
Abstract
Objectives
To assess compliance with the European Society for Human Reproduction and Embryology (ESHRE) guidelines on the investigation and management of women with premature ovarian insufficiency at the Leeds Teaching Hospitals NHS Trust (LTHT) and to determine whether this varies depending on the clinical setting in which the women present.
Study design
A retrospective review of all females diagnosed with premature ovarian insufficiency between 1 July 2016 and 30 June 2017, presenting to one of the following clinics: reproductive medicine, specialist menopause, general gynaecology, oncology long-term follow-up, general endocrinology or paediatric endocrinology.
Main outcome measures
Proportion of patients who had the necessary investigations performed and relevant treatment options discussed.
Results
103 women were included in the study. Overall, 40.6% had a karyotype. Screening for the Fragile-X pre-mutation, thyroid peroxidase and 21-hydroxylase antibodies occurred in 7.4%, 11.1% and 13.6% of women, respectively. Only 35.9% had their bone mineral density measured. There was significant variation in the performance of a karyotype (p < 0.001) and thyroid peroxidase antibodies (p < 0.01) between the different clinical settings. Overall, lifestyle advice was offered to 30.1%. Estrogen replacement, contraception, fertility options and bone protection were discussed with 76.0%, 38.4%, 59.0% and 75.0%, respectively. Psychological support was offered to 25.2%. There was significant variation for all apart from contraception.
Conclusion
The investigation and treatment of women with premature ovarian insufficiency at the LTHT is not consistent with the ESHRE guidelines and requires improvement. Furthermore, there is significant variation in management depending on the department to which the patient initially presents.
Keywords
Introduction
Premature ovarian insufficiency (POI) is a clinical syndrome defined by loss of ovarian function before the age of 40. The prevalence is approximately 1%1–4 and is affected by factors such as ethnicity,3,5 smoking,6,7 exercise,8,9 body mass index,8,10 socio-economic status 11 and intelligence quotient.12,13
POI is associated with numerous different aetiologies, including chromosomal and genetic defects and autoimmune disorders. It may also be iatrogenic following surgery, radiotherapy and/or chemotherapy for various indications. In many women diagnosed with POI, the cause remains elusive.14–16
POI is characterised by amenorrhoea or oligomenorrhoea of at least four months duration, with raised gonadotrophin and low estradiol concentrations. It can manifest before or after menarche. Women with POI may therefore complain of a variety of different symptoms including delayed puberty, menstrual disturbance, infertility and symptoms associated with estrogen deficiency. Due to this variation in presentation, women may be seen by medical practitioners in a range of different clinical settings, including general gynaecology, reproductive medicine, specialist menopause services, general endocrinology, paediatric endocrinology and oncology.
The management of women with POI is multifactorial encompassing lifestyle advice, hormone replacement, contraception, fertility, bone protection, cardiovascular health and psychological support. Due to women with POI presenting to various different clinical settings, it is not inconceivable that management may vary according to the awareness and expertise of the medical practitioners within each specialty or subspecialty.
In December 2015, the European Society for Human Reproduction and Embryology (ESHRE) produced guidelines on the management of women with POI. 17
Aim
The aim of this study was to determine overall compliance with the ESHRE guidelines 17 at the Leeds Teaching Hospitals NHS Trust (LTHT) and to assess whether this varies according to the clinical setting in which the women initially present.
The standards were identified from the ESHRE guidelines 17 and are illustrated in Table 1.
Target and actual results for each standard.

POI: premature ovarian insufficiency; TPO Ab: thyroid peroxidase antibody; 21-OH Abs: 21-hydroxylase antibody.
Methods
We undertook a retrospective review of all females diagnosed with POI (follicle-stimulating hormone concentration ≥25 iu/l and estradiol <200 iu/l) between 1 July 2016 and 30 June 2017, presenting to one of the following clinics at the LTHT: reproductive medicine, specialist menopause, general gynaecology, general endocrine, paediatric endocrine and the oncology long-term follow-up clinics. Cases were identified by an electronic search of the biochemistry results server.
