
Abstract
Musculoskeletal pain, arthralgia and arthritis are all more common in women, and their frequency increases with age and in some appears to be associated with the onset of menopause. The clinical assessment, investigation and management of women presenting with musculoskeletal pain, arthralgia or arthritis at the time of menopause are reviewed. Common causes of arthralgia and arthritis in this population are discussed. The epidemiological and trials evidence for the effects of hormone replacement therapy on musculoskeletal pain and arthritis (primarily from RCTs of HRT for other menopausal symptoms) are discussed. Lastly, the possible underlying aetiological roles of sex hormones including estrogen, and their deficiency, in predisposing to musculoskeletal pain and arthritis are overviewed. Although the association appears strong, a causal link between estrogen deficiency and musculoskeletal pain or different types of arthritis is lacking; there have been few studies specifically within this group of symptomatic patients, and there is much still to understand about musculoskeletal pain and arthritis at the time of the menopause, and about how we might prevent or treat this.
Introduction
Chronic musculoskeletal pain represents an enormous health burden, affecting over 50% of adult populations. Common sites of pain are the spine, knee, hand, hip and shoulder.1,2 There is a female preponderance irrespective of the cause of the pain.1,3,4 At the time of menopause, musculoskeletal pain is reported by more than half of women. 5 Presentation with joint pain in women is greatest between 45 and 55 years of age. 6 Although this appears to implicate the menopause and estrogen deficiency, direct causal evidence of a role for menopause is lacking, partly because musculoskeletal pain is so common throughout life. Women are approximately twice as likely to have joint