
Abstract
Voiding difficulties are more common in the elderly. This occurs because of physiological changes such as replacement of muscle fibres with collagen, from life effect insults such as the effects of childbirth, lead to a reduction in contractility and changes in the nerve supply from cholinergic to NANC fibres lead to a change in sensation leading to a delay in first sensation. Symptoms are often similar to those of overactive bladder and the history in older women should include those of hesitancy and poor flow. Likewise, the diagnosis should be considered in women presenting with recurrent urinary tract infections. A failure to consider voiding difficulties can precipitate a crisis and simple strategies such as teaching self-catheterization and using estrogen cream may prevent problems occurring. When acute problems occur, catheterization is required and a review of precipitating factors may identify medications contributing to the condition. The mainstay for treatment, however, remains draining with an indwelling catheter or clean intermittent clean catheterisation.
Introduction
Sub-clinical voiding difficulties occur commonly in the elderly but they are seldom considered when planning treatment for other conditions. Failure to recognize this potential may precipitate an avoidable crisis prior to treatment modalities such as elective or even emergency surgery.
Preventative strategies include treating other conditions such as constipation and those conditions that may contribute to voiding complications, such as atrophic vaginitis; treating these may help prevent problems but acute retention requires catheterization; attempts to improve voiding with alpha blockers and cholinergics have proven disappointing.
Bladder physiology and effects of distension
Bladder function requires an intact central nervous system and in particular an intact midbrain, pons and pontine micturition centre (PMC). The sensation of fullness is detected in the periaquaductal grey matter (PAG) which is activated prior to the PMC stimulation and this is often thought of as the ‘emotional control of voiding’.
The bladder is supposed to be a compliant organ with small pressure changes for a large change in volume. It spends 99% of its time in a storage function and 1% in voiding. Normal storage pressures run between 0 and 10 mm Hg with voiding pressures of up to 25 mm Hg.
Injury occurs when pressures above 10 mm Hg are enough to suppress bladder wall perfusion; if this occurs for extended periods the bladder wall is at risk of ischaemic change. Injury may also occur when the bladder is stretched past the normal elastic limit (plastic distension). The immediate effect is that the bladder then may not recover and fails to contract and empty properly. If managed immediately and carefully, this effect is almost always reversible.
Effects of bladder injuries
In the short-term, the effects of injuries on bladder function may be reversible as the bladder appears to recover; but these small injuries do result in change at a microscopic level. One consequence of this is an alteration in the nerve supply to the bladder making the muscle more sensitive to the neuro transmitters 1 in the nerve endings and also a change in the nerve type with a gradual change in the autonomic nerve supply from the usual adrenergic and cholinergic fibres of the sympathetic and parasympathetic nervous system to nonadrenergic noncholinergic (NANC) fibres that use a purinergic transmitter more commonly thought of as secondary messengers, such as ATP. 2
At the same time, the damaged detrusor muscle fibres are replaced with collagen. Collagen is a structural protein which, whilst depending on the degree of crosslinking may have flexible characteristics, but is not a muscle fibre and does not demonstrate the same ability to distend in a compliant manner as detrusor fibres or more importantly to contract. The net effect of this is that the bladder starts to lose the elasticity required for compliant distension and the loss of muscle leads to a net reduction in contractile force, so the ability to empty may reduce. These changes have been examined in animal models where the effects have been reproduced with a loss of the bladder’s ability to empty.3–5 To add insult to injury there is an even more subtle effect of reperfusion. Oxidative stress adds a second layer of injury onto the bladder; 6 this stimulates the bladder to produce nerve growth factor. This effect appears to be reduced after repeated insults 4 and this may be the driver for the change in innervation.
Effects of aging on the bladder and urethra
The combination of the events described above in small repeated insults over time – during events such as pregnancy and childbirth, or as a result of infections – results in delayed sensation and reduced capacity. The combination of these two changes produces a reduction in warning time due to disruption or reduced/delayed sensation in the bladder and reduced ability to distend hence losing capacity. These events may be critical in the development of urgency and urgency incontinence. Likewise, these factors can be compounded by the replacement of the muscle fibres with collagen and their effect on contractility leading to incomplete emptying and a reduction in the functional bladder capacity due to an increased residual urinary volume.
