
Abstract

Introduction
In June 2013, NICE (National Institute of Health and Clinical Excellence) recommended women at moderate or high risk of breast cancer due to their family history, have opportunity to discuss the use of the Selective Oestrogen Receptor Modulators (SERMs) tamoxifen or raloxifene if risk-reducing surgery and surveillance was unsuitable or unacceptable. 1 Despite the estimated significant impact in reducing the risk of breast cancer diagnosis in this population cohort, uptake and adherence to chemoprevention in routine clinical practice remain very low. 2 An important impediment is patient and healthcare professional concern about treatment side effects, which are all associated with changes to estrogen activity. 2 An added consideration, not fully explored by the 2013 NICE guidance and still unresolved, is which clinical specialities should have responsibility for counselling, prescribing and monitoring chemoprevention when neither tamoxifen nor raloxifene are licensed for this indication in the UK. GPs and clinicians working in family history or clinical genetics settings appear to have many issues relating to this. 3 Noticeable in its absence from the NICE guidance and debate surrounding improving implementation of chemoprevention is the potential role menopause specialists could have given they are best placed to advise about the management of estrogen-related side effects. This review summarises current recommendations surrounding breast cancer chemoprevention in the UK with the intention of highlighting aspects of care relevant to gynae-endocrine practice.
SERMS and breast cancer chemoprevention trials
In the 1980s, the results from large randomised adjuvant treatment trials of tamoxifen in women with early breast cancer reported a significant reduction (∼35%) in the risk of diagnosis of contralateral breast cancer. 4 The main adverse effects of an increased risk of diagnosis of endometrial cancer and thromboembolic events were uncommon and considered sufficiently low to support initiation of four placebo-controlled randomised tamoxifen chemoprevention trials in higher risk healthy women. 5 To determine whether it was a safer alternative to tamoxifen in the chemoprevention setting due to a known anti-estrogenic effect in the breast and lack of an estrogenic effect on the endometrium, breast cancer events were evaluated with exposure to raloxifene in placebo-controlled trials in postmenopausal women who had either osteoporosis, risk factors for coronary heart disease and in a direct head-to-head randomised chemoprevention trial with tamoxifen.6–8 Initial overview of the main outcomes from these trials confirmed a significant reduction in the risk of diagnosis of estrogen receptor positive (ER+ve) but not estrogen receptor negative (ER−ve) breast cancer, and tamoxifen was confirmed to be equally effective in both pre and postmenopausal women. 5 Both tamoxifen and raloxifene were associated with an increased risk of venous thromboembolic events. 5 Subsequent meta-analysis of all randomised chemoprevention trials utilising SERMs showed the beneficial reduction in diagnosis of ER+ve breast during the active treatment phase (i.e. 5 years) continued following treatment cessation and that the risk reduction with tamoxifen in postmenopausal women was greater than that observed in women allocated to receive raloxifene (38% vs. 27%, respectively). 9 Longer term follow-up has shown the ‘carry-over’ benefit with tamoxifen to be associated with a reduction in the risk of breast cancer diagnosis for at least 20 years. 10 As most side effects stop with tamoxifen cessation, this has favourable implications for tamoxifen’s overall risk-benefit ratio. Other SERMs (i.e. lasofoxifene, arzoxifene) are still subject to evaluation as potential chemoprevention agents as are aromatase inhibitors. The latter are associated with a greater reduction in the risk of diagnosis of contralateral, ER+ve breast cancer risk compared with tamoxifen in adjuvant treatment trials but at the expense of arthralgia and increased fractures. 11
The recommendations about chemoprevention in the 2013 NICE familial breast cancer guidance (NG164) was based on review of nine studies (two systemic reviews of randomised trials, five randomised controlled trials, one case series and one qualitative study) out of a total of 132 assessed to be relevant and of sufficient clinical quality using GRADE methodology and NICE checklists. The Guidance Development Group (GDG) concluded overall, the harm from iatrogenic side effects with tamoxifen and raloxifene (i.e. endometrial cancer, thromboembolic events, fractures and stroke) was outweighed by the potential benefit in reducing the risk of breast cancer diagnosis. 1
Aromatase inhibitors were not recommended for chemoprevention as at the time of the NICE review, the only randomised study to differentiate between the different aromatase inhibitors was considered too low quality for clinical recommendations to be made despite a significant (65%) reduction in the diagnosis of ER+ve cancer with exposure to exemestame.1,12 Subsequent to the NICE guidance, anastrozole has been shown to reduce the diagnosis of ER+ve breast cancer by 58% after a median follow-up of five years compared with placebo. 13 In both trials, women experienced significant vasomotor symptoms and arthralgia. Anastrozole was also associated with significant vaginal dryness, joint stiffness, carpel tunnel syndrome, hypertension and dry eyes. 13
NICE CG164: Recommendations for clinical practice 1
The following summarises the key recommendations of the GCG:
Women at higha and moderateb risk are considered eligible for discussion of chemoprevention for a maximum of five year’s duration.
