
Abstract
Despite numerous campaigns, influenza vaccination of healthcare workers remains insufficient in France. The highly cognitive approach of persuasion models in healthcare poorly explains this non-vaccination. A survey of 794 French nurses and nurse aides in 2018 highlights the role of psychological reactance. The greater their perceived threat to freedom due to vaccination pressure, the more it generates situational reactance and strategies for restoring their threatened freedom: denial or minimization of the health threat (low perceptions of severity and vulnerability to influenza) and diminished attractiveness or denigration of the recommended option or its source (low perceptions of efficacy and benefits of vaccination), leading to rejection of the recommended behavior (flu vaccination). This original modeling of variables traditionally seen as antecedents to reactance explains persuasive failure and is contextualized and discussed through objective characteristics (age, profession). Managerial recommendations and avenues of research follow.
Introduction
In the context of influenza prevention, vaccination is considered the best way to prevent flu and is actively recommended to healthcare workers (HCWs) (Ochoa-Hein et al., 2021). Yet, their vaccination rate remains low, particularly in France: only 28.8% of nurses and 19.1% of nurse aides were vaccinated in 2021/2022 (Santé Publique France, 2022). However, neither the lethality nor the detrimental consequences of influenza, particularly for elderly or frail patients (Thompson et al., 2006), and for healthcare institutions (Li et al., 2021; Ling et al., 2019; Yan et al., 2017), nor even the fact that HCWs can be carriers of infection are disputed (Ahmed et al., 2014; Hofmann et al., 2006; Kuster et al., 2011). Thus, preventing influenza spread is a major public health issue. Nevertheless, the many incentive campaigns in favor of HCW flu vaccination, implemented at all levels of health institutions, struggle to convince these professionals, despite an improved access to vaccination. 1 Consequently, from a social marketing perspective (Gallopel-Morvan, 2006), it raises questions on the (in)effectiveness of such communication.
The major risk of this “vaccine hesitancy” (Larson et al., 2016) is that it turns into refusal (Yaqub et al., 2014). Via explicit or implicit reference to the main theoretical models (see Appendix 1): Health Belief Model (HBM, Rosenstock, 1966), Protection Motivation Theory (PMT, Rogers, 1975), or Extended Parallel Process Model (EPPM, Witte, 1994) in particular, and also Theory of Planned Behavior 2 (TPB, Ajzen, 1991), the relationships between the common variables of these models: perceived susceptibility or vulnerability, severity, efficacy, and HCW flu vaccine hesitancy, or, more often, its opposite – vaccine acceptance (see Corace et al., 2016, for a systematic review) have been examined. In general, their conclusions are: “Perceptions of vulnerability and severity . . . have been consistently proven to be associated with compliance with this measure [flu vaccine]” (Bellia et al., 2013). So, the lower the perceptions of severity, vulnerability, and/or efficacy, the lower the flu vaccination intention/behavior (e.g., Habib et al., 2000; Prematunge et al., 2012; Shahrabani et al., 2009).
However, these models do not explain why HCWs, aware of the consequences of influenza for themselves or, at least, for their frail patients and their community (Prematunge et al., 2012; Yaqub et al., 2014), and of their professional responsibility in this domain (Colaprico et al., 2022), manage to paradoxically develop low perceptions of severity, vulnerability and/or efficacy for themselves and even for others (Hollmeyer et al., 2009; Raftopoulos, 2008). Moreover, these traditional models and variables do not explicate why, in some studies (e.g., Chen et al., 2021), the individuals who feel most vulnerable are also the most reluctant to be vaccinated. Related to this, Vallée-Tourangeau et al. (2018) consider that the main weakness of these models is assuming that HCW vaccine decision-making is rational. In the same vein, Bodelet et al. (2021) wonder if the HCW flu vaccine might not instead be “a matter of emotion.” Therefore, searching for other mechanisms to explain such paradoxes is needed. Our research aims to provide a new understanding of HCW reluctance to flu vaccination, likely to more fully explain HCW flu (non)vaccination through different modeling of the traditional common variables.
Indeed, the psychological reactance theory (PRT), which postulates that situational reactance occurs when people feel that one of their individual freedoms is reduced, suppressed, or threatened (Brehm, 1966; Brehm and Brehm, 1981), has already clearly shed light on this negative reaction in a context of noncompliance, in this case, the patient’s non-adherence to treatment (Fogarty, 1997). When people experience situational reactance, they feel anger, develop counter-arguments toward the behavior threatening their individual freedom, and, above all, seek to restore their threatened freedom through behaviors sometimes totally opposite to the recommended action (Dillard and Shen, 2005; Quick and Stephenson, 2008). This famous “boomerang effect” is the most emblematic strategy of freedom restoration, but other softer and lighter strategies also exist, such as increased liking of the threatened option, source derogation, denial of the threat existence, or practice of a different kind of freedom. This situational reactance and its freedom-restoring strategies have been regularly identified in various health persuasion contexts (Dillard and Shen, 2005; Fogarty and Youngs, 2000; Grandpre et al., 2003; Quick et al., 2015; Rains and Turner, 2007) and even through psychophysiological measures (Spelt et al., 2019). Nevertheless, to the best of our knowledge, only Witte (1994) has explicitly considered reactance into a persuasion model – EPPM, but with reactance being just seen as based on a defensive motivation leading to message rejection and processes of fear control, particularly by way of reactance (message derogation or minimization and perceived manipulation intent) or defensive avoidance. However, in the spirit of the PRT (Brehm, 1966; Brehm and Brehm, 1981), perceptions of severity and vulnerability, as well as perceptions about the efficacy of the recommended behavior (here, HCW flu vaccination), considered predictors in the traditional models, can be seen as the expression of indirect strategies to restore threatened freedom (here, freedom to be vaccinated or not). Moreover, Witte (1994) raised questions as to the place of these variables seen by her as predictors of reactance since she observed that the defensive avoidance or the negative reactance toward the message leads to an altered perception of threat (severity/vulnerability) and recommended responses. It, therefore, suggests a different place for all these variables in health persuasion modeling. More generally, it also calls for a better understanding and consideration of psychological reactance, particularly freedom restoration strategies, in health persuasion processes. The main explanation provided by PRT is that people exposed to an injunctive message perceived as threatening their individual freedom of behavioral choice (feeling of threat to freedom) will first manifest their reactions to this threat on their freedom (situational reactance in terms of anger and counter-argumentation toward the source of freedom threat, namely, the persuasive message/source attempting to “impose” a specific behavior), and second will try to restore their threatened freedom through diverse indirect and/or direct strategies: denigration, derogation, denial of the threat on health or of the recommendation/source for the first ones, and/or total rejection of the recommended behavior (seen, in the traditional models, as the logical outcome of a correct assessment of the threat in terms of severity and vulnerability and the recommended response efficacy), and possibly choice of the opposite behavior (boomerang effect) for the second ones. So, when coping with situational reactance toward the persuasive message perceived as the source of a threat to freedom, people are likely to develop a biased and somewhat irrational assessment of the threat to health evoked in the message (e.g., a specific risk or danger, such as a risk of infection) in order to restore their threatened freedom (e.g., a behavioral choice). Recently, McGuire and Ball (2022) adopted a similar view by observing an indirect freedom restoration strategy – the denial of COVID-19 threat – to a message advocating recommendations related to COVID-19 and inducing freedom threat and reactance. However, these authors do not take into consideration other variables among those mentioned above and, therefore, do not propose a more integrative view, as we seek to do in this article. Furthermore, freedom restoration strategies have received little attention from researchers as noticed by Li and Shen (2022). These authors (p. 48) also point out that among the many forms of freedom restoration suggested by researchers, it is almost only attitudes and behavioral intentions toward the recommended behavior that have been examined, while the other ways to restore threatened freedom “may play equally important roles in understanding the nature and effect of reactance.”
Taking such a perspective and considering that HCWs who feel their hand forced by urging them to get the flu vaccine could experience situational reactance, this research aims to better understand the negative effect of top-down health institutional communication on HCW flu (non)vaccination behavior by integrating situational reactance with a focus on a variety of freedom restoration strategies. It thus allows for a better understanding of what may lead HCWs to make a decision that seems to be contrary to their own benefits and/or those of their patients and their institutions. It responds to the call for more emphasis placed on addressing the negative attitudes and barriers that lead to HCW flu vaccine refusal (Doebbeling et al., 1997; Takayanagi et al., 2007). Furthermore, to better explain this psychological reaction due to the pressure from health institutions, our research also considers some objective characteristics of nurses and nurse aides.
To the best of our knowledge, our cross-sectional study of 794 French nurses and nurse aides, either vaccinated or non-vaccinated during the 2018 winter season of flu vaccination, is the first to shed light on their hesitancy in such a comprehensive and original manner. Next, we draw attention to the literature: first, on HCW flu vaccination hesitancy in light of major, but open to criticism, social cognitive models on the one hand, and communication efforts on the other hand; second, on PRT and particularly situational reactance to persuasion and HCW pro-vaccination campaigns. We then specify our methodology, present our results, and finally discuss them, their contributions, limitations as well as possible research avenues.
Conceptual framework
Flu vaccination and HCW hesitancy in view of major but questionable models
Many existing social cognitive theories and models applied to health behaviors (e.g., HBM, PMT, EPPM, and TPB) focus on individual social cognitive factors of health behavior acceptance (cf. Appendix 1). The major common variables considered by these models can be classified into two groups. The first refers to threat appraisal: (1) perception of severity (seriousness of disease consequences) and (2) perception of vulnerability (perceived likelihood or susceptibility). The second relates to coping appraisal: (1) effectiveness of the recommended behavior (response efficacy) or perceived benefits of preventive action and (2) self-efficacy (perception of his or her ability to perform the behavior). PMT also mentions perceived barriers to preventive action which more directly relate to hesitancy or refusal.
