
Abstract
Hot flushes and generalised sweating are relatively common presenting complaints, with hypogonadism an important differential diagnosis in both sexes and menopause being the most typical cause in females of climacteric age. However, a variety of other conditions do need to be carefully considered in respect of eugonadal individuals and also for those hypogonadal ones where properly dosed sex steroid replacement has failed to control flushing and sweating, or where the presentation is atypical. Alternative aetiologies may be immediately obvious from the history and physical examination, but more unusual conditions may require deeper scrutiny. This clinical review elaborates on the non-menopausal endocrine and non-endocrine causes of flushing and sweating, including both common and rarer conditions.
Background
There is a paucity of robust epidemiological studies on the frequency and aetiologies of flushing and sweating, partly explained by the different routes via which patients with similar symptoms come to medical attention, and also due to the difficulties in defining flushing and sweating in lay terms in respect to pathological frequency and chronicity. As such, the generalist’s experience of managing flushing and sweating will undoubtedly be at variance with the selective group of patients with persistent symptomatology of unclear aetiology referred to endocrinology. Nevertheless, hot flushes and generalised sweating are common presenting complaints to both the general physician and the endocrinologist. Although most commonly associated with the menopause in the female of typical climacteric age, a variety of causes need to be carefully considered in both sexes. Some of these may be obvious from the presenting history and physical examination, but others require more careful elucidation. To the gynaecologist, an atypical presentation, or failure to control flushing and sweating in peri- and post-menopausal females achieving adequate serum estradiol levels on hormone replacement therapy (HRT) should trigger a scrutiny for alternative aetiologies.
