
Abstract
In the UK, breast cancer represents the most commonly diagnosed cancer in females and carries with it a significant morbidity and mortality. An established national screening programme is in place to identify those with the disease at an early stage in order to optimise treatment and prognosis. This article provides an overview for the non-breast specialist clinician whose practice regularly deals with women who may be the subject of the screening programme. It outlines the diagnostic methods employed in the screening programme, the controversies that have surrounded it and the evolving technologies that will improve detection and diagnostic accuracy.
Introduction
In the UK, 49,000 new cases of breast cancer were diagnosed in 2011 alone. 1 It is the second commonest cause of cancer-related death in women and it is estimated that a British woman’s lifetime risk of developing breast cancer is one in eight, or 12.5%. 2 The underlying causes of breast cancer are not fully understood; however, a number of genetic and environmental factors have been found to increase the risk of the disease, including BRCA 1 & 2 status, smoking, obesity, early menopause, alcohol, HRT therapy and a positive family history of the disease.3–6
Given its prevalence and incidence, an established national screening programme is in place as it is recognised that diagnosis of breast cancer at an early stage leads to a reduction in the mortality associated with the disease, and a better prognosis for the patient.7–9
In this review article, we will give an overview of the NHS Breast Screening Programme (NHSBSP) including the controversies that have surrounded it in the recent past, and offer a summary of the techniques and approaches employed in the diagnosis of breast cancer. The article will serve as a reference for the clinician whose primary specialty is not breast related, yet has a considerable female patient population who are invited to attend for breast screening.
Screening and diagnosis
The purpose of screening for a disease is to ‘advance the time of diagnosis so that prognosis can be improved by earlier intervention’. 9 The test, or group of tests within a screening programme, must ideally meet a set of standards which include being of low cost, high yield, reliable and acceptable to the population due to be screened. 10 No test is 100% sensitive and specific for the disease it is trying to detect. The individual undergoing screening must be fully informed of this prior to participating in any programme of screening, so that they may make an informed decision regarding their participation. 11
History of the programme and its current form
The NHS Breast Screening Programme was developed following a report into breast screening published by Professor Sir Patrick Forrest in 1986. 12 The UK programme began in 1988 inviting women between the ages of 50 and 64 to be screened with the acquisition of a single mammographic view of each breast. Today the programme invites women aged 50–70 years old for two mammographic views of each breast 13 every three years with the invitation for the first screening round (prevalent screen) sent shortly before the woman’s 50th birthday. 14 Screening women at less than three yearly intervals has not been shown to provide any real benefit in cancer diagnosis or mortality. 15
Not every woman who is invited for screening actually takes up the offer to attend with national screening coverage around 70% annually. 16 For the year 2011/2012, the programme screened 2,261,942 women, an increase of nearly one million women since 1996/1997 17 and at an annual cost of £96 million pounds. 18 There are 80 screening units based in the UK, the locations of which vary with some being based at a local hospital and other services provided by mobile units. For the year 2011/2012, there were 18,745 cancers detected of which 61% were diagnosed in screened women between the ages of 50 and 64. 17
If a woman accepts the invitation to screening she attends the screening unit and undergoes two view mammography of each breast, at different projections, craniocaudal (CC) and mediolateral oblique (MLO), thus giving four mammographic images in total. Examples of the four images obtained are detailed in Figure 1.