In this broad perspective of vaccination hesitancy or refusal, MacDonald (2015: 4163), stated that “vaccine hesitancy refers to delay in acceptance or refusal of vaccination despite availability of vaccination services.” Concerning the HCW flu vaccine, with a more specific focus on hesitancy/refusal, some articles, explicitly or not, referred to the above traditional social cognitive models. A review article on flu vaccination programs, aimed at identifying their success and failure causes and attitudes and beliefs of HCWs, pointed out in particular that misconceptions and misperceptions about influenza and its risks were key factors (Hofmann et al., 2006). Similarly, the systematic review of Corace et al. (2016) emphasized that in all the studies considered, the perceived need for vaccination of HCWs who were not vaccinated toward influenza was low. In the same vein, Raftopoulos (2008), through focus groups with Greek nurses in order to examine more in depth their knowledge, attitudes, and beliefs about flu vaccination, underlined that they mainly explained their non-vaccination by a good health, a low vulnerability to flu, a low perception of flu vaccine usefulness for themselves, and effectiveness. In addition, they mentioned a fear of possible vaccine adverse effects, such as causing the flu. For other authors (Ballestas et al., 2009; Corace et al., 2013; Cornally et al., 2013; Dini et al., 2018; Real et al., 2013) too, the non-vaccinated HCWs did not perceive a personal danger related to flu, but their perception of vaccine adverse effects (vaccine causes illness) and allergies was stronger than those of vaccinated HCWs. Looijmans-van den Akker et al. (2009) also confirm that non-vaccinated HCWs’ perception of personal risk is significantly lower: while 40.4% of vaccinated respondents perceive a high personal risk for influenza infection, there are only 9.6% perceiving a high personal risk among non-vaccinated HCWs.
Likewise, a World Health Organization (WHO) systematic review of influenza vaccine hesitancy from 2005 to 2016 for various targets including healthcare personnel (i.e., both healthcare and non-healthcare occupations) highlighted that low-risk perception associated with influenza, as well as low perceptions of the likelihood of getting flu and the severity of flu, were barriers to vaccination. Nevertheless, there is no full consensus around the barriers and predictors of flu (non)vaccination, nor a high reliability of the results (Corace et al., 2016). Dey et al. (2001) noted that despite the low flu vaccination rate of their sample of HCWs in the United Kingdom, flu severity and vulnerability, as well as vaccine safety, were perceived by over 90% of respondents, but 88% of them thought that flu vaccination was ineffective. They conclude that the communication based on HBM, in their case inefficient, is not sufficient to change HCWs’ behavior. Similarly, Cairns et al. (2012: 3) concluded that the evidence about the relevancy of TPB or HBM as useful theoretical frameworks is weak, especially because knowledge is not sufficient in order to increase vaccination intention or behavior.
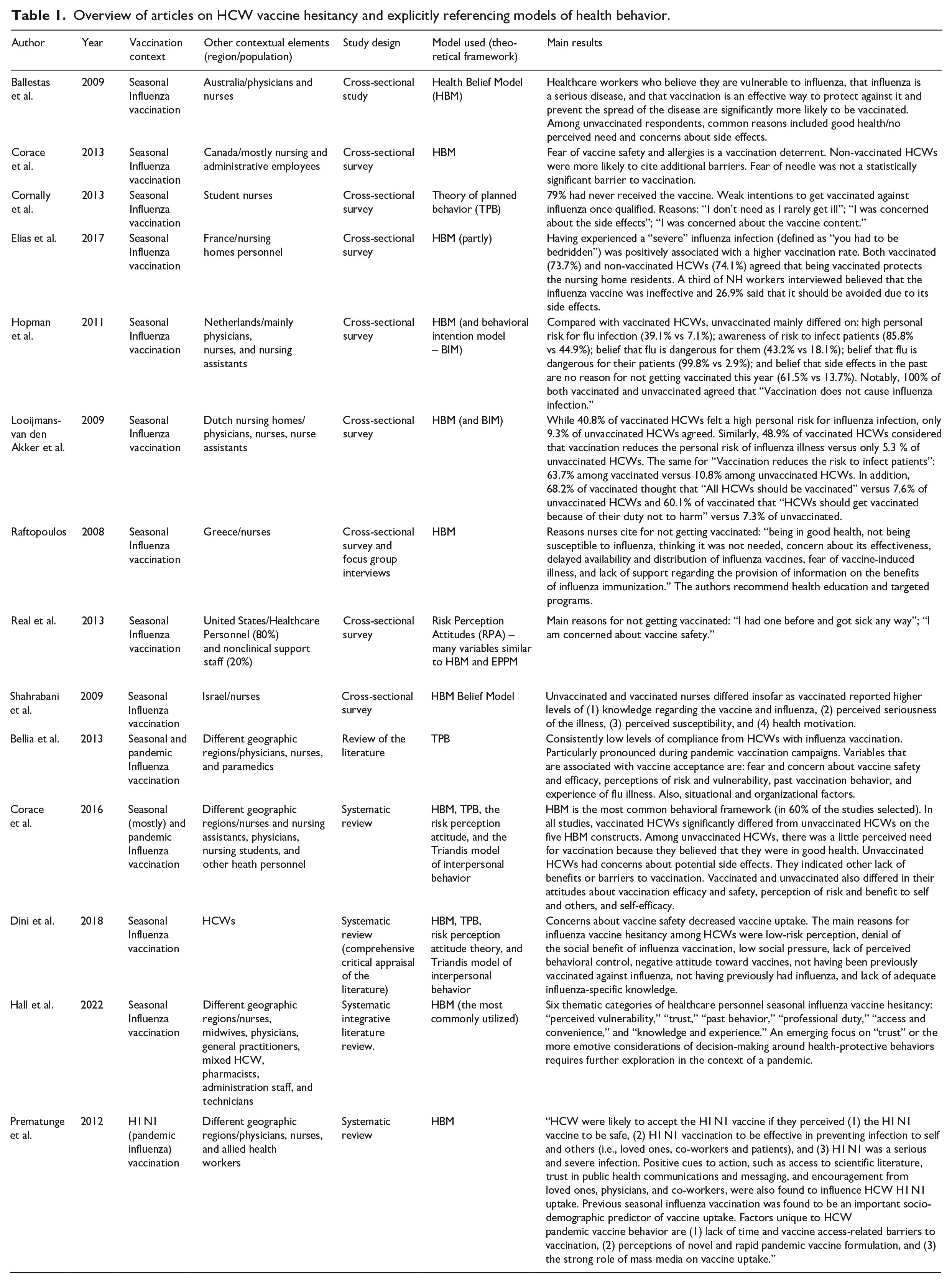
Furthermore, Hollmeyer et al. (2009) noticed, about 21 studies, that there is a high heterogeneity among the reasons for refusing flu vaccination expressed by HCWs. In that respect, “(1) none of the reasons in any study were mentioned by more than 60% of participants, (2) no category of reasons was covered by all studies, and (3) every category was represented in at least one study as the top category” (Hollmeyer et al., 2009: 3937). Likewise, conclusions about HCWs’ self-perception and perceptions related to others and, more particularly, to patients are not fully convergent. While the previous authors observe that HCWs are more motivated by personal benefits when they decide to be vaccinated against flu than by benefits for their patients, on the contrary, Bodelet et al. (2021: 1462) state that “the primary reason HCWs themselves cite for obtaining vaccination is the protection of their patients (Hofmann et al., 2006; Yaqub et al., 2014),” bringing them to a prosocial conception of HCW vaccination, confirmed by Hopman et al. (2011). From this divergence, Jones et al. (2015: 568) state that “despite a large body of research supporting the influence of HBM variables on health behavior, ambiguity still exists concerning which variables are most important and how variables interact within the model.” Thus, these various findings question the relevance and sufficiency of the underlying theoretical models presented above for the purpose of explaining HCW flu vaccine hesitancy. Table 1 shows an overview of articles on HCW vaccine hesitancy that explicitly refer to models of health behavior. The table presents only works with an explicit reference to at least one model in which the question of hesitancy is addressed explicitly or implicitly through non-compliance or the comparison of vaccinated/non-vaccinated HCWs (cf. Table 1).
Overview of articles on HCW vaccine hesitancy and explicitly referencing models of health behavior.
More generally, these models have been the subject of criticisms, likely to explain, at least in part, their inability to fully explain certain health behaviors (or lack of behavior). They converge with some of the above conclusions regarding their assumption of rationality in HCW vaccination choice (Vallée-Tourangeau et al., 2018), the ignorance of emotional factors (Walker, 1999) and optimistic perceptions of themselves (Freimuth, 1992, cited by Obregon, 2000). Similarly, concerning EPPM, even if Witte (1992) highlights the place of emotion (fear) in her model, Dutta-Bergman (2005: 112) points out that “much of the experience of emotions in EPPM is dependent on cognitive appraisal.”