For high-risk women, the evidence of benefit is sufficiently strong to outweigh potential harms or side effects so ‘chemoprevention should be offered’. For moderate risk women, the balance of evidence between benefits and risks is less certain but it would be inappropriate to prevent access so ‘chemoprevention should be considered’. Tamoxifen should be offered to, or considered in premenopausal women for five years. Tamoxifen should be offered to, or considered in postmenopausal women who have had a hysterectomy for five years. Tamoxifen or raloxifene should be offered to, or considered in postmenopausal women with a uterus for five years. Tamoxifen and raloxifene are not recommended for women at high risk of breast cancer who have had bilateral mastectomy. Inform women that they should stop tamoxifen at least:
Two months before trying to conceive (there is a lack of any data regarding potential teratogenic effects). Six weeks before elective surgery due to the small associated risk of thromboembolic events.
aWomen at high risk include those confirmed to have a cancer-predisposing gene mutation (e.g. BRCA1, BRCA2, TP53) or more than a 30% lifetime risk of breast cancer based on their family history.
1
bWomen at moderate risk have between a 17% and 30% lifetime risk of breast cancer based on their family history. 1
Presenting the risks and benefits from chemoprevention
NICE recommends discussion and provision of written information including absolute risk estimates associated with breast cancer and non-breast cancer outcomes to ensure appropriate individualised advice. However, neither the 2013 guidance nor a further up-date in August 2015 provided any such information, instead presenting risk ratios and percentage changes, which are open to misinterpretation.
1. Breast cancer diagnosis and breast cancer mortality
Absolute reduction in breast cancer diagnoses with five years’ treatment with tamoxifen.
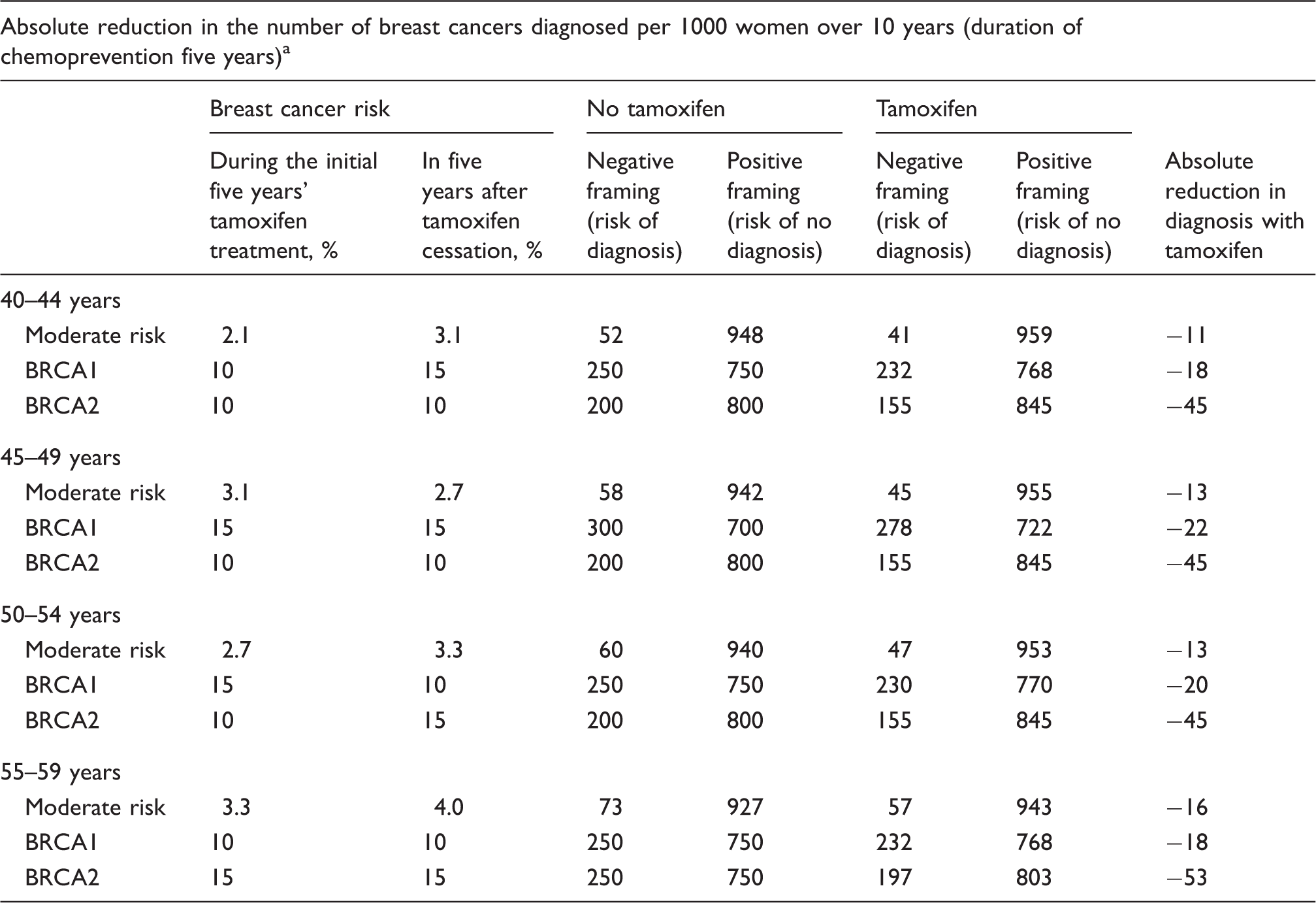
Estimates are based on following assumptions. (1) ∼75% of breast cancers diagnosed in women at moderate risk and BRCA2 mutation carriers are ER+ve and 25% of cancers in BRCA1 mutation carriers are ER−ve. (2) The risk reduction with five years’ tamoxifen treatment is 38% and the risk reduction in the five years following cessation of tamoxifen is 22%. (3) Five-year breast cancer risk for moderate risk women is based on a fourfold increase in baseline risk and calculated using the Gail risk model. 15
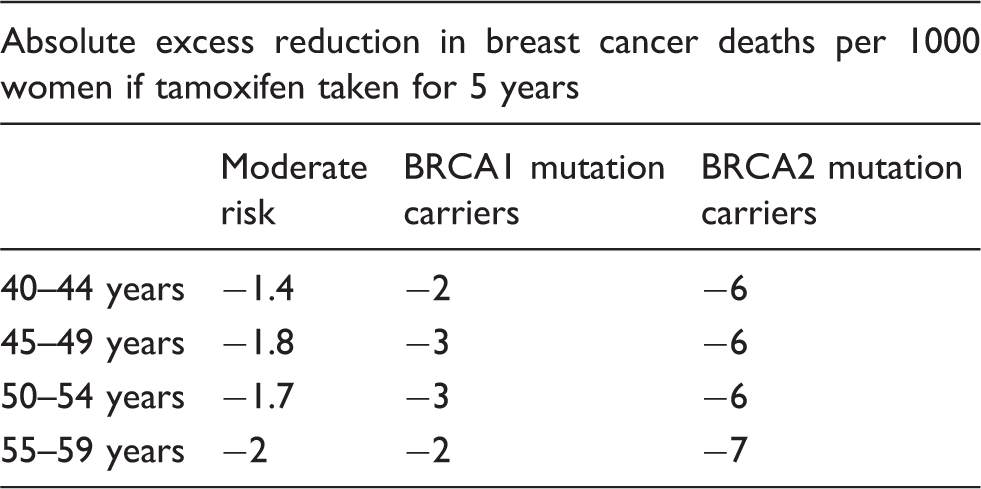
Estimated absolute reduction in breast cancer deaths with five years’ treatment with tamoxifen.
