
Abstract
Over the last year, there have been over 12 international high profile conferences on longevity. It is intriguing to view who attend these conferences; one would expect that they would be people with medical backgrounds relating to therapeutic intervention and outcomes. But no, this is not the case. Many of those attending are there because of business interests.
Who organises these conferences? One would expect that they be medical bodies of the Royal colleges in the UK or their international equivalents, again with the intention to educate medical professionals in a fashion to improve the outcomes for patients especially in terms of longevity, the older patient. That is an intention to influence and produce positive clinical outcomes. But in the majority of these conferences, this is not the case.
So who is organising these conferences and what are their aims?
The vast majority are related to financial and business interests of commercial companies heavily involved in the actuarial world of predicting future trends, not particularly from the point of view of positive health outcomes or well-being, rather from the point of view predicting income, predicting profits from a whole variety of areas from housing, to pensions, funeral and life assurance and from the point of view of changing the patterns of lifespan and the possibilities of commercial advantage and profit in these areas.
Properly applied, they may well bring benefit to individuals by providing essential pathways for caregiving and accommodation.
The ageless society is changing definitions
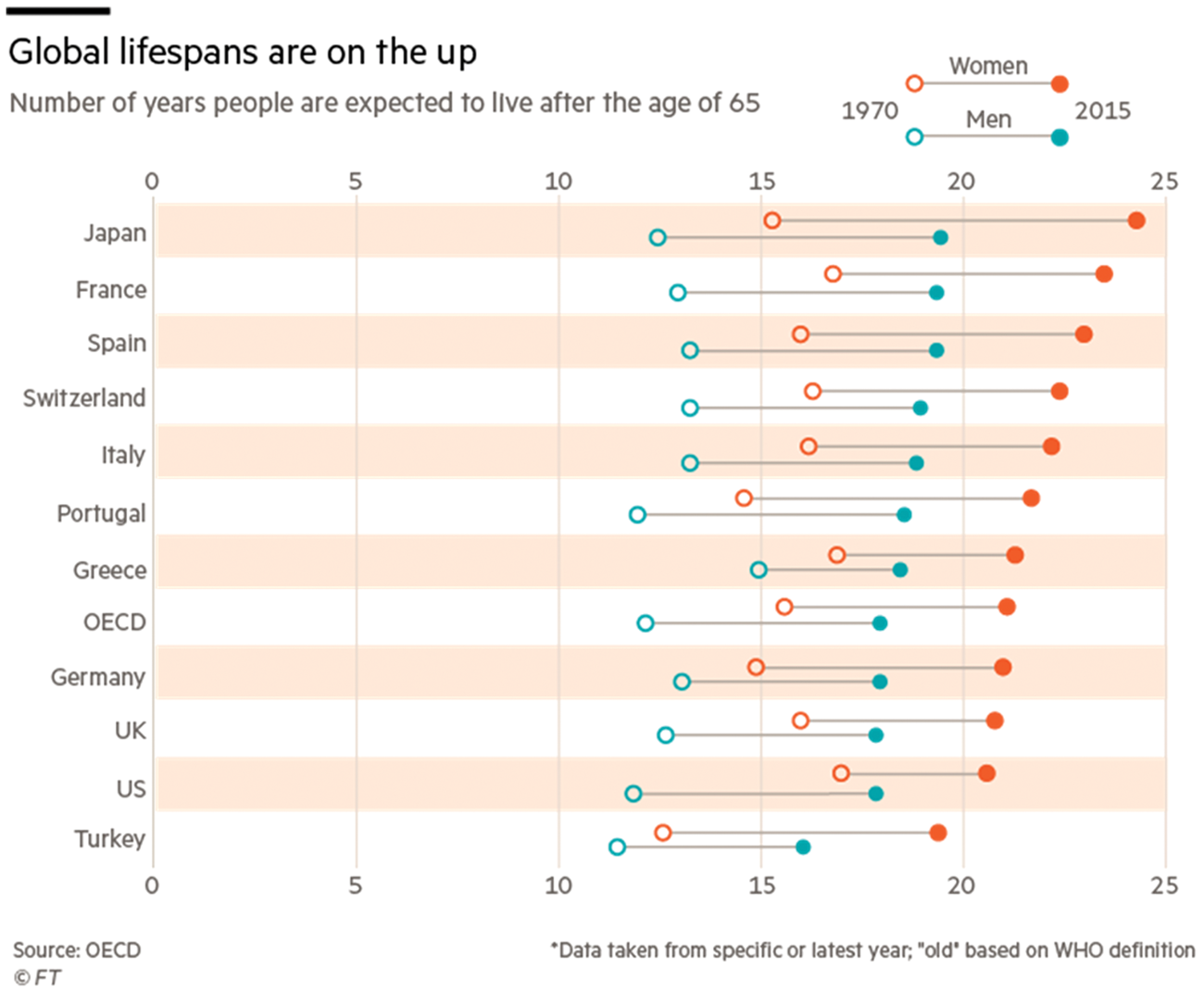
In contrast to the World Health Organization’s definition of old at 65, middle-age is extending into the mid-70s, the ‘young–old’ 60–75 or even older, the ‘old–old’ very different and should be the concern of the geriatricians in that they will have life expectancy with disability.
