
Abstract
Premature ovarian insufficiency can have significant implications for the affected women. This review assesses the fertility desires, choice of hormone replacement, and the effect of time since menopause on the bone density of these women. This is a retrospective analysis of 223 consecutive new referrals. The average age (mean [±standard deviation]) of the women was 37.35 (±5.88) years, with 24.1% (n = 19/79) presenting within 12 months of the onset of symptoms, most commonly, vasomotor type symptoms (n = 98/223; 43.9%). Of the women included, 58.7% (n = 131/223) took hormone replacement therapy (HRT), most commonly, an oral (n = 90/131; 68.7%) sequential preparation (n = 91/131; 69.5%), with a significant number of women >40 years of age preferring the transdermal route (n = 26/54; 48.1%; p<0.01). A total of 37.7% (n = 84/223) of the women expressed concerns regarding their future fertility, more notable in women ≤40 years (n = 72/142; 50.7%; p < 0.01). Of these, 41.7% (n = 35/84) took HRT, most commonly, a sequential regimen (n = 26/35; 74.3%) with oral estradiol (n = 30/35; 85.7%); 69.5% (n = 155/223) of the women had had a bone densitometry scan performed, with 66.5% (n = 103/155) showing normal bone mineral density (BMD), but a greater likelihood of having reduced BMD the greater the time delay in presentation. No difference was seen for the three broad categories of BMD when further analysed for the cause of premature ovarian insufficiency, but a significant difference was noted for the spinal Z-scores, whereby women who underwent a surgically induced menopause were noted to have lower BMD compared with the other causes (p < 0.01). These findings can be useful in counselling women and guiding clinicians in their management of women with premature ovarian insufficiency.
Introduction
Premature ovarian insufficiency (POI) can have widespread implications for the affected patient population secondary to the deficiency of sex steroids, with physical, psychosocial and reproductive health concerns.1–5
POI remains largely under-researched and there is a lack of evidence from randomised trials to guide clinical practice regarding the optimal hormone replacement regimen in this context. As a result, considerable variations exist in prescription practices among clinicians looking after this group of women. We carried out this review to assess fertility desires, choice of hormone replacement in women with POI, and the effect of the duration of time since the onset of the menopause on bone mineral density (BMD).
Methods
This is a retrospective analysis of 223 consecutive new referrals of women with POI to a tertiary referral menopause service, during the period June 2004 to April 2011. The parameters assessed included presenting symptoms, fertility desires, bone density at presentation and choice of hormone replacement. We also assessed whether the age of the women at presentation had an effect on these parameters, particularly in terms of patients’ choice of hormone replacement.
Our service includes five clinics a week that are dedicated to the management of women with menopause symptoms within which women with POI can be seen.
Large variations exist in the age limits used to define premature menopause, with many studies using an age limit of 40 years to define premature menopause, and 40 to 45 years to describe an early menopause.6,7 The upper age limit used in this review was 45 years. This was based on the recommended cut-off age used in the 2007 British Menopause Society Consensus Statement on the management of premature menopause, and as used in other reports.6,7 The argument for this being that women who become menopausal between the ages of 40 and up to the age of 45 years are exposed to the effects of estrogen deficiency for a significant number of years compared to those who become menopausal at the age of 52 years or beyond.
Data were collected from the patients’ electronic hospital records and paper notes and entered onto an Excel spreadsheet. Statistical analysis was carried out using the Statistical Package for Social Sciences (SPSS Version 17.0). Variables that were normally distributed are presented as means and standard deviations (±SD) and were analysed using the independent and paired t test. The Chi square or Fisher’s exact were used as appropriate for independent nominal data. Confidence intervals were used where appropriate and statistical significance was defined as a p value of less than 0.05.
Results
The mean (±SD) age of the women seen in the clinic was 37 (±5.88) years, (range 17 up to 45 years). Of the total number of women, 142 (63.7%) were up to and including 40 years of age, and 81 (36.3%) were above 40 years of age. A total of 182 (81.6%) women were referred by their General Practitioners, with 22 (9.9%) women referred from other hospitals, 12 (5.4%) from the general gynaecology clinics in our hospital and seven (3.1%) patients were referred from the oncology department.