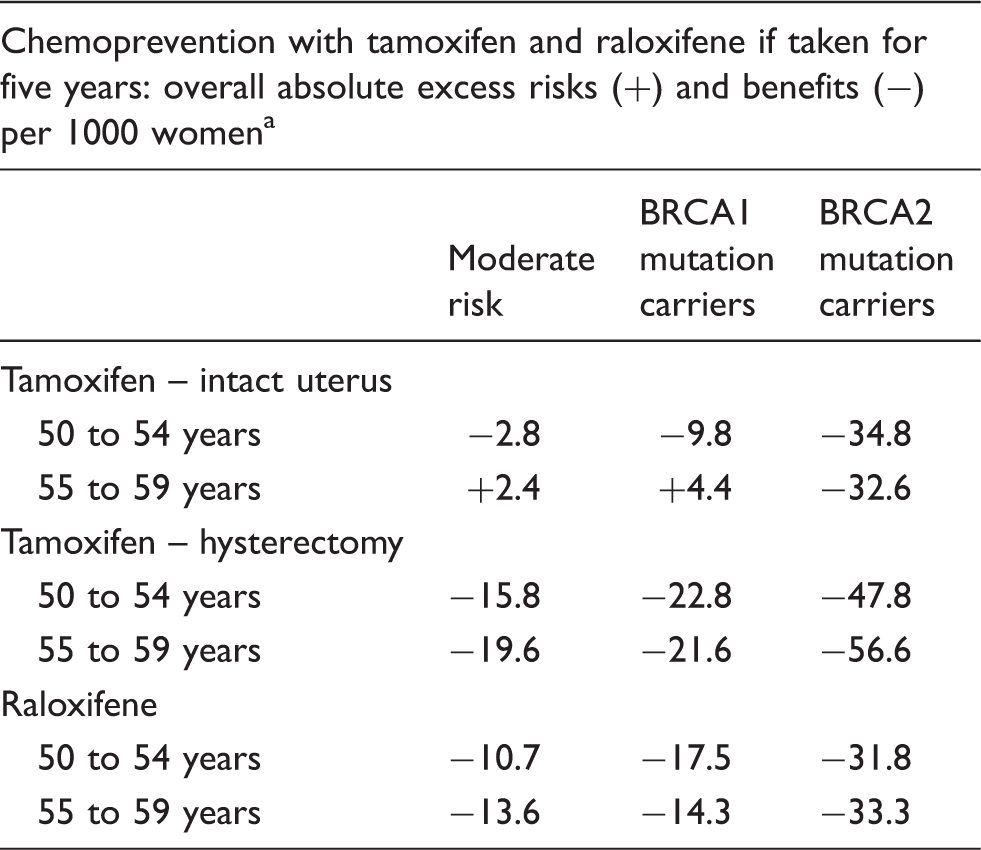
2. Non-breast cancer side effects and outcomes with tamoxifen and raloxifene
Tamoxifen and raloxifene; potential risks and benefits.
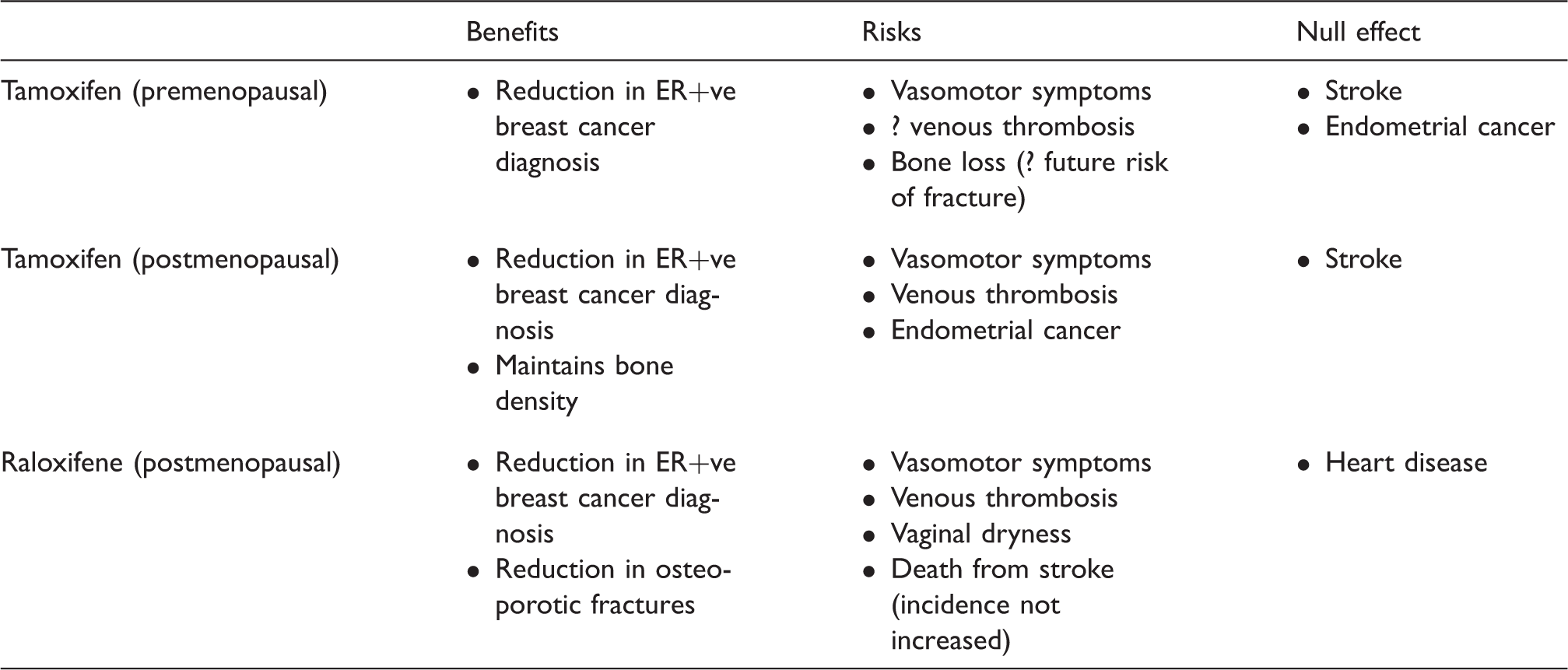
Vasomotor symptoms and vaginal dryness are common side effects with both drugs. Hot flushes are worse with tamoxifen and vaginal dryness with raloxifene. 21 Randomised tamoxifen chemoprevention trials that permitted the concomitant use of hormone