Flu vaccination and HCW hesitancy in view of promotion efforts
In parallel, the effectiveness of such persuasive communications is also questioned. Despite the multiplication of communication and promotion campaigns aimed at convincing HCWs that, at the personal level, influenza is a serious disease, and they are likely to catch it, and, at the prosocial level, they can/must protect their frail patients by getting vaccinated against influenza, their vaccination rate remains low. “Still, a large proportion of HCW continue to oppose vaccination regardless of facts, evidence, and information presented” (Corace et al., 2016: 3240), such as: the positive impact of HCW flu vaccination on the reduction in mortality of the elderly and/or at high risk of complication patients (Carman et al., 2000; Dolan et al., 2012; Elder et al., 1996; Pereira et al., 2017; Potter et al., 1997); the higher risk (up to 2.5 times compared with healthy adults) of flu infection for HCWs (Jacek Jedrzejek and Mastalerz-Migas, 2022; Kuster et al., 2011) with the result that up to 25% of the HCWs are infected in winter (Elder et al., 1996; Jacek Jedrzejek and Mastalerz-Migas, 2022; Odelin et al., 1993; Pereira et al., 2017), many of these infected workers continuing to work (Ahmed et al., 2014; Jacek Jedrzejek and Mastalerz-Migas, 2022) and potentially being a vector for the virus circulation (Potter et al., 1997); and significantly lower rates of HCW sickness absenteeism from flu vaccinated HCWs (Pereira et al., 2017; Saxén and Virtanen, 1999). In addition, the side effects of vaccination, often evoked by unvaccinated HCWs (see Table 1), seem to be largely overestimated by them since numerous studies have shown that their prevalence is low: 13% but with only 2% of associated absence from work (Smedley et al., 2007), and that the few symptoms actually reported (Colaprico et al., 2022) are not serious (nasal congestion and sore throat in particular).
Similarly, Parrish-Sprowl (2018) believes that research is too focused on message content and information and ultimately too little on how HCWs make vaccination choices and their feelings, emotions, or intuitions. HCW vaccine hesitancy persists despite the information and knowledge provided, highlighting that both are needed to change behaviors but not sufficient (Corace et al., 2016). More broadly, MacDonald (2015) concluded that communication, if poorly designed, can increase vaccine hesitancy. Educational efforts, particularly those aimed at reassuring the targets of pro-vaccine communications, can have effects similar to the famous backfire effects on individuals who are doubtful or opposed to vaccination (Vallée-Tourangeau et al., 2018). This would increase negativity and resistance. Indeed, both these communication campaigns and existing models fail to explain why, in different health contexts including vaccination, individuals who feel the most vulnerable are, at the same time, the least favorable to vaccination (Chen et al., 2021) or to change their risky health-related behavior (Courbet, 2003).
From that point of view, it is essential to take a different look at the mechanisms likely to explain HCW intention to be vaccinated or not. Certain elements mentioned above lead to take into consideration a theoretical framework neglected until now in the context of HCW hesitation to be vaccinated against influenza, and more generally the barriers to vaccination, that of situational psychological reactance. The parallel between anti-vaccination and anti-consumption – a specific form of resistance (Roux, 2007) – has been successfully explored on a more general level (Chaney and Lee, 2022; Lee and Male, 2011), and the topic of vaccine refusal has also been addressed through the issue of freedom (Colgrove and Samuel, 2022). In contrast, the parallel between vaccine hesitancy and situational reactance, another form of resistance, has not been explored to our knowledge in the specific context of HCW non-vaccination against influenza and very rarely in the context of vaccination in general (Sprengholz et al., 2021). Yet, the question of freedom of choice (at the origin of situational reactance) appears to be one of the major themes in the explanation of anti-vaccination (Lee and Male, 2011). In France, the issue of individual freedom is a particularly sensitive one, and the freedom of vaccination has long been rooted in a culture of defending individual freedoms and resisting attempts to impose vaccination behavior: “Even before the COVID-19 health crisis revealed a strong anti-vaccine sentiment in France, signs of an oppositional tendency had appeared, with roots in several controversies beginning in the 1990s” (Guimier, 2021: 1). It is also important to bear in mind that, more broadly, “people are not as receptive to information when they are in a reactive of defensive state . . .” (Parrish-Sprowl, 2018: 6530). This could explain the low effectiveness of pro-vaccine campaigns in the case of situational reactance caused by them.
Psychological reactance theory
PRT (Brehm, 1966) explains “why people often do the opposite of what they are asked to do, and why efforts to persuade are often ineffectual” (Fogarty, 1997). Brehm (1966) defines the concept of psychological reactance as “a motivational state oriented towards the recovery of free behaviors that have been eliminated or threatened with elimination” (p. 9). Subjects react to attempts to control their behavior by restoring the threatened freedom: rejection of the message, opposite behavior (“boomerang effect”), and so on.
Four elements underlie PRT: (1) individual freedom, (2) perceived threat to freedom, (3) situational reactance, and (4) freedom restoration (Brehm, 1966). Indeed, individuals expect to be free to adopt or not adopt certain behaviors and value these freedoms. Any pressure to limit or prevent individual freedom is perceived as a threat (e.g. Wilhelm and Gavard-Perret, 2022). In such situations, they experience an aversive motivational state (situational reactance) seen as a combination of intertwined emotional and cognitive reactions (Dillard and Shen, 2005). As a result, reactance is modeled as a two-step process, with freedom threat being a kind of “induction check” (Reynolds-Tylus, 2019: 4). Cognitive and affective reactive states may then lead to attitudes and behaviors of denial, message rejection, or behavior contrary to that requested, in order to restore the threatened freedom (Buller et al., 1998; Rains and Turner, 2007).
Originally considered from the point of view of the reactance state that an environment can generate (situational reactance), psychological reactance has also been considered from the point of view of reactance trait (Kelly and Nauta, 1997), that is, the tendency of individuals to be more or less reactant and therefore to react more or less strongly to what they perceive as a threat to their free choice. However, in the present work and based on our research objective, only situational reactance is considered.
Situational reactance, persuasive communication, and HCW pro-vaccination campaigns
Because of reactance, the attractiveness of the eliminated or threatened option is increased, and “boomerang effects” have been clearly observed in the context of health interventions (Ringold, 2002). Burgoon et al. (2002), therefore, stress the importance of identifying the reasons behind reactance to health messages in order to avoid triggering it. Any persuasive communication can indeed be perceived as an infringement of free choice, and in the specific situation of health communication, reactance is frequently generated because the communication aims to modify behavior (Burgoon et al., 2002; Rains and Turner, 2007). In a health context, persuasive communications are becoming more and more frequent due to the increasing emphasis on preventive medicine based on primary prevention. Many authors explain, through reactance, the failure of health campaigns (Hornik, 2002; Salmon and Murray-Johnson, 2001) or their low effectiveness (Snyder, 2001). Röttger et al. (2017) found that subjective norms, used in order to increase perceptions of social desirability and pressure to participate in workplace health promotion programs, lead to lower intentions. They suggested psychological reactance as a relevant explanation. Dillard and Shen (2005: 145) also highlighted that “high-pressure communicators are likely to be seen as threats to freedom (Brehm and Brehm, 1981; Wicklund, 1974).” Li and Shen (2022) emphasized that explicit persuasive intent and forceful or dogmatic language can also be perceived as a threat to freedom.
However, the traditional models do not integrate psychological reactance. Only Witte, in her 1994 research, explicitly refers to reactance and takes it into account. But she only considers reactance as the expression of a fear appeal failure. More specifically, in the case of defensive motivation because of high fear arousal, there are message rejection responses: defensive avoidance and reactance. The main explanation provided by Witte is that this negative reaction is due to a high perception of threat (severity, vulnerability) but a low perception of efficacy. So, Witte’s EPPM, probably because of her possibly too cognitively dependent vision (Dutta-Bergman, 2005), only sees the role of reactance as a consequence of threat assessment and the recommended responses. In fact, Witte (1994) considers and measures reactance only from the cognitive point of view of message derogation and minimization and perceived manipulation, not from its emotional angle (anger, irritation). Furthermore, there is no specific measurement of threat to freedom, even though it is a necessary condition to ensure the existence of a state of situational reactance and not any other form of resistance, and she never evokes freedom restoration strategies which are yet major elements of PRT. However, certain observations made by Witte (1994: 129–130) herself when taking reactance into consideration in her EPPM model indicate possible limitations of this narrow view of reactance, from the point of view of PRT: “When individuals defensively avoided the threat or reacted against the message (i.e., perceived manipulation, minimized the message), they did not think about the responses recommended to avert the threat.” Similarly, Witte (1994: 130) observed that: “the more defensive avoidance and message minimization occurred, the less threatening AIDS became.” It means that when people react to a message trying to impose a recommended behavior, their strategies of freedom-restoration (such as message minimization) lead them to consider the threat as being less threatening and to ignore the responses recommended. In other words, reactance impacts both perceptions of severity/vulnerability (perceptions of threat) and perceptions of efficacy (perceived benefits of the recommended behavior). It suggests that these different perceptions allowing the evaluation of the threat (severity, vulnerability, efficacy), included as reactance antecedents in Witte’s model, can be seen as potential outcomes of the situational reactance to the message threatening an individual freedom in a modeling including psychological reactance in accordance with PRT. Indeed, Witte (1994: 131) herself points out that: “several of the specific hypotheses were not supported in this study. Thus, it is possible that parts of the model are incorrectly specified and in need of modification.”
Concerning more specifically the context of vaccine uptake, it is now clearly admitted that Media campaigns that promote vaccination, as any health communication campaign (Quick et al., 2018), can be ineffective if people perceive them as a pressure on their autonomous decisions. When people experience such a threat to their freedom by controlling messages or persuasive attempts, this is a perceived freedom threat (Verpaalen et al., 2023: 2).
For instance, Bell et al. (2022: 21) observed that “participants that reported greater agreement with the statement ‘I feel/felt under pressure from my employer to get a COVID-19 vaccine’ were significantly more likely to decline the vaccine even after demographic factors were controlled for.”