For each case identified, the following information was sought: age; clinic setting of initial presentation; whether the necessary investigations (chromosome analysis, Fragile-X pre-mutation, 21-hydroxylase antibodies (21-OH Ab) (or adrenocortical antibodies (ACA)), thyroid peroxidase antibodies (TPO Abs) and dual-energy X-ray absorptiometry (DEXA) scan) had been performed and if so what the results were; and what management options had been discussed (and documented) including lifestyle advice, hormone replacement, contraception, fertility options, bone protection and psychological support.
If women were seen in more than one clinic setting, the results were analysed according to the setting in which they originally presented.
The Chi-square test was undertaken to determine whether any differences in practice observed between the different clinic settings were significant.
Results
The search identified 171 patients. Sixty-eight of these were excluded for the following reasons: not seen at the LTHT (n = 62), not less than 40 years old (n = 3), diagnosis not POI (n = 2) and not female (n = 3). Data were collected for the remaining 103 patients.
Although 41.7% of patients included were between the ages of 35 and 40, the median age was 31.7 years (IQR 21.0–37.4 years). The youngest patients seen were only 9.9 years old (Figure 1).
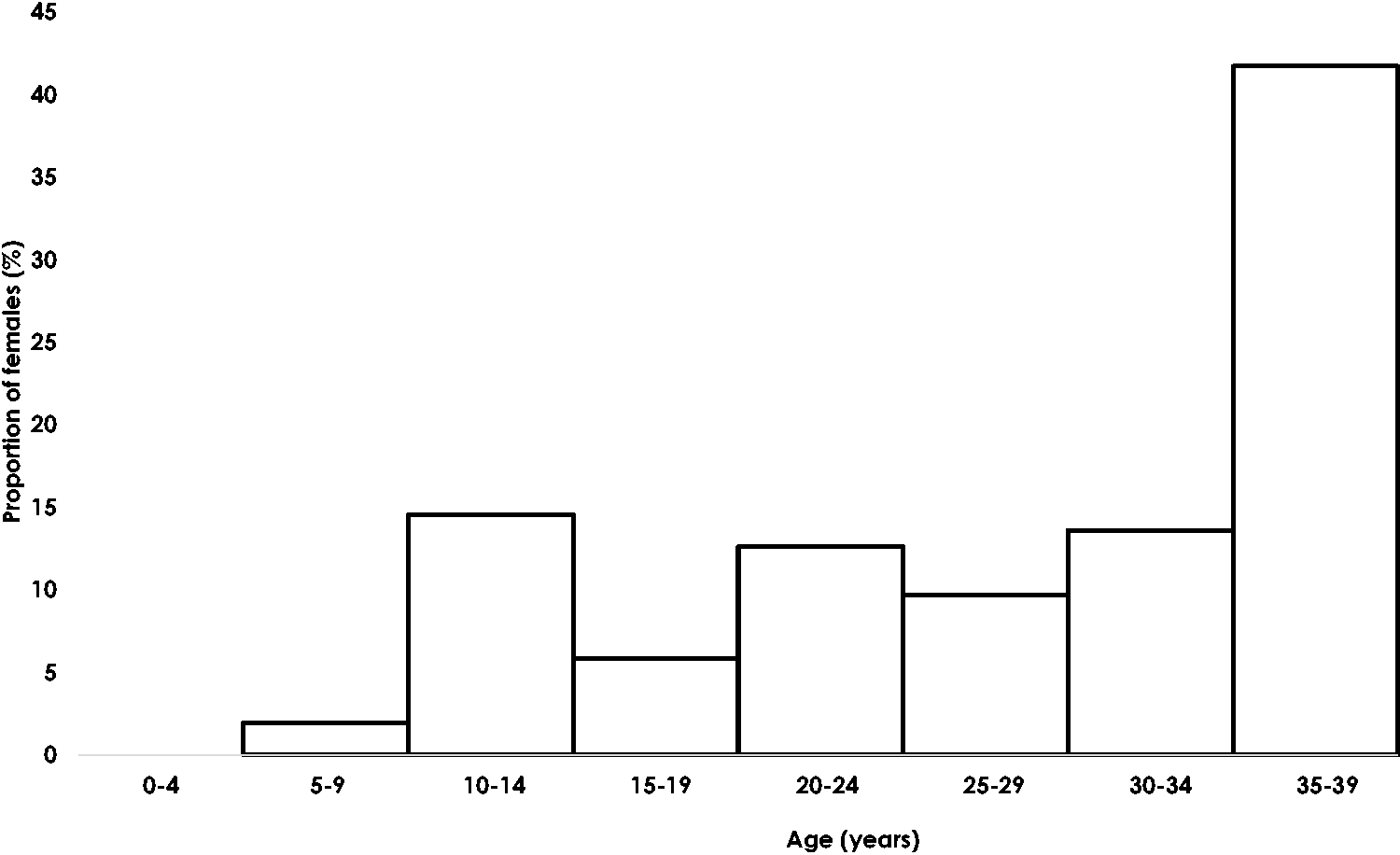
Age distribution of females diagnosed with POI.
