthcare services faced additional challenges in obtaining reliable information, leading to further disparities in knowledge.5,53
Studies also highlighted instances in which healthcare providers themselves had insufficient knowledge about GDM diagnosis, management, and long-term follow-up. This limitation may have reduced the accuracy and depth of information shared with patients during antenatal visits.29,56 In many settings, antenatal education sessions prioritised topics such as labour preparation, nutrition, or infant care, leaving limited time for detailed discussions on GDM, particularly where routine screening was not consistently practised.30,56
Perceptions and attitudes towards GDM
The studies included in this review revealed diverse and often contrasting perceptions and attitudes toward GDM. A common finding was that many women perceived GDM as a temporary condition that resolved after childbirth, which contributed to reduced concern about its long-term implications for their own health and that of their children.37,58 This perception was particularly evident among women who experienced few symptoms or whose condition was managed through dietary changes alone. For some, GDM was not seen as a serious medical condition, especially in comparison with pre-existing diabetes mellitus, leading to limited motivation to adopt lifestyle modifications or engage in postpartum follow-up care. 37 Misconceptions regarding the causes of GDM frequently shaped negative emotional responses. Several studies reported that women attributed their diagnosis to personal shortcomings, such as poor diet choices or inadequate self-care, resulting in feelings of guilt, self-blame, and shame. 58 These emotional reactions influenced their readiness to accept the diagnosis and participate in recommended management strategies.
Despite these challenges, other studies highlighted more positive and proactive attitudes toward GDM. Some women expressed acceptance of their diagnosis and demonstrated willingness to engage with recommended screening, treatment, and lifestyle modifications.23,35,54 Women who understood the potential risks of uncontrolled GDM for foetal health showed stronger motivation to adhere to dietary recommendations, physical activity, glucose monitoring, and follow-up appointments.20,52 Supportive interactions with healthcare providers played a significant role in fostering such positive attitudes, as women valued clear communication, reassurance, and guidance from clinicians. 51 Additionally, women with prior exposure to diabetes through family experience tended to respond more confidently to the diagnosis and demonstrated greater acceptance of GDM management requirements. 27 However, practical challenges such as household responsibilities, financial limitations, and insufficient family support commonly interfered with adherence to recommended behaviours. 39 Women’s perceptions of susceptibility also shaped their behaviour: those who believed they were at low risk for complications were less likely to engage in preventive actions. 35
Social and cultural contexts further influenced women’s attitudes and practices. Cultural norms around food, family expectations, and limited autonomy in decision-making sometimes restricted women’s ability to prioritise their health needs.56,58 Emotional responses to diagnosis also played a critical role. Many women experienced anxiety, fear, or distress, particularly regarding potential harm to the baby and the possibility of childbirth complications, which, in some cases, hindered their capacity to engage effectively in self-management. 37
Discussion
Knowledge and awareness of GDM among women
The findings of this review show that women’s knowledge and awareness of gestational diabetes mellitus (GDM) remain inadequate across different settings and populations. Many women demonstrated only basic awareness of GDM and had limited understanding of its causes, risk factors, screening procedures, management strategies, and long-term consequences.3,5,26,30,33,59 Although some studies reported moderate awareness levels, detailed and functional knowledge required for effective prevention and self-management was often lacking.18,19,38,42 These findings suggest that existing antenatal education approaches may increase awareness without necessarily improving women’s understanding of the condition in ways that support informed decision-making and sustained behavioural change.
A consistent finding across studies was the variability in women’s understanding of GDM. Knowledge gaps were commonly reported in relation to risk factors, screening schedules, diagnostic criteria, postpartum follow-up, and disease management.17,21,22,31,43,60 Women with prior exposure to diabetes, regular antenatal attendance, or positive interactions with healthcare providers generally demonstrated better understanding than those with limited healthcare access or lower health literacy.4,64 However, misconceptions remained common. Some women believed that GDM was caused entirely by poor diet or personal negligence, leading to confusion, guilt, and self-blame.58,65 These misconceptions indicate the need for clearer and culturally appropriate public health messages that present GDM as a complex pregnancy-related metabolic condition rather than a personal failure.