These findings can be related to the conclusions of Reynolds-Tylus (2019: 2), who explicitly stated that “Direct restoration may include directly engaging in an admonished behavior (e.g., consuming alcohol after exposure to an anti-drinking message), or by resisting an advocated behavior (e.g., refusing a flu vaccination after exposure to a pro-flu vaccination message),” it means a direct freedom restoration (“boomerang effect”). But, this author (p. 2) also evokes the possibility of indirect restoration by “derogating the source of the freedom threat, denying the existence of the threat, or by exercising a related freedom.” The approach adopted by McGuire and Ball (2022) that considered the denial of COVID-19 as a public health threat is fully in line with the conclusion of Reynolds-Tylus (2019). With this in mind, the denial of influenza as a severe disease, and even more so for HCWs assumed to have the medical knowledge and experience of patients who have had influenza, can be seen as a way to restore a threatened individual freedom (freedom of choice) more than a rational and responsible information processing. The same reasoning can be applied to other variables of the traditional theoretical models, such as the perception of vulnerability to influenza and the effectiveness of vaccination, generally seen as predictors of vaccination behavior. In the light of the PRT, the latter can rather be seen as forms of denial and denigration also intended to regain a little control and room for maneuver in the face of individual freedom of behavior (to be or not to be vaccinated), which is considered to be threatened by the persuasive pro-vaccine pressures of multiple communication sources. PRT explains that when people feel that their freedom is threatened because they are being forced to choose one option (e.g., flu vaccination) over another (vaccination refusal), the attractiveness of the “forced choice” decreases while that of the opposite option increases (Miron and Brehm, 2006; Worchel and Brehm, 1971).
On the basis of the above knowledge and findings, and in line with the conceptualization of the reactance process (PRT), we first hypothesized that the perception of a threat to their individual freedom to be or not to be vaccinated against influenza by HCWs confronted with high-pressure pro-vaccination campaigns will positively influence the manifestations of situational reactance (affective in terms of anger and cognitive in terms of counter-argumentation) and that they will, in this case, be all the less inclined to be vaccinated. Nevertheless, and in accordance with the intertwined cognitive-affective model (Dillard and Shen, 2005), considered the most adequate model of the reactance process (Rains and Turner, 2007), although affective (anger) and cognitive (counter-argumentation) reactions are measured independently to ensure their existence, they will not be considered independently in our model and data analyses due to their intertwined status. They both reflect a state of reactance. On this basis, we propose the following first hypothesis.
H1: The more HCWs perceive a threat to their freedom to be vaccinated against influenza due to pro-vaccination communications directed at them, (1) the higher their cognitive-affective reaction state (H1a) and (2) the less likely they are to be vaccinated against influenza (H1b).
Then, considering the limitations related to an integration of the situational reactance in a traditional model of persuasion in a health context, such as EPPM (Witte, 1994) that we have noticed previously, we assume different modeling for a persuasion process taking into account situational reactance in accordance to PRT. More specifically, we assume that situational reactance will cause freedom restoration strategies (Reynolds-Tylus, 2019), first indirect strategies through denial of the threat (flu infection) both in terms of perceived severity of the illness and perceived vulnerability toward this disease, then indirect strategies too, but through denigration of response efficacy and benefits of flu vaccination, and finally direct restoration strategies via rejection of the recommended behavior and adoption of the opposite behavior. According to traditional models such as EPPM, there are two successive appraisals, the first for the threat to health and the second for the recommended response. On this basis, we consider that the first round of indirect freedom restoration strategies refers to a biased assessment of the threat to health (because of the threat to freedom and reactance), and the second round of indirect freedom restoration strategies relates to a biased assessment of response efficacy. This means a general assumption about the mediating role of threat perception (severity and vulnerability), then perceived response efficacy and vaccination benefits, between HCWs’ situational reactance to pro-vaccine communications and their choice to be vaccinated against influenza. This leads to the following second hypothesis.
H2: The higher the situational reactance of HCWs, (1) the lower the perceived severity of influenza infection (H2a) (2) the lower their perceived vulnerability to influenza (H2b), and then (3) the lower the perception of effectiveness and benefits of the flu vaccine (H2c and H2d), and finally (4) the less likely they are to be vaccinated against the flu (H2e).
Figure 1 details our model.
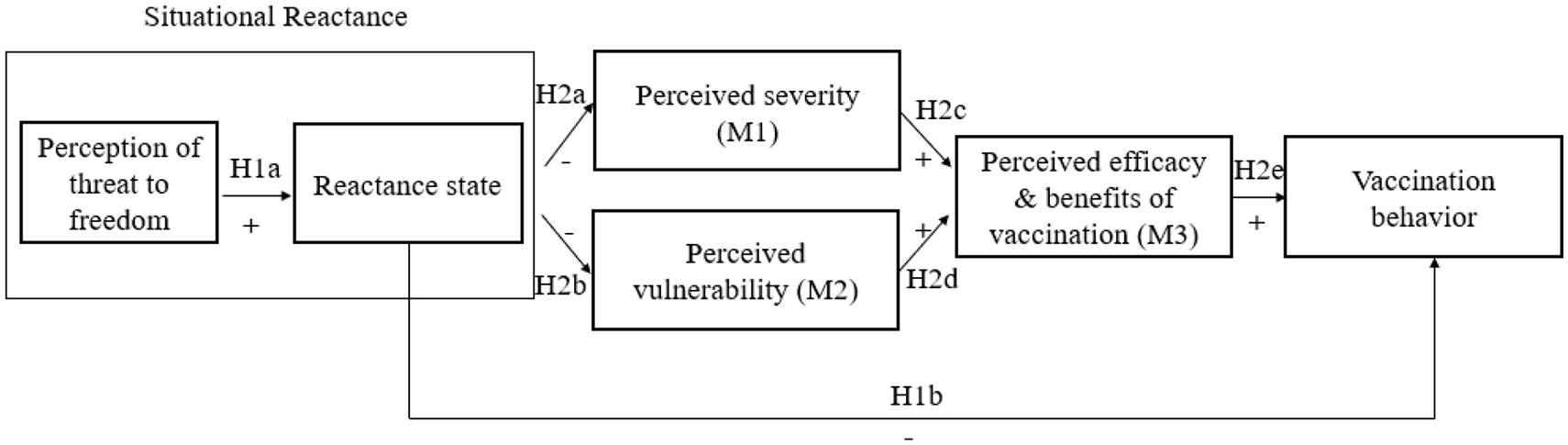
Model tested in the study.
Methodology
Data collection procedure
Between February and August 2018, we conducted a field survey among nurses and nurse aides from 10 French hospitals and other health institutions through the websites www.flu-ideas.com and www.flu-ideas.fr. We shared the links on various social networks (cf. Appendix 2–Poster inviting HCW to participate in the study). Our work corresponds to an epidemiological study involving the human person with research in the health field. According to the article R121-1 of the Public Health Code and the reference methodology MR-004 established by the “National Commission for Data Processing and Liberties” (CNIL) in France, before accessing the questionnaire, an explanatory text informed participants about the research and its strictly anonymous and voluntary nature. It was also explicitly stated in the introduction to the questionnaire that the respondent should feel free to complete it (or not). It was further explicitly written that the responses would be used exclusively for scientific research purposes. The participants could, if they wished, flash the QR code available on the awareness posters or click on the link of the questionnaire present on various social networks.
We administered the questionnaire via Qualtrics. In total, 1,515 French HCWs participated in the survey, but only 794 nurses and nurse aides fully completed the questionnaire. Data collection began at the end of the winter vaccination season in France and extended until the summer, which made it possible to measure vaccination behavior over the season taken into consideration. In this study, we decided to focus on the flu vaccine hesitancy from nurses and nurse assistants because their vaccination rate is lower than that of physicians. So, we obtained a database of 794 respondents, aged between 20 and 67 (mean 37 ± 10.6), 85% of whom were women, mostly working in hospitals. The demographic characteristics of the sample are shown in Table 2.
Demographic characteristics of participants.

Measurements
Participants completed an online questionnaire that included the measures required for the overall research project. For this article’s purpose, we focus only on those related to the process of psychological reactance toward the flu pro-vaccination communication from health institutions, as well as the dependent variables (those expressing freedom restoration strategies): (non)vaccination behavior during the winter season, perceived severity of the disease for oneself and patients, perceived vulnerability to influenza consequences for oneself and patients, perceived response efficacy, and benefits of vaccination for oneself and patients (see Appendix 3: Questions from the questionnaire related to these specific variables 3 ). Moreover, data were collected about demographic variables: age, gender, family status, profession (nurse aide, nurse), place of work (hospitals, nursing homes, etc.), department (surgery, medical emergency, etc.), graduation year, and number of years of seniority in the current institution. All the measures were based on 5-point Likert-type scales.