Most patients presented to reproductive medicine (22%) and the least to general endocrinology (12%). Similar numbers presented to oncology (19%), general gynaecology (16%), paediatric endocrinology (16%) and specialist menopause (15%). Only nine patients (8.7%) were seen in more than one clinic: eight of these were referred to reproductive medicine from elsewhere and one to the specialist menopause clinic.
Investigations
Overall, only 40.6% of patients with non-iatrogenic POI had a karyotype performed and 7.4% of patients had screening for the Fragile-X pre-mutation. Only 11.1% and 13.6% of patients with POI of unknown cause had screening for 21-OH and TPO Abs, respectively, and only 35.9% of women had a DEXA scan to measure their bone mineral density (Table 1).
Between the different clinical settings, there were no significant differences in the proportions of patients who had screening for the Fragile-X pre-mutation, 21-OH Abs or bone mineral density loss. However, all patients seen in paediatric endocrinology had a karyotype performed but only 13.3% of patients seen in general gynaecology did. Similarly, half of the patients seen in general and paediatric endocrinology had screening for TPO Abs, but none of those who attended a general gynaecology clinic did. These differences were found to be statistically significant (Table 2).
Proportion of patients who had the necessary investigations performed according to clinical setting at presentation.

DEXA: dual-energy X-ray absorptiometry; TPO Abs: thyroid peroxidase antibodies; 21-OH Abs: 21-hydroxylase antibodies.
The results were slightly better for the nine patients who were seen in more than one clinic, with 71.4% having a karyotype and 44.4% having a DEXA scan. No patients were seen in multiple clinics; however, the patients had screening for the Fragile-X pre-mutation, 21-OH or TPO Abs.
Of the 103 patients, 42 (41%) had iatrogenic POI following treatment of conditions such as lymphoma, leukaemia, thalassaemia, sickle cell, medulloblastoma, glioblastoma, bilateral salpingo-oophorectomy (BSO) for dysgerminoma and prophylactic BSO for a BRCA mutation. Eight patients (8%) had Turner’s syndrome, one was found to have Fragile-X syndrome, one had an XY karyotype and one had Nijmegan breakage syndrome. Three women had all the necessary investigations and were classified as having idiopathic POI. The remaining 47 (46%) were not fully investigated, so the cause, if any, of their POI could not be established.
Management
Overall, less than half of patients had the offer of psychological support (25.2%) or information regarding lifestyle changes (30.1%) and contraception (38.4%). More women had a discussion regarding fertility (59.0%), bone protection (75.0%) and estrogen replacement (77.1%) (Table 1).
There was significant variation in the management between the different clinic settings with regard to the provision of lifestyle advice and psychological support as well as information regarding estrogen replacement, fertility options and bone protection. With regard to estrogen replacement and bone protection, all patients seen in the specialist menopause and paediatric endocrinology clinics had a documented discussion, but only 33.3% of patients attending a reproductive medicine clinic had a similar discussion documented. Unsurprisingly, all patients seen in reproductive medicine had a discussion regarding the fertility options available to them, but only 33.3% of patients attending the specialist menopause service and 35.7% of those attending a general gynaecology clinic were given the same information (or referred on). Lifestyle advice and psychological support were offered to 70% and 50% respectively of patients attending an oncology clinic, but no patients attending a general gynaecology clinic. There was no significant difference between the different clinical settings regarding the provision of contraceptive advice, which was generally poor (Table 3).
