
Abstract
There is wide variation in reporting the prevalence of hyperplasia and cancer in endometrial polyps in women with postmenopausal bleeding. Most studies reported heterogenous populations of pre- and postmenopausal women both symptomatic and asymptomatic, making data interpretation difficult. The aim of this work is to quantify the prevalence of hyperplasia and cancer in polyps in women with postmenopausal bleeding aiming to produce data that help inform clinical practice as whether it is safer to remove all polyps, or some women could be offered expectant management. The search terms used were Medical Subject Headings terms, text words, truncations and word variations of the words or phrases ‘endometrial polyp’ or ‘uterine polyp’ or ‘womb polyp’ and ‘postmenopause’ or ‘menopause’. Search was limited to human studies and English language articles. Studies reporting separate analysis for women with postmenopausal bleeding were included. The included articles were assessed for risk of bias using the ‘Quality in Prognosis Studies’ tool. The prevalence was estimated with a random effect model using ‘DerSimonian and Laird’ method. The pooled estimate of prevalence of hyperplasia and cancer was 9% (95% confidence interval: 6.5%–11.5%). An I2 statistic of 77.2% suggests likely substantial heterogeneity. However, adjustment for small study effects had no influence on the pooled prevalence estimate suggesting no evidence for publication bias. Sensitivity analyses showed that no study exerted a big influence on the pooled estimate. The prevalence of hyperplasia and cancer in endometrial polyps in women with postmenopausal bleeding is high enough to warrant removal for accurate histopathological diagnosis.
Introduction
Endometrial polyps are commonly found on investigating women with postmenopausal bleeding (PMB) and may also be found incidentally in bleeding-free women investigated for other indications. 1 There is wide variation in reporting the prevalence of endometrial polyps in women with PMB with a range of 5.3%2,3 to 32.9% 4 in various studies, reflecting the populations heterogeneity in terms of menopausal status, presence or absence of abnormal uterine bleeding and clinical parameters. The largest two studies in the literature reported the prevalence of hyperplasia in endometrial polyps in women with PMB as 7% 5 and 10.1% 6 and cancer as 1% 5 and 3.7%. 6 A systematic review and meta-analysis found that the risk of endometrial hyperplasia and cancer in polyps was 4.4-fold higher in women with PMB when compared with asymptomatic postmenopausal women. 7 Furthermore, many studies, investigating the relevance of very thickened endometrium (≥10 mm) and the risk of malignancy, reported the difficulty of distinguishing between endometrial hyperplasia or cancer and endometrial polyps on transvaginal ultrasound scan.8–10
There is lack of consensus amongst gynaecologists as whether benign-looking endometrial polyps ought to be removed in women with PMB. No universal algorithm exists in relation to the diagnostic management of these women; however, the common practice is to perform hysteroscopic-guided resection or morcellation when polyps are identified during investigation for PMB. The real challenge is in managing women with multiple comorbidities when outpatient morcellation is not available, technically difficult, or not tolerated. Most of the existing studies reporting the prevalence, risk factors, risk of malignancy and management were relatively small retrospective case series including a mixture of pre- and postmenopausal women both symptomatic and asymptomatic.7,11,12 This makes it difficult to produce guidelines for management. Further, one randomised controlled trial (RCT) 13 and three systematic reviews7,11,12 failed to produce evidence as regards the best management of endometrial polyps in women with PMB. The RCT was discontinued after 26 months because of lack of recruitment to the expectant management arm. Most women and doctors deemed office hysteroscopy a rather minimally invasive procedure and opted for allocation on the hysteroscopic polypectomy arm. The three systematic reviews7–9 suffered from severe heterogeneity in the population studied (a mixture of pre- and postmenopausal women both symptomatic and asymptomatic) and the outcome measures. In one of them, meta-analysis was not performed since pooling of data was not possible. 11
Given the inability of obtaining evidence from RCT or meta-analyses, and the retrospective design of published reports, we conducted this systematic review and meta-analysis to quantify the prevalence of hyperplasia and cancer in endometrial polyps in women with PMB. We aim to produce data that help inform clinical practice as whether it is safer to remove all endometrial polyps when first diagnosed or some women could be offered expectant management.
Methods
Search strategy
We searched the published literature using strategies developed by a medical librarian for the concepts of endometrial polyp and postmenopausal women. These strategies were developed using a combination of standardised terms and key words and were implemented in PubMed, EMBASE 1974–2018, and clinicaltrials.gov. The search terms used were Medical Subject Headings (MeSH) terms, text words, truncations and word variations of the words or phrases ‘endometrial polyp’ or ‘uterine polyp’ or ‘womb polyp’, and ‘postmenopause’ or ‘menopause’. We also did a hand search of the bibliography lists of the included studies. Search was limited to human researches and English language articles. Since our aim was to extract a distinctive subgroup of women, there were no limitations to the study design. All searches were completed on 31 May 2018. Details of the search strategy are presented in the Supplementary Material, Appendix S1.