A standard set of screening mammograms. From right to Left: RMLO; LMLO; RCC and LCC.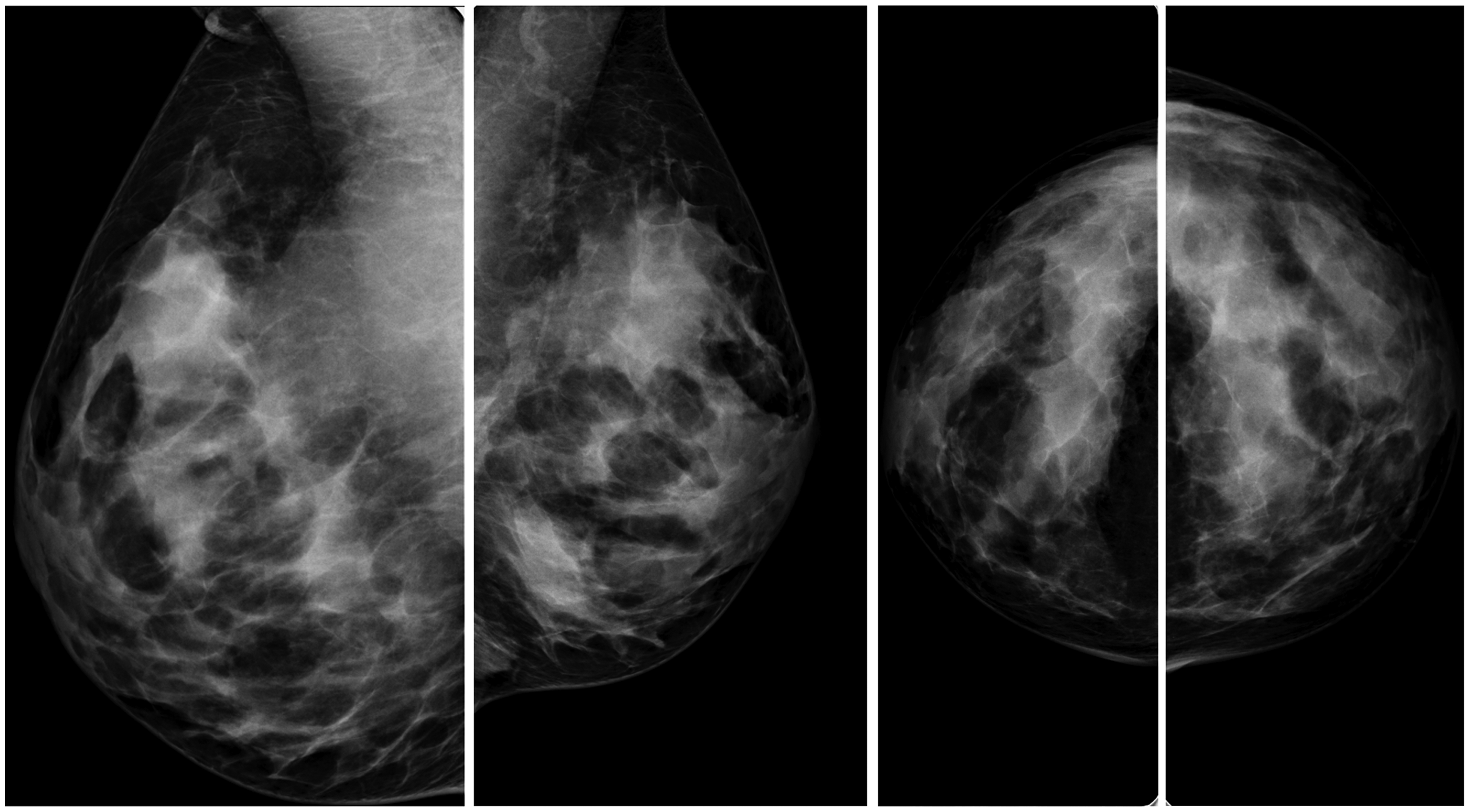
Compression is used to make the layers of breast tissue thinner. This allows the X-ray exposure to be reduced and makes the image sharper. It also aids in reducing summation artefact, which is the presence of composite shadows giving rise to a pseudo mass.
Spray deodorants and the use of talc should be avoided on the day of the mammogram as they can cause artefacts on the film. 19
Once acquired, the mammograms are subsequently read by two trained screen readers, independent of one another to avoid bias. The screen readers may be a consultant radiologist or a sub-specialist breast radiographer who has undertaken further training in mammography film reading. The utilisation of non-consultant screen readers has developed due to a critical shortage in the number of trained breast radiologists nationally. 20
The screen reader inputs their interpretation electronically onto the national screening programme database, a tool that forms a major part of the overall quality assurance programme. Should a discrepancy arise between the two film readers, that is to say one reader detects an abnormality and the other does not, then the mammograms are assessed again by a third reader or a local arbitration panel. This is a process within the breast department which consists of multiple readers assessing the films together to come to a consensus decision on whether the abnormality warrants a recall of the patient for triple assessment. The time taken from image acquisition to the time the woman receives her screening result should be no longer than two weeks. 14 If the woman is recalled, either due to a technical abnormality on the film or for triple assessment of a mammographic abnormality then this should occur within three weeks of the initial mammogram.
The vast majority of women attending for screening will receive a letter informing them that no abnormality was detected at that time and that they will be invited for a further screen in three years. The letter also reminds them that should they become suspicious of an abnormality before their next screening appointment they should see their GP. If an abnormality is detected on the screening mammograms the woman is asked to attend for further assessment which utilises mammography, ultrasound and clinical assessment in order to determine whether it actually represents true pathology. Of the total number of women called for screening in a single screening around approximately 5% will be recalled for assessment. 21 The number of women recalled who are attending for their first mammogram (prevalent screen) is usually higher than those attending for subsequent rounds 22 as there are usually no previous studies for comparison. However, the numbers should not exceed 10% for first time attenders, or 7% for those having subsequent mammograms in further rounds. 14 As most women called for screening are ‘well’, a rigorous process as described above must be adhered to before calling a woman for further assessment as this carries with it significant anxiety and psychological distress. 23 The time interval between a recall for assessment and the actual clinic appointment is kept as short as possible for this reason, and should ideally not exceed one week in duration.
