
Abstract
Objective
Our objective was to evaluate the occurrence of congenital anomalies in pregnant women who received at least one dose of COVID-19 vaccine from conception up to 11w and 6d in comparison to those vaccinated after 12 weeks of pregnancy or not vaccinated at all.
Methods
This study is a Registry-Based Cohort Study carried out in the cities of Yasuj and Hormozgan, Iran. Participants involved divided into three groups for analysis: unvaccinated individuals, vaccinated during the teratogenic window (defined as women who received at least one dose of COVID-19 vaccine from conception up to 11w and 6d) and participants who received the vaccine after the first 12 weeks of pregnancy, (categorized as women vaccinated outside the organogenesis period). The primary outcome was congenital anomalies, which were identified as the presence of at least one birth defect detected prenatally through ultrasound.
Results
Overall, most congenital anomalies were rare and occurred at very low frequencies across groups. Atrioventricular septal defects (AVSD) were observed more frequently in women vaccinated within the teratogenic window compared with unvaccinated women (SMD = 0.22). Cleft palate also occurred slightly more frequently in this group (SMD = 0.13). For all other anomalies, effect sizes were small (SMD < 0.15) and no clinically meaningful differences were observed.
Conclusion
This study provides preliminary descriptive evidence regarding the occurrence of congenital anomalies following COVID-19 vaccination during early pregnancy. Because of the low number of events and the exploratory nature of the analyses, no causal inference can be made.
Introduction
The coronavirus disease 2019 (COVID-19) outbreak started in December 2019 and rapidly turned into a pandemic affecting many people throughout the world. Up to February 2022, the number of patients with COVID-19 and the number of COVID-19-related deaths were more than 414 million and six million in the world and more than six million and 134,000 in Iran, respectively (behdasht.gov.ir). 1
Approximately 210 million pregnancies occur each year, indicating that pregnant people are not a marginal population. 2 SARS-CoV-2 infection in pregnancy is associated with several severe consequences, 3 highlighting the need for prevention measures against SARS-CoV-2 infection. The American College of Obstetricians and Gynecologists (ACOG) and the Society of Maternal and Fetal Medicine (SMFM), two leading obstetric care organizations, recommend that all pregnant women be vaccinated against COVID-19.4,5 Despite international recommendations, COVID-19 vaccine acceptance among pregnant people is much lower than that in the general population.6,7 The main reason for the low rate of COVID-19 vaccine uptake is safety concerns about COVID-19 vaccines regarding both mothers and babies, but these concerns are supported by only limited data. 8 On the other hand, during the early stage of the pandemic, pregnant individuals were frequently excluded from clinical trials of vaccines, 9 which led to knowledge gaps regarding the safety and effectiveness of COVID-19 vaccines.
An increasing number of following data have shown that the COVID-19 vaccination could effectively prevent severe COVID-19 in pregnant women. Regarding the adverse events of COVID-19 during pregnancy as well as the efficacy and safety of COVID-19 vaccination during pregnancy, the WHO recommends the use of several COVID-19 vaccines in pregnant women. 9 As of December 30, 2022 Iranian health government on Covid-19 vaccination while pregnant recommended for some or all. However, COVID-19 vaccination strategies for pregnant women vary from country to country. For example, China does not recommend vaccination against COVID-19, while Israel and Europe encourage pregnant women to be vaccinated.10–12
Evidence supports the safety of COVID-19 vaccinations during pregnancy, particularly concerning perinatal outcomes like stillbirths, and early pregnancy events such as miscarriages.13,14 Nonetheless, data is extremely limited regarding the potential link between COVID-19 vaccinations or SARS-CoV-2 infections in early pregnancy and congenital anomalies.15–20 However, most conclusions are limited by small sample sizes, restricted generalizability or unbalanced confounding factors. 21
Several studies have explored neonatal effects following maternal COVID-19 vaccination, including the occurrence of congenital defects. However, there is a scarcity of research focusing on the potential occurrence of congenital defects when vaccines are administered during the first trimester - a critical period due to the increased risk of teratogenic effects.18,22 Evidence supports the safety of COVID-19 vaccinations during pregnancy, particularly concerning perinatal outcomes like stillbirths, and early pregnancy events such as miscarriages.13,14 Nonetheless, data is extremely limited regarding the potential link between COVID-19 vaccinations or SARS-CoV-2 infections in early pregnancy and congenital anomalies.15–20 In contrast, certain viral infections during early pregnancy, such as rubella and Zika virus, are established causes of specific congenital anomaly syndromes.23,24 Additionally, the risk of anomalies may be influenced by fevers resulting from infections or by medications used to treat these infections. 23
Further research is needed to improve the existing evidence base. Due to the limited high-quality data concerning the risk of congenital anomalies associated with COVID-19 vaccine, our objective was to evaluate the risk of congenital anomalies in pregnant women who received at least one dose of the COVID-19 vaccine from conception up to 11 weeks and 6 days, in comparison to those vaccinated after 12 weeks of pregnancy or not vaccinated at all.
Methods
Design and data collection
This study was conducted as an observational cohort analysis nested within the Iranian electronic health record system (SIB), which captures routine prenatal care data for the majority of the population in the study regions. It was carried out in the cities of Yasuj and Hormozgan, Iran, over the period from 2022-2023. The research received ethical approval from the Ethics Committee of Yasuj and Hormozgan University of Medical Sciences, Iran, under the codes IR.YUMS.REC.1401.061 and IR.HUMS.REC.1402.018. Written informed consent was obtained from all participants, who were also advised that they had the option to withdraw from the study at any time. Prior to participation, the objectives of the study were clearly explained to the participants, and assurances regarding the confidentiality of their responses were provided, followed by the acquisition of written informed consent.