Selection of studies and reporting
We included only studies reporting separate analysis for women with PMB. Case reports, case series, and review articles were excluded. The diagnosis of hyperplasia and cancer in polyps must be confirmed by histopathology. The reporting conformed with the Meta-analyses Of Observational Studies in Epidemiology standards (MOOSE). 14
Data extraction
The authors AG, MSEF and ASA screened 2637 titles and abstracts. Full-text articles were retrieved if they appeared relevant or if there was ambiguity as to whether the article was relevant. Full-text articles were independently reviewed against inclusion and exclusion criteria by the authors AG, MSEF and ASA. An attempt was made to contact the authors of all articles meeting inclusion criteria by e-mail or phone when there was insufficient information to extract data. However, we received only one reply from Lieng et al. 15 advising that the data were destroyed after five years of publication. Data were extracted into a standardised abstraction form by the author AG. Any discrepancies in decisions regarding study inclusion and exclusion were resolved by discussion with the senior author AE.
Outcomes
The primary outcome was quantifying the prevalence of hyperplasia and cancer in endometrial polyps in women with PMB. For the purposes of this study, endometrial hyperplasia and cancer were combined as a single category.
Quality assessment
Articles included in the study were assessed for risk of bias using the Quality in Prognosis Studies (QUIPS) tool. 16 We used the three domains that are relevant to our primary outcome: study participation, prognostic factor measurement, and outcome measurement. Appraisal of each domain provides a subjective assessment of risk of bias, ranked as low, moderate, or high. All three domains had to be ranked as low risk of bias in order to give the study an overall rank as ‘low’. One moderate risk of bias domain would make the overall rank as ‘moderate’. Two or more moderate risk of bias domains or one or more high risk of bias domain would make the overall rank as ‘high’.
Meta-analysis
The prevalence of hyperplasia and cancer within endometrial polyps in women with PMB was estimated with a random effect model using the method of DerSimonian and Laird. 17 Exact confidence intervals (CIs) were calculated for the individual studies.
Heterogeneity was assessed using the I2 statistic and calculation of 95% prediction intervals for the response proportion in a new study.18–20 In interpreting I2, we describe values from 0% to 30% as being ‘likely minimal’, values from 30% to 60% as ‘likely moderate’, and values from 60% to 100% as ‘likely substantial’ heterogeneity.
The possibility of small study effects (e.g. publication bias) was assessed by asymmetry of funnel plots and the potential impact quantified using the Duval and Tweedie non-parametric ‘trim and fill’ method. 21 The ‘trim and fill’ method is a non-parametric (rank-based) data augmentation technique. The method is used to adjust the pooled prevalence for the missing studies from a meta-analysis, i.e. publication bias. It aims both to identify and correct for funnel plot asymmetry arising from publication bias. The basis of the method is to (1) trim, i.e. remove the smaller studies causing funnel plot asymmetry, (2) use the trimmed funnel plot to estimate the true centre of the funnel and then (3) replace the omitted studies and their missing counterparts around the centre (filling). The method then performs a meta-analysis of the original and filled studies to calculate the pooled prevalence that is adjusted for the publication bias. 21
We also performed one-study removed cross-validation as sensitivity analyses to determine the effects of individual studies on the overall effect estimate. 22 This involved removing studies one at a time and calculating pooled prevalence estimate for the remaining studies.
Results
Out of 2637 studies retrieved on applying the search strategy, 10 studies including 2505 women were deemed eligible for the meta-analysis. The flowchart of studies identification is presented in Figure 1. The findings of the included 10 studies are summarised in Table 1.
