
Abstract
Cancer treatment may result in loss of ovarian function through surgical removal of the ovaries, chemotherapy or radiation. While menopausal symptoms, such as hot flushes, night sweats, sleep disturbance, memory concerns and mood issues can be extremely bothersome to some women going through menopause naturally, women who undergo an induced menopause usually experience more sudden and severe symptoms. Pain and vaginal dryness can occur whether a woman has a sexual partner or not. In women with breast cancer, the aetiology of impaired sexual functioning, and lowered sexual desire, is often multifactorial, and may be related to physical and/or psychological reasons. Pain and vaginal dryness in women without a history of breast cancer can usually be safely treated with vaginal estrogens, in the form of a cream, pessary or ring, and simple lubricants or vaginal moisturisers. Safe usage of vaginal estrogen replacement therapy in breast cancer patients has not been studied within randomised clinical trials of long duration; the guidelines below reflect a clinical consensus.
Keywords
Introduction
Cancer treatment may result in loss of ovarian function through surgical removal of the ovaries, chemotherapy or radiation. While menopausal symptoms, such as hot flashes, night sweats, sleep disturbance, memory concerns and mood issues can be extremely bothersome to some women going through menopause naturally, women who undergo an induced menopause usually experience more sudden and severe symptoms.
Pain and vaginal dryness can occur whether a woman has a sexual partner or not. In women with breast cancer, the aetiology of impaired sexual functioning, and lowered sexual desire, is often multifactorial, and may be related to physical and/or psychological reasons.
It is important to discuss sexual difficulties and/or discomfort so that appropriate treatment can be offered.
Pain and vaginal dryness in women without a history of breast cancer can usually be safely treated with vaginal estrogens, in the form of a cream, pessary or ring, and simple lubricants or vaginal moisturisers. Safe usage of vaginal estrogen replacement therapy (ERT) in breast cancer patients has not been studied within randomised clinical trials (RCTs) of long duration; the guidelines below reflect a clinical consensus.
Recommendations
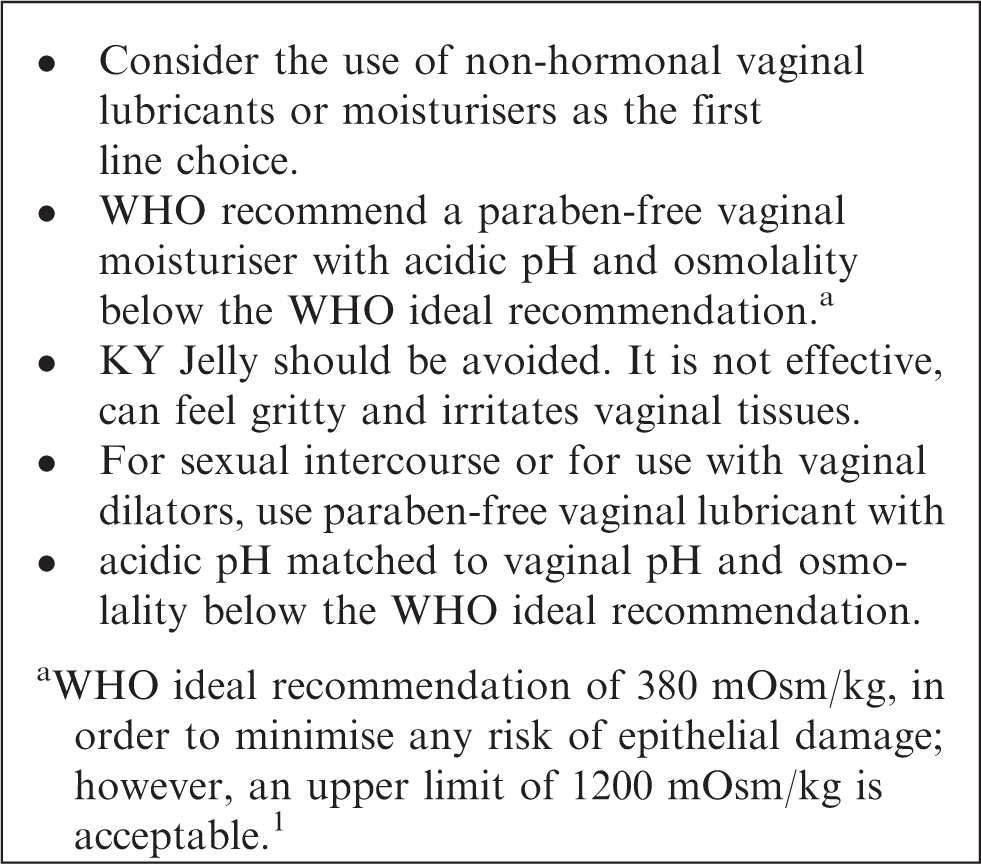
Vaginal moisturisers and personal lubricants
Vaginal moisturisers are absorbed into the skin and adhere to the vaginal lining, mimicking natural vaginal secretions. They are non-hormonal and are intended to alleviate the general discomfort of vaginal dryness/atrophic vaginitis/vaginal atrophy. They are applied regularly, from every day to once every 2–3 days. The effects are long-lasting (2–3 days) than lubricants.
Vaginal moisturisers change the fluid content of the endothelium and lower the vaginal pH, thereby maintaining moisture and acidity; they do not reverse the changes associated with estrogen deficiency.
Personal lubricants
Lubricants act rapidly to provide short-term relief from vaginal dryness and related pain during intercourse. They are particularly beneficial for women whose vaginal dryness is a concern only or mainly during sex. A wide variety of personal lubricants are commercially available, either as water-, silicone-, mineral oil- or plant oil-based products and are applied to the vagina and vulva (and the partner’s penis if required) prior to sex.