Aims
This clinical review aims to elaborate on the various non-menopausal causes of flushing and sweating, some of which are directly relevant to the gynaecologist. We will use a real clinical case to initiate discussion of the various possible endocrine and non-endocrine causes and their investigative strategies. This paper will not cover infective and malignant conditions which can present with sweating, nor the detailed management of each specific cause.
Introduction to clinical case
A 24-year-old female was referred from her GP to our out-patient endocrine department with a few months’ history of flushing and sweating. Her symptoms had appeared within months of receiving a contraceptive implant (Nexplanon® – Etonorgestrel 68 mg in radio-opaque flexible rod), which had also resulted in amenorrhea – about which she was extremely pleased. Systemic enquiry was unremarkable. She was a non-smoker, drank no alcohol and denied using any prescribed, or non-prescribed drugs.
Differential diagnoses
Possible endocrine causes of sweating and flushing with diagnostic clues from clinical assessment and suggested screening tests.
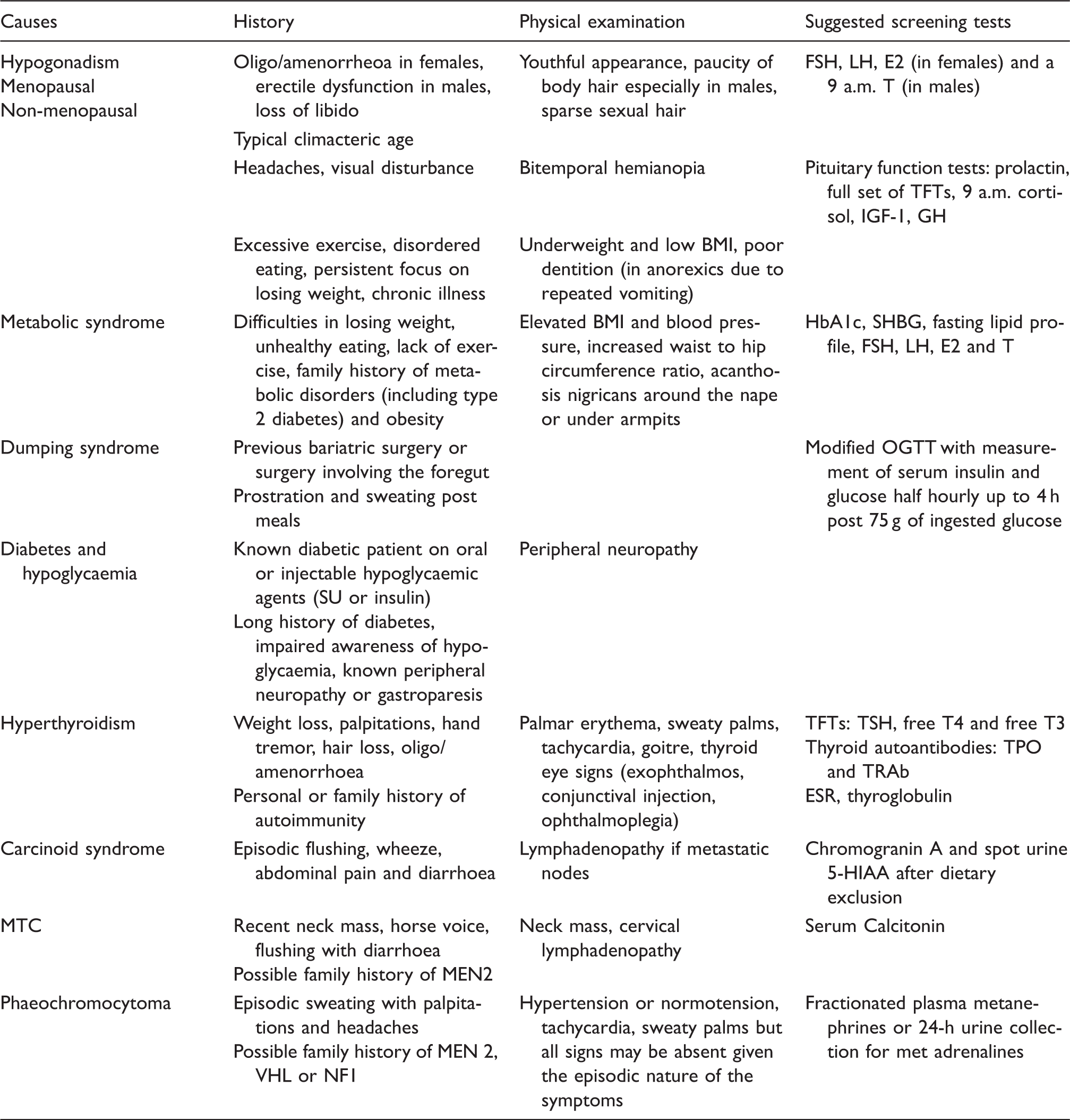
FSH: follicle-stimulating hormone; LH: luteinising hormone; T: testosterone, TFT: thyroid function tests; IGF-1: insulin-like growth factor 1; GH: growth hormone; BMI: body mass index; HbA1c: glycated haemoglobin; OGTT: oral glucose tolerance test; SU: sulphonyl urea; TSH: thyroid-stimulating hormone; free T4: free thyroxine; free T3: free triiodothyronine; TPO: thyroid peroxidase antibody; TRAb: TSH-receptor antibody; ESR: erythrocyte sedimentation rate; MTC: medullary thyroid cancer; MEN 2: multiple endocrine neoplasia type 2; VHL: Von-Hippel Lindau; NF1: neurofibromatosis type 1.
Possible non-endocrine causes of flushing and sweating.
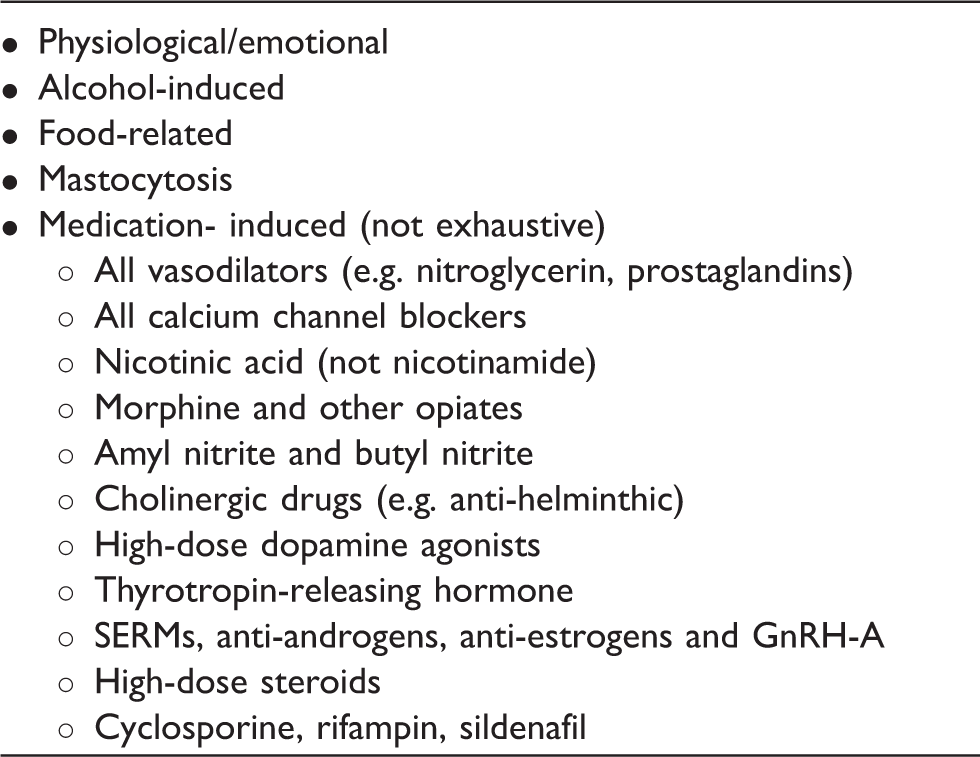
SERM: selective estrogen receptor modulator; GnRH-A: gonadotropin-releasing hormone analogue.