Briefly, the study involved all pregnant women who referred to urban health centers in Yasuj and Bandar Abbas provinces, Iran. They had electronic health records in SIB using their national identification numbers. The SIB network is part of a larger prospective population-based cohort study that includes demographic, administrative and health data for more than 88% of the Iranian population, approximately 72 million individuals. 25 These women were then contacted via telephone and invited to visit a healthcare center for the purpose of data collection.
Data collection was performed through a structured questionnaire. It is important to mention that specific data concerning sonographic scan anomalies and other necessary details were retrieved from the SIB system. Whenever additional information was required, patients were consulted directly. Congenital anomalies were ascertained based on prenatal ultrasound findings recorded in the SIB system, as described in the following paragraph. Participant self-report was used only to supplement incomplete registry data and not for primary outcome determination. All questionnaires were filled out by professionals who had received appropriate training.
Regarding participant inclusion, the criteria specified were as follows: being pregnant with a single fetus, being between the ages of 18 and 35, expressing a willingness to engage in the study, and having undergone an anomaly ultrasound scan between 18 and 20 weeks of gestation. The exclusion criteria were any history of preterm birth, previous births of infants with abnormalities, intrauterine growth restriction (IUGR), undergoing in vitro fertilization (IVF), or possessing a familial history of genetic disorders in either the participant, their spouse, or immediate family members.
Description of study
Participants were divided into three groups for analysis: 1. Unvaccinated individuals 2. Vaccinated during the teratogenic window, defined as women who received at least one dose of a COVID-19 vaccine from conception up to 11 weeks and 6 days. This period is considered critical as it may pose a risk of teratogenic effects and corresponds to what is termed the “highly sensitive period of action of teratogens,” which is crucial for studying congenital malformations.
26
3. Participants who received the vaccine after the first 12 weeks of pregnancy were categorized as having been vaccinated outside the organogenesis period. Exposure during this later stage is not deemed etiologically significant for the investigation of congenital malformations.
Outcomes
The primary outcome included congenital anomalies, which were identified as structural abnormalities detected during routine prenatal anomaly scans performed according to national clinical guidelines. These scans are the standard screening tool for fetal anomaly detection in Iran and are routinely conducted irrespective of maternal vaccination status.
The outcomes in this study reflect anomalies detected during prenatal screening rather than clinically confirmed diagnoses. Systematic postnatal confirmation using specialized imaging or infant medical records was not feasible within the scope of this study. Therefore, the reported outcomes represent ultrasound-detected anomalies as observed in real-world clinical practice. The observed anomalies were categorized into genetic, major, or minor types, following the classification system established by EUROCAT. 27 Anomalies with a genetic basis were grouped separately as per the EUROCAT guidelines. The International Classification of Disease 10th revision (ICD-10) was employed to code each specific congenital anomaly. 28
Additionally, we gathered the following data: 1. Demographic data: age, body mass index (BMI), education, occupation, and planning for pregnancy. Moreover, we considered Consanguineous marriages have been described as an important factor in increasing congenital anomalies. A consanguineous marriage can be characterized by the degree of relatedness between the spouses: first cousins, double first cousins, half first cousins, first cousins once removed, second cousins, second cousins once removed and third cousins. Estimated consanguinity ratios in different parts of Iran ranged from 30 to 85%.
29
Because of high consanguinity rates within the Muslim population, the incidence of congenital malformation in Islamic countries is between 10 to 45%
30
2. Pregnancy-related information: gravid, parity, history of abortion, intake of folic acid, history of infertility, severe vomiting during pregnancy, any previous abortion history, any occurrences of bleeding during pregnancy, preterm pre-labor rapture of membrane (PPROM), and the gestational age. The gestational age was determined based on the embryo’s crown-rump length (CRL) measured during the first trimester ultrasound. Additional details collected included the fetus’s gender, any systemic diseases of the mother, and any abnormal laboratory results from the first trimester of pregnancy. 3. Pre-pregnancy history: history of low birth weight (LBW), intervals between pregnancies under three years, fetal anomalies history, and history of neural tube defects (NTD). 4. COVID-19-related information: COVID-19 infection in teratogenic window in mother, and details regarding the vaccination received (timing and type). Information on COVID-19 vaccination was obtained from electronic health records. Vaccine products were analyzed as a grouped exposure due to ethical and regulatory constraints, and individual vaccine brand names were not disclosed (A: Inactivated whole virus: Inactivated whole virus: Viral vectored: Viral vector: Inactivated whole virus). Any related information is available from the authors (SA. T) on direct request. This classification allows readers to better understand potential differences related to vaccine platform while respecting the ethical constraints mentioned. No mRNA vaccines were administered to any participant in this cohort.
Briefly, data were collected using a structured questionnaire specifically designed for this study. The instrument was developed based on standard perinatal research variables and EUROCAT guidelines for congenital anomaly classification (Supplemental file). It was pilot-tested on 25 participants (≈1.8% of the total sample), and necessary revisions were made. Because the questionnaire mainly collects objective demographic, medical history, and checklist-based anomaly data (with primary outcome information extracted from the SIB registry), formal psychometric validation was not conducted. This approach is consistent with many registry-based and reproductive health studies.
Statistical analysis
This study employed a census sampling method of all eligible pregnant women registered in the SIB system in the selected provinces. Therefore, no formal a priori sample size calculation was performed. The final analyzed sample included 1,352 participants, which provided sufficient numbers for descriptive comparisons and standardized mean difference analyses. However, due to the rarity of individual congenital anomalies, the statistical power for detecting small differences in specific anomaly subtypes remained limited.