Parabens
Parabens are included as preservatives in a variety of personal care, cosmetic and food products, and are found in some personal lubricants. Parabens are weakly estrogenic compounds and there is some debate as to whether they present an endocrine-disrupting risk. They have been detected in breast tumours, but associations with carcinogenesis have not been convincingly demonstrated.
Allergies
Those with specific allergies to plant-based products (e.g. nuts or Kiwi) or shellfish may wish to patch test products or consult the manufacturer prior to use. Consider the partner’s allergies when products are used at the time of intercourse.
Vaginal (local) estrogen therapy
There are three available preparations of vaginal estrogen: cream, ring and tablet (pessary). Studies show that the use of the low-dose (10 mcg oestradiol hemihydrate) vaginal oestradiol, Vagifem®, does not result in sustained serum estrogen levels exceeding the normal menopausal range.2–4
Data do not show an increased risk of cancer recurrence among women currently undergoing treatment for breast cancer or those with a personal history of breast cancer 5 who use vaginal estrogens to relieve urogenital symptoms. A nested case–control analysis of a cohort study of women with breast cancer who either did or did not use vaginal estrogen showed no increase of recurrence in vaginal estrogen users. 6
Vagifem® has been found to significantly raise serum oestradiol levels, in the short term, in women on aromatase inhibitors (AIs) for breast cancer, 7 but these levels were not sustained over time. 8
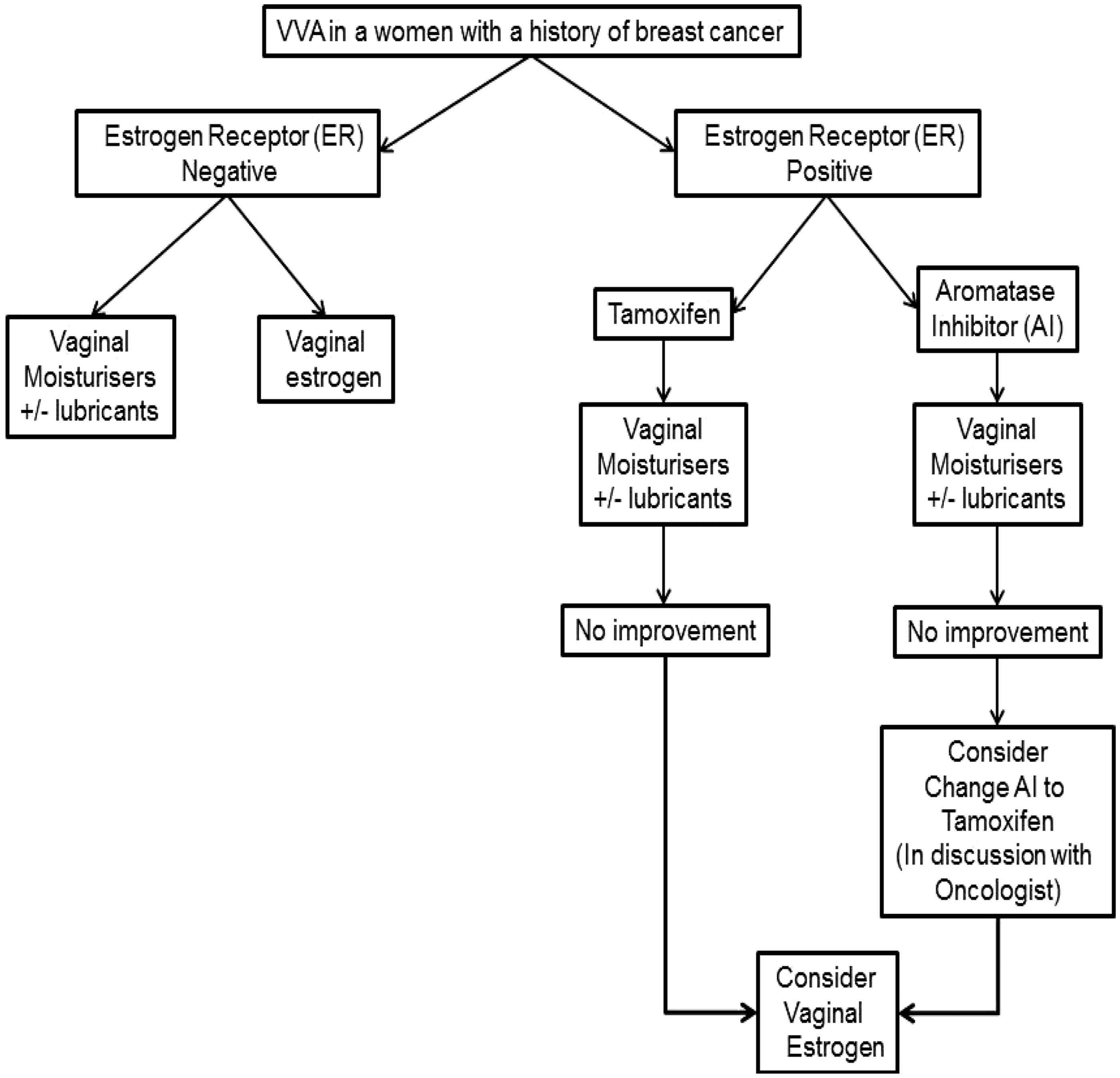
Flowchart for the management of vulvovaginal atrophy after breast cancer.

Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
JS.
Contributorship
JS researched literature and wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.