Hyperthyroidism or thyrotoxicosis is a commonly encountered endocrine cause of these symptoms, with up to 90% of patients presenting with heat intolerance and sweating. 1 Other associated symptoms include hair loss, palpitations, hand tremor, anxiety and oligo/amenorrhoea in fertile females. Hyperthyroidism can be endogenous (autoimmune, inflammatory or autonomous) or exogenous (secondary to thyroxine over-replacement or surreptitious use of thyroid hormones for weight loss). These causes and their frequency vary across the sexes, the populations studied and the age spectrum. 2 As such, autoimmune hyperthyroidism is more commonly seen in young females, whereas autonomous thyroid nodules are more common in older women.
Hypogonadism is an under-recognised cause of flushing/sweating in both sexes. It may be physiological (the transition through menopause in females) or pathological – failure of the gonads to secrete adequate levels of sex hormone due to an insult to either the gonads or the hypothalamo-pituitary gonadal axis. Episodic sensation of heat, sweating and flushing may typically last a few minutes, occurring repeatedly throughout the day and night.3,4 The diagnosis of physiological hypogonadism (menopause) is usually clinical and based on females of climacteric age (around 51 years) presenting with typical symptoms of flushing and sweating. 5 The detection of a low circulating serum estradiol (E2) level combined with elevated serum FSH levels clinches the diagnosis, but is not recommended routinely and this combination of findings may anyway be absent during peri-menopause. 6
Secondary hypogonadism, where gonadotropins are low or inappropriately normal, may present in a variety of ways, most notably with cessation of periods in females and hypogonadal symptoms in males (impotence, loss of libido and bodily hair, but also sweating, flushing, or normocytic anaemia). Parasellar lesions can cause pressure symptoms, with headaches and peripheral visual field loss, and/or features of pituitary hormone hypersecretion (growth hormone-IGF1 axis in acromegaly; ACTH-cortisol axis in Cushing’s disease, or much more commonly prolactinoma). Although females with parasellar lesions typically present early due to cessation of menses, this effect is initially masked in women taking combined oral contraceptives. In acromegaly excessive growth, hormone production from the pituitary gland is associated with persistent sweating (both eccrine and apocrine) and greasy skin. In retrospect, there may be evidence of altered physical appearance over many years, with coarsening of features, prognathism and increasing shoe or ring size.
The human hypothalamo-pituitary gonadal (HPG) axis is sexually dimorphic in its responses to bioenergetic deficit and excess (e.g. underweight and overweight respectively). In females, bioenergetic deficit (e.g. over-exercise/eating disorder or unintentional malnutrition) can result in physiological HPG axis suppression (hypothalamic amenorrhoea), for which there is an obvious evolutionary basis as well as a potential genetic-environment interaction. 7
The male HPG axis is far more resistant to bioenergetic deficit, but is uniquely susceptible to both bioenergetic excess (obesity) and corticosteroid excess (i.e. endogenous or iatrogenic Cushing’s syndrome). By contrast, females with obesity or corticosteroid excess tend to express ovarian hyperandrogenism, rather than HPG axis-suppression. 8
Increasingly sweating is being associated with the metabolic syndrome in our clinics. With the change in lifestyle behaviour in the western world, a growing proportion of the population is developing obesity and its associated metabolic complications including diabetes or a pre-diabetic stage. Obesity (in males, but not females) has been associated with down-regulation of the hypothalamo-pituitary gonadal axis resulting in secondary hypogonadism – sweating being a symptom thereof. 9 In addition, the state of pre-diabetes, impaired glucose tolerance, or even very early stage Type 2 diabetes is characterised by a diminished “first phase” insulin secretory response to oral loading with glucose or mixed meal, with preserved second phase response.10–12 There is thus the potential for unregulated release of endogenous insulin to cause transient, minor hypoglycaemic episodes with associated sweating in susceptible individuals with metabolic syndrome ±obesity. 13 A more pronounced syndrome of sweating and prostration is recognised following surgery involving the foregut (including bariatric gastric bypass procedures), resulting from the uncoordinated release of endogenous insulin from the pancreatic beta-cells, well after the peak of glucose influx from the intestines: referred to a post-prandial hypoglycaemia. Classically, patients report excessive sweating and dizziness within hours post meals commonly referred to as dumping syndrome.