Statistical analysis was performed using descriptive statistics, including frequency, percentage, and mean ± standard deviation. Standardized mean differences (SMD) were calculated for all baseline characteristics, pregnancy-related variables, pre-pregnancy history, and COVID-19-related variables to quantify the magnitude of imbalance between study groups independent of sample size. SMD values ≥0.1 were considered small, ≥0.2 moderate, and ≥0.3 large imbalance.
Hypothesis testing using chi-square tests for categorical variables and one-way ANOVA for continuous variables (with Bonferroni post hoc analysis where appropriate) was performed only for study outcomes of interest. The Kolmogorov–Smirnov test was used to assess normality of continuous variables. A two-sided p-value <0.05 was considered statistically significant for outcome analyses. All analyses were carried out using the Statistical Package for the Social Sciences (SPSS, version 21; SPSS, Chicago, IL). No missing data were present, and therefore no imputation methods were necessary. This study adheres to the STROBE guidelines for reporting observational studies.
Results
Baseline characteristics of participants
A total of 1,352 pregnant women participated in the study, including 303 unvaccinated, 262 vaccinated inside the teratogenic window, and 787 vaccinated outside the teratogenic window. None of the participants received mRNA vaccines (Figure 1). CONSORT flow diagram of study.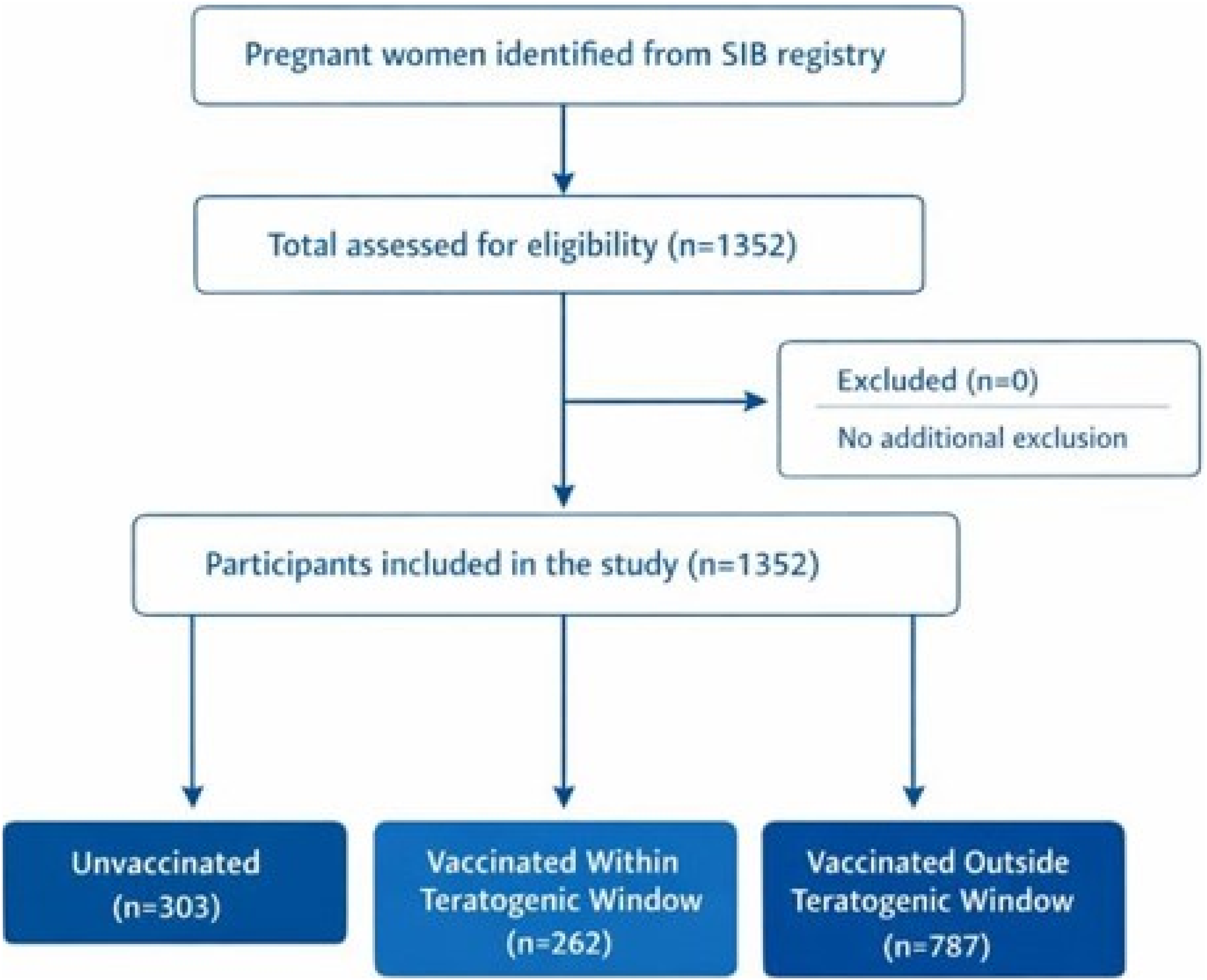
Demographic and pregnancy characteristics by vaccination group, Yasuj and Hormozgan, Iran, 2022–2023.