These effects are mirrored in the urethra, where a replacement of muscle fibres with collagen fibres makes the urethra less compliant. This change is seen as a reduction of the maximal urethral closure pressure (potentially increasing risk of ‘failure’ of the sphincter) and secondly a reduction in distensibility during voiding reducing the ability to distend and hence reducing the caliber and hence the urinary flow rate.
Impact of voiding dysfunction
Many women will have suboptimal voiding, but this remains subclinical until symptoms reach a tipping point. The implications for women are three-fold. Firstly, symptoms related to reduced flow, poor contractility and delayed/reduced sensation of frequency and urgency, poor stream, double voiding and nocturia. Secondly, difficulty with conventional treatment for urgency as the reduction in cholinergic fibres which may reduce the effectiveness of anticholinergics, whilst increasing side effects such as increasing urinary residuals. 7 Likewise, constipation, a known side effect from anticholinergic therapies may have an indirect effect on bladder emptying and irritative bladder symptoms and as such again reduces their effectiveness. Theoretically, the introduction of mirabegron, may confer some benefit in these patients having less impact directly or indirectly on voiding function.
The third issue is the sequelae of poor emptying such as urinary tract infections (exacerbated by atrophic vaginitis and constipation) which can be complicated by upper urinary tract infections and a subsequent effect on renal function.
Precipitating factors
In the elderly, a simple change in environment or circumstance may be enough to create disruption to either routine or habit. Many women avoid using public toilets which may lead to overdistension. Likewise, any condition affecting mobility can create problems with toileting and access to toilets.
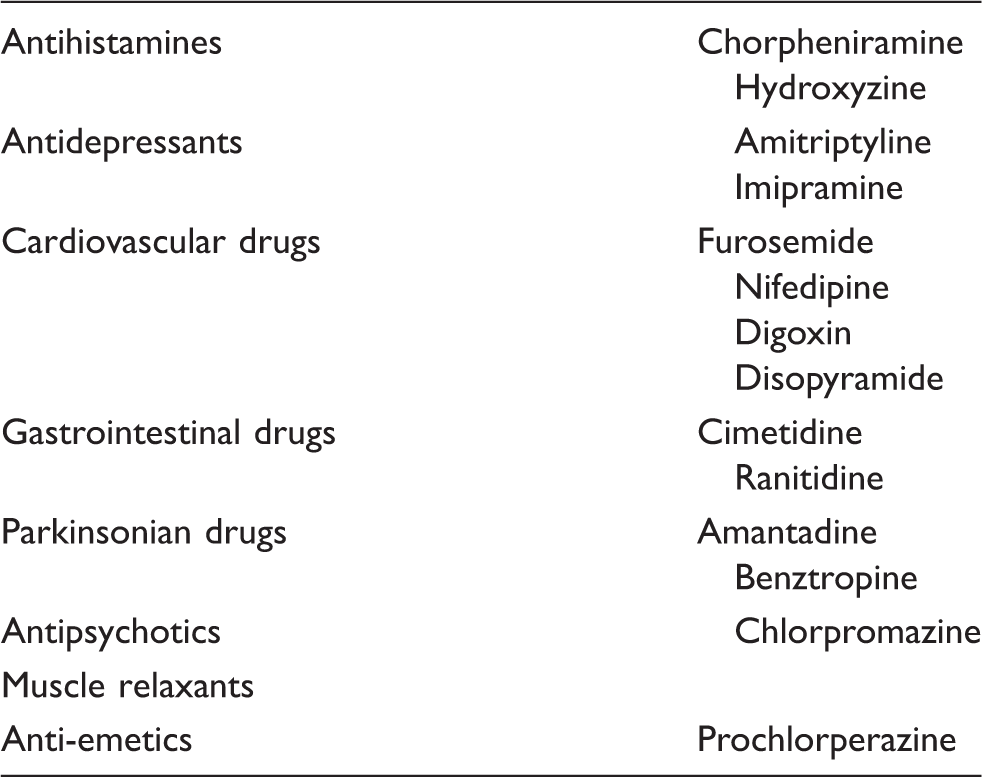
Drugs with anticholinergic effects.