Proportion of patients who had the relevant treatment options discussed according to clinical setting at presentation.
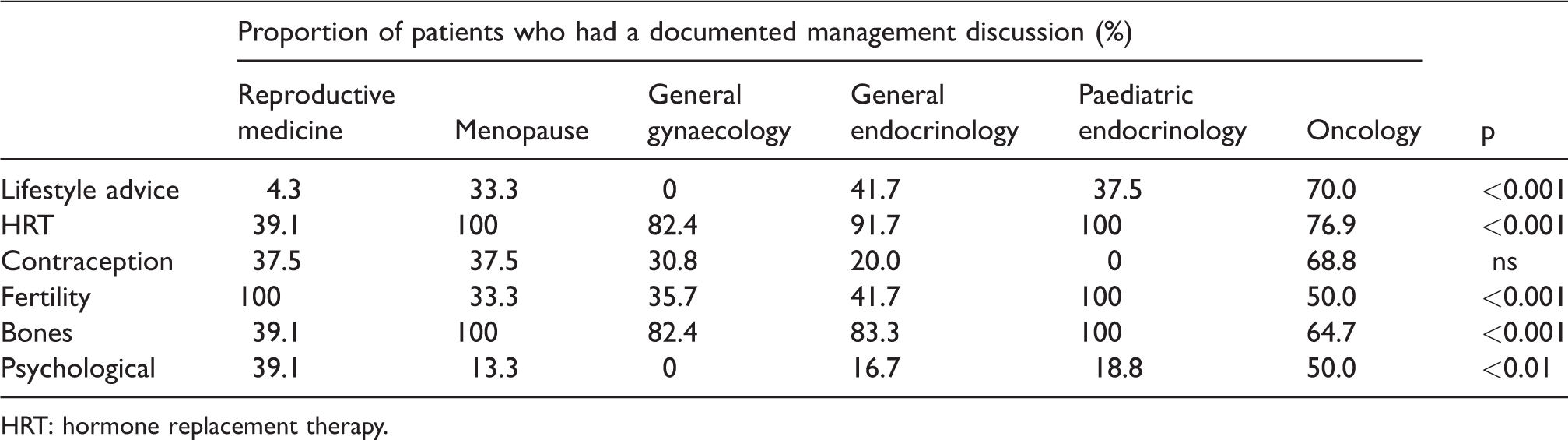
HRT: hormone replacement therapy.
Results were slightly better for the nine patients who were seen in more than one clinic, with 44.4% receiving lifestyle advice, and information regarding estrogen replacement, contraception, fertility and bone protection being given to 77.8%, 42.9%, 88.9% and 77.8%, respectively. However, still only 22% were offered psychological support.
Discussion
Our results have demonstrated that the management of women with POI at the LTHT is suboptimal and not compliant with the internationally recognised ESHRE guidelines. 17 Furthermore, there is significant variation in the management of women with POI depending on the clinical setting in which they present. Whilst this variation in practice may be understandable, it is not acceptable.
We suspect that, on the whole, the limited investigation performed in women with POI is a reflection of a lack of awareness of the current guidelines. However, some may argue that investigating the cause of POI is an unnecessary expense and use of resources, as it does not significantly alter how women are managed in the long term. This is not strictly true. Whilst the majority of women after investigation will be diagnosed with idiopathic POI, the finding of a chromosomal, genetic or autoimmune cause in the minority not only has consequences for the health of the patient but may also have important implications for her relatives.
Studies have shown that 10–12% of women diagnosed with POI have a chromosomal abnormality, of which the majority relate to the X chromosome (X structural abnormalities or X aneuploidy). Diagnoses such as Turner syndrome, which was identified in 8% of patients in our study, have significant health implications for those affected. Karyotyping may also reveal, as it did for one patient in our study, the presence of Y chromosome material. These individuals have a 45% risk of developing gonadal neoplasia, and hence gonadectomy is recommended. Whilst the incidence of an abnormal karyotype is higher in those presenting before menarche than those presenting afterwards (21% versus 11%), a specific age cut-off limit for undertaking a karyotype in POI is not recommended because, in one study at least, amongst women with secondary amenorrhoea and an abnormal karyotype, 33% were older than 30 and 8% older than 35 years. 17 In our study, one patient found to have a Turner mosaicism was over 30 years of age.