pain and stiffness around the time or after the menopause than their premenopausal counterparts, when adjusted for age.5,7 However, many such epidemiological studies do not differentiate musculoskeletal pain from arthritis, so assessing the burden of arthralgia and arthritis in these populations is difficult.
Arthralgia is a subjective term, describing pain in a joint or joints. The implication is that this does not cause harm to the joints and is quite separate from arthritis, which refers to an underlying pathological process within the joint associated with clinical symptoms but also signs. It is imperative to consider early arthritis, or another underlying inflammatory rheumatic disorder in anyone presenting with joint pain. However, patients experiencing arthralgia around the time of menopause often do not have or develop an associated arthritis. The pain may be associated with hormonal changes at this time, or other secondary reversible conditions which are important to exclude. 8 In this review, the clinical approach to the peri- or post-menopausal woman with joint pain will be set out, including investigations and management. Possible pathogenetic factors in the development of musculoskeletal pain in relation to the menopause will be discussed; the evidence for the effects of hormone replacement therapy (HRT) in this setting and areas with lack of evidence will be highlighted.
Clinical assessment of the menopausal patient with joint pain
Causes of musculoskeletal pain in the perimenopause.

IBS: irritable bowel syndrome.
Causes of arthralgia in menopausal women.
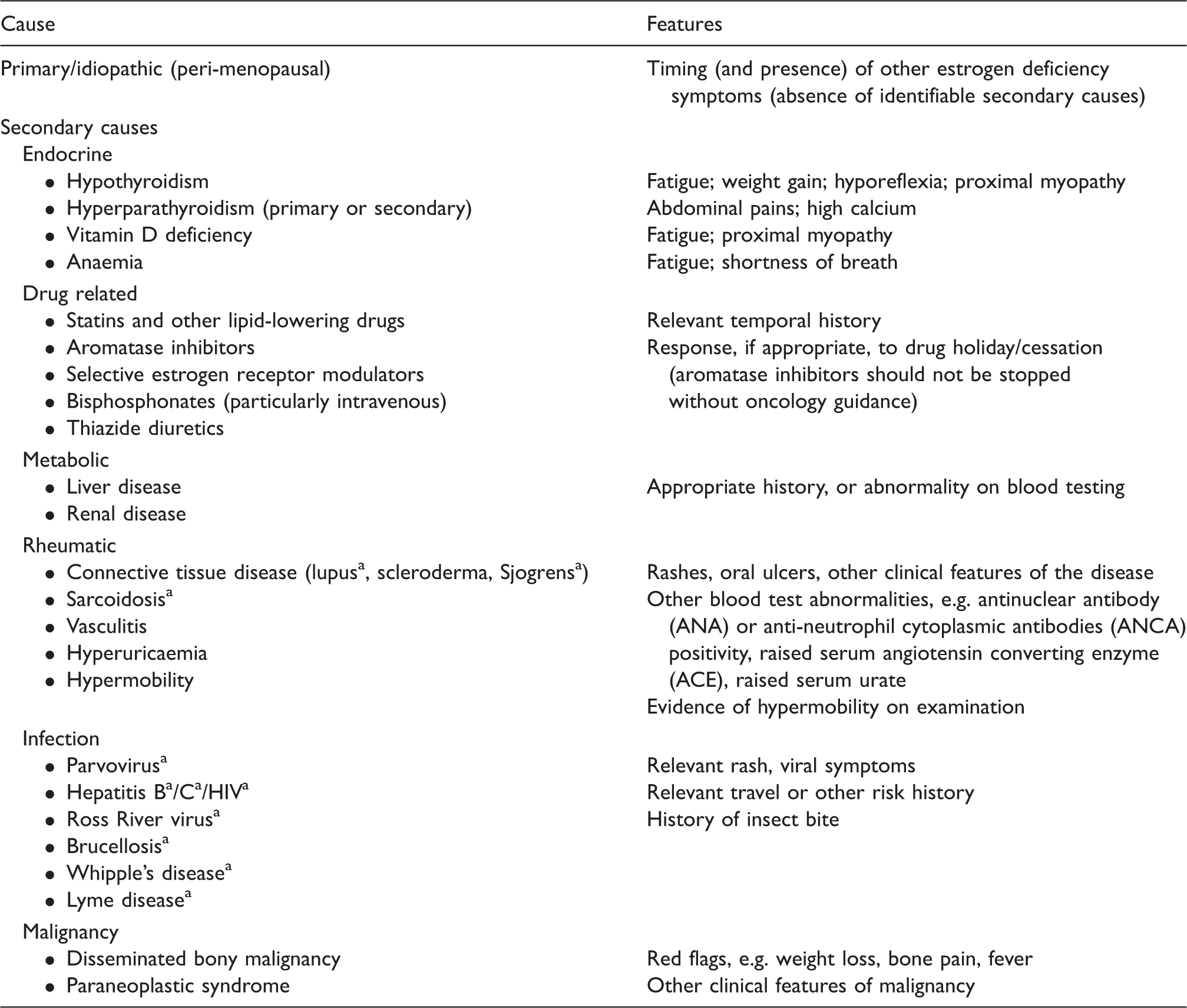
May be associated with arthralgia or a frank arthritis.
Differentiating features of arthritis: the ‘3 S’ approach.
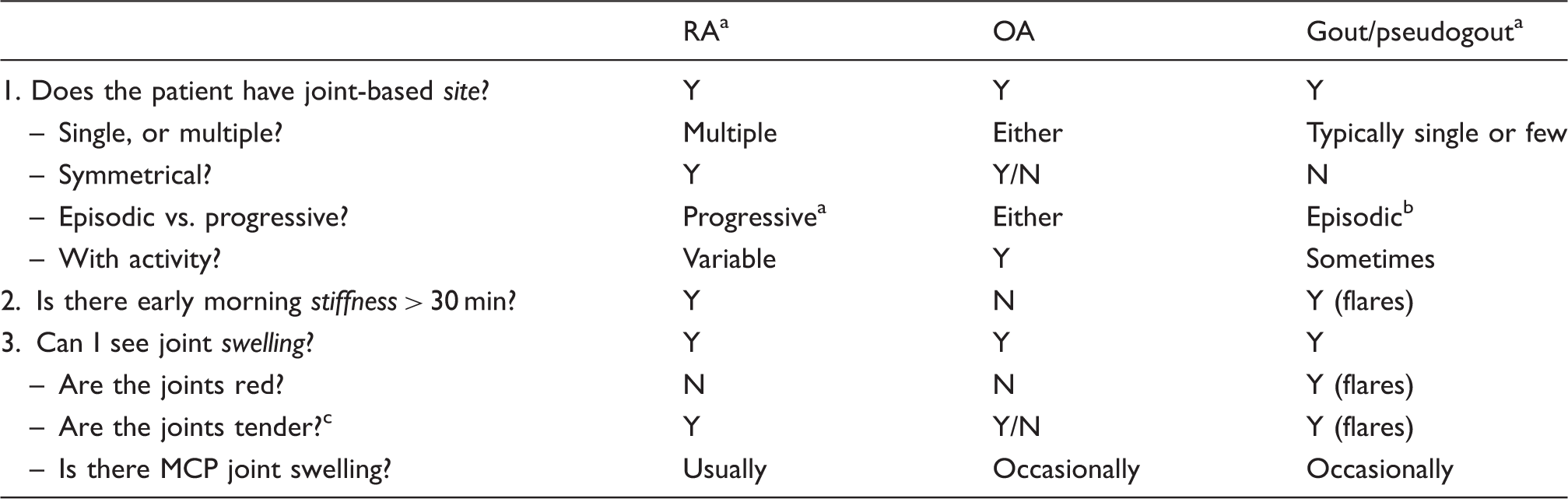
RA Early, established disease (rarely palindromic RA can occur, with episodes of flare and remission.