Cause of POI
The cause of POI was idiopathic in 164 (73.5%) cases and secondary to radiotherapy/chemotherapeutic interventions in 30 (13.5%) women. Other causes included surgically induced menopause (n = 26; 11.7%) and genetic causes (n = 3; 1.3%). The genetic causes included two cases of POI secondary to Turner’s syndrome (one of these being Turner’s mosaic) and one case of POI secondary to 46XT (X:22) with a balanced translocation between the long arm of the X chromosome and the long arm of chromosome 22.
The mean (±SD) age of the patients at presentation in relation to the aetiology of POI was 37 (±5.59) years for women with idiopathic POI, 36 (±7.64) years for POI secondary to radiotherapy/chemotherapeutic interventions, 40 (±4.22) years for surgical menopause and 31 (±7.02) years for genetic causes, (p < 0.01).
Presenting symptoms
Presenting symptoms of women with POI.
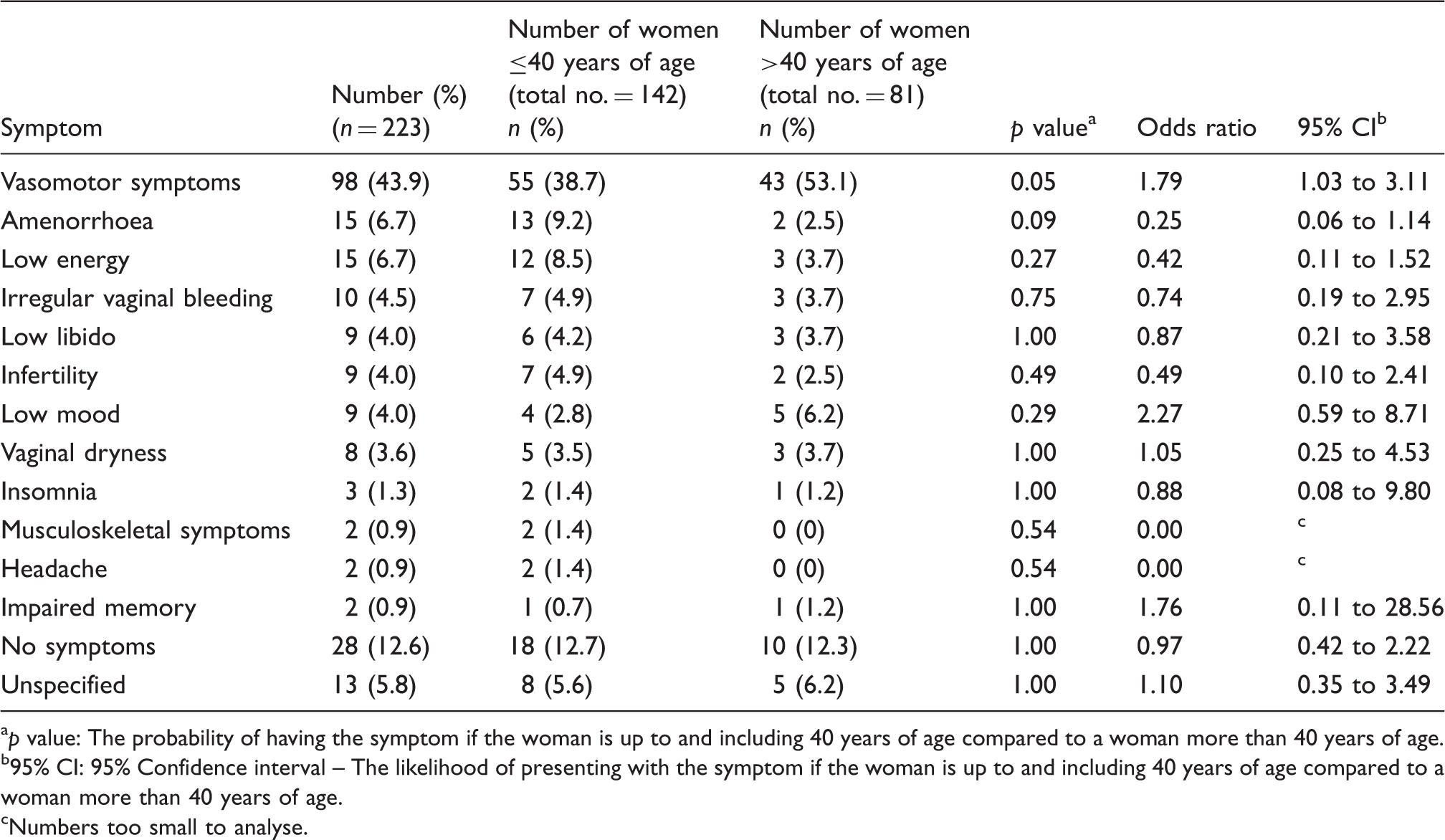
p value: The probability of having the symptom if the woman is up to and including 40 years of age compared to a woman more than 40 years of age.