Urinary tract infections may precipitate retention/voiding difficulties or alternatively be a sequelae of it. It is important to exclude this and send a sample for culture and sensitivity. The importance of microbiology becomes more relevant in chronic conditions and gives evidence as to whether infections are recurrent (as in frequently occurring) or whether they are resistant to clearance as a result of altered virulence, e.g. as part of a biofilm on a catheter or stone, or by becoming intracellular.
Voiding problems may co-exist with prolapse and occasionally present directly with bladder symptoms such as urgency or voiding difficulties, but more commonly sub-clinically to the more direct symptoms of a lump/bulge in the vagina. All patients presenting with prolapse should be asked about voiding function prior to surgery. If there is any doubt then the minimum of a post-micturition residual should be performed or in more complex cases urodynamics may be indicated. If poor voiding is identified then the option of a suprapubic catheter may be considered at the time of surgery.
Occasionally, the first presentation of other medical conditions will be bladder-related and in particular neurological conditions such as multiple sclerosis may present with voiding difficulties (although it more commonly presents as overactivity initially). Other conditions such as a CVA or diabetes can also present with loss of lower motor neurone (LMN) function.
Pelvic causes
Urethral stenosis is unusual in women but can occur especially if there is a history of untreated or delayed diagnosis of STDs (especially gonorrhea) or previous urethral surgery. Urogenital atrophy may also present with a distal urethral stricture at the meatus.
One should exclude pelvic masses causing anatomical distortion and this is easily done by an abdomino-pelvic examination.
Managing unexpected post-operative retention
Surgery is often a tipping point and may precipitate a loss of normal mobility meaning patients are unable to get to a toilet or sit normally, and secondly, finding the lack of mobility intimidating when having to use a commode. Pelvic surgery may disrupt normal function, due to a structural change (e.g. prolapse repair), or functionally with a disruption of the nerve supply (especially radical cancer surgery); in this situation there may well be a loss of normal voiding reflexes which coordinate normal micturition and disrupt the order of events in attempts to void.
More generally, surgery may impact on bladder function from anxiety and pain from the surgery and through localized bruising and swelling. Specific continence surgery may affect the bladder outlet, and intravesical onabotulinum toxin injections have been shown to reduce bladder contractility.
Unless specifically investigated, retention and sub-optimal voiding leading to deterioration in voiding function may be missed and may not be clinically an issue until after the patient is discharged. This is especially an issue with onabotulinum toxin, where the patient may be treated in an ambulatory setting and discharged on the same day, but potentially the effects may not be fully effective for up to 2 days.
Management is conservative with initial free drainage, with the option of a suprapubic catheter or intermittent self-catheterization (ISC) if required for longer term.
Self-catheterization can create a number of physical and psychological issues for women. These traditionally have had lip service paid to them and the physical need overshadowed any emotional sequelae. This is now subject to research 8 and certainly the support offered to women learning this skill has significantly improved in many units. Certainly, where the possibility of needing to learn clean intermittent clean catheterisation (CISC) is noted, then it is often better to teach women before reality. This means that women may learn the skill in a controlled environment rather than when they ‘feel as though the world is caving in’.
Generally speaking, CISC is preferred to suprapubic catheterization as it gives control back to the woman and allows her to dictate how and if the need to catherize impacts on her. Suprapubic catheterization can be used where there are physical impediments to CISC such as body habitus, reduced manual dexterity or visual impairment (although many of these patients may manage to catheterize or have a carer perform intermittent catheterization). Suprapubic catheterization is not without its risks. 9 Current NPSA guidance highlights the risk of bowel injury and the need for training with abdominal ultrasound to reduce any risk of bowel injury during insertion particularly under elective conditions.