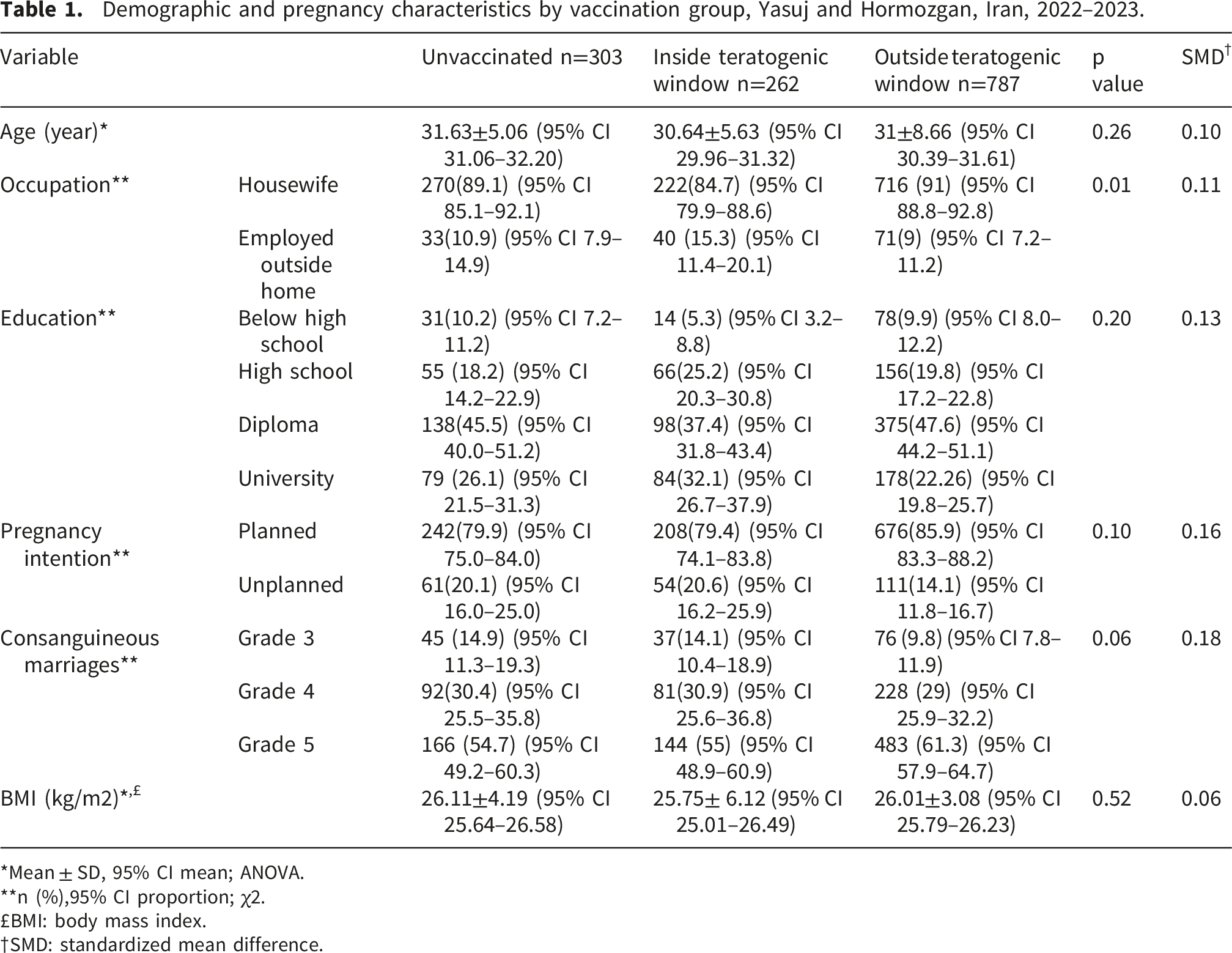
*Mean ± SD, 95% CI mean; ANOVA.
**n (%),95% CI proportion; χ2.
£BMI: body mass index.
†SMD: standardized mean difference.
Pregnancy characteristics
Pregnancy characteristics of patients by vaccination group, Yasuj and Hormozgan, Iran, 2022–2023.
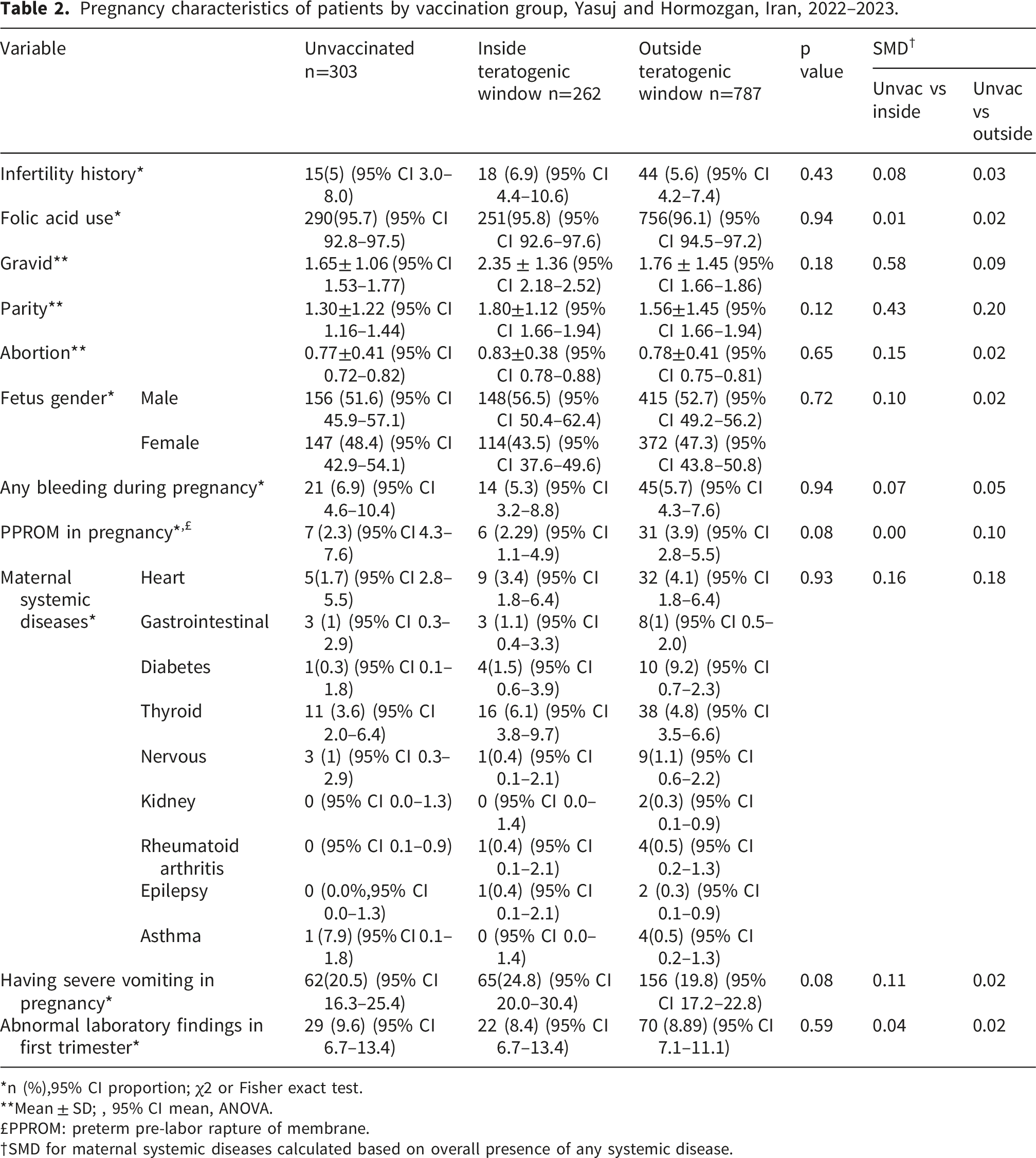
*n (%),95% CI proportion; χ2 or Fisher exact test.
**Mean ± SD; , 95% CI mean, ANOVA.
£PPROM: preterm pre-labor rapture of membrane.