The prevalence of the Fragile-X pre-mutation is 0.8–7.5% in women with sporadic POI (0.97% in our study) and up to 13% in women with a family history of POI.18,19 Although women who carry the pre-mutation do not have an increased risk of intellectual disability, there is a possibility of them developing the Fragile-X-associated tremor/ataxia syndrome in later life, which manifests as progressive cerebellar gait ataxia and intention tremor. Furthermore, the presence of the mutation has major implications for family members who may also be affected and hence themselves have a 13–26% increased risk of developing POI 19 or of having children with Fragile-X syndrome. If family members know they carry the pre-mutation before having children or going through the menopause, there are reproductive and diagnostic options available to them including fertility preservation and/or pre-implantation genetic diagnosis.
Although in our study, no patients were found to have 21-OH Abs and only two patients (1.9%) were found to have TPO Abs (and both of these had iatrogenic POI following treatment for bilateral dysgerminomas), this is more likely due to the fact that so few patients were screened (11.1% and 13.6% respectively) than the rarity of these findings in the POI population. In actual fact, autoimmune disorders are more frequent in women with POI than in the general population, and POI is more frequent in women with certain autoimmune disorders than others. 16 Addison’s disease is the most important autoimmune disease associated with POI, and it is recommended that 21-OH Abs or ACA should be measured in every patient with POI because of the possibility of subclinical or latent Addison’s disease in these patients. Early recognition of adrenal insufficiency is essential to avoid unnecessary morbidity and mortality associated with the condition.
POI is also commonly associated with thyroid autoimmunity, 20 and the frequency of TPO Abs in the POI population is approximately 24% (compared to 12–15% in the general population). 21 Although, unlike Addison’s disease, untreated hypothyroidism is not life-threatening, it can severely affect one’s quality of life, which may already be compromised following a diagnosis of POI. 22 Furthermore, the presence of TPO Abs, alone or in combination with (clinical or subclinical) hypothyroidism, is an important consideration in women embarking on a pregnancy (either spontaneous or after oocyte donation). 23
In our study, 47 patients were not fully investigated. Potentially therefore, if 10–12% of these have a chromosomal abnormality and up to 7.5% have the Fragile-X pre-mutation and a further 24% have TPO Abs, the potential for identifying a cause or contributing factor for the diagnosis may have been missed in up to 20 women.
With regard to the suboptimal and variable treatment of women with POI, this is likely due to a combination of factors including: a lack of awareness of all the different aspects which need to be addressed; patients presenting with overriding specific complaints, for example subfertility, menstrual cycle dysfunction or troublesome vasomotor symptoms; consultation time restrictions and poor documentation.
It is unsurprising that all those who presented to the specialist menopause service or paediatric endocrine clinic were given information regarding hormone replacement and bone protection. What is concerning, however, given that the same advice applies to all women with POI, is that overall only 75.0–77.1% of women were given this information. A quarter of all the women in this cohort are therefore potentially not receiving any form of hormone replacement and not only is this indicated for the treatment of symptoms of estrogen deficiency, 24 which they may well be experiencing to some greater or lesser extent, it also has a very important role in primary prevention of diseases of the cardiovascular system 25 and for bone protection. 26 Hormone replacement therapy (HRT) may therefore have an indirect effect on both quality of life 27 and life expectancy. 28 Furthermore, as there are minimal risks associated with HRT in women who have gone through the menopause prematurely29–31 and very few absolute contraindications to its use, there is no acceptable reason why such a large proportion of patients have not been advised regarding early initiation and continuation of it until at least the average age of the natural menopause.