b95% CI: 95% Confidence interval – The likelihood of presenting with the symptom if the woman is up to and including 40 years of age compared to a woman more than 40 years of age.
cNumbers too small to analyse.
Fertility desires
A total of 39 (17.5%) women included in the review already had children at the time of diagnosis, and 84 (37.7%) expressed concerns regarding their future fertility. Of these, a total of 72/142 (50.7%) women up to and including 40 years of age expressed concerns regarding their future fertility, compared to 12/81 (14.8%) women over 40 years (p < 0.01).
A total of 71/164 (43.3%) women with idiopathic POI had concerns about their future fertility potential, compared to 7/30 (23.3%) women with POI secondary to radiotherapy/chemotherapeutic interventions, 3/26 (11.5%) women with POI secondary to surgical causes, while all three (100%) women with POI secondary to a genetic cause expressed concerns regarding their fertility potential (p < 0.01).
Of the women with fertility concerns (n = 84), 44 (52.4%) received counselling regarding fertility options and two (2.4%) were referred for fertility treatment. A total of 35 (41.7%) women who had a desire for future fertility were prescribed hormone replacement therapy (HRT), while three (3.5%) opted to take the combined oral conceptive pill (COCP) at the time of presentation. Of those prescribed HRT (n = 35), 26 (74.3%) women were prescribed a sequential regimen, whilst nine (25.7%) took a continuous preparation. Furthermore, 30 (85.7%) opted for oral estradiol, whilst two (5.7%) women took estrogen in the form of a patch and two (5.7%) women were prescribed an implant. In one (2.9%) case, the mode of estrogen administration was not specified.
Choice of hormone treatment
Treatment choices of women with POI.
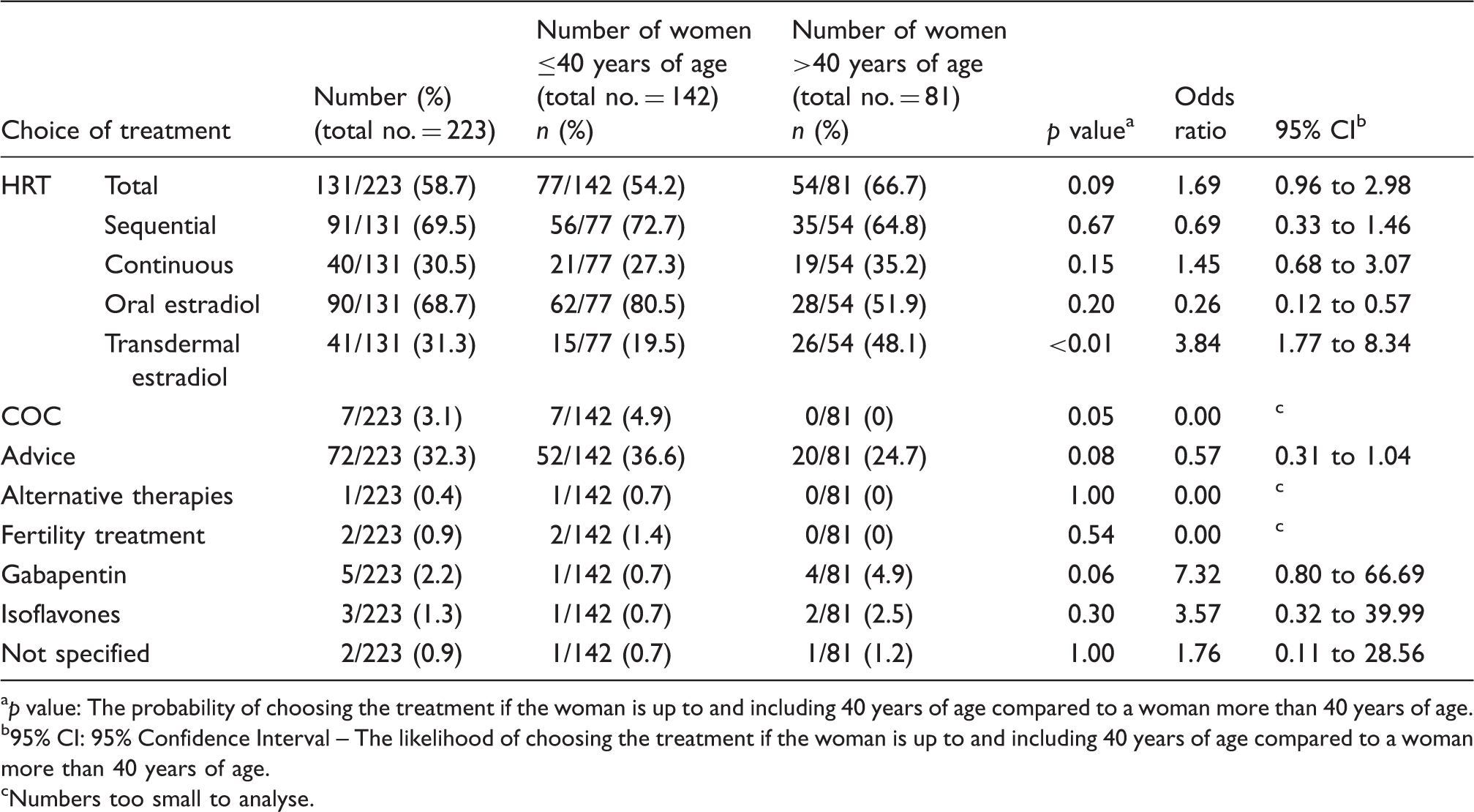