replacement therapy (HRT) for symptom relief have not reported an increased risk of breast cancer diagnosis but as the observed reduction was less compared with the use of tamoxifen alone, it would be counter-intuitive to prescribe HRT in this context.10,22
Tamoxifen and absolute number of health events in pre and postmenopausal women.
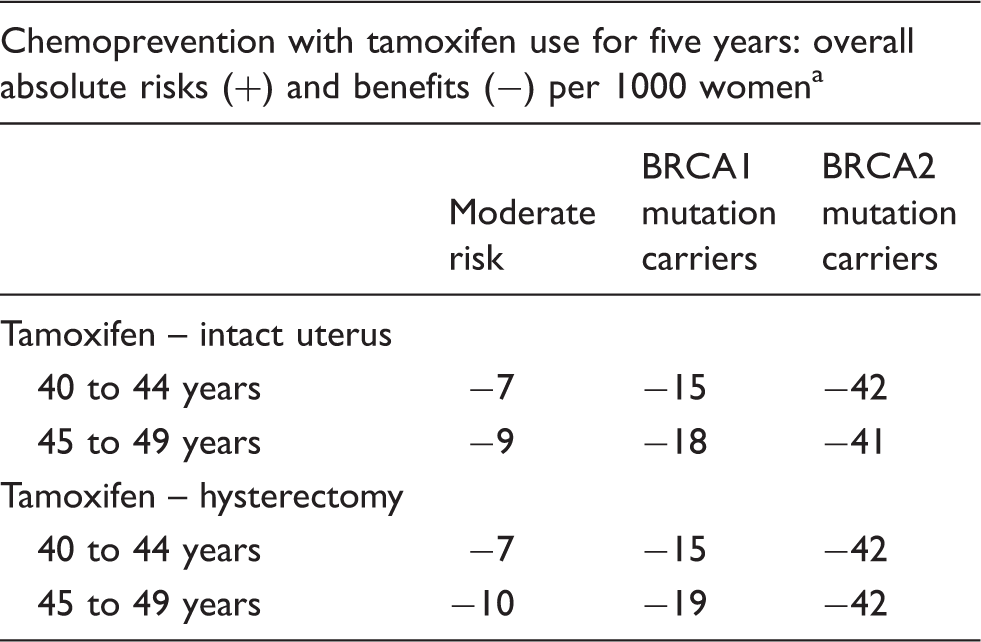
Tamoxifen and raloxifene and absolute number of health events in postmenopausal women.
