
Abstract
Objectives
The study aimed to assess obstetric care providers’ practices and associated factors towards birth companionship in public hospitals of South Gondar zone, North West Ethiopia, 2025.
Methods
An institution-based cross-sectional study was conducted from January 01 to February 28, 2025 among obstetric care providers working in 10 public hospitals of South Gondar zone, North West, Ethiopia. A census of 218 participants was conducted. Data were collected using a structured, self-administered questionnaire. The data were entered into EpiData version 4.6 and analyzed using Statistical Package for Social Science version 27. Descriptive statistics were computed, and both bivariate and multivariate logistic regression analysis were performed, and statistical significance was declared at P< 0.05. Ethical clearance was obtained and informed consent was secured from all the participants.
Results
A total of 211 respondents participated in the study, making the response rate 96.7%, of these the prevalence of birth companionship practice among obstetric care providers was 16.59% (95% CI, 11.6-21.6). Obstetric care providers who had received training on Compassionate and Respectful care, Respectful Maternity Care, Basic Emergency Obstetric and Newborn Care were 1.55 times (AOR: 1.55; 95%CI: 1.09- 2.21) more likely to practice companion presence during childbirth. Additionally, health professionals working in facilities equipped with privacy measures between delivery couches were 1.48 more likely to permit companion presence during childbirth (AOR1.95; 95%CI: 1.08-2.02).
Conclusion
Birth companionship remains poorly practiced among obstetric care providers in South Gondar zone public hospitals, pointing deep rooted gap between the existing policies and the implementation. Training on respectful maternity care and presence of privacy measures emerged as key factors shaping provider practice. Strengthening policy enforcement, embedding companionship with provider training programs and ensuring adequate privacy infrastructures in labor wards are essential steps forward to encourage of practice.
Keywords
Introduction
Childbirth is a profound and life-changing experience for women and their families, affecting them emotionally and physically. During this journey, every woman should receive high-quality, evidence-based care and compassionate support to ensure both her and her newborn’s wellbeing. 1 However, as childbirth becomes increasingly institutionalized and medicalized, continuous emotional and psychosocial support for women in labor has often been neglected. 2
Global maternal health strategies have historically focused on reducing maternal mortality and morbidity, mainly by expanding access to institutional delivery and skilled care. More recently, the emphasis has broadened to include the quality of maternity services, positive childbirth experiences, equitable care, and the preservation of women’s dignity and respect.3,4 Central to this shift is the recognition that women greatly value and benefit from the presence of a trusted person to support them throughout childbirth. 3 Furthermore, there is a tremendous need for companionship, empathy, and support for women during labor. These forms of support are reflected in key components of childbirth care, including emotional reinforcement, praise, reassurance, active listening, and continuous physical presence. 5
Respectful Maternity Care (RMC) is a globally recognized framework that upholds women’s rights during childbirth, encompassing principles such as self-determination, privacy, dignity, and compassionate support. One essential component of RMC is labor companionship, which is defined as continuous support provided to a woman during labor and childbirth by a partner, family member, friend, doula, or healthcare professional.6–8 It emerged as low-cost, effective strategy to improve women childbirth experience. 9 Obstetric care providers including midwives, nurses, and physicians involved in intrapartum care play a critical role in either enabling or restricting this practice. 10
Evidence from systematic reviews demonstrated that women supported by a companion are more likely to have vaginal deliveries and less likely to require obstetric interventions. Labor tends to be shorter and spontaneous; the need for pain medication decreases, and women are more likely to have newborns with improved immediate health outcomes.11–13 Beyond clinical benefits, birth companionship contributes to a more satisfactory childbirth experience, and a reduced risk of complications during childbirth and puerperium14,15 and bridges communication gaps between health workers and laboring women. 10 Given this evidence, the World Health Organization (WHO) recommends that that every woman in labor be allowed to have a chosen companion during labor and childbirth to provide continuous support and reassurance. 16 This low-cost yet highly effective strategy, has been incorporated into the policies of more than half of African countries, including Ethiopia as a standard component of maternity care. 17