The main construct for this article is situational reactance to institutional pro-vaccination recommendations targeted at HCWs through the different variables involved in the reactance process in accordance with PRT. The first stage consisted of ensuring the presence of the different components of the reactance process as described in the PRT. This allowed us, in particular, to verify that the reactions of anger and counter-argumentation from HCWs toward pro-vaccine communications were indeed induced by the feeling of threat to freedom caused by the pressure felt with regard to these flu vaccination recommendations. This is how situational reactance can be differentiated from other forms of resistance. So, we first used a measure proposed by Dillard and Shen (2005) completed by Gardner (2010) and adapted to the context of the research. It is a complete and indirect measure of reactance with (1) a perception of threat to freedom (four items) and then (2) the affective (three items) and cognitive (three items) manifestations of a state of situational reactance (anger and counter-arguments). The ultimate dependent variable is the behavior promoted by the pro-vaccination campaigns, that is, HCW flu vaccination (one item – dichotomous variable: vaccination behavior during the studied winter season of flu vaccination vs non-vaccination behavior 4 ), and the other variables are, based on PRT, the indirect ways of restoring the individual freedom of choice toward HCW flu vaccination: flu threat perception in terms of severity (two items) and vulnerability (two items) for themselves and their patients; perceived response efficacy and benefits of HCW flu vaccination (four items). We decided to include perceived vaccine safety in the measure of perceived benefits of vaccination (or response efficacy) because Corace et al. (2013) showed that HCW perception of vaccine safety was considered a major perceived benefit. Nonetheless, and as already explained above, so as to take into account the intertwined status of the reactance state, the latter has been measured through a global score (combining anger and counter-argumentation). This way, we were able to test Hypothesis 1.
However, in order to simplify the test of our complex model, we then used a single measure of situational reactance. For this, we decided to proceed in a very similar way to what was done by Jonas et al. (2009) and calculated a composite measure from the above measures taken into account in the reactance development process (threat to freedom and the intertwined state of reactance), so as to have an overall situational reactance index. We nevertheless verified this possibility by examining the number of dimensions through a principal component analysis (PCA). With regard to the number of dimensions, the analysis indicates that the 10 items can be grouped into 1 dimension. This allows us to use a single-dimension measure for situational reactance. We finally calculated an average situational reactance index for each respondent. We introduced it in the complete model and the richer relational chain based on PRT. Doing so, we considered the situational reactance as an antecedent of two levels of indirect freedom restoration strategies and then a third level of direct strategies for restoring freedom threatened by pro-vaccine messages. This type of analysis, therefore, gave rise to the testing of a quite complex model based on a combination of serial mediations and parallel mediations in accordance with our Hypothesis 2.
Analysis of the measurement quality
We validated the quality of the scales. For scales with two items, we checked their reliability using Pearson’s correlation coefficient (perceived severity: r = 0.419, p < 0.001; perceived vulnerability: r = 0.404, p < 0.001) and Cronbach’s alpha for scales with more than two items (reactance: α = 0.946, perceived response efficacy and benefits: α = 0.903).
Following this, and before calculating mean scores for our variables, 5 we checked the structure of the scales, using PLS-SEM analysis in SmartPLS 4. The Jöreskog Rhô confirms the reliability of the scales (> .80 for each of the scales; see Appendix 4). Convergent validity is established when items converge to represent the underlying construct. AVE (Average Variance Explained) is calculated as the mean of the squared loadings of each indicator associated with a construct. This indicator shows that convergent validity is respected (see Appendix 4; the loadings of each item to the latent variable are also present in the appendix). Regarding discriminant validity, and based on the recommendations from Henseler et al. (2015), the HTMT – HeteroTrait-MonoTrait ratio of correlations – indicates that all correlations are below 0.85 (in the original sample as well as on average, with a sample bootstrapped 5,000 times). So, discriminant validity is validated: each scale measures a concept that is different from the other concepts in the model (see Appendix 4).
Data analyses for the hypothesis tests and preliminary analyses
We used SPSS for all analyses. We performed correlations, linear regressions, logistic regression, and mediation analyses via Hayes macro (Hayes, 2017). In this way, variables are mean-centered. We used linear regressions and model 80 (with 5,000 bootstrapped samples), a model for testing a serial mediation, but including, for the first level of mediation, two mediation variables in parallel.
Moreover, we ran preliminary tests for the linear regressions before conducting regressions via macro process models. Five conditions must be met in order to conduct regression analysis on quantitative data (Delacroix et al., 2021). First, the sample size: the sample is large enough to generalize the regression results (Hair et al., 1995 cited by Delacroix et al., 2021). Second, the linearity of the relationship: (1) simple regressions related to the effect of reactance on perceived severity and on perceived vulnerability were performed. The same for the effect of reactance on perceived response efficacy and benefits of the vaccine; (2) a logistic regression about the effect of perceived response efficacy and benefits of flu vaccination on vaccination behavior was carried out. Third, the homoscedasticity, that is, the constant variance of errors, was verified (see Appendix 5, which shows the graph between the “studentized” errors, i.e., divided by their standard deviation, e.g., with “reactance” variable for the dependent variable of “perceived severity”). Fourth, we checked the normality of the error terms (e.g., Appendix 5). Fifth, we have ensured the absence of autocorrelation of the residuals. Durbin-Watson (DW) tests were performed (see Appendix 5). In the DW table for a sample size N between 750 and 800, the absence of autocorrelation is indicated by a test result between 1.833 and 2.167. Thus, there was no auto-correlation of the error terms for the simple regressions. So, these preliminary analyses confirmed that we could conduct the next step of analysis. Also, Pearson’s correlations were calculated to assess the relationships between vaccination behavior and the other variables considered in this article. As shown in Table 3, the constructs were correlated with each other as expected. Some correlations are strong but do not exceed the threshold of 0.70, thus avoiding the existence of multicollinearity. Specifically, there were significant positive correlations between behavior and perceived severity, perceived vulnerability, perceived response efficacy, and benefits of the vaccine. As expected, we also observed negative correlations between situational reactance and all the other variables.
Correlations between variables.

The mean and standard deviation are not calculated for the vaccination behavior, a binary variable.
p < 0.05; **p < 0.01; ***p < .001.
Results
Descriptive statistics
At first, we analyzed the descriptive statistics for the variables of our model. As a reminder, the 5-point Likert-type scales used were based on: 1 – totally disagree to 5 – totally agree. Thus, a score of 3 represents the midpoint of the scale. Table 4 details the means and standard deviations for the total sample and, respectively, for the nurses and nurse aides.
Means and standard deviations of the studied variables.

t-test between nurses and nurse aides’ groups. Results are in bold when significant.
The means on the whole sample are around the mid-point, slightly below for the perceived response efficacy and benefits, and the manifestations of reactance (cognitive and affective), slightly above for the perceived threat of freedom and perceived vulnerability, and more distinctly above for the perceived severity. It appears that the nurse aides developed a higher level of situational reactance than the nurses, and this was statistically significant for the perception of threat of freedom, the affective manifestation, and cognitive manifestation (respectively, t(1,792) = −4.604, p < 0.001, t(1,792) = −4.482, p < .001, and t(1,792) = −4.316, p < 0.001). The differences in perceived threat (severity, vulnerability) were not significant, whereas the difference in perceived response efficacy and benefits of HCW flu vaccination was significant (t(1,792) = 5.96, p < 0.001), the nurses perceiving greater efficacy and benefits for flu vaccine of HCWs (cf. Table 4). We also observed differences in the mean values of the variables according to the type of structure and department in which the HCW is working. Using an ANOVA and post hoc tests (Bonferroni), we identified a significant difference in the severity of influenza, perceived as higher in nursing homes than in University Hospital and General Hospital (MNH = 3.89, MGH = 3.55, MUH = 3.62, F(4,789) = 4.063, p = 0.003). Concerning the differences related to the department, there was no mean statistical difference from the others on the ANOVAs performed, except for perceived severity (F(8,785) = 2.504, p = 0.011). However, the post hoc tests were not significant. This can be explained by the low number of respondents from certain departments and the high number of modalities.
Results of hypothesis testing
First, we began by observing HCWs’ perception of a threat to freedom caused by these pro-vaccination institutional communications. The latter is statistically higher for non-vaccinated HCWs than for those vaccinated (Mnonvac = 3.43, Mvac = 2.22, t(1,792) = 12.05, p < 0.001). We obtained similar results about the affective manifestation of reactance (anger; Mnonvac = 2.71, Mvac = 1.64, t(1,792) = 12.24, p < 0.001) and the cognitive manifestation (counter-argumentation; Mnonvac = 2.66, Mvac = 1.71, t(1,792) = 11.57, p < 0.001), the non-vaccinated HCWs developing higher levels of affective and cognitive situational reactance. Moreover, Figure 2 shows the differences in means of situational reactance between vaccinated and non-vaccinated HCWs (t(1,792) = 13.50, p < 0.001).

Means of situational reactance between vaccinated and non-vaccinated subjects.
Then, in line with our Hypothesis 1 concerning the detailed process of reactance, and the effect of HCWs’ perception of threat to freedom and reactance state on their vaccination behavior, we conducted a serial mediation. We used the SPSS macro process, model 4 (5,000 bootstrapped samples), which allows us to test a model with a serial mediation. The last analysis of the model (analysis of vaccination behavior) was a logistic regression because the measure of vaccination is a dichotomous variable (vaccinated = 1, non-vaccinated = 0). Table 5 presents the results of the test. Perceived threat to freedom to be vaccinated has a positive effect on the intertwined cognitive-affective reactance state (B = 0.683, SE = 0.019, confidence interval (CI) (0.646, 0.720); H1a), which in turn leads to (non)vaccination behavior (B =−0.553, SE = 0.132, CI (−0.811, −0.294); H1b). Thus, our first hypothesis is confirmed: the more HCWs perceive a threat to their freedom to be vaccinated against influenza due to pro-vaccination communications directed at them, (1) the higher their cognitive-affective reactance state and (2) the less likely they are to be vaccinated against influenza (χ2 = 146.8, p < 0.001).
Mediation analysis results using the PROCESS macro (model 4) on vaccination behavior.