Limited awareness of the long-term implications of GDM was also evident across the reviewed studies. Many women were unaware that GDM increases the future risk of type 2 diabetes mellitus and other cardiometabolic complications for both mothers and their children.37,45,53 This poor understanding may contribute to low rates of postpartum screening and weak adherence to long-term preventive behaviours reported in previous studies.4,64 The findings therefore suggest that knowledge alone may not be sufficient to improve outcomes. Women also require supportive environments, practical guidance, and continuous follow-up to translate knowledge into sustained lifestyle modification and long-term risk reduction.4,64
Healthcare providers and antenatal clinics were consistently identified as the main sources of GDM information.5,16,30 Studies showed that structured and targeted educational interventions were more effective than routine counselling in improving women’s understanding of GDM.5,16 However, limited consultation time, competing clinical priorities, and inconsistent provider knowledge often reduced the quality and depth of information delivered during antenatal care visits.29,56 These limitations are important because effective communication and supportive patient–provider relationships have been associated with improved engagement in screening, treatment adherence, and postpartum follow-up.51,66 Strengthening provider training and integrating structured GDM education into routine antenatal care may therefore improve women’s understanding and engagement with care.
The review further showed that many women relied on informal sources of information, including family members, peers, and online platforms.37,56 These sources often provided incomplete or inaccurate information, especially in settings where access to formal health education was limited. Low literacy levels, language barriers, and socioeconomic challenges further influenced women’s ability to access and understand accurate health information.5,53 These findings highlight the importance of community-based and culturally sensitive educational strategies that extend beyond health facilities. Community health workers, peer support systems, and digital health interventions may help improve access to reliable GDM information, particularly in underserved settings.
Perceptions and attitudes towards GDM
The review showed that women’s perceptions and attitudes toward GDM were shaped by personal experiences, emotional responses, cultural beliefs, and social circumstances. A common perception across studies was that GDM is a temporary condition that resolves after childbirth.7,37,58 Women who experienced mild symptoms or managed the condition through dietary changes alone were particularly likely to minimise its seriousness. As a result, some women viewed GDM as less severe than pre-existing diabetes and showed lower motivation for postpartum follow-up and long-term lifestyle modification.37,67 These findings indicate that women may underestimate the long-term health implications of GDM for themselves and their children.
Emotional responses to GDM diagnosis were also prominent in the reviewed studies. Women frequently reported feelings of guilt, anxiety, fear, shame, and self-blame, especially when they believed that their condition resulted from poor lifestyle choices or inadequate self-care.58,68 Stigma associated with the diagnosis sometimes further affected women’s confidence and willingness to engage fully with management recommendations. 68 These findings demonstrate that GDM is not only a medical condition but also a psychological and social experience that can influence women’s attitudes toward care and self-management.
Despite these challenges, several studies reported positive attitudes toward GDM management. Women who understood the potential risks of uncontrolled GDM for maternal and foetal health were more likely to adopt recommended dietary practices, engage in physical activity, monitor blood glucose levels, and follow medical advice.20,23,35,52,54 Supportive relationships with healthcare providers also encouraged positive engagement with treatment and follow-up care.51,69 In addition, prior family exposure to diabetes appeared to improve women’s acceptance of the diagnosis and their understanding of disease management. 27 These findings suggest that supportive counselling, peer support, and family involvement may strengthen women’s motivation and confidence in managing GDM.
However, the review also identified a persistent gap between women’s attitudes and their ability to implement recommended self-care practices. Even when women expressed willingness to follow medical advice, structural and social barriers often limited adherence to dietary recommendations, physical activity, glucose monitoring, and follow-up care.3,39,52,61 Financial difficulties, household responsibilities, limited social support, and restricted access to healthy foods commonly interfered with self-management efforts. Cultural norms and family expectations also influenced women’s ability to prioritise their health and maintain lifestyle changes.56,58,70 These findings indicate that improving GDM outcomes requires more than education alone. Effective interventions should address the broader social and structural conditions that shape women’s health behaviours. Healthcare systems also played an important role in shaping women’s perceptions and experiences of GDM. Although healthcare providers were major sources of information and support, inconsistent counselling, limited consultation time, and inadequate provider knowledge sometimes reduced opportunities for comprehensive patient education.64,69 Studies consistently showed that structured and patient-centred educational interventions improved women’s understanding, confidence, and engagement with GDM care. 66 These findings highlight the importance of strengthening antenatal education, improving provider communication skills, and integrating culturally appropriate counselling approaches into routine maternal healthcare services.