ap value: The probability of choosing the treatment if the woman is up to and including 40 years of age compared to a woman more than 40 years of age.
b95% CI: 95% Confidence Interval – The likelihood of choosing the treatment if the woman is up to and including 40 years of age compared to a woman more than 40 years of age.
cNumbers too small to analyse.
Further analysis according to the woman’s age, showed a total of 77/142 (54.2%) women under the age of 40 years opting to use HRT, whilst 54/81 (66.7%) women over 40 years of age chose HRT over other forms of treatment (p = 0.09). Of these, 56/77 (72.7%) women under the age of 40 years, opted for the sequential regimen, compared with 35/54 (64.8%) women over 40 years of age (p = 0.67). 21/77 (27.3%) women under the age of 40 years were prescribed a continuous HRT preparation, in contrast to 19/54 (35.2%) women over 40 years of age (p = 0.15). A total of 62/77 (80.5%) women under the age of 40 years were prescribed oral estradiol as part of their HRT regimen compared with 28/54 (51.9%) women over 40 years of age (p = 0.20), while 15/77 (19.5%) women under the age of 40 years were prescribed transdermal estradiol, compared with 26/54 (48.1%) women over 40 years of age (p < 0.01). In contrast, 7/142 (4.9%) women under the age of 40 years opted to take the COCP, compared with 0/81 (0%) women over 40 years of age (p = 0.05). These findings have been summarised in Table 2.
Bone density
A total of 155/223 (69.5%) women had had a BMD assessment carried out. Of these, a total of 103/155 (66.5%) women had normal BMD scans at presentation, 45/155 (29.0%) women had osteopenia and 7/155 (4.5%) women presented with osteoporosis. Sixty-eight (30.5%) women did not have a bone density assessment carried out.
Bone density in relation to cause of POI.