†SMD for maternal systemic diseases calculated based on overall presence of any systemic disease.
Pre-pregnancy history
Pre-pregnancy history characteristics by vaccination group, Yasuj and Hormozgan, Iran, 2022–2023.
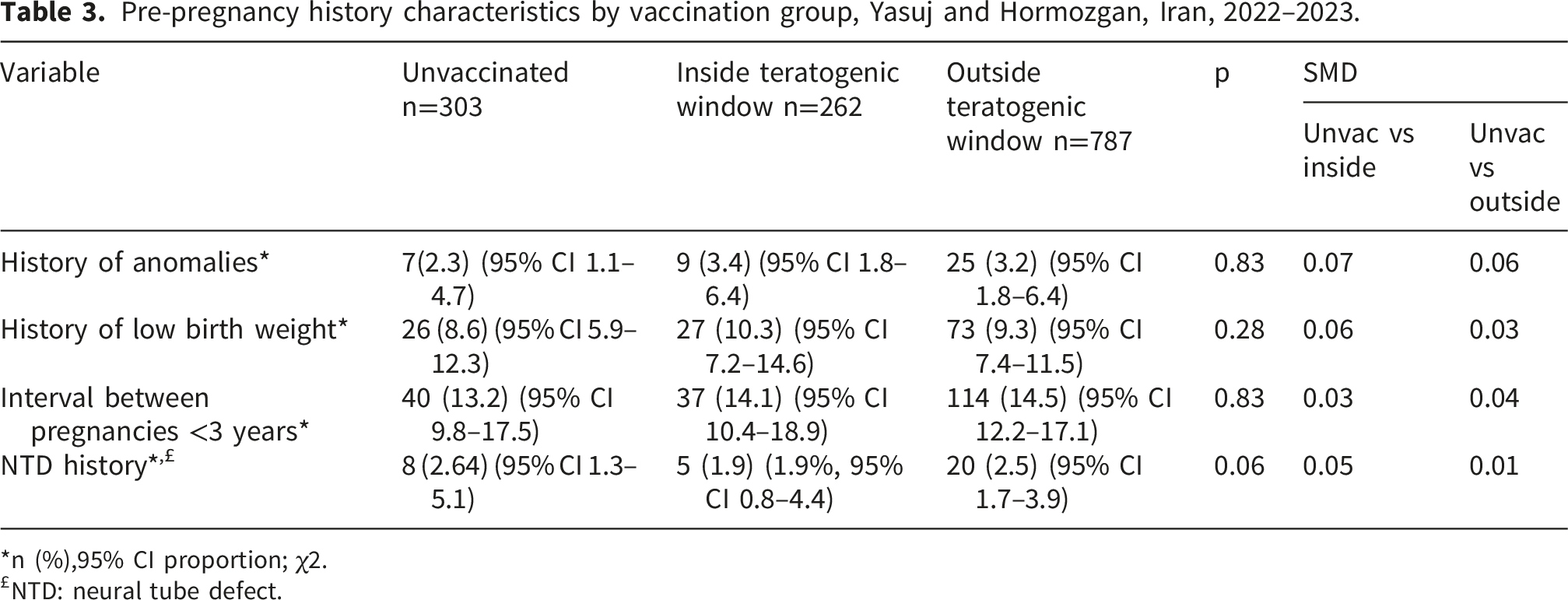
*n (%),95% CI proportion; χ2.
£NTD: neural tube defect.
COVID-19-related information
Information related to COVID-19 of patients by vaccination group, Yasuj and Hormozgan, Iran, 2022–2023.