Patient uptake of and adherence to chemoprevention
Both uptake and treatment adherence need to be high for chemoprevention to impact on breast cancer diagnosis. NICE assumed their recommendation for chemoprevention would have a significant impact on clinical practice with an estimated an uptake of 25%. 1 However, this has not been the case. In the UK and elsewhere, less than 10% of eligible women agree to do so. 2 The most consistent reason identified appears related to unfavourable perception of risks and benefits and side effect management in the absence of access to HRT. 2 Adherence data from women participating in clinical trials, where continuance rates are anticipated to be higher than in a non-clinical trial setting, show a decline over time. 2 In only one study did more than 80% of women persist with treatment by five years. Poor treatment continuance is associated with use of tamoxifen rather than raloxifene, smoking, depression and older age. 2
Who should have responsibility for counselling, prescribing and monitoring chemoprevention?
It is recommended that only healthcare professionals within a specialist genetic clinic should discuss and provide written information about chemoprevention and its absolute risks and benefits to women at moderate and high familial risk. 1 However, the current organisation of and demand for UK specialist genetics services means generally only patients at high familial risk are offered an appointment in such clinics. This raises the issue of where moderate risk women should be counselled and by whom. Even in the specialist clinic setting, clinicians admit to difficulty in interpreting the NICE guidance, particularly if their perception of chemoprevention benefit is low and in primary care, GPs appear to have less awareness of chemoprevention and the issues surrounding it use. 3 Regardless of where counselling takes place, the complexity of discussion required potentially will involve significant time commitment. At the time of publication of the NICE guidance, neither tamoxifen nor raloxifene had a UK license for chemoprevention of breast cancer and to date, they still do not. Therefore, the healthcare professional who discusses and prescribes chemoprevention has full responsibility for this and has to obtain documented informed consent. It is unsurprising therefore GPs appear reluctant to initiate prescriptions, preferring to continue a prescription originating in secondary or tertiary care. 3
Little clinical guidance was provided by NICE about monitoring treatment other than promoting attendance for breast cancer surveillance and referral of women in the event of development of post-menopausal bleeding. 1 As GPs admit to a low level of awareness and knowledge about chemoprevention, it can be questioned whether follow-up in primary care is optimal as things stand. However, other options are limited in that specialist genetic clinics are not set up to provide on-going review of medication and breast clinics need to focus their increasingly limited resource on the diagnosis and treatment of women with cancer. Given the side effect profile of SERMS, pathways should be developed that utilise expertise of and support from menopause specialists.
Summary
There are still outstanding questions regarding the risk-benefit implications of current chemoprevention strategies for hormone-responsive breast cancer. Even if all were resolved, in clinical practice, initiation and monitoring treatment requires ability of involved health professionals to provide reliable information about breast and non-breast cancer outcomes and strategies for their management as appropriate. Most issues are related to changes in estrogen activity and are beyond the expertise of many GPs, health professionals in family history or clinical genetics clinics or surgeons in breast clinics and require menopause expertise. Given the recent NICE menopause guidance recognised the importance of menopause specialists in the management of symptomatic breast cancer patients, 26 it is hoped that similar recommendation will be made in the next familial breast cancer guidance up-date, which is scheduled for publication in March 2017. If not, health professionals involved in providing gynae-endocrine services should take the initiative. The author will provide a summary of the up-dated NICE guidance for the Journal of Post Reproductive Health following its publication.
Footnotes
Declaration of conflicting interests
The author is on the counsel of the British Menopause Society and British Association of Day Surgery and was the chief investigator for the UK randomised trial of HRT in symptomatic women with early breast cancer. In the last year, the author has presented two lectures sponsored by Mylan.
Funding
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Guarantor
JM.
Contributorship
JM is the sole contributor.