Mechanisms of urinary retention after surgery
The effects of medications and especially analgesics/anaesthetics are often ignored. One study looking at the length of time it took for return of bladder sensation in postnatal women demonstrated effects of spinal anaesthetic for up to 12 h after Caesarean Section. 10
Loss of a co-ordinated sequence of voiding (dyssynergia) may occur as a result of neurogenic injury (disruption of the normal efferent and afferent pathways during surgery). Causes include iatrogenic (e.g. medications used in pain relief or with anticholinergic side effects) and psychogenic factors, such as the patients’ response to pain, fear or anxiety. Constipation may disrupt bladder emptying and pain may result in failure of the urethra to relax11–14 and sympathetic drive increase the sphincter activity on external sphincter (evidence of bladder contractions). 15 More directly, post-operative perineal pain may result in a failure to relax the pelvic floor as well as the inability to generate a detrusor contraction. 16 This increased sympathetic activity also offers an explanation of why cholinergic medications such as bethanacol are ineffective as the results in those with established voiding difficulties using these medications were poor. 17
Several studies have looked at the use of α-antagonists to try and assist the detrusor in contraction. These studies have been conducted in a variety of environments from gynaecology to orthopaedics and all have disappointing results with universally poor outcomes. The one placebo-controlled trial failed to demonstrate any difference. 18
Assessment of voiding dysfunction
Acute retention requires catheterization. Failure to catheterize results in bladder distension and further deterioration in detrusor function with associated damage to the nerve supply. One misconception is that if the bladder is not painful then the distension is not clinically relevant.
Managing expectation
Despite extensive research, urodynamics have consistently failed to predict voiding difficulties. The performance of the test provides an opportunity to discuss any identified pathophysiology and the likely impact of this. This process has been demonstrated to lead to better compliance with treatment regimens. 19
If voiding difficulty occurs after insertion of retropubic (or transobturator) slings during incontinence surgery, one must consider whether conservative or invasive management is most appropriate. Traditionally, most surgeons have had a conservative approach with either indwelling or intermittent catheterization, but more recently there has been a vogue for early intervention with a return to theatre and loosening of the tape. Direct evidence from cutting of these tapes suggests that there may be up to a 20% recurrence of symptoms. 20 Huwyler et al. 21 used these data for retrospective modelling and demonstrated that the excess failures may potentially occur with early intervention. Likewise, these authors demonstrated that less than 3% had long-term problems requiring tape lysis. In the authors’ unit, the normal post-operative management is conservative with an indwelling catheter for one week and then ISC or suprapubic catheter if the patient is unable or unwilling to do ISC. The indication for loosening of the tape is reserved for patients expressly not wanting conservative management or who are unable to void at all post-operatively. Loosening of the tape may be carried out up to around 10 days post-operatively. Likewise, discussing the differences in continence surgery between retropubic and transobturator 22 routes and possible voiding dysfunction may be appropriate in involving the choice of procedure where there is concern and where an obturator may just offer an advantage.
Onabotulinum toxin therapy has revolutionized the treatment of overactive bladder. Despite this as an effective therapeutic option, the RELAX study 23 found a fourfold increase in voiding difficulties over placebo with 16% vs. 4%. This rate is reduced by reducing the dosage of toxin used from the 200 i.u. (in the RELAX study) to 100 i.u. More recent unpublished data (from our own unit) suggest that voiding difficulty appears to be a consistent event with those experiencing this after the first injection often having problems after repeat therapy and extremely few ‘de novo’ voiding difficulties. Our unit now uses 100 i.u. as the first dose and increases to 200 i.u. if not effective. 24 The reduction in the voiding dysfunction is balanced against a slight reduction in the median return of symptoms.
Treatment
Whilst drainage of the bladder with an indwelling or intermittent catheter remains the mainstay of treatment, addressing the emotional and psychological sequelae or precipitating factors is also critical. The patients’ observations should be reviewed; treatment for pain should be ensured and should not be over treated because of the potential negative impact of opioids. Likewise, the regular medications and their side effects should be reviewed. Any infection or constipation should be treated. However, probably the most important is to have discussed the relative risks and likelihood pre-operatively, and the use of patient-related outcome measures as an individualized tool often allows the clinician to discuss the impact of such problems and allows them to gauge the appropriate treatment beforehand.
Conclusion
Voiding difficulties are more common with aging. Clues may often be in the history with symptoms of a poor stream and hesitancy or recurrent urinary tract infections. Treatment usually involves catheterization regimens and identifying precipitating factors such as anticholinergic effects of medications. Post-operatively, all aspects of care should be considered to identify factors associated with problems.
Footnotes
Auditable standards
BSUG database for surgery for prolapse and incontinence.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest
None declared