Gout. Based on new presentation of gout. Established, tophaceous gout can give persistent pain, and progressive arthritis.
Tenderness is usually present in arthritis, but not always in arthralgia.
Investigation of the patient with polyarthralgia or arthritis
Laboratory investigations for polyarthralgia and arthritis.

CRP: C-reactive protein; ESR: erythrocyte sedimentation rate.
Autoantibodies may be positive in the absence of inflammatory arthritis. Only request these tests in the context of symptoms and signs of inflammatory arthritis.
General management
Features suggesting rheumatoid arthritis.

Note: Adapted from Aletaha et al. 9
In the case of arthralgia, the likely cause should be identified as far as possible (Table 2) and management with the aim of improving pain instituted. Identification of a possible drug cause for arthralgia needs careful discussion between the patient, physician and other relevant healthcare professionals, taking into account the effects on quality of life, and the relative risks and benefits of staying on the drug versus reducing drug dose, switching to another drug within the same or different class or simple cessation. Statin-induced myalgia or arthralgia is actually extremely uncommon (other causes of pain should be actively sought); if suspected on temporal grounds, the risk benefit of reducing or stopping the drug should be carefully discussed and documented, prior to either drug holiday, cessation or class-switching.
Common forms of arthralgia occurring in perimenopause
Menopause-associated arthralgia
Arthralgia is a menopausal symptom in at least 50% of women (musculoskeletal pain is one of the most commonly reported symptoms in international populations).10–13 In this situation, by definition no secondary cause has been found.
Clinical features
Usually pain is not the main menopausal symptom, but part of a wider syndrome. However, it is the predominant symptom in 21% of women. 5 Arthralgia and muscle pain of any origin is often associated with fatigue, mood change, sleep disturbance, raised body mass index (BMI), anxiety or stress. 14 Given that these features are also frequently also associated with menopause, they can have both a potentiating effect on the presence of arthralgia and be compounded by its presence. Menopause-associated arthralgia is typically transient and self-limiting and may not present to a physician, but may be a source of persistent pain for a minority of women, or evolve into arthritis or chronic widespread pain in susceptible individuals. For this reason, persisting arthralgia should be intermittently reviewed to ensure no change in the diagnosis.
Management
There is little evidence for the optimal management of menopause-associated arthralgia. General advice for musculoskeletal pain is to control weight (with planned weight loss where BMI is raised) and to take regular exercise. This can be both aerobic and joint specific. There is some evidence that moderate levels of physical activity improve peri-menopausal arthralgia and other menopause-related symptoms. 15 If there is deconditioning evident, a graded and gradual increase in exercise should be planned, avoiding sudden overloading of painful joints, which may exacerbate pain and cause loss of confidence and adherence. Avoidance of heavy lifting or repetitive joint use, for example in hand arthralgia, is often helpful.