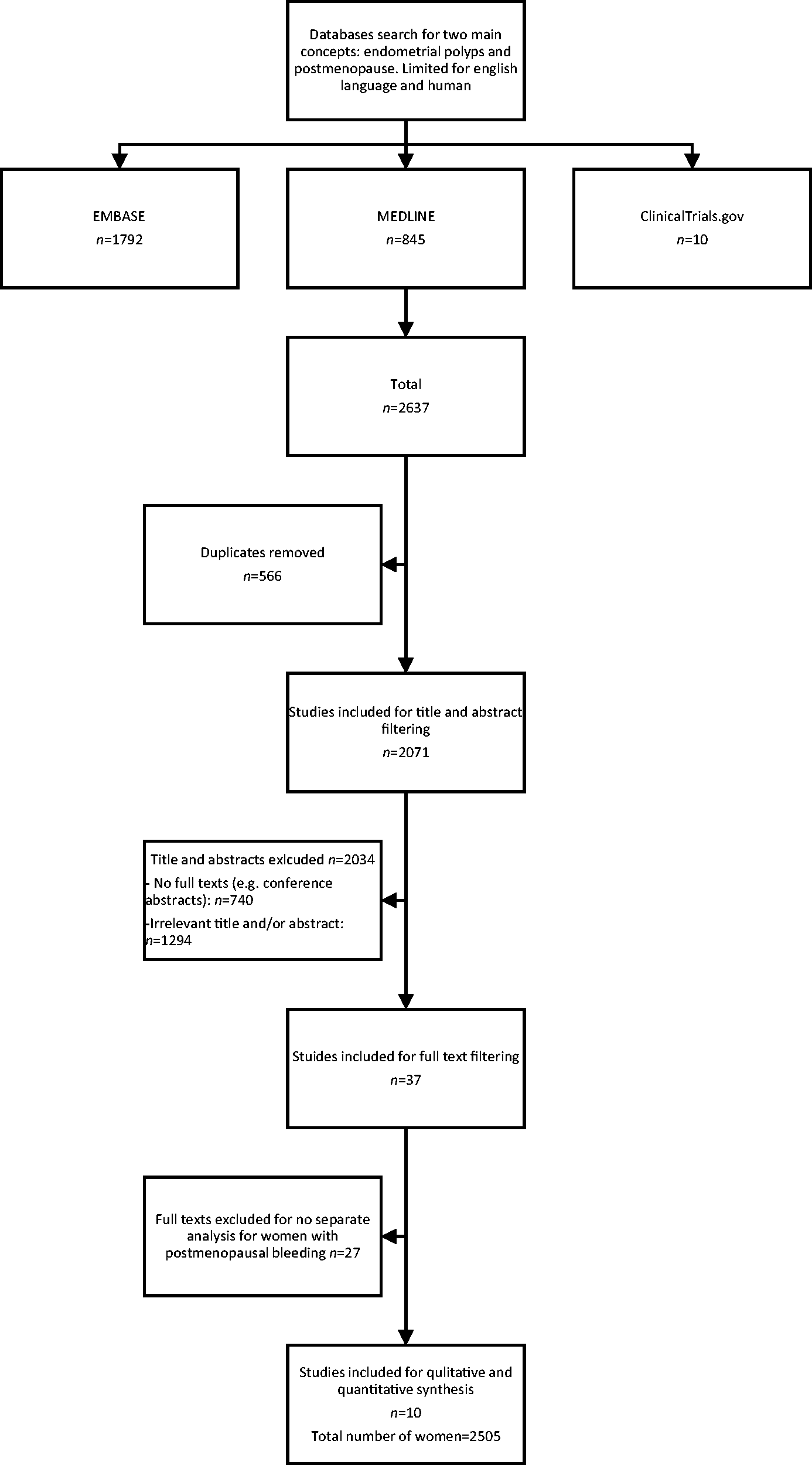
Flowchart to illustrate the process of studies selection.
Summary of findings of the included 10 studies (2505 women).
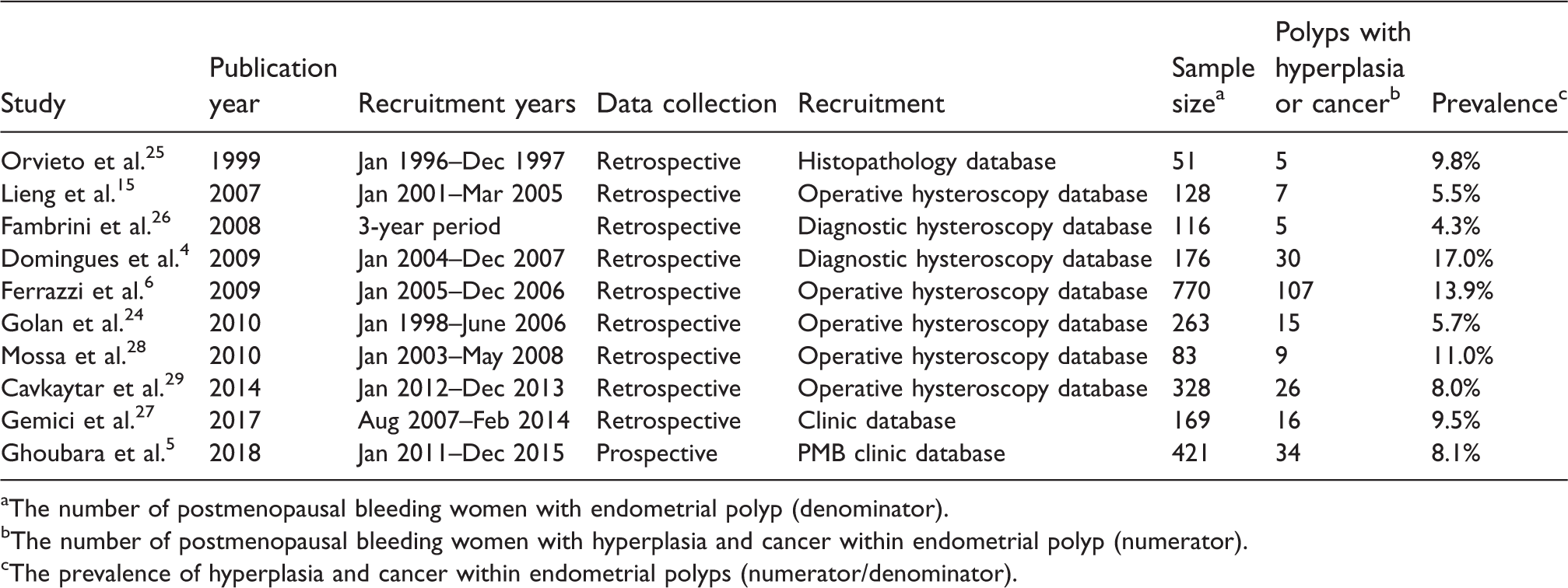
aThe number of postmenopausal bleeding women with endometrial polyp (denominator).
bThe number of postmenopausal bleeding women with hyperplasia and cancer within endometrial polyp (numerator).
cThe prevalence of hyperplasia and cancer within endometrial polyps (numerator/denominator).
Quality assessment
Three studies were graded as high risk of bias, five as moderate, and two as low. A summary of the justification of the risk of bias in the included studies is provided in Table S1.
Meta-analysis
The pooled estimate of prevalence and 95% CI of hyperplasia and cancer in women with PMB was 9% (6.5%–11.5%) (Figure 2). An I2 statistic of 77.2% suggests likely substantial heterogeneity. Using the trim and fill method and the funnel plot, adjustment for small study effect had no influence on the pooled prevalence estimate suggesting no evidence for publication bias (Figure 3).
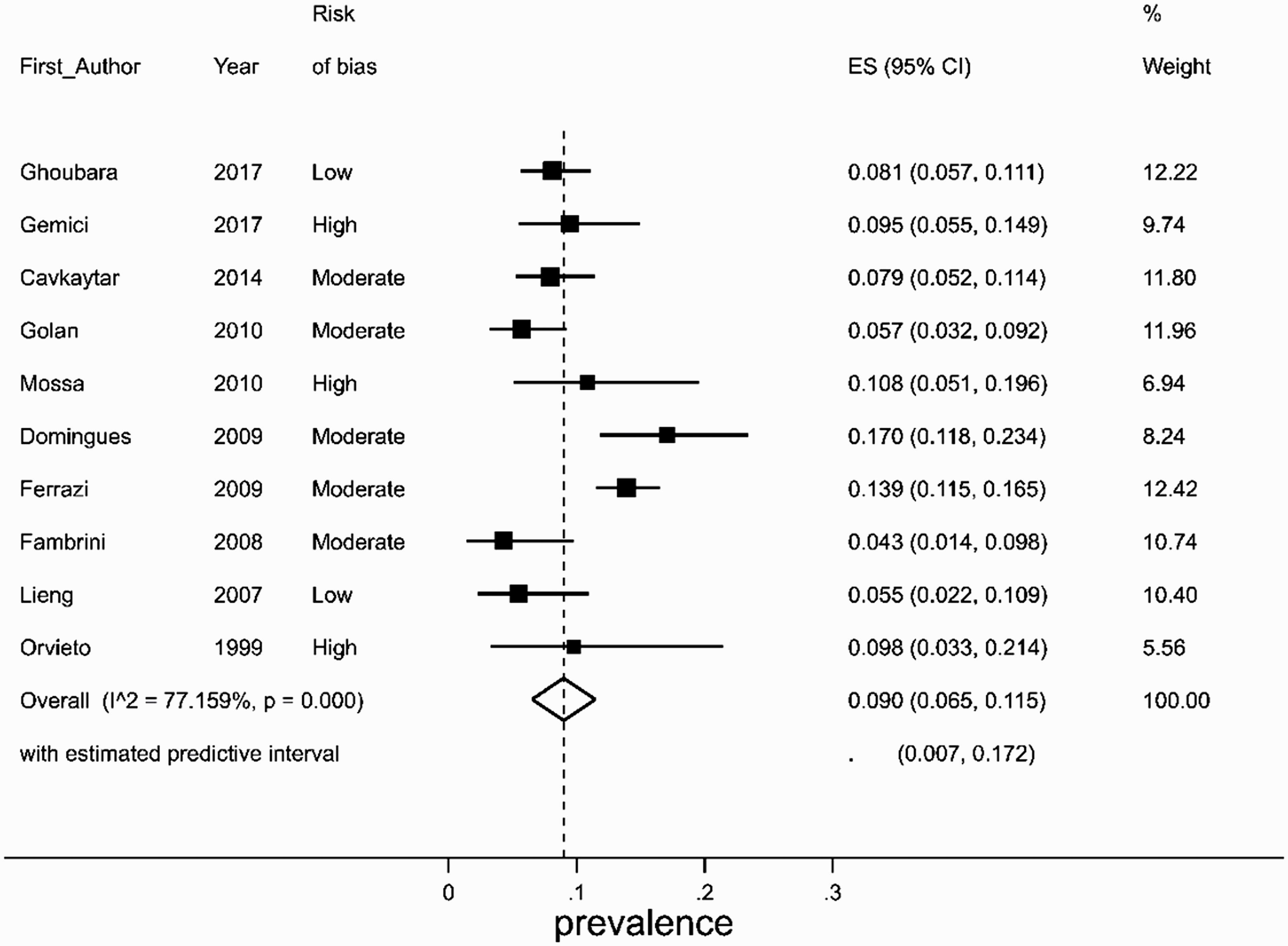
Forest plot showing study specific and pooled prevalence estimates of hyperplasia and cancer within endometrial polyps together with 95% confidence intervals. CI = confidence interval; ES = effect size (the prevalence of hyperplasia and cancer within endometrial polyps); I2 = The I2 statistic for estimation of heterogeneity.