The presence of a birth companion during labor is well-established and widely integrated into maternity care in many high-income countries. 18 However, despite policy commitment, the practice remains limited in low and middle income countries, where barriers such as overcrowding, lack of privacy, restrictive hospital policies, and infection concerns hinder implementation.19,20 For instance, a study in India found that while most healthcare providers understood the concept and benefits of birth companionship, institutional barriers prevented its adoption. 7 Similarly a study in Kenya showed that 67% of women were allowed continuous support during labor but only 29% were allowed continuous support during delivery; the reasons proposed by the health professionals were related to privacy concerns and other reasons mainly related to distrust of companions. 21 Consistent with these findings, midwives working at a tertiary hospital in Limpopo, South Africa, revealed that at that none of them encouraged the presence of a birth companion during labor and birth. 22 A similar pattern was also observed in Tanzania; among providers, only 26.1% and 10.0% reported allowing a labor companion and birth companion, respectively. 23
In Ethiopia, research examining the implementation of birth companionship from the perspective of healthcare professionals remains limited, even though a substantial body of literature has explored maternal preferences to be accompanied by a partner or family member during childbirth.24,25 The few studies conducted in Ethiopia, notably those from West Shewa zone and Addis Ababa consistently revels a low level of practice and acceptance of birth companionship within among obstetric care providers.26,27 However, these studies are geographically confined to central and western Ethiopia, leaving significant regional gap in the evidence base, therefore understanding the local context is essential as institutional culture, resource availability and provider attitude may differ substantially across regions.
Furthermore, RMC training has been increasingly promoted in Ethiopia as a means of improving provider attitude and practice towards women-centered care. Providers trained in RMC are expected to be more informed about and receptive to practices such as birth companionship. We therefore hypothesized that obstetric care providers who had received prior training in RMC would be more likely to practice and allow birth companionship compared to those without such training.
Therefore, this study aimed to assess obstetric care providers’ practices and associated factors towards birth companionship in public hospitals of South Gondar Zone, Northwest Ethiopia, in 2025. Filling this gap is essential to improve the maternal experience and support the integration of birth companionship into routine obstetric care in Ethiopia.
Methods
Study setting and period
The study was conducted from January 1–February 28, 2025 at public hospitals in the South Gondar Zone, Amhara regional state, Northwest, Ethiopia. South Gondar zone is one of the 11 zones in Amhara regional state, Ethiopia. Debre Tabor is the administrative town of the zone and is located about 669 km northwest of Addis Ababa, the capital city of Ethiopia, and 97 km South West of Bahir Dar, the capital city of the Amhara regional state and it has an elevation of 2706 m above sea level. Based on the 2021 Amhara regional state population estimation, this zone has a total population of 2,651,350, of which 1,320,659 are women, 536,368 are non-pregnant women aged 15–49 years, and 89,351 are the estimated number of pregnant women. 28 The zone includes 10 public hospitals, comprising nine primary hospitals and one comprehensive specialized hospital.
Study design and population
An institution-based cross-sectional study was conducted among obstetric care givers working at public hospitals in the South Gondar Zone, Northwest, Ethiopia, to assess their practice regarding companion presence during childbirth. This design was appropriate for evaluating current practice and associated factors at a single point in time.
The source population comprised health professionals giving obstetric care service in public hospitals of South Gondar zone. These included Midwives, General practitioners, Obstetricians and Integrated emergency surgical officers (IESO), who are directly involved in labor and delivery care, although the level of involvement may vary by professional role.
The total number of obstetric care givers working in public hospitals of south Gondar zone is 225, since the number of obstetric care givers is small and manageable, a census was used, therefore all of them were included in the study. Of the 225 obstetric care providers, 130 worked at Debre Tabor Comprehensive Specialized Hospital and 95 at primary hospitals. Seven providers were on leave during data collection (unavoidable absence), resulting in a final of 218 participants.