Supportive treatment should also aim to improve symptoms of stress, anxiety or depression and sleep quality (if sleep disturbance is present). Again, there is little or no trial evidence in this setting, although good evidence in related conditions such as fibromyalgia. 16 Dietary measures aiming to regulate estrogen levels may help improve arthralgia. A recent controlled clinical trial showed that a complex intervention which included dietary and exercise supervision reduced arthralgia. 17 The use of supplements such as phytoestrogens, evening primrose oil, starflower oil, fish oils or ginseng are reportedly used by 32% of post-menopausal women for non-vasomotor symptoms including arthralgia. 18 These agents may be helpful in controlling menopausal symptoms but there is a lack of evidence for their effects, specifically on arthralgia.
Where pain is persistent and moderate to severe, a regular analgesic such as acetaminophen may be required. It should only be continued if found to be effective. Non-steroidal anti-inflammatory drugs (NSAIDs) may be helpful either topically or orally in managing persistent symptoms unresponsive to acetaminophen, although there is a lack of evidence for this specific setting. Sparing use and monitoring of oral agents are advisable because of potential gastrointestinal, renal or cardiovascular toxicity.
Current indications for systemic HRT are vasomotor and gynaecological menopausal symptoms not responding to local or conservative therapies. Joint pain and stiffness were noted to be modestly reduced in the active arms of RCTs including WHI (76.3% vs. 79.2%, P = 0.001) 19 and an Australian RCT. 20 Epidemiological studies in this area are conflicting, as many patients may seek HRT because of musculoskeletal symptoms. 21 If arthralgia is severe and persisting, unresponsive to other measures, temporally related to menopause, where quality of life is impaired and particularly in the presence of other incapacitating menopausal symptoms, it may be reasonable to discuss whether HRT could be tried. Patient-reported measures of pain and menopause symptoms and their change should be recorded.
Aromatase-induced arthralgia
Aromatase inhibitors used in the management of breast cancer in this group are a particularly common cause of arthralgia, which may be seen in as many as half of users. 22 If medically required and where there are no reasonable alternatives, active management of arthralgia symptoms may be necessary to maintain therapy. 23 Mild arthralgia should be treated symptomatically with lifestyle advice including exercise and weight loss, and response documented. For more severe symptoms, treatment with an oral analgesic such as acetaminophen or NSAID should be offered to enable continuation of therapy (risk-benefit of NSAIDs/coxibs should be carefully considered). Any decision to modulate, switch or change a drug should always be made by the treating oncologist. Switching to an alternative agent within- or between-class may sometimes lead to an improvement in symptoms. There is no clinical trial evidence to support the use of omega-3 oils to treat this type of arthralgia. 24
Fibromyalgia (chronic widespread pain)
Among the most common sources of chronic arthralgia and myalgia in adult women is fibromyalgia (previously known as myofascial pain syndrome). The cause of this condition is not fully understood: but genetic and hormonal influences are likely to be important in generating heightened pain sensitivity, and tendency to other chronic pain syndromes.16,25
Clinical features
Pain is usually present in all four quadrants: primarily axial, with diffuse aching in the neck, shoulders, back and pelvis. A history of poor sleep (sleep disturbance, or seemingly adequate sleep but feeling unrefreshed in the morning) and persistent unexplained fatigue are typical. Arthralgia and myalgia are typically accompanied by multiple other symptoms, including tingling, burning or swelling of limbs. Female gender, catastrophizing personality, high depression or anxiety scores are all risk factors. There is no detectable joint swelling or synovitis (although peripheral puffiness may be seen), and muscle strength is normal. Characteristic tender ‘trigger points’ may be found, although these are not necessary for a diagnosis of Chronic Widespread Pain. Patients with fibromyalgia tend to display heightened pain sensitivity at other non-joint, non-spinal sites as well, or have pain affecting other systems, for example migraine, irritable bowel or bladder, premenstrual syndrome or pelvic pain, non-specific chest pain. 26 It is likely that there is a common pathogenesis to different manifestations of chronic pain. Many of these conditions, such as migraine, are more common at the time of menopause. The relationship of fibromyalgic symptoms to menopausal symptoms should be noted.