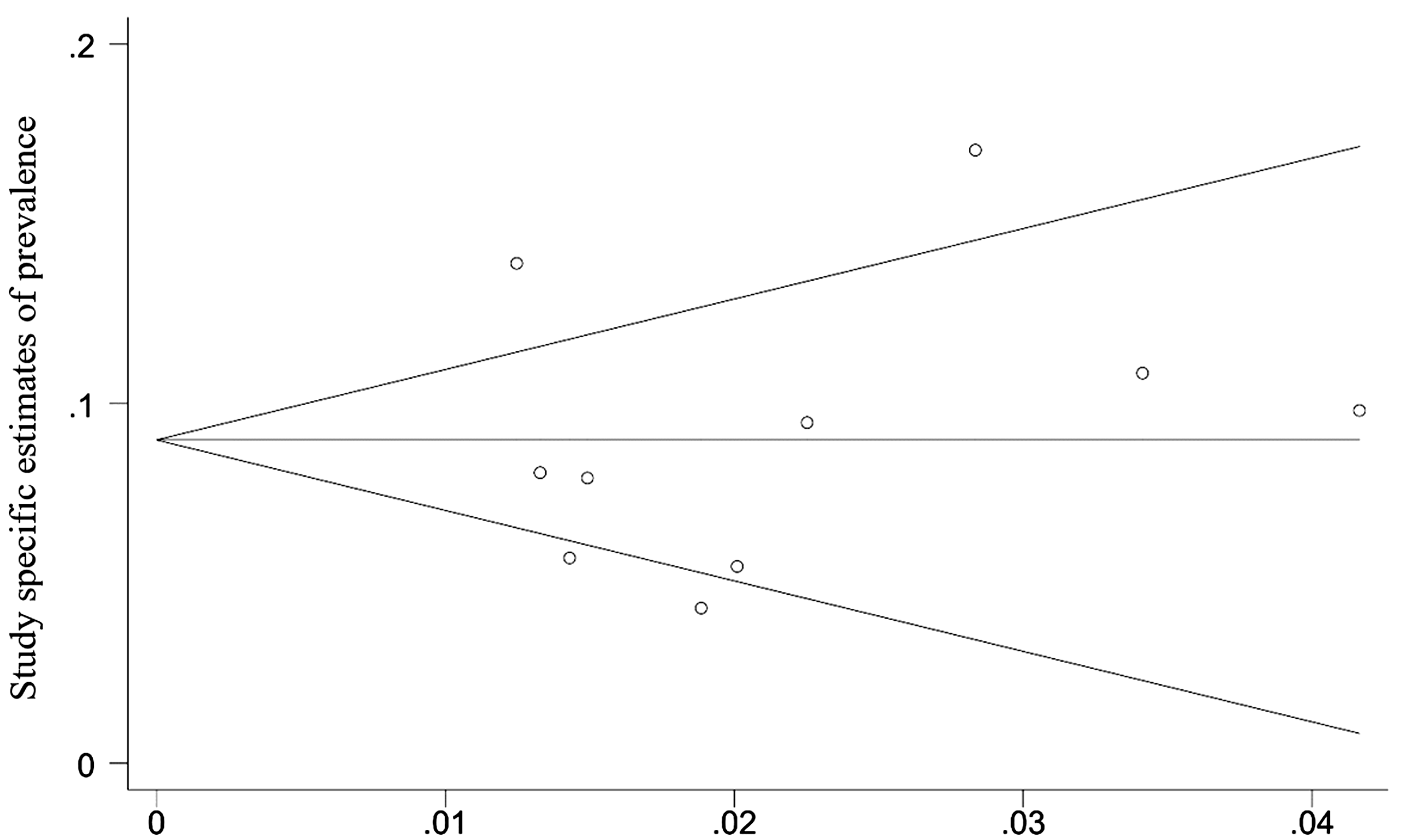
Funnel plot of study specific estimates of prevalence of endometrial hyperplasia and cancer in polyps in women with PMB. s.e. = standard error (precision). This funnel plot has the following elements: Dots: Each dot represents a study estimate (n = 10). Y-axis (vertical): represents the pooled estimate of prevalence after correction of publication bias using the ‘trim and fill’ method. Looking at the tip of the funnel on the graph on the left-hand side, the prevalence of hyperplasia and cancer is 0.9 (9%). The figure was the same before conducting the ‘trim and fill’ method indicating that the estimate is not contaminated with publication bias. X-axis (horizontal) represents the accuracy of estimate of each study. The less accurate studies are plotted towards the right side of the x-axis. The two oblique lines represent the pseudo 95% CI, which delineate the boundaries of the funnel.
Sensitivity analyses showed that no study exerted a big influence on the pooled estimate with the largest change being down to 8.1% and 8.3% coming from the removal of Ferrazzi et al. 6 and Domingues et al., 4 respectively (Figure 4).
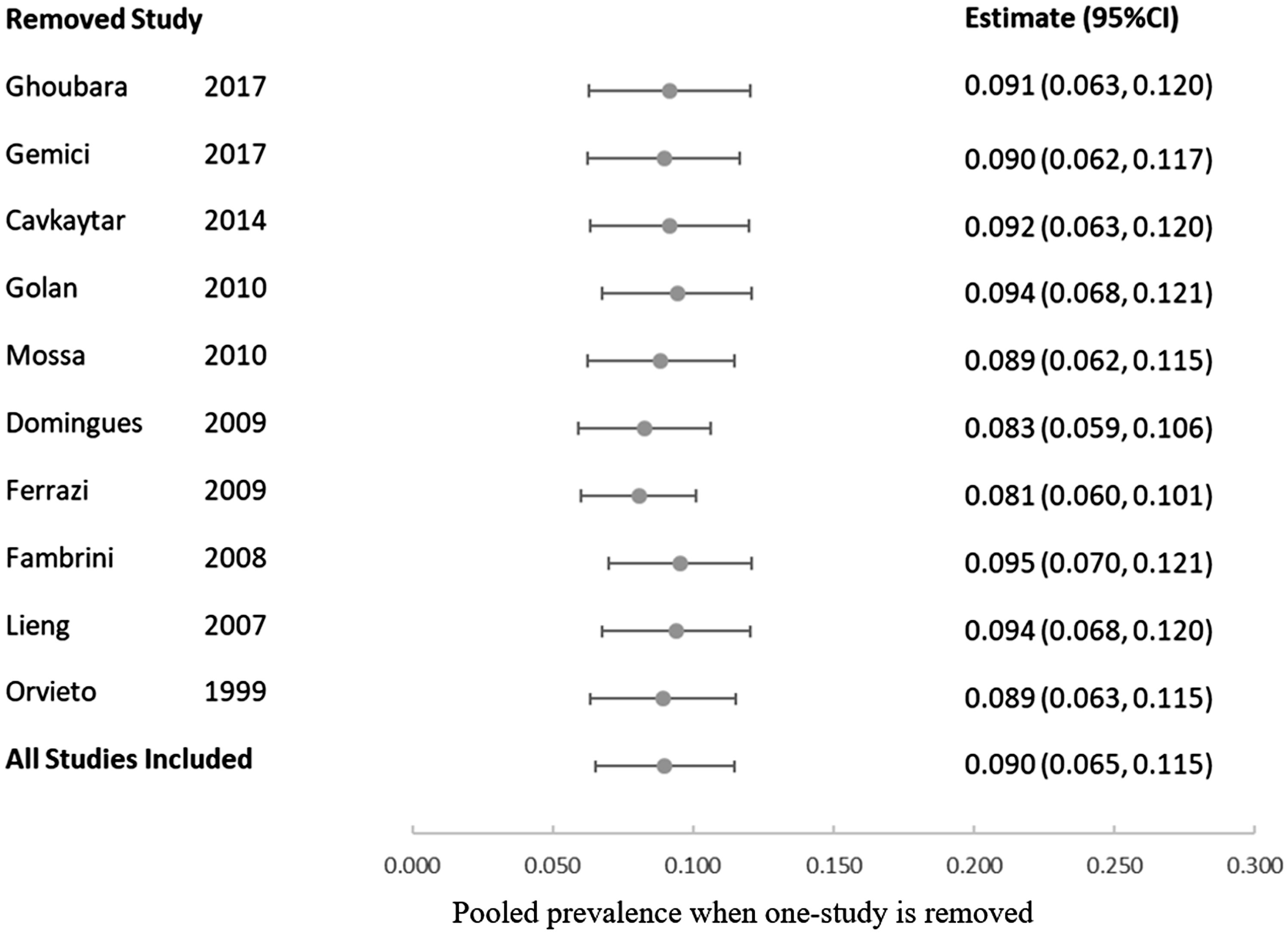