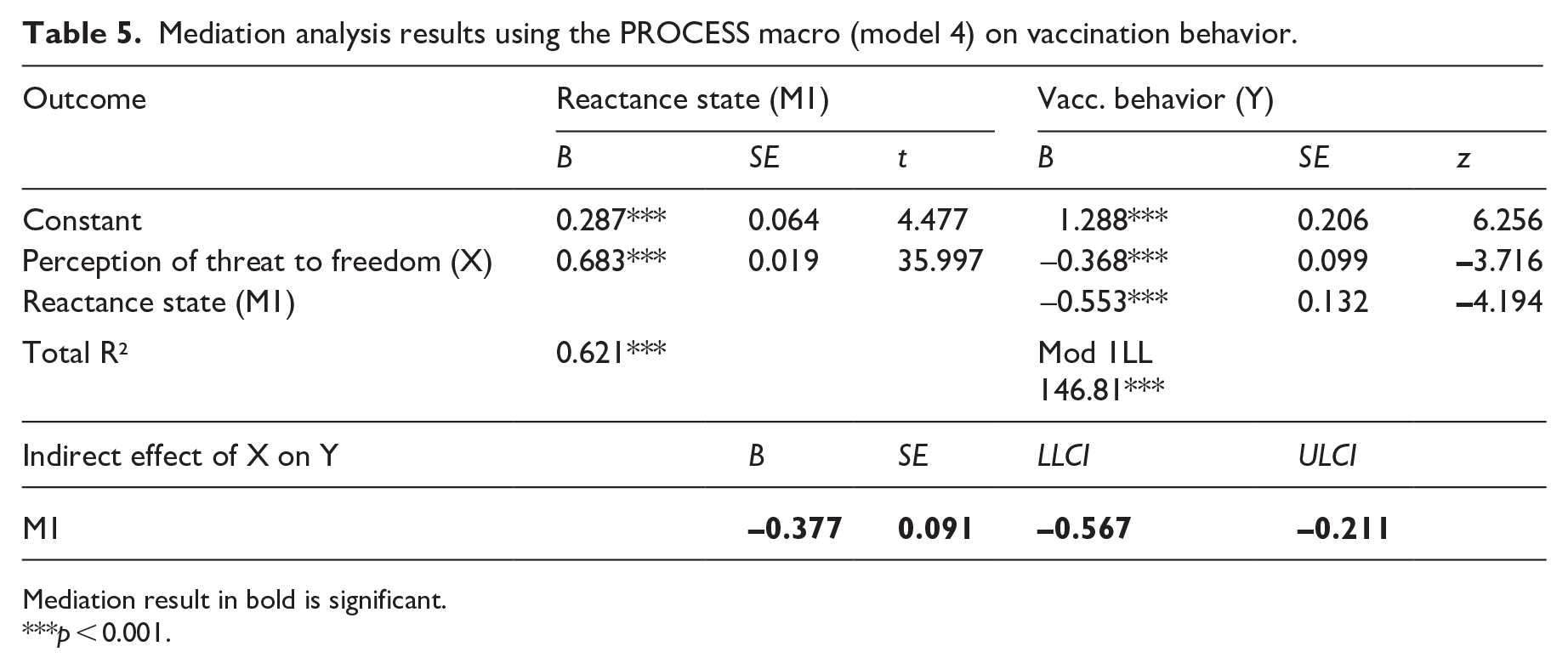
Mediation result in bold is significant.
p < 0.001.
Then, we carried out a serial mediation to test our main model on the population of nurses and nurse aides. Our second hypothesis is that the felt reactance influences the different indirect and direct ways through which individuals can restore their threatened freedom, namely, first the perception of threat (severity and vulnerability), then the perception of response efficacy and benefits of HCW vaccine, and finally the choice of behavior. So, the higher the HCW situational reactance (index) toward the pro-vaccination campaigns, the lower the perceived severity of flu and perceived vulnerability to the disease, the lower the perceived response efficacy and benefits of HCW vaccination, and the lower the vaccination behavior.
For these analyses, we used the SPSS macro process, which enables us to test mediations in series and in parallel via linear regressions. We ran model 80 (5,000 bootstrapped samples), which allows us to test a model with a parallel mediation for the first part of the mediation, as well as a serial mediation, with two successive mediators. The last analysis of the model (analysis of vaccination behavior) is a logistic regression because the measure of vaccination is a dichotomous variable (vaccinated = 1, non-vaccinated = 0). Figure 3 shows the model and the coefficients between the variables.

Model with path coefficients using the Process macro (model 80) on vaccination behavior.
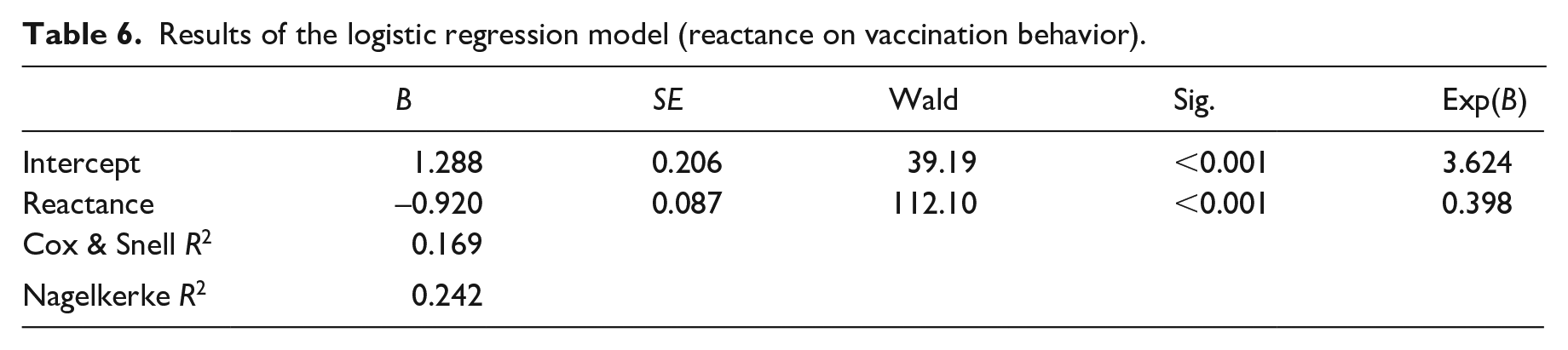
This logistic regression confirmed a direct effect of situational reactance on the choice of vaccination, with non-vaccination being considered as the main direct strategy of freedom restoration (“boomerang effect”) (χ2 = 146.8, p < 0.001). Table 6 presents the results of the logistic regression model. However, this direct effect was no longer visible when we tested the serial mediation. Table 7 presents the results for this serial mediation model.
Results of the logistic regression model (reactance on vaccination behavior).
Mediation analysis results using the PROCESS macro (model 80) on vaccination behavior.

Mediation results are in bold when significant.
Thus, it is a case of indirect-only mediation. It allowed us to think that the mediators identified were consistent with the hypothesized theoretical framework (no mediator seems to be omitted) and correctly explained the behavior (Zhao et al., 2010). Perceived situational reactance (index) has a negative effect on the perceptions of severity (H2a) and vulnerability (H2b), each of which in turn has a positive effect on the perceived benefits of vaccination (H2c and H2d), leading, via perceived severity: B =−0.11, SE = 0.021, CI (−0.155, −0.074) and perceived vulnerability: B =−0.05, SE = 0.012, CI (−0.076, –.030)), to (non)vaccination behavior (H2e). Simply put, the more individuals situationally react to pro-vaccine communications from institutions, the less severe they perceive the disease to be for themselves and their patients, and the less they feel themselves and their patients likely to be susceptible to getting it, the less they perceive the efficacy and benefits of HCW flu vaccination and the less likely they are to be vaccinated (χ2 = 294.4, p < 0.001). We also tested the model for nurses only and then for nurse aides. In both cases, we obtained similar results, and serial mediation was validated for these two populations. Thus, Hypothesis 2 is confirmed.
To rule out the possibility of reverse causality, we tested alternative models, more in line with the logic of traditional persuasion models in the health context, since reactance would be generated by the perception (severity; vulnerability) of the health threat in the first place, and by the perception of the efficacy and benefits of vaccination in the second, and it would be reactance that would lead to (non)vaccination behavior (Perceived severity -> perceived efficacy and benefits -> reactance -> vaccination behavior, and Perceived vulnerability -> perceived benefits -> reactance -> vaccination behavior). We used model 6 of the macro Process (5,000 bootstrapped samples). These models revealed no serial mediation (perceived severity: B = 0.068, SE = 0.057, CI (−0.040, 0.018), perceived vulnerability: B = 0.050, SE = 0.046, CI (−0.033, 0.146)), which would tend to statistically confirm the relevance of the proposed model based on PRT.
Finally, given the heterogeneity of our sample, we also control the possible effects of co-variables, such as age, profession, gender, number of years in the institution, and establishment structure (these variables were included as co-variables in models 6 and 80). We found, as already shown previously, an effect of the profession on the reactance level (B = 0.48, SE = 0.09, CI (0.285, 0.673)) and on the perceived efficacy and benefits of HCW vaccination (B = −0.34, SE = 0.07, CI (−0.476, −0.207)): nurse aides feel more reactance toward pro-vaccination communication and lower efficacy and benefits of HCW vaccination than nurses. Moreover, age had a slight effect on the reactance (B = −0.009, SE = 0.004, CI (−0.017, −0.001)), on the perceived severity of the disease (B = 0.011, SE = 0.003, CI (0.006, 0.017)) and on the perceived efficacy and benefits of HCW vaccination (B = −0.009, SE = 0.003, CI (0.004, 0.015)): the older the respondent, the lower their reactance, the greater the perceived risk of the disease and the perceived efficacy of vaccination. The other variables do not have any significant effect.