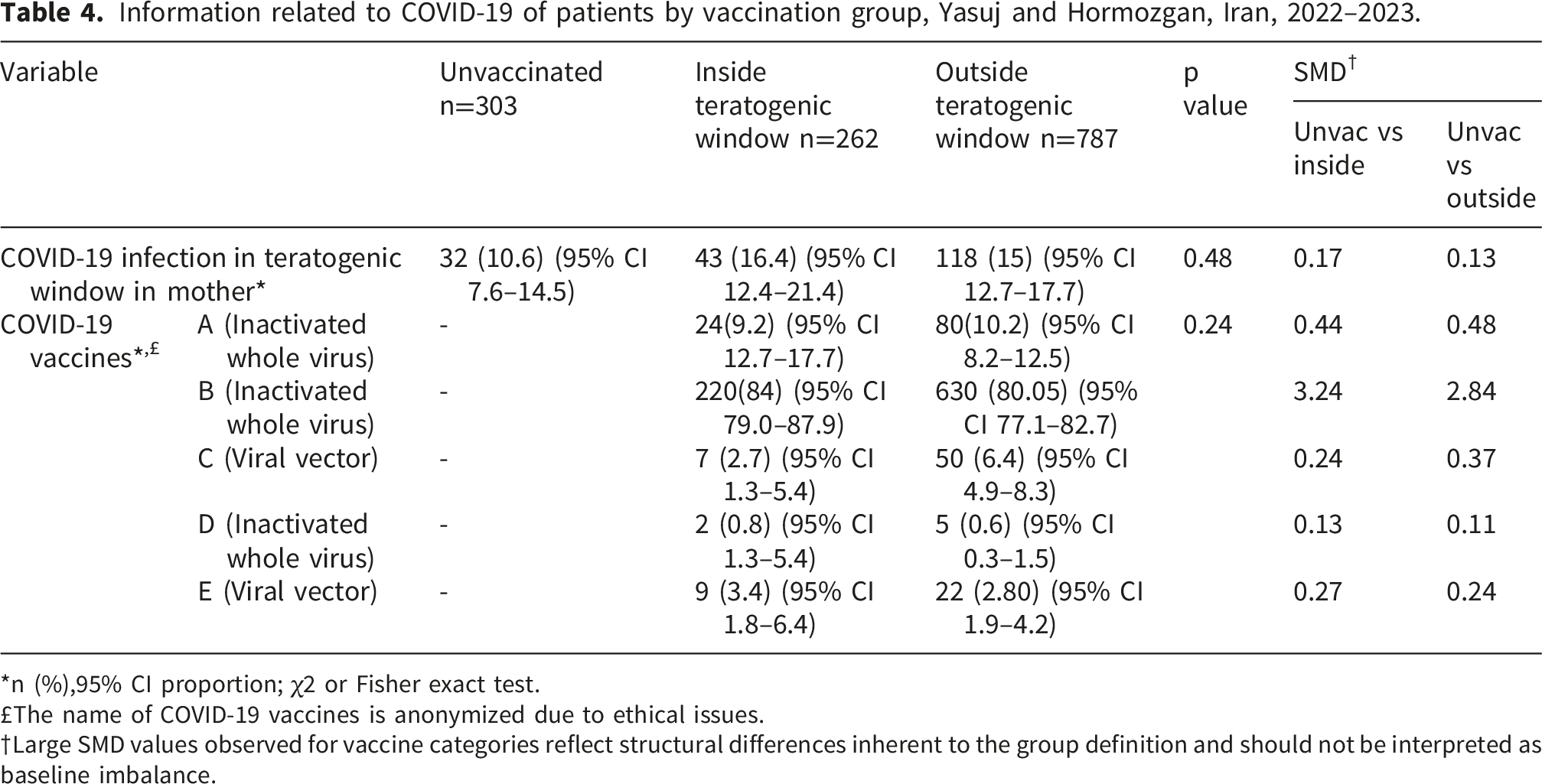
*n (%),95% CI proportion; χ2 or Fisher exact test.
£The name of COVID-19 vaccines is anonymized due to ethical issues.
†Large SMD values observed for vaccine categories reflect structural differences inherent to the group definition and should not be interpreted as baseline imbalance.
Congenital malformations
Congenital malformations in sonography scans of patients by vaccination group, Yasuj and Hormozgan, Iran, 2022–2023.