Diabetic patients on the other hand may experience hypoglycaemic symptoms from insulin or its secretagogues (e.g. sulphonyulreas) – an effect potentially exacerbated by exercise, alcohol intake, or missed meals. The adrenergic symptoms (palpitations, tremor, sweating) of acute hypoglycaemia are usually easily identified by the diabetic patient, but those with long-standing diabetes and known autonomic neuropathy may only experience neuro-glycopaenic/cognitive symptoms (e.g. confusion, irritability, reduced responsiveness) and nocturnal sweating.
Other rare endocrine causes of sweating include carcinoid syndrome, medullary thyroid cancer and secretory paraganglioma. Patients with carcinoid syndrome classically report episodic flushing, sweating, wheeze and abdominal pain followed by diarrhoea, sometimes triggered by the ingestion of alcohol, chocolate or beef. Various secretory products, including serotonin, prostaglandins and histamine, from the altered metabolism of tryptophan in carcinoid tumours have been implicated in the range of clinical manifestations. 14 Carcinoid syndrome commonly occurs once neuro-endocrine tumours (NET) of the small or large bowel have metastasised to the liver, but can also occur in primary bronchial NETs, where it is commonly also associated with bronchospasm. 15
Medullary thyroid cancer (MTC) is a rare neuro-endocrine malignancy of the C cells of the thyroid gland causing excessive calcitonin production. It may occur sporadically or follows an autosomal dominant inheritance as part of multiple endocrine neoplasia 2 (MEN2). In the latter case, patients may report a positive family history for hyperparathyroidism, phaeochromocytoma, and/or MTC. Secretory paragangliomas are catecholamine-producing tumours of the adrenal medulla (phaeochromocytoma) or sympathetic ganglia. Patients may report episodic sweating associated with headaches, palpitations, and sustained or paroxysmal hypertension. 16 Patients may report a family history of paragangliona, multiple endocrine neoplasia 2, neurofibromatosis type 1 or Von-Hippel-Lindau syndrome.
Sweating with flushing can also result from intake of alcohol, certain foods and a wide range of prescribed and abused drugs. Alcohol or its metabolite, acetaldehyde, can directly vasodilate the blood supply to the skin. Ethnic Asians with a deficiency of an isoenzyme of liver aldehyde dehydrogenase develop extensive flushing in response to relatively low amount of consumed alcohol, due to elevated serum concentrations of acetaldehyde. 17 Flushing due to food ingestion is common, but may rarely also be the presenting feature of an underlying endocrine condition. 18 Although foods containing capsaicin (spicy), or preservatives (sodium nitrate or sulphites) can particularly cause flushing or sweating per se, these symptoms may also indicate underlying secretory NET or paraganglioma (see above). Mastocytosis is a rare disorder of non-neoplastic mast-cell accumulation, whereby release of vasoactive mediators such as histamine through explosive degranulation occurs in response to environmental triggers, including spicy food, alcohol, certain medications, infections and physical factors. 18
Drugs that can cause flushing and sweating are listed in Table 2. 19 This is by no means an exhaustive list since many more medications have hyperhidrosis listed in their rare side effects profile. Nevertheless, psychiatric and opioid medications are common culprits and obtaining a reliable history of prescribed and OTC medications from the patient is paramount. A temporal relationship from the start of the culprit medication and the development of symptoms may sometime be ascertained from the history but not always. Hence, medication-induced sweating and flushing are mostly a diagnosis of exclusion, and in clinical practice, a diagnostic trial of stopping the offending drug can be a useful and rewarding one for the patient. The mechanisms involved in medication-induced sweating and flushing differ across the spectrum. For instance, cholinergic-agonists directly stimulate the sweat glands and hydralazine and nitroglycerin vasodilate the dermal vasculature.