Work and employment are important for the ‘young–old, 60–75+’ In Japanese culture, they promote a sense of ‘IKIGAI’, or reason for being.
We should be looking at the discrepancies in ageing between the poor and affluent social groups, with a widening gap in disability-free life expectancy in the UK is in the order of 20 years, something that is getting wider and has done over the last 100 years despite the efforts of everybody from Lloyd George to Beveridge and even Tony Blair. Some of this has been due to eradication of smoking in the more informed groups, whilst the deprived and poor continue to smoke.
Stopping smoking has been one of the reasons for improved life expectancy. However, major efforts are unlikely to continue, the UK government being rather slow in these areas as opposed to Japanese, especially with regard to obesity and healthy diet.
There is a place to treat ageing as an illness or disease? It is suggested that if this were done, it would improve research and spending in the area. For as long as the authorities and those who fund healthcare fail to recognise ageing as a modifiable process, it is not seen as a legitimate target for intervention. As a consequence, the pharmaceutical industry has little interest in investing in this area.
A ray of sunshine is one clinical initiative in this area. The Targeting ageing with Metformin (TAME) trial, a double-blind trial using Metformin and placebo is due to report in 2021. 1
Another positive note, the International classification of diseases published last year mentions old age.
Research on ageing 0.2 bn
NHS budget 106 bn spent on over 65s 42 bn UK Budget 715 bn
What should the aims of longevity conferences be?
Fostering a culture of openness within health services. Recent report 2 in this area highlights formidable impediments including legacies of detriment arising from speaking up; cultural change is much more daunting given the deep-rooted and pervasive assumptions about what should be said and the consequences of mis-speaking, together with ongoing ambivalences in the organisational environment about the propriety of giving voice to concerns.
There are serious issues surrounding the introduction of the statutory ‘duty of candour’ including the threat of prosecution for those failing to uphold the policy.
From a pure medical perspective one would say, conferences are for improving well-being health and clinical outcomes for those growing older, answering questions regarding the outcomes of various interventions and their ability to improve or reduce disability, thereby improving disability-free life expectancy.
There are a variety of examples: Cataract surgery, Cochlear implant, knee and hip replacement.
We should be able to look at these interventions from both the clinical outcome perspective and also an economic health benefit perspective. Thirty-five years ago in the NHS, this was early standard practice.
This is what the current commissioning teams are doing throughout NHS England and why there is such a postal code lottery in the provision of services.
That astonishing positive results in terms of recovery from massive brain injury can occur is shown in the recent TV programme on the topic. “QUOTE”. Horizon programme on Richard Gray. Andrew Marr “My brain and Me” This should should encourage the development of rehabilitation with physiotherapy departments, fully staffed, with appropriate equipment and things like swimming pools for rehabilitation for aqua therapy, plus the appropriate occupational therapy, and other supporting inputs.
Not using these facilities to their best extent is short termism in the extreme. Economic nonsense from the point of view of attempting to reduce disability, and improved disability free life expectancy, Health service ‘cultural heresy’.
The Accelerated Access Collaborative Group (AAC) is a joint government/industry group, launched in May 2019 to promote innovation across the NHS. Search out the best ideas. Identify and fast-track cutting-edge treatments. Chairman, Lord Darzi, goes on to state ‘everyone we have encountered in our work agrees that the adoption of innovations in the NHS is a problem. The AAC is the basis of the solution’. 4
It is a tragedy that until there is reform of the health service and its culture it ‘is not clear that such endeavours will succeed in the absence of an infrastructure that underwrites positive words with consistent organisational action’. 2
Is a Royal Commission the answer looking at health service, including caring and the ageless Society? Or does Lord Darzi of Denham have the solution?