Eligibility criteria
• Inclusion Criteria- All obstetric care providers, including midwives, doctors and IESOs, who were currently providing or had previously provided delivery care in those health facilities and had at least six months of work experience in the labor and delivery unit were eligible to participate. • Exclusion Criteria- Obstetric care providers who were on leave (annual, maternity, sick or study leave) during the data collection period and had less than six months of experience working in the labor and delivery unit.
Variables of the study
Dependent variable
• Obstetric care givers practice regarding companion presence during childbirth.
Independent variables
• Socio-demographic factors: age, sex, marital status, religion, profession, level of education, and years of experience. • Institutional factors: type of health facility (HF), structural factors such as presence of screen/curtain, number of couches in the delivery room, and administration protocol of the HFs. • Individual factors: number of work hours per week, number of deliveries conducted per month, having training on Compassionate, Respectful and Caring (CRC), RMC and Basic Emergency Obstetric and Neonatal Care (BEmONC).
Operational definition
• The practice of birth companionship was considered “Practiced” if providers reported allowing companion presence for all or most mothers, from the second stage of labor until the mother was transferred to the postnatal room. “Always” indicates the provider allows a companion for all deliveries they attend, while “most of the time” refers to allowing a companion for more than half but not all of deliveries. The measure captured the provider’s routine practice across all deliveries attended during the study period, not just the most recent case, and was based on providers’ self-reported frequency. • BEmONC-trained: Participants were classified as having received training if they completed the standardized BEmONC training course including both theoretical and practical components, with competency assessed through post-training evaluation.
29
• CRC/RMC-trained: providers in previous studies are defined as those who have participated in formal Compassionate, Respectful, and Caring (CRC) or respectful maternity care training programs offered to health workers.
30
• The presence of screens or curtains between delivery couches was recorded as “yes” if at least one functional screen or curtain was present for privacy, and “no” if none was present. • The number of delivery couches in each facility was counted and categorized. • Restructuring of the health facility -Restructure the organization of the delivery room (e.g., availability of space and privacy measures), as the physical structure of maternity wards, particularly overcrowding and shared delivery spaces, may affect the feasibility of allowing birth companionship.
Data collection procedure and instrument
A self-administered structured questionnaire, which was adapted from different studies31–33 used (See Supplementary File 1). The questionnaire was initially developed in English, and was then translated into Amharic for data collection purposes, and subsequently back-translated into English to ensure consistency and accuracy.
Data quality control
Three BSc midwives supervised the data collection. Their roles included coordinating the data collection activity, checking completeness and addressing any issue that arose during data collection. Prior to data collection, the questionnaire was pretested on 11 obstetric care providers working at Addis Alem Primary Hospital representing 5% of the total population, to determine the accuracy of the responses and the appropriateness of data collection tool. Based on the pretest findings, some questions were reworded for clarity, response options were adjusted accordingly. In addition, internal consistency of the questionnaire was assessed using Cronbach’s alpha, yielding a coefficient of α=0.72, which indicates acceptable reliability.
Data processing and analysis
After checking for completeness and consistency, the data were coded and entered into EpiData version 4.6 and exported to SPSS version 27 for analysis. Incomplete questionnaires were excluded, and any minor inconsistencies were cross-checked and corrected where possible before analysis. Descriptive statistics were computed and presented using tables with appropriate explanations. Bivariate logistic regression analysis was performed to assess the association between dependent variable and independent variables using odds ratios (OR) with 95% confidence intervals (CI). Variables with a p-value < 0.2 in the bivariate analysis were considered for inclusion in the multivariable logistic regression model. The goodness of fit of the model was assessed using the Hosmer-Lemeshow test, which indicated an adequate model fit (p > 0.05). Multicollinearity among independent variables was checked, and no significant multicollinearity was detected. Finally, multivariable logistic regression analysis was conducted to identify independent predictors while controlling for potential confounders. Statistical significance was declared at p-value < 0.05.
Results
Socio-demographic characteristics
Socio-demographic characteristics of obstetric care providers working in public hospitals of South Gondar Zone, North west, Ethiopia 2025 (N = 211).