Importantly, hypogonadism-associated vasomotor symptoms can occur with drugs predisposing to central HPG axis suppression – such as gonadotropin-releasing hormone (GnRH)-analogues in the treatment of prostate cancer, opiates and (via hyperprolactinaemia-effect) dopamine-antagonists – or peripheral antagonists of sex hormone action, such as cyproterone acetate, selective estrogen receptor modulators (tamoxifen, raloxifene, clomiphene – used in relation to breast cancer, osteoporosis and infertility).
Physical examination and diagnostic tests
The physical examination can provide important clues to the possible underlying cause of sweating and flushing as elaborated in Table 1. The BMI importantly may point to the metabolic syndrome or secondary hypogonadism from being severely underweight. Hypertension may be present in phaeochromocytoma or in obesity. Bilateral hand tremors and sweaty pink palms are harbingers to hyperthyroidism. Large pituitary lesions can present with visual anomalies detected as bitemporal hemianopia on confrontational testing with red object. Importantly, combining key history and examination findings will help rationalise and focus diagnostic testing.
Our patient’s body mass index (BMI) was 26 kg/m2; blood pressure 130/75 mmHg and pulse rate 70 beats per minute. Visual fields were full and the general physical examination, including cardiovascular and cutaneous, was unremarkable. However, her laboratory indices revealed HPG axis suppression: serum LH 0.8 IU/L (2.0–12 IU/L), FSH 1.4 IU/L (2.0–9.0 IU.L) and Estradiol 80 pmol/L. Pituitary function was otherwise normal, as were her full blood count, liver function tests, urea and electrolytes and thyroid function tests. We attributed her symptoms of flushing and sweating to secondary hypogonadism, induced by her contraceptive implant. The high systemic level of progestogen, via inhibition of gonadotropins, resulted in a relative estrogenl deficiency. The therapeutic options available to her are to either replace the Nexplanon® with Mirena® IUD (levonorgestrel-releasing intrauterine device) or add back oral or transdermal estradiol aiming to achieve a serum estradiol level in the 300 to 500 pmol/L range. It should be noted that Nexplanon® is not licensed to prevent estrogenic stimulation of the endometrium so that consideration would also have to be given to the addition of endometrial protective progestogen, leading to a complicated regimen if continuing with use of Nexplanon®.
Conclusion
Flushing and sweating, though commonly associated with the climacteric phase in females, are also present in the non-menopausal population. These symptoms should be seriously investigated given that they may be associated with malignancies or infectious diseases. However, other benign aetiologies are numerous and only a thorough clinical assessment can help direct diagnostic testing and subsequent management. In the absence of flushing and when no cause is found, a diagnosis of idiopathic hyperhydrosis is contemplated.
For the gynaecologist dealing with menopausal women, consideration should be given to the possibility of other pathologies accounting for sweating and flushing, especially if symptoms fail to improve with conventional HRT. However, it should also be recognised that current practice in relation to hormone replacement in hypogonadal females is remarkably loose in terms of choice of hormone and whether any monitoring of serum estradiol levels is performed, 6 compared with the situation in hypogonadal men, or even in gonadectomised transgender women. 20 For instance, the WHO has long mandated the use of native testosterone rather than synthetic androgens for sex hormone in men, and doses are individualised according to objective parameters, including serum testosterone levels, haemoglobin/haematocrit, patient’s symptoms and bone densitometry. For transgender women, replacement therapy is with native 17, betaEstradiol (E2), with serum E2 levels monitored as to achieve levels in the upper half of the late-follicular normal range. By contrast, young hypogonadal cis-gendered women are typically offered unmonitored fixed-dose preparations, sometimes comprising of xenoestrogens (e.g. conjugated equine), or a synthetic estrogen-analogues (ethinylestradiol) as part of combined oral contraceptive regime, wherein hypogonadism recurs one-week-in-four, due to unreplaced estrogen during their breakthrough period.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Contributorship
Vikram Lal and Yaasir Mamoojee contributed equally to manuscript writing, Richard Quinton contributed to manuscript review and corrections.