Management
Fibromyalgia is also a diagnosis of exclusion. Following appropriate clinical assessment and investigation, giving a clear diagnosis and full explanation is essential to prevent ongoing, fruitless medical investigation and over-medicalisation. Advice on pacing, sleep hygiene, weight control and exercise are important. 16 Institution of an aerobic conditioning programme with graded exercise can be helpful. Analgesia is often important, starting with standard analgesics such as acetaminophen, or NDAIDs where indicated. Opiates are often ineffective. Consistent with the concept that the pain of fibromyalgia is related to aberrant neurotransmission or pain processing, other neuroactive ‘neuropathic’ medications which have been approved for treatment of fibromyalgia include pregabalin, gabapentin, duloxetine and milnacipran. Tricyclic antidepressants such as low-dose amitriptyline as well as the later-generation SSRIs are routinely used, the latter particularly when depression is present. Treatment of fibromyalgia may be challenging. Addressing any identifiable biopsychosocial aspects to the presentation and ongoing pain is essential. Some cases may benefit from multidisciplinary specialist pain management.
Common forms of arthritis occurring in the peri-menopause
Osteoarthritis
Osteoarthritis (OA) is the most common form of arthritis; the lifetime risk for women is 47%. 27 It is a whole organ disease (affecting articular cartilage, bone, synovium, ligament). 28 In many, it leads to progressive loss of cartilage and change in bone (leading to classical ‘osteophytes’ on X-ray) with associated joint pain, swelling and loss of function (Table 3). OA ultimately leads to joint failure for many and is the commonest reason for total joint replacement, with high associated socioeconomic cost. 29 However, in early disease, symptoms may often stabilise or improve, with marked variation in symptoms between individuals at any radiographic stage. 30
Although the initiating processes are not fully understood, it is clear that osteoarthritis is an active, cellularly driven process which includes excessive degradation and abnormal repair responses in joint tissues, in part driven by mechanical factors. 31 Blockade of critical pathways such as proteinases protects from the disease 32 ; interestingly, female mice are relatively protected, but this protection is lost following ovariectomy, implicating sex hormones in disease pathogenesis. 32 Important risk factors for OA include age, obesity, female gender, congenital joint abnormality or deformity, a history of substantial joint injury, excessive joint loading and family history (∼60% of risk is genetic). 33
Clinical features
The commonest affected sites are the knee, hip and hand. Pain in joints can be intermittent or constant, typically worse with use (Table 3). In the hand, the distal interphalangeal and proximal interphalangeal joints are most commonly affected, followed by the base of the thumb. There may be apparent bony swelling (‘nodes’) of the interphalangeal joints, which if present are highly suggestive of OA. Blood tests listed in Table 4 are typically normal, although there may be a modestly raised CRP. Diagnostic changes are detectable by X-ray in established disease, but may be absent in early disease. At all sites, there is a female preponderance. Hand OA appears different to other forms in having a definite upsurge in incidence around the age of the menopause in women. 6 Approximately 90% of individuals in secondary care clinics with hand OA are female.34,35 In such ‘peri-menopausal’ cases, symptoms may resolve over two to five years; however, there is no proven causal link between estrogen deficiency and OA.
Management
A clear diagnosis of osteoarthritis should be made and shared with the patient. Management should be focused on the individual, including an assessment of the effect of OA on their work, leisure and quality of life. Patients should be educated and given constructive messages about their disease, including its natural history and possibility of improvement early in disease with or without intervention.36,37 All patients with OA should be encouraged to remain in work and to exercise. 38 Management of osteoarthritis falls into four broad areas: supportive/lifestyle measures (encouraging weight control or loss, general exercise), non-pharmacological (such as joint-specific exercises, or devices such as base of thumb splints, or knee braces that mechanically ‘offload’ joints), pharmacological measures and ultimately evidence-based surgical interventions, such as joint replacement (there is no evidence that simple washout of the joint is helpful for those with OA, and this should be avoided). 39 Not all those with OA will need regular oral analgesia. For those who do, acetaminophen and topical NSAIDs are the first-line treatments. Stronger analgesia such as opiates or oral NSAIDs may be indicated, but should be used with caution given the risks associated with these drugs; intra-articular steroid injections are often helpful in managing symptoms and flares. The current incomplete understanding of this disease means that, unlike in RA, disease-modifying drugs do not yet exist for OA. Newer agents which target pain-generating, or disease-modifying biological pathways are currently in clinical trials.