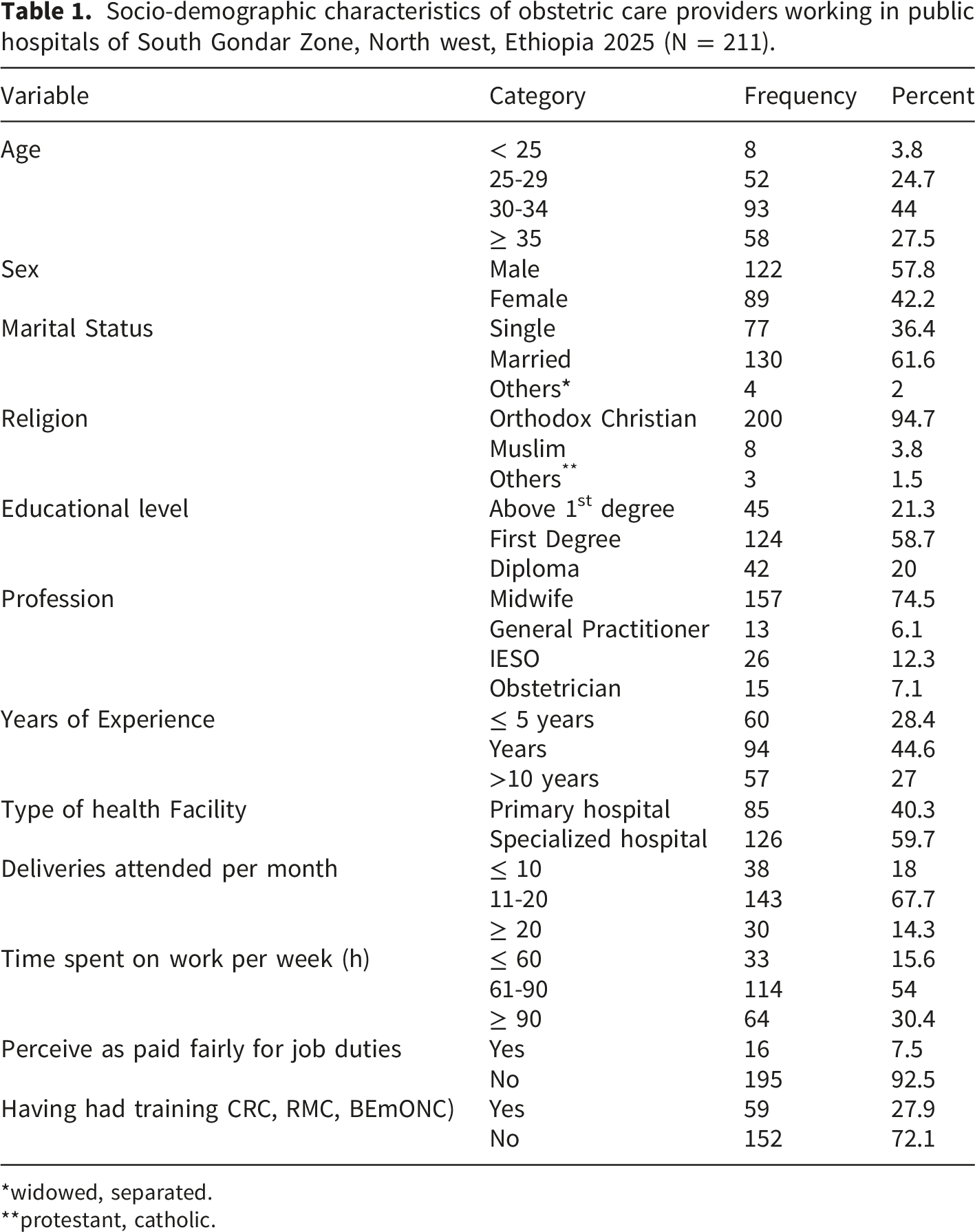
*widowed, separated.