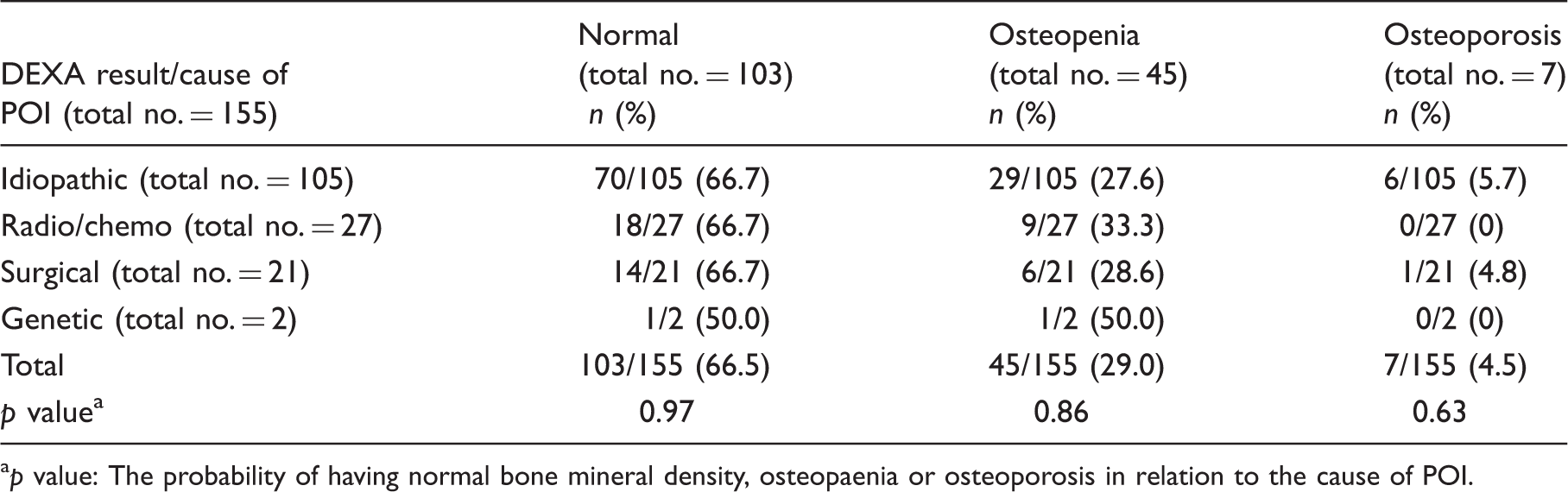
ap value: The probability of having normal bone mineral density, osteopaenia or osteoporosis in relation to the cause of POI.
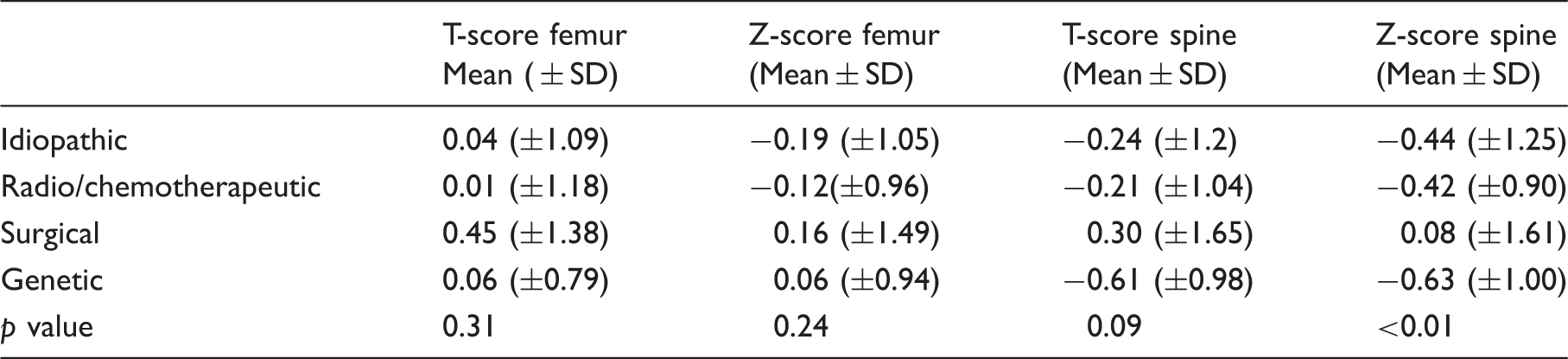
Bone density results, T and Z scores, in relation to cause of POI.
Bone density results in relation to time since the onset of symptoms.