Reproductive medicine specialists appear to be the main culprits, having only discussed HRT with 39.1% of their patients. This is likely to be because their patients present with a very specific agenda – to conceive – and hence their initial further management is very much focussed on that. However, not all patients go down the route of IVF (with oocyte donation), and for those that do, there is often a long wait for an appropriate donor; hence, HRT should still be discussed with all women. Furthermore, women who do achieve a pregnancy need to know to commence HRT afterwards, and if this is not something which has been discussed with them pre-pregnancy (and communicated to their general practitioner), it represents a missed opportunity and it may be years before it is rectified.
Conversely, reproductive medicine specialists were excellent at discussing the fertility options available to women with POI. The other specialties (excluding paediatric endocrinology which only had one patient in whom it was considered appropriate) were less good, only discussing it with between one third and one half of all patients. This may be because the patients did not request any information or because during the consultation they expressed their families were already complete, or it may be because the clinician did not realise that there were any options available to them once a diagnosis of POI had been established. Whilst there are no known treatments which reliably increase ovarian activity, ovulation or conception, 32 IVF with oocyte donation is very successful, and a possibility which, within the United Kingdom, may be included in NHS funding for IVF as long as all the other usual criteria are met. It is therefore important that all specialties either discuss this with their patients and either document that it is not required or refer them on to reproductive medicine.
Overall, only 38.5% of patients had a discussion regarding contraception and all specialties were equally irresponsible. This may be understandable for the reproductive medicine specialists for obvious reasons, but less so for all other clinicians. One quarter of women with POI may show subsequent evidence of ovarian function, 33 especially early on in the natural history of the condition, and spontaneous conception may occur in 5–10%. 32 This may or may not be desirable, and due to absent or irregular menses, the pregnancy may go unnoticed for a longer period of time which may have consequences for subsequent antenatal care or termination requests. Additionally, the cause of POI should be considered in women with a spontaneous pregnancy, in case it has implications for the pregnancy and/or the child (for example, in women with the Fragile-X pre-mutation or Turner syndrome). Since HRT itself is not contraceptive (unless a Mirena coil is used as the progestogenic component), all women with POI who do not wish to conceive, and who have not been previously sterilised, may benefit from using a combined oral contraceptive pill (COCP) containing ethinyl-estradiol for their hormone replacement requirements (as long as there are no contraindications) rather than traditional HRT. However, this needs to be balanced against the fact that the COCP may be less beneficial in improving bone health 26 and cardiovascular markers 25 than traditional HRT.
Finally, a diagnosis of POI can have a detrimental effect on emotional and psychological wellbeing, with those affected reporting higher levels of depression and perceived stress and lower levels of self-esteem and life satisfaction than those unaffected. 22 This may be due to the diagnosis itself and/or the associated symptoms. Although reproductive medicine specialists and oncologists performed significantly better than other clinicians, overall only one quarter of women with POI were offered any information or advice on the availability of support, counselling or other suitable therapy. This is perhaps a reflection of the more widespread availability and utilisation of counsellors generally in reproductive medicine and oncology settings.
Whilst the factors described above may explain the results observed in our study, it does not justify them, and hence efforts should be made to standardise the management of women with POI. This could be achieved in a variety of ways: education of all clinicians involved in the care of women with POI; development of a POI clerking proforma/patient checklist; a patient information sheet to be available in all clinic settings where women with POI are seen and/or introduction of a specialist multi-disciplinary POI clinic (composed of reproductive medicine and menopause specialists, endocrinologists and psychologists) to which all patients with POI be referred following confirmation of the diagnosis.
Conclusion
This study has demonstrated that the investigation and treatment of women with POI at the LTHT is not consistent with the internationally recognised guidelines and requires improvement. Furthermore, there is significant variation in management depending on the department to which the patient initially presents. We suspect that similar results will be found in many other hospitals both nationally and internationally. We have proposed remedial action and plan to reassess following its implementation.
Footnotes
Acknowledgements
We would like to thank Dr Julian Barth for his assistance in this project.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Guarantor
AR.
Contributorship
AR researched the literature, conceived the study, developed the protocol, collected and analysed the data and wrote the first draft of the article. SH helped with data collection. All authors reviewed and edited the article and approved the final version of the article.