There is at present no definite evidence for the use of HRT in this setting. Those in the estrogen-containing arm of WHI were noted on post hoc testing to have significantly lower rates of joint arthroplasty (hip, and to a lesser extent knee). 40 A protective effect of HRT on hand and knee radiographic disease has been described previously at a population level. 41 However, no interventional studies of HRT have been run specifically studying those with symptomatic osteoarthritis.
RA
RA is a classical form of inflammatory arthritis. It is three times more common in women than men; peak age of onset is between ages 35 and 55, and it commonly affects peri-menopausal and post-menopausal women.42,43 Genetic factors, the possession of the HLA DR ‘shared epitope’, cyclic citrullinated peptide (CCP) antibodies (which may predate the disease by many years) and cigarette smoking all predispose to the disease.44,45 RA often goes into remission during pregnancy, but despite this, a causal relationship for hormones has not yet been defined. HRT may reduce CCP antibodies in the presence of the shared epitope 46 ). Synovial inflammation leads to ‘pannus’, a destructive, dysregulated tissue within the joint where infiltrating immune cells (lymphocytes and macrophages) release proteinases and pro-inflammatory cytokines such as tumour necrosis factor (TNF)-α, leading to loss of articular cartilage and bony erosion. 47 Untreated, this leads to progressive, irreversible joint damage, with ensuing functional impairment and disability.
Clinical features
RA typically affects multiple peripheral joints in a symmetric and progressive manner, with associated signs of inflammation: pain, swelling, warmth, loss of function and sometimes redness (although marked erythema over joints is more typical of gout or septic arthritis) (Table 3). Prolonged morning stiffness is typically present in active disease, along with some systemic symptoms (fatigue, malaise, sweats). 42 This systemic disease can involve other organs (lungs, pericardium, eyes, skin, nerve). Laboratory studies usually reveal elevated acute-phase proteins (ESR, CRP); rheumatoid factor is commonly found in patients with RA (Table 4). The possession of rheumatoid factor, or the more specific anti-CCP, is associated with increased risk of erosion and joint damage, which is worse in smokers and those with shared epitope. 48 Ultrasound and other imaging modalities are used in the assessment and monitoring of RA. 49
Management
The treatment of RA has been transformed in the last 20 years by the new biologics era. Early diagnosis (ahead of damage) is vital, and rapid, early disease modification, initially with disease-modifying anti-rheumatic drugs (DMARDs). Treatment is escalated until disease remission is achieved, with use of biologic therapies such as anti-TNF where necessary.42,50,51 A detailed review of therapeutics in this area is outside of scope.
What effect does HRT have on RA? In small RCTs, it appears safe (checking usual exclusions: cardiovascular risk is increased in those with RA, so this should be borne in mind when prescribing). No significant effect on incidence or severity of RA was seen in the active arms of WHI. 52 HRT has been reported to mitigate against bone loss and improve some symptoms.46,53
Aetiology: Sex hormones, musculoskeletal pain and inflammation
Cartilage
Estrogen is synthesised by aromatase in connective tissues and estrogen receptors are present in all joint tissues including articular cartilage, subchondral bone, ligaments and synovium. 54 Low-level estrogens appear to promote cartilage growth or prevent its degradation.55,56 After ovary removal, resistance to articular cartilage compressibility is reduced, but appears to be reversed by estrogen replacement. 57 Increased articular cartilage volume is seen by MRI in those taking HRT. 58 Many animal studies suggest estrogen and selective estrogen receptor modulators (SERMs) may be protective of arthritis.54,59 However, there is far less data on the effects of HRT on musculoskeletal pain and arthritis in humans.