**protestant, catholic.
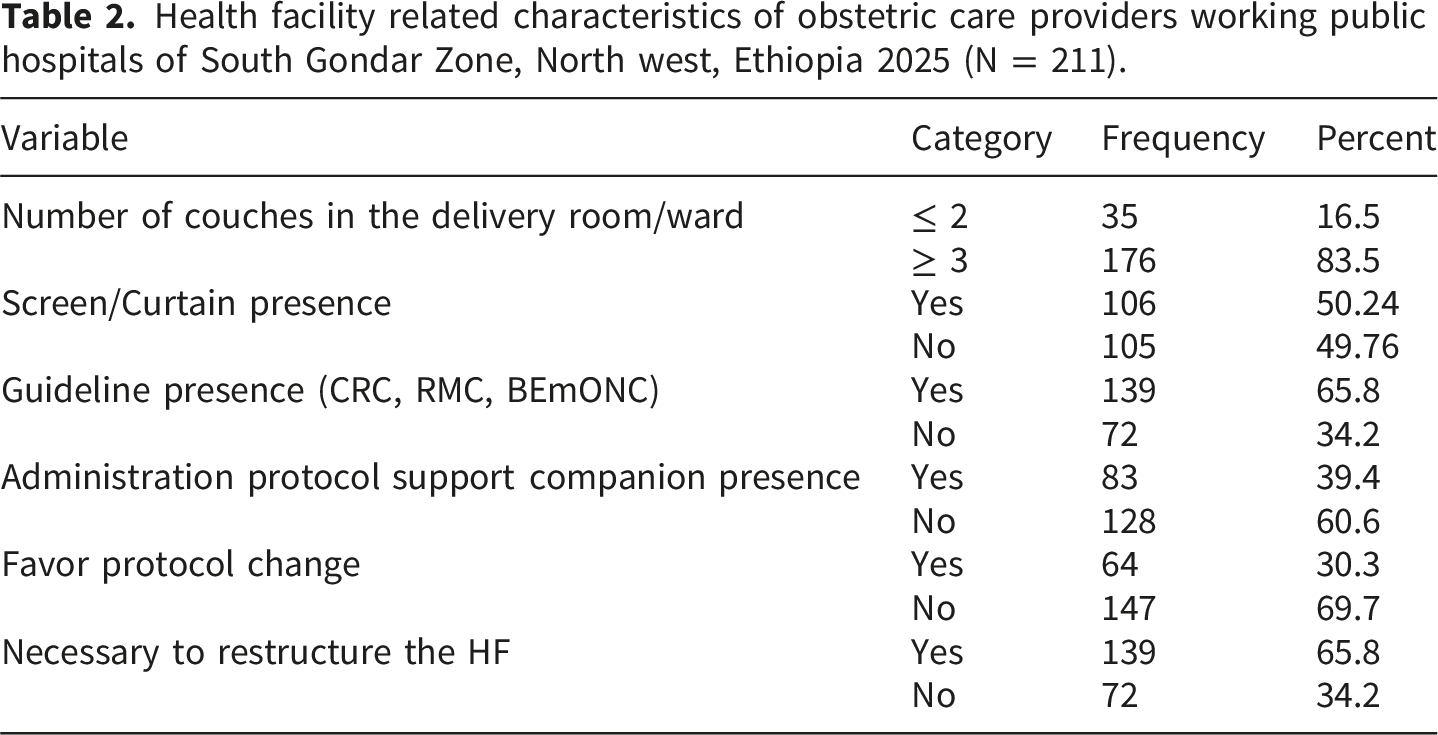
Health facility related characteristics
Health facility related characteristics of obstetric care providers working public hospitals of South Gondar Zone, North west, Ethiopia 2025 (N = 211).
Practice of obstetric care providers regarding birth companion presence during childbirth
Practice of obstetric care providers’ regarding companion presence during childbirth in public hospitals of South Gondar Zone, North west, Ethiopia 2025 (N = 211).

Factors associated with the practice of obstetric care providers’ regarding companion presence during childbirth
Factors associated with the practice of obstetric care providers’ regarding companion presence during childbirth in public hospitals of South Gondar Zone, North west, Ethiopia 2025 (N = 211).