Discussion and conclusion
Discussion of the main results
This study examined the hesitancy of HCWs, more particularly French nurses and nurse aides, to be vaccinated against influenza via reactance to pro-vaccination communication from health institutions. Our results clearly show that when nurses and nurse aides feel stronger situational reactance, their perceptions about flu (severity and vulnerability) and flu vaccination (benefits/efficacy) are lower, explaining that they are less likely to choose vaccination. These results highlight the differences of perceptions between vaccinated and unvaccinated HCWs and are convergent with the vast majority of studies summarized in Table 1. However, the latter are more easily understandable thanks to the lens of situational reactance.
Moreover, our data confirm that the more they perceive their freedom to be vaccinated (or not) against the flu as being threatened, the more they manifest their situational reactance with anger and counter-arguments, and the less they are vaccinated. This boomerang effect (behavior opposite to the recommended response) caused by psychological reactance is the ultimate direct freedom restoration strategy. However, other indirect freedom restoration strategies are activated by HCWs perceiving their freedom of choice as threatened by pro-vaccination pressure from their institution. The first ones are based on a lower appraisal of the threat to health from influenza: the more the nurses and nurse aides feel situational reactance toward communications in favor of flu vaccination for the HCWs, the less they perceive influenza as a serious disease in terms of severity and vulnerability. The second one refers to their appraisal of the recommended response: the more they react, the less they perceive the threat as being serious and then, the less they perceive the benefits of flu vaccination (response efficacy). It means that their perception of a threat to their freedom of vaccination choice and their reactance state (cognitive and affective intertwined) caused by this threat negatively impact their vaccination behavior but also, in a serial mediation way, their dual assessment of influenza threat in terms of severity and vulnerability, and then their assessment of flu vaccination efficacy and benefits.
Theoretical contributions
Our survey on French nurses and nurse aides, whether or not they have been vaccinated against influenza in the winter season, allows us to investigate more specifically if and how psychological reactance felt toward repeated pro-vaccination communication from health institutions better explains non-vaccination behavior for these HCWs than the main variables from traditional persuasion models (perceived severity, vulnerability, and response efficacy). The latter are seen either as predictors of reactance in these models (EPPM; Witte, 1994) or, more often, not at all explicitly linked with reactance. On this first topic, our results clearly confirm that there is a significant difference between HCWs who chose to be vaccinated and those who opted for non-vaccination from the point of view of the feeling of threat to their individual freedom of behavior and the resulting state of reactance. Given the presence of a feeling of loss of freedom, our results support the idea that it is not just any type of resistance that is developed more intensely by the non-vaccinated, but psychological reactance (Brehm, 1966; Brehm and Brehm, 1981). Our results also match with the conclusion of the review by Cairns et al. (2012) on the lack of evidence to consider that models such as TPB and HBM provide an appropriate framework for the vaccination context in general. More generally, our approach sheds light on the way people may react negatively to persuasive communication and incentives perceived as limiting their individual freedom. This view is fully in line with the foundations of PRT (Brehm, 1966; Brehm and Brehm, 1981; Wicklund, 1974) and with many explanations and observations provided by major authors on this subject (Byrne and Hart, 2009; Quick and Stephenson, 2008; Rains, 2013; Reynolds-Tylus, 2019). Health messages aimed at preventing “bad” behavior or promoting “good” behavior are, almost intrinsically, likely to induce a feeling of threat to individual freedom of behavioral choice and, by the same token, to generate situational reactance (Burgoon et al., 2002; Dillard and Shen, 2005). Nevertheless, promotional and persuasive messages are not exclusive to public service messages focusing on social marketing issues, such as those relating to the vaccination of HCWs against influenza. In commercial and marketing communication, persuasive objectives are omnipresent and are therefore likely to provoke similar effects and reactions in the same way, based on feelings of infringement of freedom and the development of situational reactance (Clee and Wicklund, 1980). Many other commercial and marketing situations can also be perceived as limiting individual freedom (loyalty programs, promotion, product unavailability, unsolicited advice, intrusive marketing, etc.) and, as a result, lead consumers to psychological reactance (Fitzsimons and Lehmann, 2004; Kivetz, 2005; Lee and Wicklund, 1980; Wendlandt and Schrader, 2007; Wilhelm et al., 2019). Our observations, therefore, constitute an interesting knowledge base for marketing in general by providing a better understanding of the mechanisms that can lead to a refusal on the part of consumers exposed to a stimulus they perceive as an attack on their freedom.
But the most important theoretical contribution of our research concerns a major aspect of PRT, too often neglected by researchers, as various authors have pointed out (Li and Shen, 2022; McGuire and Ball, 2022): the consequences of provoking situational reactance, that is, the various efforts made to restore threatened freedom. Taking into account situational reactance to persuasive campaigns in favor of HCWS flu vaccination, in a manner consistent with PRT, suggests a very different modeling of classical variables such as perceptions of flu severity and vulnerability (or susceptibility), and perception of response efficacy (or vaccine benefits). The originality of our approach, based on the PRT (Brehm, 1966; Brehm and Brehm, 1981), is to reconsider the role and place of these variables. The latter are proposed as antecedents/predictors of the intentions/behaviors in the main social cognitive models and theories such as HBM, EPPM, or PMT (see Appendix 1), and when Witte (1994) takes reactance into consideration, it is as an outcome, in addition only cognitive, of these predictors. In our view, in full accordance with PRT, these variables related to assessments of the threat to health and of the recommended response are preceded by a step of assessment of the threat to individual freedom. Insofar as this first feeling of threat causes a reactance state (intertwined anger and counter-argumentation toward the persuasive pro-vaccination communications), HCWs who strongly react to this situation of infringement of their behavioral freedom develop a somewhat irrational and biased assessment of the threat to health and of the response mentioned in the “directive” communications. This is the way to regain a feeling of control and to restore their threatened freedom. This fresh light on HCWs non-vaccination behavior specifically strictly respects the conceptualization of psychological reactance stated by the pioneer author (Brehm, 1966) and based on a tryptic: (1) if people think that their individual freedom is threatened, (2) they experience a motivational state of psychological reactance (situational reactance) and because of the latter (3) they become motivated to restore their threatened freedom. Our approach is also in conformity with the recommendations from the main authors of this theoretical framework to model reactance as a complete process (Dillard and Shen, 2005; Quick and Considine, 2008; Quick and Stephenson, 2008; Rains, 2013; Reynolds-Tylus, 2019). It enables a different understanding of HCW flu vaccination hesitancy, and the relevance of this modeling is confirmed by our results.
From this viewpoint, our vision moves away from the traditional vision of the classic socio-cognitive models and, doing so, offers a better understanding of HCWs’ reactions and choices, in the context of HCWs’ flu vaccination, which can be seen as paradoxical and difficult to comprehend. Above all, our reactance model sheds new light on what HCW low perceptions of severity and/or vulnerability to influenza or of the efficacy of influenza vaccination can mean, while health communications, scientific studies, and field statistics regularly show and demonstrate the seriousness of this disease and the high probability for HCWs to catch and transmit it. With all the consequences, sometimes dramatic, that this diffusion can have on fragile patients, but also the strong organizational impacts generated in healthcare institutions, notably because of the absenteeism caused (Gianino et al., 2019; Ip et al., 2015). For instance, the study conducted in France by Elias et al. (2017: 4–5) on the flu vaccination of nursing homes personnel (not only nursing staff) showed a clear opposition in the responses between 52.9% of the personnel answering that “Getting the vaccine will prevent me from getting influenza” and 33.4% answering that “The flu vaccine is ineffective.” Another point is quite surprising: the flu vaccination coverage is higher for administrative employees than for HCWs, while one would assume that the medical knowledge of the latter about vaccination, vaccines, and influenza is higher than that of administrative staff. With all this in mind, our research follows the same approach as that of McGuire and Ball (2022) and confirms their findings. In their research, because of the situational reactance experienced due to a feeling of threat to individual freedom, people engage in attempts to indirectly recover their freedom by denying the very existence of the threat (in their case, COVID-19). In our work, our results cover a broader spectrum of indirect freedom restoration strategies that can be implemented by individuals: denial or denigration of the severity of the threat (here, flu) and of the vulnerability to the risk, but also denial or denigration of the benefits of the recommended behavior (here, vaccination against flu) and therefore of its efficacy. The paradoxical reactions and responses from HCWs above are more easily understandable when considered as a way for them to restore threatened freedom and as a defensive information processing, therefore not optimal from the point of view of rationality and cognitive processing, but effective in reestablishing freedom and control. Research works mentioned by Parrish-Sprowl (2018) clearly show, even by the observation of the amygdala, that people process information in a different way when they develop a defensive state. Similarly, Quick and Stephenson (2008) showed that people who develop a high level of reactance consider the message as less persuasive. Our results confirm that most reactant HCWs do not form the same cognitive evaluations of the pro-vaccine messages, either in terms of threat or response. Furthermore, in our research, both forms of freedom restoration are integrated as mediating variables in a full process of psychological reactance based on the state of situational reactance (in terms of intertwined cognitive and affective manifestations induced by the feeling of threat to freedom). This insight is a useful complement to the freedom restoration strategy most commonly explored by the authors: direct restoration through behaviors contrary to those recommended and leading to a backfire or boomerang effect. In fact, our results also show the existence of a complete (and statistically significant) reactance process explaining flu vaccination refusal by HCWs of our sample as a direct freedom restoration strategy. Even if some research work has already studied a certain type of individual strategy for restoring freedom (Dillard and Shen, 2005; Grandpre et al., 2003; McGuire and Ball, 2022; Miller et al., 2007; Quick, 2012; Rains, 2013), none has, to our knowledge, encompassed all of the major possible freedom restoration strategies from an empirical perspective and through a complete modeling of the reactance process.