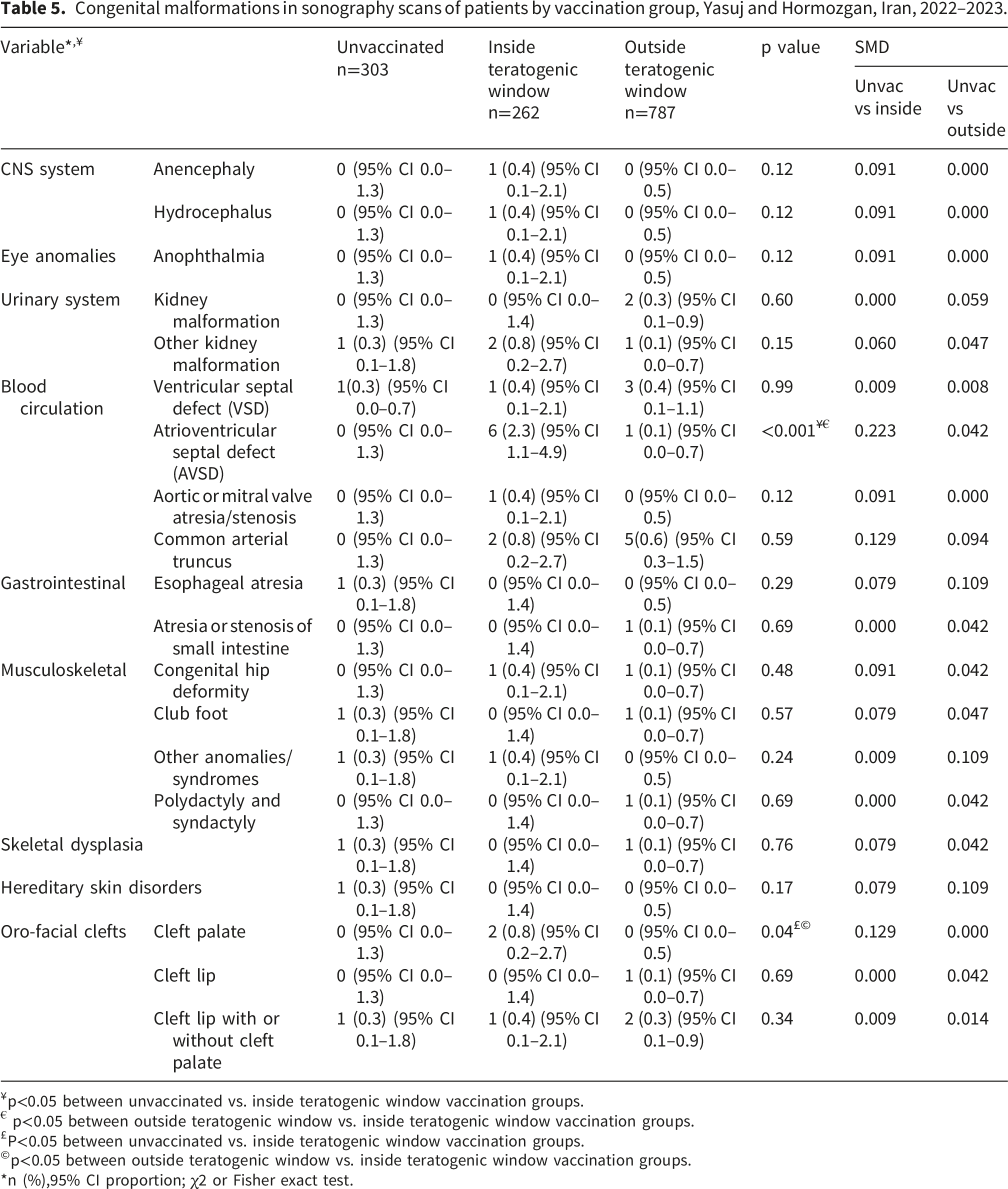
¥p<0.05 between unvaccinated vs. inside teratogenic window vaccination groups.
€ p<0.05 between outside teratogenic window vs. inside teratogenic window vaccination groups.
£P<0.05 between unvaccinated vs. inside teratogenic window vaccination groups.
©p<0.05 between outside teratogenic window vs. inside teratogenic window vaccination groups.
*n (%),95% CI proportion; χ2 or Fisher exact test.
Discussion
Many countries commonly advise that women who are pregnant should be vaccinated against COVID-19 during their pregnancy.31–33Therefore, research assessing whether these vaccines could influence embryonic development is crucial. We evaluated known maternal factors and exposures that could affect fetal development. In this study of 1,352 pregnant women, a slightly higher occurrence was observed of atrioventricular septal defects (AVSD) and cleft palate in women vaccinated inside the teratogenic window. However, the absolute number of cases was small. All other congenital anomalies were rare and occurred at low frequencies across groups.
In contrast to earlier studies relying on passive surveillance systems, recent large comparative cohort investigations have provided more robust evidence regarding the safety of COVID-19 vaccination in pregnancy. A multisite observational cohort study using data from the U.S. Vaccine Safety Datalink, including 42 156 pregnancies with first-trimester mRNA COVID-19 vaccine exposure, found that the adjusted prevalence ratio for selected major structural birth defects among live-born infants was 1.02 (95% CI, 0.78–1.33), indicating no increased risk compared with those unvaccinated in the first trimester. 34 Similarly, a population-based cohort and sibling-matched analysis reported no association between first-trimester mRNA COVID-19 vaccination and major congenital anomalies overall or by organ system, with results consistent across various subgroup and sensitivity analyses. 35 While these comparative studies suggest that early pregnancy vaccination is not linked to a broad increase in major structural anomalies, our descriptive analysis found slightly higher frequencies of atrioventricular septal defects (AVSD) and cleft palate in women vaccinated inside the teratogenic window. Given the limited event counts and descriptive design, causal inference cannot be drawn, but these observations underscore the importance of continued surveillance and pooled data analyses to investigate rare congenital outcomes. From a biological perspective, potential mechanisms linking maternal vaccination during pregnancy to fetal developmental outcomes remain largely hypothetical and warrant cautious interpretation. Further research, including experimental and animal studies, is needed to elucidate whether immune-mediated pathways may play any role in fetal development following vaccination. To date, there is no direct evidence demonstrating that maternal inflammatory responses induced by COVID-19 vaccination adversely affect fetal development or increase the risk of congenital anomalies. However, previous studies have shown that maternal immunization with inactivated influenza vaccines during pregnancy may be associated with transient increases in inflammatory biomarkers.36,37 This has led to broader interest in the concept of maternal immune activation and its potential implications for fetal and neonatal development. Evidence from animal models and selected human studies suggests that maternal immune activation during pregnancy may be associated with long-term neurodevelopmental or neuropsychiatric outcomes in offspring,38–40 possibly mediated by pro-inflammatory cytokines affecting placental function or fetal brain development. 41 Nevertheless, current evidence remains limited, and the extent to which vaccination-induced immune responses resemble those triggered by infection is not well understood. Importantly, any potential effects may vary by timing of exposure during gestation. 42 These considerations should be viewed as hypothesis-generating and highlight the need for further well-designed studies rather than evidence of a causal relationship.