Discussion
The overall practice of birth companionship among obstetric care providers in this study was 16.59% (95% CI, 11.6-21.6). Given that the WHO explicitly recommends birth companionship as a routine, evidence based component of maternity care, this prevalence is substantially below the expected standard. Studies conducted in West Shewa zone (19.5%), Addis Ababa (17.6%), Arba Minch (13.8%) and in Debre Markos (14.6%) report comparable figures, suggesting that the failure to implement birth companionship is a nationwide problem rather than an institution specific one.31–34 Furthermore, studies from other Ethiopian regions including Addis Ababa, 35 Gondar, 36 South West Ethiopia, 37 and in Shashemene Town, 38 have supported this pattern collectively pointing to systemic barriers within the Ethiopian maternity care system. Common challenges reported across these studies include high patient load, shortage of space, inadequate privacy arrangements, and limited emphasis on respectful maternity care within routine obstetric services.
Beyond Ethiopia comparable findings have been reported across sub-Saharan Africa. Studies in Kenya, 21 South Africa 22 and in Burkina Faso 39 similarly report birth companionship implementation rates below 20%. While direct comparison across these studies is limited by differences in study design, sample population and measurement approaches, the consistently low rates across diverse settings suggest shared regional challenges, including inadequate facility infrastructure, limited implementation of respectful maternity care policies, and provider centered models of care that do not prioritize women’s autonomy and support needs during childbirth.
While sub- Saharan countries continue to struggle with implementation, substantially higher level of birth companionship practice have been reported in high income countries such as United Kingdom, the United states and Norway.10,40 The observed disparities may be explained by stronger health policies, better resourced health facilities, adequate staffing and labor wards designed to ensure privacy and accommodate companion. Furthermore maternity care system in those countries are generally guided by policies that promote maternal autonomy, shared decision making and positive childbirth experience. 6 However it’s important to acknowledge that these differences are not only attributed to resource availability, but also high income countries have also benefited from decades of sustained policy development and advocacies for women-centered care, which are very different from the Ethiopian health systems historical trajectory.41,42 This gap in practice underscores the urgent need for policy level commitment and resource investment in Ethiopia and similar settings.
Consistent with our hypothesis, prior training of CRC, RMC, and BEmONC was the strongest predictor of birth companionship practice, with trained providers being 1.55 times more likely to allow companionship. This finding corroborates evidence from earlier study done in west Shewa zone 31 where training was similarly identified as a key factor affecting companion practice. An interventional study conducted across three regions of Ethiopia demonstrated that targeted training significantly improved provider practice of birth companionship, 43 while a study in South West Ethiopia shows that providers with training have positive perception towards birth companionship, 37 a plausible explanation is that such training emphasizes patient centered care, respect for women’s rights, and the psychosocial benefits of continuous support during labor, thereby shifting providers’ attitude from task oriented to compassionate care, increasing awareness of international guidelines and equipping them with the skills and confidence to implement evidence-based respectful practices, including facilitation of birth companionship. 44
Providers working in facilities equipped with curtains or other privacy partitions were 1.48 times more likely to allow companion, reinforcing the critical role of physical infrastructure in enabling respectful maternity care. This aligns with findings from another study conducted in Ethiopia, which specifically identified the absence of privacy measures as a structural barrier, with providers reporting concerns about exposing laboring women in shared wards and compromising their confidentiality and dignity. 31 These concerns are important because, in communal labor setting the presence of a companion without privacy measures can increase woman’s vulnerability. This is evidenced by various studies done in Ethiopia, for instance a study in Addis Ababa and Gondar shows that absence of partition or curtains is a major barrier to allowing companion during labor and childbirth.35,36
Overall the findings of this study imply that birth companionship remains far from institutionalized in Ethiopian public hospitals. The consistently low prevalence across multiple settings, combined with the identified roles of training and physical infrastructure, suggests that implementation barriers are both attitudinal and structural. The persistence of these gaps despite existing national and international policy framework points to a significant disconnect between policy intent and ground level practice in Ethiopian maternity care.