Discussion
This large retrospective analysis of 223 consecutive new referrals of women with POI to a tertiary centre, assessed fertility desires, the choice of hormone replacement and effect of time since the onset of menopausal symptoms on bone density in women with POI. The average age of the women was 37 years and the majority presented more than 12 months after the onset of symptoms, the latter, most commonly being vasomotor type symptoms. One-third of patients expressed concerns regarding their future fertility and this was more notable in women less than 40 years of age. Approximately half of these women, whom had concerns regarding their future fertility potential, were prescribed HRT. Of these women, the majority opted for a sequential regimen with estradiol administered orally. Approximately three quarters of all women had a bone densitometry scan performed, with nearly half showing normal BMD and being nearly twice as likely to present with reduced BMD the longer the time delay in presentation. No statistically significant difference was seen for the BMD result when further analysed for the cause of POI, although women who had a surgically induced menopause had statistically significant lower spinal Z-scores compared to those who had POI secondary to other causes. More than half of the patients opted to take HRT, with the majority preferring sequential preparations with estrogen administered orally, but a significantly greater number of women more than 40 years of age opting for the transdermal route of administration.
Over a third of the women in this study expressed concerns regarding their future fertility. This was more predominant in women who did not already have children and those under the age of 40 years. Van Kasteren and Schoemaker 8 reported a systematic review that assessed the reproductive outcomes of women with POI. The combined data of observational studies, both controlled and uncontrolled, showed that approximately 5–10% of women with POI achieved a spontaneous pregnancy at some stage after their diagnosis. Approximately 80% of these women had a healthy live-birth outcome, with a miscarriage rate of 20%, comparable to that in the general population. The mean age of the women included in the studies was 31–34 years, and the median age range within these studies was 31–35 years.
Egg donation, however, remains the realistic option for many of these women who wish to conceive,1,6 and alternatively adoption. 2 The implications of this choice are complex and can be multi-fold in terms of acceptance of not being able to have their own genetic child as well as cost, legalities and the processes associated with finding a suitable donor. Access to counsellors and fertility services thus becomes of paramount importance whereby the patient’s expectations can be appropriately addressed.
Developments in the field of Reproductive Medicine, however, have increased the potential fertility options, other than oocyte donation, for those at risk of developing POI. Oocyte or embryo cryopreservation is increasingly being offered to women prior to undergoing gonadotoxic therapy and may also be an option for women at risk of developing POI, such as those with a strong family history of POI. The live birth rates with the use of cryopreserved oocytes are improving but still remain lower than that for patients undergoing fresh in vitro fertilisation/intracytoplasmic sperm injection (IVF/ICSI) cycles. 9 Cryopreservation of ovarian tissue followed by auto-grafting 10 or in vitro culture may offer a valuable option in conserving fertility. However, its clinical application remains a challenge and more research is needed to assess this area. Cryopreservation of ovarian tissue holds the promise of providing a large pool of primordial and primary follicles for future use. 11 Cryopreservation of ovarian tissue followed by orthotopic transplantation is currently the only practical option available for pre-pubertal girls and women who cannot delay the start of their gonadotoxic treatment, with a handful of reported live births to date. 12 In vitro maturation of the oocytes may provide a more promising prospect, although this is not yet near clinical application and further research is needed to evaluate this area. 11
Li J et al. 13 reported on activation of dormant ovarian follicles with a PTEN inhibitor (Phosphatase with TENsin homology, deleted in chromosome 10) and a PI3K activating peptide thereby increasing the nuclear exclusion of the transcriptional factor Foxo3 from primordial oocytes. This has significant implications for women with reduced ovarian reserve and cancer patients in whom ovarian tissue can be cryopreserved. The same research group applied this principle to infertile women, whereby they removed the ovaries of 27 POI patients. They disrupted the Hippo signalling pathway, stimulated Akt signalling with drug treatments (PTEN inhibitor and PI3K activator), undertook auto-transplantation of the treated tissue and observed follicular maturation. Eight women showed signs of follicular growth. These patients then underwent ovarian stimulation with follicle stimulating hormone (FSH) and mature oocytes were collected from five patients. Intracytoplasmic sperm injection (ICSI) was then carried out, and this resulted in the birth of a healthy normal baby boy. 14 Further research is needed to assess the safety of these interventions and there is also a need to reproduce these findings in larger studies, but these findings can set the foundation for future research in this area.