Although this registry-based study attempted to include all eligible pregnant women attending urban health centers in Yasuj and Bandar Abbas provinces, Iran, several limitations should be considered when interpreting the findings. First, the results should be interpreted within the context of the Iranian population and the predominant use of non-mRNA COVID-19 vaccines during the study period. Therefore, generalizability to populations with different ethnic backgrounds, healthcare systems, or predominant use of mRNA vaccines remains uncertain and requires confirmation in future studies.
Although the overall sample size was relatively large, the number of fetuses exposed to COVID-19 vaccination during the critical teratogenic window was limited, primarily because vaccination during the first trimester was uncommon due to prevailing recommendations to delay vaccination until after 12 weeks of gestation. Consequently, the number of congenital anomaly events within exposure groups was very small, substantially limiting statistical power to detect rare outcomes or small effect sizes. As this study utilized all available eligible registry cases, no formal sample size calculation was performed. Sparse outcome data also resulted in imprecise estimates with wide confidence intervals and precluded reliable multivariable adjustment using conventional regression approaches. Rare-event methods, including Firth or exact logistic regression, were considered; however, the presence of multiple zero-event cells and insufficient events-per-variable limited the stability and interpretability of adjusted models. Similarly, sensitivity analyses—including restriction to major EUROCAT anomalies, exclusion of multiple gestations, and complete-case analyses—yielded unstable and difficult-to-interpret estimates because of severe data sparsity. Therefore, the findings should be interpreted as preliminary descriptive and hypothesis-generating observations rather than definitive causal evidence. Future studies with larger sample sizes, higher event rates, and alternative designs such as case–control studies may provide more robust estimates for rare congenital outcomes.
Residual confounding also remains possible. Although some imbalance in gravidity and parity was observed between groups, the low number of outcome events prevented reliable confounder adjustment. Additionally, because multiple anomaly categories were evaluated, the possibility of type I error related to multiple comparisons cannot be excluded, and some statistically significant findings may have occurred by chance alone.
Outcome ascertainment represented another important limitation. Congenital anomalies were identified based on routine prenatal anomaly scans rather than postnatal clinical confirmation. Although prenatal ultrasound is the primary screening modality for fetal anomalies, its diagnostic sensitivity varies according to anomaly type and may be limited for conditions requiring specialized imaging, such as fetal echocardiography or advanced craniofacial assessment. Participants were not followed through delivery, and anomalies detected prenatally were not systematically confirmed using postnatal medical records. Consequently, some anomalies may have been misclassified, underdetected, or not confirmed after birth. Importantly, the aim of this study was not to estimate the true prevalence of congenital anomalies, but rather to compare the frequency of ultrasound-detected anomalies between vaccinated and unvaccinated pregnancies.
The study population was derived from women registered in the SIB system who could be contacted for supplementary data collection. Although this may limit complete population representativeness, internal comparisons between exposure groups are unlikely to have been materially biased. In addition, some mothers with prior SARS-CoV-2 infection may have been misclassified as uninfected because of the absence of documented RT-PCR confirmation. Genetic disorders, congenital infections, and anomalies associated with spontaneous abortion or medically indicated early pregnancy termination were also not fully captured because such conditions were not consistently documented in the registry and because spontaneous abortions occurring before routine anomaly screening were excluded from the study.
Additionally, the questionnaire underwent pilot testing but did not receive formal psychometric validation. Nevertheless, the risk of information bias was likely limited because the primary outcomes were obtained mainly from the SIB electronic registry rather than maternal self-report alone. Furthermore, vaccine-specific analyses could not be conducted because vaccine product information was grouped in accordance with ethical approval requirements. Consequently, the findings reflect the overall association between COVID-19 vaccination and prenatal anomaly scan findings rather than the effects of individual vaccine platforms.
Finally, this study did not evaluate neurodevelopmental outcomes that may emerge later in childhood, which would require substantially longer follow-up. Accordingly, despite generally reassuring preliminary findings, the results should be interpreted cautiously and confirmed through larger, methodologically robust studies with extended follow-up and postnatal outcome verification.
Conclusion
In conclusion, this registry-based study provides preliminary descriptive and hypothesis-generating evidence regarding ultrasound-detected congenital anomalies following COVID-19 vaccination during early pregnancy. Given the low number of events and the absence of adjusted analyses, causal interpretations cannot be made.
Supplemental material
Supplemental material - Association of COVID-19 vaccination before 12 weeks of gestation with ultrasound-detected congenital anomalies compared with later or no vaccination: A registry-based cohort study
Supplemental material for Association of COVID-19 vaccination before 12 weeks of gestation with ultrasound-detected congenital anomalies compared with later or no vaccination: A registry-based cohort study by Seyed-Abdolvahab Taghavi, Fatemeh Bazarganipour, Mohammad Moradi-Joo, Zahra Seyedi, Fatemeh Dabiri, Leila Bozorgian, Leila Manzori in Sage Open Medicine
Footnotes
Ethical considerations
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments. The research received ethical approval from the Ethics Committee of Yasuj and Hormozgan University of Medical Sciences, Iran, under the codes IR.YUMS.REC.1401.061 and IR.HUMS.REC.1402.018.
Consent to participate
Written informed consent was gained from all patients; all participants were informed that they could withdraw at any point during the study.
Author contributions
SAT, FB, ZS, LM, FD, LB and contributed to conception, design and drafting of the manuscript; LB, FD and SZ contributed to data collection; AM, SAT, FB and MM contributed to manuscript drafting. All authors approved the final version of the manuscript before submission. FB supervised the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research grant provided by Research Deputy of Yasuj University of Medical Sciences (YUMS) and Hormozgan University of Medical Sciences (HUMS), Iran. The role of the funding body was collection and analysis.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The primary data for this study are available from the authors (SA.T) on direct request.
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.