Our results are also consistent with the observations from other authors about the negative role of pressure to vaccinate. Interviews conducted by Bell et al. (2022) with health and social care workers in the United Kingdom clearly showed that when individuals feel under pressure from their employer to get vaccinated (in their case against COVID-19), they are “more likely to decline the vaccine” (p. 21). Our explanation by reactance due to a perception of threat to freedom and leading through situational reactance to a desire to recover the lost or reduced freedom provides a relevant theoretical framework to understand these negative reactions. By emphasizing the seriousness of influenza, pro-vaccination communications may lead HCWs with a high perceived vulnerability to “process the strategic message as intended, but do not properly comply” (Obermiller, cited by Byrne and Hart, 2009: 14). This author explains this kind of contradiction by way of mechanism such as psychological reactance (Brehm and Brehm, 1981). So, vulnerability would not only be a freedom restoration strategy but also the cause of psychological reactance when the most vulnerable people are exposed to messages stressing the gravity of an illness. Because of this mechanism, it seems possible to explain the observation from Chen et al. (2021) about the fact that the most vulnerable respondents are also the most hesitant to be vaccinated. Our modeling provides useful keys to understanding such inconsistent reactions.
Considering low perceptions of flu severity and flu vaccination benefits as potential indirect freedom restoration ways also brings a different view on reactions that are mainly viewed as cognitive and rational responses and processing supposed to guide subsequent actions. On this last point, Beauvois (1995), as Chaney (2010: 110) reminds it, had a very different understanding: “Man does not act according to his thoughts, but thinks according to the circumstances of the act led him to.” Moreover, when people react, they do not react in a cognitive way only. They also react in an affective way, through anger. Some existing research observed that the impact of anger in the reactance process is stronger than those from counterarguments (Rains and Turner, 2007; Varava and Quick, 2015).
Moreover, situational reactance is a highly context-dependent variable. In this perspective, considering some possible antecedents would help to understand the influence of the context (e.g., working conditions) and of personal characteristics (e.g., reactance trait) on the perception of threat on freedom by HCWs, and then on (non)vaccination behavior.
Managerial implications
Regarding communications of vaccine recommendations from all levels of health institutions, our study clearly shows that they generate situational reactance and that this psychological resistance to top-down communications perceived as limiting individual freedom of choice is a factor that sheds light on the non-compliance of HCWs with incentives to vaccinate. It is therefore essential to design communication campaigns that avoid or limit the emergence of psychological reactance, for example, by choosing communication sources and characters that appear more similar (such as peers), by taking care not to use overly prescriptive language, and by favoring horizontal (such as social networks) rather than vertical (top-down) communication and also narrative messages. In addition, the elements to be highlighted in the messages must be chosen carefully. For instance, Larson et al. (1982) have shown that postcard reminders based on the HBM were significantly more effective in improving influenza vaccination compliance than more neutral reminders or no reminders.
Our focus on the role of reactance and on the various ways by which HCWs try to regain freedom provides a novel and better understanding of HCW negative reactions toward flu vaccination and leads to more easily determining how pro-vaccination messages should be designed to be effective from a persuasion point of view (or conversely, what they should not be so as not to generate reactance). It might be better to focus on educating health students so that they become convinced during their studies, and therefore outside of an overtly persuasive context, that influenza is a serious disease and that, although healthy, they are vulnerable to it too. If this information is given while they are working as HCWs, it risks appearing as an unbearable incentive communication because it hinders their individual freedom. Similarly, it is essential to find ways of raising awareness and persuading targets that minimize possible reactance effects and thus gently promote compliance. For example, Corsaro et al. (2017) showed that a forum theater was an innovative and participative strategy useful in order to foster HCW engagement regarding flu vaccination. Likewise, in a completely different context (diphtheria-tetanus-polio vaccination) and with a different target (young adults), Plichon et al. (2020) emphasized the differences in the effects obtained on the attitude and intention to vaccinate (which can go as far as an outright counter-productive effect) depending on the type of framing and argument used. Co-produce interventions (study of Thorneloe et al., 2021) 6 could also be a good way to avoid or limit reactance in involving employees.
Furthermore, it is important to choose sources of information that limit the activation of situational reactance. The health institution is clearly not the best source of information, at least in France, due to increased distrust. Moreover, sources perceived as close and similar are preferred (Bertrandias and Vernette, 2012).
The difficulty of convincing HCWs to be vaccinated may also highlight an insufficiency of health communication. As Rundle-Thiele (2015) pointed out, a full social marketing approach is rarely implemented. Prevention and health promotion are not enough to tackle an issue as delicate and complex as vaccination.
Limitations and further research avenues
We must consider some limitations of this study. The first limitation is that we collected data from a convenience sample that is not fully representative of the selected population. Selection bias may have played a role. In fact, the overrepresentation of unvaccinated HCWs in our sample could be an indicator of this bias, as unvaccinated HCWs are likely to be more interested in the topic as they are more defensive on this issue.
Another limitation of our work comes from a coding error in the questionnaire which did not allow us to collect the past vaccination behavior of respondents who answered having been vaccinated in the season considered. We were, therefore, unable to verify the impact of past decisions on the decision under review. However, numerous studies and systematic reviews have very clearly underlined the strong influence of past vaccination behavior on the decision to be vaccinated, even going so far as to mention “a default effect,” whether for patients or for HCWs and in many countries, including France (Bish et al., 2011; Shaham et al., 2020). This observation is also one of those which led us to prefer to examine the responses relating to behavior rather than to intention because the responses of respondents who have not been vaccinated in the past but who express a fairly strong or even very strong intention of vaccination in the coming year do not seem very reliable in view of previous observations. Without even mentioning the significant gap regularly shown between intentions and behavior.
Third, our measures of severity and vulnerability perceptions, each based on two items, show fairly low correlations (around 0.40). Another way to measure vulnerability (or susceptibility) might be to use absolute measures of perceived risk (e.g., van der Pligt, 1998), a numerical probability scale (e.g., Joseph et al., 1987), or a four-item scale (e.g., Bryan et al., 1997). For severity, some existing scales include more items (e.g., Bryan et al., 1997; Mai et al., 2021).
Fourth, we used self-reported data only, whose weak points are known. It would be interesting to cross such data with real behaviors and observations but also with more comprehensive methods such as interviews or projective and associative techniques. The use of implicit measurements rather than explicit ones could be a better way to have a less biased view of such situations. Moreover, our research was based on a cross-sectional survey. The only method that really allows us to predict vaccination intention/ refusal is the experimental approach. It is essential to develop research that manipulates pro-vaccination communication factors in order to identify adequate levers. However, a controlled but realistic experimental approach seems particularly difficult to implement, as it would be necessary to measure HCW reactions after exposure to experimental persuasive stimuli, but in the absence of any previous exposure to comparable stimuli, in order to be certain that perceptions of severity, vulnerability, and response effectiveness have not already been developed through such exposure. In France, as in most other countries, pro-vaccination communication campaigns are recurrent and the sources of exposure to such messages are numerous. Nevertheless, it would be interesting to see how different perceptions evolve over the course of exposure, in particular, to see whether feedback loops exist between reactance and perceptions of threat and recommended response. Likewise, based on PRT, we have proposed a new set of relationships and roles between common variables and situational reactance. From a theoretical point, it is relevant and our data analyses confirm this approach. However, Rodhain (1997) emphasized that the relationship between action and thought is cyclical due to a continuous mutual influence. Research considering this potential cyclical process would be very useful. In the same way, it would be judicious to explore the relationship between inoculation and reactance in the spirit of what Richards et al. (2017) did in order to mitigate psychological reactance by means of an inoculation strategy.
In addition, the perception of individual freedom being very situational and cultural, it would be important to see what it is like in other countries than France, where the claims of freedom are very strong. Considering more global context issues, such as social, political, and health contexts, is needed in order to understand potential environmental aspects that could exacerbate the feeling of threat to freedom and, consequently, the reactance process. When people feel under pressure for other reasons, they become more sensitive to other pressures (like pro-vaccination pressure). In this perspective, a more comprehensive orientation would be particularly interesting. Pechmann (2015) strongly recommends adopting social marketing research that is more Transformative Consumer Research-oriented insofar as it better takes into account social-cultural and situational contexts.
Finally, our conclusions are based on flu vaccination of nurses and nurse aids, but our findings and recommendations could also be very useful in other settings where the vaccination rate of HCWs is too low, such as hepatitis B (Doebbeling et al., 1996) and COVID-19. It would, therefore, be interesting to validate our findings in other healthcare settings (nursing homes, for instance, specific hospital departments, etc.), but also with other populations (elderly, parents for children vaccination) and other vaccines. Furthermore, the process of reactance being not specific to health and vaccination, it would be relevant to test our modeling in other persuasion and influence situations in marketing and commercial contexts.
Footnotes
Appendix 1
Appendix 2
Poster inviting HCW to participate in the study.
Appendix 3
Appendix 4
Appendix 5
Acknowledgements
We would like to warmly thank Annick Valette and Emmanuel Abord de Chatillon for their contribution to the overall project and to an earlier version of the article. We would also like to thank Laurent Bertrandias, the journal’s editor-in-chief, and the reviewers, who made a major contribution to repositioning and improving our article. Finally, this article is also part of the work of the Grenoble IAE research chair “Marketing at the Service of Society” (M2 S).