Implications for policy, practice, and GDM management
The findings of this review demonstrate the need to strengthen educational frameworks and health literacy initiatives targeting GDM across diverse populations. At the policy level, ministries of health and public health authorities must formally recognise GDM education as a core component of antenatal care rather than an optional supplement. National screening programmes should mandate structured patient education at diagnosis, and incorporate clear information about risk factors, long-term maternal and child health consequences, and preventive strategies. Furthermore, policies must ensure adequate consultation time for healthcare providers to deliver meaningful patient education rather than brief, information-dense encounters that overwhelm women. Investment in culturally adapted, multilingual educational resources is essential to address disparities in health literacy and reach socioeconomically disadvantaged populations. Additionally, provider training programmes for obstetricians, midwives, nurses, and dietitians should incorporate communication skills, behaviour change counselling, and health literacy principles to enhance the quality of patient-provider interactions. Accreditation standards for maternal health services should include provisions for patient education quality, ensuring that all pregnant women receive consistent, evidence-based information about GDM regardless of geographical location or healthcare setting.
Moreover, healthcare systems must establish multi-channel health promotion strategies that extend beyond clinical consultations to reach women during preconception and throughout pregnancy. Public health campaigns utilising mass media, social media platforms, and community outreach can raise population-level awareness about GDM and its implications. Furthermore, antenatal education programmes should dedicate substantial time to GDM prevention and management rather than focusing exclusively on labour and newborn care. Healthcare facilities should develop peer support networks to connect women with a lived experience of GDM to newly diagnosed patients, to facilitate knowledge sharing and emotional support. Family-centred education approaches that involve partners and relatives can enhance home-based support for dietary modifications and blood glucose monitoring. Additionally, healthcare systems must address structural barriers to care access, including transportation challenges, appointment scheduling flexibility, and affordability of healthy foods and monitoring supplies. Nevertheless, GDM outcomes require integrated approaches that address individual knowledge deficits alongside interpersonal, community, and systemic determinants of health behaviour. Healthcare providers must move beyond information transmission towards patient-centred counselling that acknowledges women’s life circumstances, cultural beliefs, and practical constraints. Postpartum follow-up systems need strengthening through reminder systems, flexible appointment scheduling, and integration of diabetes screening into routine childcare visits. Furthermore, healthcare organisations should implement continuous quality improvement processes that monitor patient education delivery, assess knowledge retention, and evaluate self-management outcomes. Educational interventions must be rigorously evaluated using standardised measures to identify effective strategies for diverse populations. Ultimately, enhanced knowledge and appropriate perception of GDM will facilitate earlier diagnosis, improved glycaemic control, and greater participation in preventive initiatives.
Limitations of this review
This review presents some limitations that may influence the interpretation and generalisability of its findings. The predominant use of cross-sectional study designs among the included studies restricts the ability to draw causal inferences about the relationships between knowledge, awareness, perceptions, and health outcomes in GDM. Whilst the inclusion of all studies regardless of quality rating enhanced comprehensiveness, it introduced the risk that findings from studies with moderate bias may affect the reliability of the synthesis. Some included studies exhibited methodological limitations, particularly in identifying and managing confounding variables such as maternal age, parity, and socioeconomic status. All eligible studies were retained to achieve thorough evidence coverage across different populations and geographical contexts. However, no subgroup or sensitivity analyses were conducted to account for heterogeneity across study populations. This might have contributed to increased heterogeneity in the outcomes. Additionally, qualitative studies consistently lacked reflexivity reporting, potentially reducing the transparency and trustworthiness of interpretations. These shortcomings may affect the internal validity of findings and should be considered when interpreting the overall results of this review. Moreover, the review focused exclusively on studies published in English, which may have resulted in language bias and the exclusion of relevant research conducted in non-English-speaking regions, thereby limiting cultural diversity and global applicability. The geographical concentration of studies in Saudi Arabia, India, and Nigeria creates a regional skew that may not reflect the realities of GDM education in other healthcare systems, especially in underrepresented regions. Furthermore, variations in how key constructs such as ‘knowledge’, ‘awareness’, and ‘perception’ were defined and measured across studies posed challenges for cross-study comparisons. Different assessment tools, scoring systems, and cut-off points for categorising knowledge levels hindered the direct comparability of findings. These methodological inconsistencies highlight the need for standardised measurement approaches in future research.