Pooled estimates of the prevalence of hyperplasia or cancer when removing one study from the meta-analysis in turn: one-study removed cross-validation sensitivity analyses. CI = confidence interval.
Discussion
Main findings
Polyp removal has been made easy with the introduction of outpatient morcellation; however, resection may constitute a dilemma in postmenopausal women, with multiple comorbidities and high anaesthetic risks, when outpatient management is not available, technically difficult, or not tolerated. This study is the first study in the literature that includes homogeneous population of women with PMB and endometrial polyps. The pooled estimate for the prevalence of hyperplasia and cancer in endometrial polyps in women with PMB was 9%. The National Institute for Health and Care Excellence (NICE) sets a 3% positive predictive value cut-off to trigger referrals to secondary care for investigations for suspected cancer. 23 The lower limit of the 95% CI of our estimate is also comfortably above the 3% threshold recommended by NICE. Therefore, women with PMB and endometrial polyps warrant polyp removal for histopathological assessment even if the background endometrium is normal.
For the purpose of this study, endometrial hyperplasia and cancer were combined as a single category because of the high rate of concurrent cancer (42.6%) and progression to cancer (28%) 24 when atypical hyperplasia is diagnosed. Endometrial hyperplasia without cytologic atypia was also combined in the same group, despite the low progression rate of <5% over 20 years, considering the recent Guidelines of the Royal College of Obstetricians and Gynaecologists that recommended at least progestogenic therapy and surveillance, i.e. these women cannot be categorised as having benign pathology. 31 The other important reason for this combination was the inconsistency in reporting amongst the included studies which would have made pooling impossible. Six studies documented separate analysis for non-atypical, atypical hyperplasia and cancer,4–6,25–27 two studies classified non-atypical hyperplasia as a normal finding,15,30 one study combined all hyperplasias together, 29 and one study reported only cancer cases. 28
Strengths and limitations
This meta-analysis is robust and adds to the existing body of literature. This is particularly relevant in women with multiple comorbidities when outpatient morcellation is technically difficult or not tolerated. We used meticulous search strategy and conducted two sensitivity analyses: one study removed cross-validation to determine the effects of individual studies on the overall effect estimate and ‘Trim and Fill’ method for correcting for small study effects. Adjustment for small study effects had no influence on the pooled estimate suggesting no evidence for publication bias. Further, cross-validation showed that no study exerted a big influence on the pooled prevalence estimate.
Nonetheless, we were unable to identify and quantify the relevant epidemiological and clinical parameters that may predict hyperplasia and cancer in endometrial polyps, such as recurrent PMB, body mass index (BMI), hypertension, diabetes, and endometrial thickness5,7,12 because of inconsistent or lack of reporting in various studies. This precluded further subgroup analyses and meta-regression. Including these predictors in the analysis would have explained some of the heterogeneity we observed and helped affirm the conclusion reached. In addition, many studies were excluded because of lack of reporting separate results for women with PMB, which might have affected the estimated prevalence in this review. A potential source of heterogeneity and bias in the study is that three studies25,28,30 had not documented the definition of the menopause used in their reports, and another study 6 defined the menopause as cessation of menstruation for ≥6 months (rather than 12 months) after the age of 45 years. It is impossible to know whether this had led to including some perimenopausal women in the analysis.