The assessment clinics are run by a multidisciplinary team and are usually led by a breast radiologist. These clinics work in close collaboration with breast surgeons, breast care nurses and specialist breast physicians.
At the assessment further specialised mammograms can be obtained to assess for artefacts and an abnormality can be assessed and potentially biopsied under ultrasound, X-ray, or MRI guidance for those cases demonstrated only on this imaging modality. If at the time of dynamic assessment, it is felt the lesion may represent a cancer the axilla is routinely examined with ultrasound to identify and facilitate biopsy of any suspicious lymph nodes. Core biopsies of a lesion are preferred to fine needle aspiration as they provide a histopathological diagnosis, as opposed to cytological assessment. 24 Obtaining tissue for histology allows accurate tumour typing, assessment of its invasiveness and immunohistochemical analysis for hormone status. The findings at triple assessment may be discussed with the patient at the time, especially if there is a suspicion that the lesion is malignant. This is ideally done in the presence of a breast care nurse specialist. Research has found that a transparent approach and forewarning of the possible outcome allow women more time to come to terms with the potential diagnosis and provide for a more favourable psychological outcome. 25
The results from assessment are discussed at the breast multidisciplinary meeting preferably before the woman has been informed of the outcome so that a treatment plan can be established and then discussed with her at the results appointment (Figure 2).
An overview of a woman’s journey through the screening programme.
Women at high risk
All screening programmes must take account of those individuals within a population whose risk of developing the screened disease is considerably greater than that of the index population. In these instances, age of entry into the breast screening programme is different and women are screened from an earlier age, usually having being identified as high risk by a geneticist, oncologist or via a family history clinic within an oncology department. As a result, other imaging and assessment techniques such as MRI may be utilised. The breast of a young woman is made up of a large amount of glandular tissue, which on conventional mammography is of a high density thus rendering the accurate assessment of the breast for a subtle lesion extremely difficult. MRI overcomes this problem by employing multiple sequences to optimise subtle differences in soft tissue and utilises dynamic contrast enhancement characteristics to further characterise the biology and significance of an abnormality (Figure 3).

Although screening for high-risk women is well established, screening for those with a moderate family history of the disease is not. There is some evidence to support screening between the ages of 40 and 49 in this particular group of women 28 ; however, this is not included in the NHS Breast Screening Programme.
Controversies in NHSBSP and the programme’s impact
The breast screening programme has not been without its critics and there has often been polarised debate regarding the actual impact it has on cancer survival, with a number of authors suggesting that it does not reduce breast cancer mortality in women and potentially causes harm due to over-diagnosis and subsequent treatment.29–31
Over-diagnosis of a breast cancer is defined as a tumour ‘that would never have clinically surfaced in the absence of screening’. 32 That is to say that a cancer is present within the breast; however, its biology and characteristics render it such that it would not have any impact upon the patient during their lifetime. Detection of this innocuous cancer, in the vast number of cases, will result in the same outcome as for other screen detected tumours which is curative surgery with the possibility of further therapies. These treatments are unnecessary as the tumour would never be a problem; however, the woman will still be subjected to them. Treatment of a cancer results in increased morbidity both secondary to the treatments administered and the psychological burden experienced by the patient. 23
In 2012, the independent breast screening report (IBSR) was commissioned, following the publication of a number of reviews questioning the efficacy of breast screening. Professor Sir Michael Marmot was commissioned by Professor Sir Michael Richards, the then National Cancer Director for the UK, and Dr Harpal Kumar, CEO of Cancer Research UK, to assess the benefits and harms of population breast screening programmes. 9 None of the members of the panel had previously worked or published in breast screening. They carried out an extensive review of the literature and heard evidence from a large range of experts. 33
Comparison of public health interventions.