Inflammation
Estrogen is known to be anti-inflammatory and mildly immunosuppressive. Its role as a steroid hormone of pregnancy requires this. (Younger) rheumatoid arthritis patients routinely note improvement or even remission during pregnancy, and much of this effect is attributed to the anti-inflammatory properties of estrogen. Joint damage in arthritis is driven by activation of inflammatory signalling pathways inducing proteinases. 28 HRT and SERMs such as levormeloxifene and raloxifene have been reported to reduce levels of inflammation and markers of subsequent matrix degradation.60–62
Bone
The effects of estrogen on bone turnover are well known from osteoporosis, although other therapeutic groups have superseded HRT in its treatment. Bone-targeting agents would appear beneficial in some forms of arthritis too. 62 In a cross-sectional study, women receiving estrogen had less OA-related bony changes on knee MRI than those who were not. 63 In monkeys, estrogen replacement after ovariectomy appeared to limit new bone formation seen in OA. 64
Pain
Estrogen receptors and aromatase are present in dorsal root ganglion, hypothalamus, limbic system, neurone and joint. Estrogen therapy has been shown to decrease synovial nerve fibre neurotophins in an animal model of OA. 65 Estrogen and testosterone both reduce pain, activating inhibitory pain pathways in the spinal cord, while progestins have been reported to promote pain. 66 During normal menstrual cycle, drops in estrogen were associated with increased pain reporting using objective measures of pain induction, whereas high estrogen/low progestin was associated with activation of the endogenous opioid system and less pain.67,68 Those with low testosterone states appear more prone to pain. 68 Entering menopause may for some be like constantly being in the ‘low estrogen’ part of the cycle, heightening the pain experience for any given pathology. Fatigue, poor sleep and mood change occurring in menopause are also well known to enhance pain perception.
Conclusions
Musculoskeletal pain is more common in women, and increases during and after menopause. Not all musculoskeletal pain is arthralgia, and not all joint pain is arthritis. Around the menopause, women have increased prevalence of OA (particularly hand) and RA. Those with symptoms and signs suggesting inflammatory arthritis such as rheumatoid arthritis should be referred urgently to an early arthritis clinic for further assessment. Definitive evidence for menopausal hormonal treatment in the prevention or treatment of either form of arthritis is lacking. There is some limited evidence HRT may help musculoskeletal symptoms or OA at a population level, but currently insufficient evidence to recommend it on an individual basis. If onset of arthralgia, or arthritis is near to the menopause and other related symptoms, it is reasonable to treat possible reversible causes and other systemic menopausal symptoms and record the response of musculoskeletal symptoms to these treatments. However, there have been few studies and no RCTs specifically including this group of symptomatic patients. There is much still to understand about musculoskeletal pain and arthritis at the time of the menopause, and about how we might prevent or treat this.
Practice points
In a patient with musculoskeletal pain, be clear on the source of the pain and likely diagnosis Not all arthralgia evolves into arthritis, but some may Menopause-associated arthralgia is a diagnosis of exclusion: consider other potential secondary causes The commonest form of arthritis is osteoarthritis; hand osteoarthritis onset is more frequent around the time of the menopause Suspected inflammatory arthritis such as rheumatoid arthritis should be urgently referred to a rheumatologist for management Lifestyle measures (weight control, dietary measures, exercise and sleep hygiene) are first line interventions for arthralgia or osteoarthritis There is a lack of current evidence to use HRT specifically to treat arthralgia, fibromyalgia, osteoarthritis or rheumatoid arthritis HRT may have a role when musculoskeletal symptoms are part of a wider syndrome of menopause which has not responded to conservative measures
Footnotes
Acknowledgements
I thank Prof Tonia Vincent for her assistance and guidance in this area.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: FW has received research grants supporting clinical studies from Astellas Pharma Inc. and Pfizer Inc. FW has received a grant from National Institute for Health Research (UK) to test the feasibility of studies of estrogen-containing therapy in osteoarthritis.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: FW is supported by the Arthritis Research UK Centre for Osteoarthritis Pathogenesis, grant ref. 20205 and by the National Institute for Health Research (NIHR) Oxford Biomedical Research Centre (BRC). The views expressed are those of the author and not necessarily those of the NHS, the NIHR or the Department of Health.
Ethical approval
Not applicable
Guarantor
FW
Contributorship
FW has solely written, reviewed and edited the manuscript and approved the final version of the manuscript.