We excluded articles written in non-English languages. Since we do not have comparison groups, our analysis is unlikely to be contaminated with language bias. Moreover, the external validity of our estimate is not compromised, as we did not limit our work on a specific country or region. A systematic review of systematic reviews included five studies, aimed at finding the effect of English language restriction when conducting systematic reviews and meta-analyses, concluded that there was evidence of a systematic bias from the use of language restrictions. 32
Other meta-analyses
Three meta-analyses in the literature failed to produce robust data. The systematic review and a met-analysis by Lee et al. found that the prevalence of cancer in endometrial polyps in women with PMB (n = 1968) versus asymptomatic postmenopausal women (n = 1654) was 4.5% versus 1.5%, respectively (relative risk: 3.4; 95% CI: 1.5–7.8). 7 The second systematic review by Lieng et al. found that the pooled prevalence of hyperplasia and cancer in postmenopausal women (n = 2586) was 1.8% and 2.3%, respectively. Nevertheless, there was no separate analysis for women with PMB and asymptomatic postmenopausal women. In addition, meta-analysis was not performed since pooling of data was not possible because of the heterogeneity of the included studies as regards the populations and the outcome measures. 11 The major weakness of these two meta-analyses was that the prevalence was not a pooled estimate but rather a simple add-up of the frequencies of hyperplasia and/or cancer in polyps in the selected studies divided by the summed total number of women. This method does not take into account the heterogeneity between studies as it gives identical results to a fixed effect model which is used when there is no or minimal heterogeneity.
The most recent systematic review and meta-analysis by Sasaki et al. found that the prevalence of hyperplasia and cancer in endometrial polyps in 21,057 women undergoing hysteroscopy to be 3.4% (95% CI: 2.8%–4.1%). However, there was high heterogeneity among the included 37 studies (I2: 80.5%; p < 0.05). The studies included a mixed population of pre- and postmenopausal women both with abnormal uterine bleeding and asymptomatic. It was found that women with PMB and premenopausal women with abnormal uterine bleeding were at higher risk for hyperplasia and cancer in polyps. The prevalence ratio (95% CI) was 1.7 (1.5–1.9) and 1.5 (1.3–1.7) in the two groups, respectively. The authors recommended interpreting the findings with caution given the high heterogeneity and publication bias. 12
Recommendation for future research
Although systematic reviews with meta-analyses provide an explicit method for synthesising evidence and demonstrating early evidence with regard to the effectiveness of treatments, they may not be as valuable as a single large observational study. 7 The literature is lacking a well-designed multi-centre prospective observational study that includes endometrial polyps only in women with PMB. The data regarding the relevant clinical parameters such as recurrent PMB, BMI, diabetes, and hypertension, as well as hysteroscopic features of polyps should be collected. This would facilitate developing evidence-based guidelines as which polyp ought to be removed at first presentation.
Conclusion
The prevalence of hyperplasia and cancer in endometrial polyps in women with PMB is high indicating that the option of expectant management should only be considered with caution. Removal of all polyps when first diagnosed may be warranted for accurate histopathological diagnosis. Nevertheless, we recommend interpreting the findings with caution given the observed heterogeneity between studies.
Supplemental Material
Supplemental material for Prevalence of hyperplasia and cancer in endometrial polyps in women with postmenopausal bleeding: A systematic review and meta-analysis
Supplemental Material for Prevalence of hyperplasia and cancer in endometrial polyps in women with postmenopausal bleeding: A systematic review and meta-analysis by Ahmed Ghoubara, Malcolm James Price, Mohamed Salah El-Din Fahmy, Abdou Saeed Ait-Allah and Ayman Ewies in Post Reproductive Health
Footnotes
Acknowledgments
The authors would like to thank Miss Nicola Dawn Ager, Service Development Librarian at Library Services, Sandwell and West Birmingham Hospitals NHS Teaching Trust, UK, for her contribution in the literature search.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. This paper presents independent research supported by the NIHR Birmingham Biomedical Research Centre at the University Hospitals Birmingham NHS Foundation Trust and the University of Birmingham. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: No fund was obtained for this study, but the research fellowship of AG was funded by Aswan University, Egypt, and the Egyptian Cultural Centre and Education Bureau in London, UK.
Ethical approval
Research Ethics Committee approval was not necessary for this study. The identified data are available in the public domain through prior publications.
Guarantor
AE.
Contributorship
AG: Performed the literature search, participated in the studies selection, data extraction and quality assessment, and wrote the first draft.
MJP: Conducted the statistical analysis and revised the final version of the manuscript.
MSEF: Participated in the studies selection, data extraction and quality assessment, and revised the manuscript.
ASA: Participated in the studies selection, data extraction and quality assessment, and revised the manuscript.
AE: Created the idea, helped with the literature search, resolved any dispute about data extraction and quality assessment, and wrote the final version of the manuscript.