In addition, a number of interventions have been applied to women with poor ovarian reserve and have now been extrapolated to women with POI. A randomised controlled study assessed the effects of dehydroepiandrosterone (DHEA) on ovarian response markers in 22 women with POI. 15 DHEA has been postulated to promote folliculogenesis and improve ovarian response to gonadotrophins. The study found that DHEA increased the antral follicle count after 16 weeks of treatment but had no significant effect on serum anti-Mullerian hormone and FSH levels. However, the study did not assess ovulation or pregnancy rates. The authors concluded that DHEA should not be routinely prescribed outside of a research setting until larger controlled trials have been conducted.
Studies have indicated that women of a younger age group may prefer the COCP over HRT. This choice may be secondary to peer pressure, and to avoid hormonal preparations that may be perceived to be associated with an older age group of women who enter a natural menopause. 16 It has also been reported that many young women prefer cyclical hormone replacement to induce regular monthly bleeding, creating some resemblance to normality. 17 Our study showed that most women had a preference for sequential HRT, with over half of women choosing HRT compared with less than 5% choosing the COCP. No patients over the age of 40 years opted for the COCP. Furthermore, of those opting for HRT, approximately three quarters of women ≤40 years of age chose a sequential regimen. However, these results may have also been influenced by the suitability of the patient to receive a continuous preparation, with women having less than 12 months of amenorrhoea being advised to take a sequential preparation.
More than two-thirds of women included in this review opted for an oral HRT preparation. Estrogen administered orally follows a first-pass hepatic metabolism pathway, with potential adverse effects on the coagulation cascade and pro-inflammatory markers such as C-Reactive Protein, compared to the transdermal route.18,19 Two large nested case-controlled studies that reviewed the United Kingdom's General Practice Research Database have shown a lower risk of stroke and venous thrombosis in naturally menopausal women between the ages 50 and 79 receiving transdermal estradiol compared to those receiving oral estradiol.20,21 However, there is a lack of evidence assessing the effects of the different routes of estradiol administration in women with POI, and further research is needed to assess this in this particular cohort of women.
Gallagher 22 reported a review of the literature on the effect of an early menopause on the risk of BMD loss and fractures. The review showed trends in a number of small studies whereby the rate of bone loss was more rapid in surgically oophorectomised women compared to naturally menopausal women, but the author was unable to draw firm conclusions in view of the small sample size of these studies. He concluded from the review that an early menopause before the age of 45 years could result in a reduction in BMD of approximately one T-score by 65 years of age, and recommended that women who experienced an early menopause, before 45 years of age, should undergo BMD assessment within 10 years of the onset of the menopause as they are at a greater risk of serious osteoporotic fractures. 22 Our data show a greater likelihood of women with POI developing reduced BMD the longer the time delay from presentation and diagnosis.
A retrospective analysis by Stavraka et al. 23 assessed bone demineralisation in gynaecological cancer survivors and noted that women with surgically induced menopause for gynaecological malignancies who received adjuvant chemotherapy had a greater degree of bone demineralisation than women with surgically induced menopause for benign conditions, with more than a third of the former group developing osteopenia and osteoporosis. 23 Our data, however, did not show a significant difference in bone density in women who had radiotherapy/chemotherapeutic interventions compared to those secondary to other causes.
In conclusion, most women in this review opted to take HRT in preference of the COCP, with the majority having a preference for oral estradiol within a sequential HRT preparation, but with a significant number of women over the age of 40 years opting to have estradiol administered transdermally. One-third of the women expressed concerns regarding their future fertility and this was more notable in women less than 40 years of age. The majority of women presented more than 12 months after the onset of menopausal symptoms and had normal BMD at presentation. However, there was an increased chance of the women presenting with reduced BMD the longer the time delay in presentation and diagnosis. These findings can be useful in counselling women and may help guide clinicians in their management of women with POI.
A Premature Ovarian Insufficiency International Database is currently underway. This aims to include clinical practice data from a large cohort of women with this condition from around the globe, with a view to improving the greater understanding of the current management practices of POI. 24 Research studies, like this one, will be brought together under a single framework and will allow a more evidence-based approach to clinical practice. This will provide useful information to guide the development of clinical guidelines in this field.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
How To Cite
Mittal M, et al. Fertility desires, choice of hormone replacement and the effect of length of time since menopause on bone density in women with premature ovarian insufficiency: A review of 223 consecutive new referrals to a tertiary centre. Post Reproductive Health 2014; 20(3): 104–111.