Strength and limitations of the study
A key strength of this study is that it focuses on assessing the utilization of birth companionship from the perspective of health professionals, which is less commonly explored in previous studies in Ethiopia. However, the study excluded health centers in South Gondar Zone, primarily due to instability in predominantly rural areas. Including these centers could have increased the study population and provided a more representative dataset because these facilities serve a large rural population and may have different staffing, resources, and practices compared with hospitals. In addition, the study did not incorporate a qualitative exploration to understand the contextual or behavioral factors influencing the allowance of a companion during childbirth such as motivation and perception that influence whether or not companions are allowed. In addition, a formal sample size calculation was not performed rather all eligible obstetric care providers were included since they were small and manageable, but this might make some results less precise. Furthermore, the use of self-reported data may have introduced social desirability bias, as respondents could have over-reported practices perceived as favorable. In addition, the questionnaire used in this study was adapted from existing tools rather than being pre-validated instrument, which may affect the comparability of findings with studies using standardized measures.
Conclusion
Birth companionship practice among obstetric care providers in public hospitals of South Gondar Zone remains critically low, reflecting a broader systemic failure to translate national and international respectful maternity care policies into routine practice. Both provider level factors particularly training on CRC, RMC, BEmONC, and facility level factors such as availability of privacy measures were significant determinants of practice, underscoring that implementation gaps are simultaneously individual and structural.
Given the low prevalence of birth companionship practice and its significant association with provider training and facility measures, targeted actions are needed. The Ethiopian Ministry of health should strengthen enforcement of existing respectful maternity care policies and incorporate birth companionship as a measurable indicator within national maternal health monitoring framework. At the facility level, health administrators and regional health bureaus should integrate components of respectful maternity care and birth companionship into routine in service training for obstetric care providers. Additionally all public hospitals should prioritize the installation of privacy measures such as curtains and partitions as a minimum infrastructure standard in labor ward. Furthermore awareness of women’s right to companion of choice should be strengthened through antenatal care services and community health platforms. Finally future research should include lower level health facilities and explore context specific barriers to implementation using qualitative approaches.
Supplemental material
Supplemental material - Obstetric care providers’ practices and associated factors towards birth companionship in public hospitals of south Gondar zone, North west Ethiopia, 2025
Supplemental material for Obstetric care providers’ practices and associated factors towards birth companionship in public hospitals of south Gondar zone, North west Ethiopia, 2025 by Rahel Birhanu Arage, Begizew Yimenu Mekuriaw, Habtam Desse Alemayhu, Mahider Shimelis Feyisa, Wassie Yazie Ferede, Besfat Berihun Erega in Sage Open Medicine.
Footnotes
Acknowledgment
Our deepest gratitude goes to Debre Tabor University college of Health Science for giving us Ethical clearance. We are also grateful to the data collection supervisors for their dedication and commitment in ensuring the quality of the data collected. And a heartfelt thanks goes to all obstetric care providers who participated in this study. Without their willingness, time and honest response this research would not have been possible.
Ethical considerations
Ethical clearance was obtained from the Institutional Ethical Review Board of college of Health sciences, Debre Tabor University with reference number DTU/0084/25 and support letter obtained from department of Midwifery and submitted to each hospital prior to data collection. Finally, written Informed Consent of the respondents was obtained after thoroughly explaining the aim of the study to individual health professionals.
Author contributions
RBA-participated in conceptualization, Study coordination, Methodology, Data curation, Data analysis, writing original draft and reviewing. BYM-participated in methodology, Data curation, and Data analysis. HDA-participated in methodology, Data curation, and Data analysis. MSF- participated in methodology, Data curation, and Data analysis. WYF- participated in methodology, Data curation, and Data analysis. BBE-participated in methodology, Data curation, Data analysis, writing original draft and reviewing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data included in this manuscript can be accessed from the corresponding author upon request through the email address with justified reason.
Supplemental material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.