Recommendations for future research
Future research should adopt longitudinal and interventional study designs to assess the long-term impact of educational interventions on knowledge retention, health behaviours, and maternal-child outcomes following GDM diagnosis. There is a pressing need for culturally diverse and context-specific investigations, particularly in underrepresented regions such as sub-Saharan Africa, Southeast Asia, and Latin America, to capture the varied educational needs across different healthcare systems. Furthermore, studies should incorporate balanced perspectives by exploring healthcare providers’ knowledge gaps, communication challenges, and educational practices to provide a holistic understanding of GDM education delivery. The development and validation of standardised tools to measure knowledge, awareness, and perceptions across diverse populations would enhance comparability across studies and facilitate evidence synthesis. Moreover, interventional studies evaluating the effectiveness of multi-channel health promotion strategies, family-centred education approaches, and technology-enhanced learning platforms will be instrumental in identifying evidence-based practices for improving GDM awareness and management outcomes globally. Lastly, future studies should explore the long-term impacts of educational interventions across diverse cultural contexts.
Conclusion
The findings from this review show that knowledge and awareness of GDM remain inadequate globally. Most women had only a limited understanding of the condition, particularly its risk factors, screening procedures, and long-term health risks. Women’s perceptions and attitudes were shaped by cultural norms, emotional responses, and the quality of healthcare interactions. While some women demonstrated positive attitudes toward management, a gap between intention and actual self-care practices was common. The findings highlight the need for targeted educational interventions, culturally sensitive resources, and enhanced patient-provider engagement. These strategies could improve understanding, encourage positive attitudes, and support better health outcomes. However, the predominance of cross-sectional studies and geographical concentration limits generalisability. Future research should employ longitudinal designs and standardised measures across diverse populations to strengthen the evidence base.
Supplemental material
Supplemental material - Knowledge, awareness, attitudes and perceptions on gestational diabetes among females: A systematic review
Supplemental material for Knowledge, awareness, attitudes and perceptions on gestational diabetes among females: A systematic review by Christiana Asiedu, PHD, MPhil, MPH, BEd., Daniel Kwabla Ahiagbede, MPhil, BSc, Eunice Johnson, MPH, BSc. M, Sarah Esi Bilson, MPhil, BSc. N, Grace Atitsogbey, BSc. N, Emmanuella Florence Odi Asiedu, BSc. N in Sage Open Medicine
Supplemental material
Supplemental material - Knowledge, awareness, attitudes and perceptions on gestational diabetes among females: A systematic review
Supplemental material for Knowledge, awareness, attitudes and perceptions on gestational diabetes among females: A systematic review by Christiana Asiedu, PHD, MPhil, MPH, BEd., Daniel Kwabla Ahiagbede, MPhil, BSc, Eunice Johnson, MPH, BSc. M, Sarah Esi Bilson, MPhil, BSc. N, Grace Atitsogbey, BSc. N, Emmanuella Florence Odi Asiedu, BSc. N in Sage Open Medicine
Supplemental material
Supplemental material - Knowledge, awareness, attitudes and perceptions on gestational diabetes among females: A systematic review
Supplemental material for Knowledge, awareness, attitudes and perceptions on gestational diabetes among females: A systematic review by Christiana Asiedu, PHD, MPhil, MPH, BEd., Daniel Kwabla Ahiagbede, MPhil, BSc, Eunice Johnson, MPH, BSc. M, Sarah Esi Bilson, MPhil, BSc. N, Grace Atitsogbey, BSc. N, Emmanuella Florence Odi Asiedu, BSc. N in Sage Open Medicine
Footnotes
Acknowledgements
The authors are most grateful to all research assistants.
Author contributions
CA and EFOA conceptualised the study and developed the review questions. CA, EFOA, DA, EJ and SEB contributed to the development of the methodology, review questions and writing of the manuscript. All authors reviewed, edited and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.