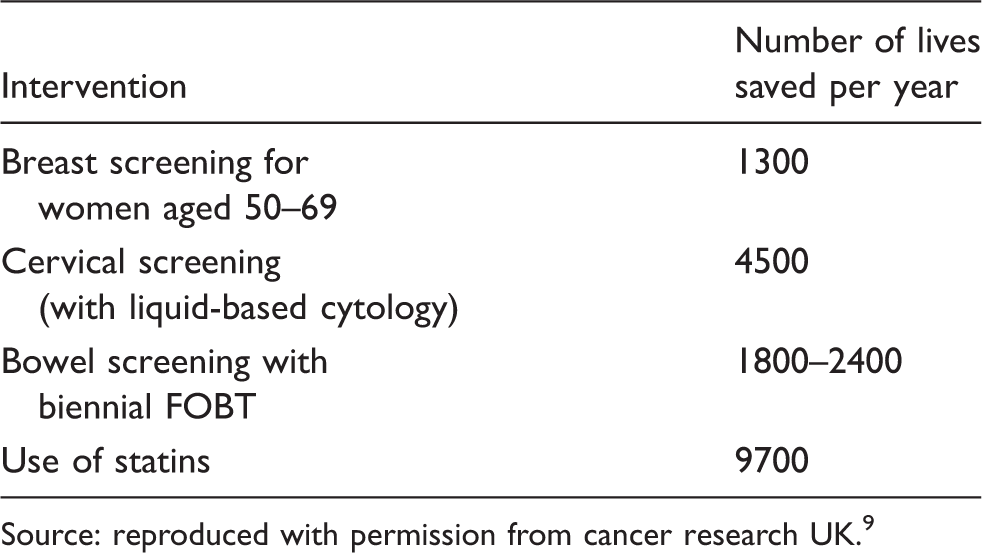
Source: reproduced with permission from cancer research UK. 9
The panel also estimated the rates of over-diagnosis and the potential harm caused to the patient as a result. It suggested that for a woman who takes up the offer of screening, and attends each round of screening over the 20 years of the programme, should she be given a diagnosis of cancer there is a 19% risk that this will represent an over-diagnosis. Put another way, of the approximately 307,000 women aged 50–52 invited to screening each year, just over 1% would have an over-diagnosed cancer during the subsequent 20 years of the screening programme.
Future developments
Randomised controlled trials are currently underway assessing the potential for extending the age range of women included in the breast screening programme, from the current 50–70 to 47–73 years old. The trials will take some time to complete as outcomes are being assessed over the course of two three-year screening rounds. 34
Technology, pathology and tumour biology are constantly evolving and new methods for breast cancer detection, diagnosis, staging and treatment are continually improving. New diagnostic techniques are being evaluated to improve tumour yield and reduce over-diagnosis.
Chief amongst them is the development of digital breast tomosynthesis (DBT), a technique utilising multiple projections of the breast in different planes. This reduces the effect of summation artefacts upon the image, which are composite tissue shadows that can either hide a lesion or create the impression of a pseudo mass. Initial data have suggested improved sensitivity and specificity for detecting breast carcinomas through the use of DBT35,36; however, this comes at the cost of a greater time required to assess the mammograms and a small increase in radiation dose when compared to conventional mammography.
Another method being investigated is the use of a single mammographic view, acquired at a specific time interval following the administration of an intravenous contrast agent. By splitting the images by the photon energies (high or low energy) suspicious lesions can be unmasked and made more prominent. 37 This technology may replace breast MRI for some clinical indications.
Given the vast number of screening mammograms to be reviewed over the course of each year and the time investment needed to do this accurately, other methods of mammographic assessment have been evaluated including the utilisation of computer-aided diagnosis (CAD). In trials assessing the technology similar sensitivities and specificities in diagnosis have been reported when comparing a traditional assessment by two film readers with a single human reader aided by CAD. 38
Molecular imaging techniques including diffusion-weighted MRI and MRI spectroscopy are being evaluated to improve tumour staging and prognostication based on tumour biology profiling prior to surgical removal of the cancer.39,40
As methods of diagnosis and detection improve, so too do the treatments offered. Chemotherapeutic agents and combinations thereof alter and become more efficient, new hormone therapies emerge and novel surgical approaches are currently being evaluated. These include percutaneous laser and high-frequency ultrasound ablation41,42 treatments, which will potentially turn some breast-tumour surgery into day case procedures performed under local anaesthetic.
Further research is underway 43 into tumour biology and its natural history so that those cancers, which are indolent and which will never be clinically significant may be identified, thereby ensuring those women are not treated unnecessarily.
Conclusion
Breast cancer represents a significant cause of morbidity and mortality amongst women and despite controversies surrounding the breast screening programme, the programme’s importance and impact in reducing breast cancer deaths have been established with the benefits of early treatment outweighing the risk of harm secondary to over-diagnosis.
As with any test, or set of tests, it will never be 100% accurate and the risk of over-diagnosis can result in psychological and physical harm to the women affected. Critically, this information must be conveyed to the woman as she embarks on her screening journey so that she may make an informed decision regarding her participation.
The programme will continue to form a cornerstone of our approach to breast cancer diagnosis and with the implementation of new technologies will yield ever greater numbers of cases, at earlier stages of the disease, with the hope that this will reduce deaths from breast cancer even further.
Footnotes
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.