
Abstract
Just how complicated can a menopause review get? The answer is very. Not uncommonly the role of the menopause clinic is to weigh conflicting views and opinions from a variety of specialists when the patient’s General Practitioner (GP) is unsure what to do for the best. It is almost a role of arbitration.
The Calman report1 and subsequent changes to specialist medical training have improved patient outcomes in specific disease areas, notably cancer. However, in the process, the expert who can take a broad view has been lost. The holistic approach of primary care will generally compensate, but high and/or conflicting levels of risk are impossible to address in a 10-min consultation without further training.
Let’s take an example. Elaine is now 72. I first met her three years ago (age 69) when she was referred to me by a breast surgeon who was retiring. She is very much in control of her own health but seeks expert guidance.
Elaine had had bronchiectasis since childhood and was very careful to avoid potential sources of infection. She spent 3 hours a day doing postural drainage. She had retired from a high-powered job in Human Resources at the age of 50 because of this.
She had always had lumpy breasts and had been diagnosed with DCIS in 2011 following an NHS breast screening mammogram. The changes were diffuse, and she had chosen to have the whole breast removed without reconstruction to minimise the time under anaesthetic. Sentinel node biopsy was negative, and no other treatment was offered. She had been followed up by my colleague with examination and an annual mammogram.
Elaine had had her last period at 55. Two or three years later, there had been post-menopausal bleeding which was investigated. A polyp was removed, and the D + C samples (!) were negative. Several gynaecologists have been involved over time, and she is known to have recurrent herpetic ulceration, atrophic vaginitis, fibroid change but normal endometrium whenever assessed. She had had annual TV and abdominal ultrasound scans. She was known to have gallbladder polyps and a calcified liver lesion, a small adnexal mass but a raised CA125 (typically 91 U/ml). All had been unchanged for several years.
Elaine had begun having hot flushes at 41. She had been on and off Hormone Replacement Treatment (HRT) ever since and gave me the long list of products that had been tried. She always felt better with it but repeatedly had been advised to stop. She had been without for six months when we first met as she had had some breast tenderness. She found that flushing and sweats had resolved but sleep disturbance, low mood, foggy brain, vaginal dryness, bladder irritability and aches and pains were still bothersome. She was taking citalopram for mood.
As if that was not enough, she was worried about her bones. She had been confirmed as osteopaenic by Bone densitometry (DXA) in 2005. Her Body Mass Index (BMI) was 21.5, her blood pressure normal, she did not smoke or drink, but exercise was limited by her breathing.
Looking at each area in turn and balancing the various options, she left our first consultation in December 2016 with a prescription for tibolone to take half of a tablet (1.25 mg) daily. This dose has been extensively investigated and shown to protect bone but was never marketed. It is achieved with the aid of a tablet splitter. She was also prescribed estriol 0.1% vaginal cream to use twice a week.
I see her annually with an interim visit if she needs to talk.
Three years on, she is still taking citalopram 10 mg and having dropped it for three months is back on tibolone 1.25 mg daily and using estriol 0.1% cream twice a week. The tibolone has been stopped and restarted a couple of times.
During the last year she has had:
A breast review with the new specialist who had advised that she stop the tibolone, as this is linked with an increased risk of breast cancer. A private upper abdominal ultrasound which had confirmed the gallbladder polyps and liver lesion to be unchanged. At the same time, a transvaginal ultrasound confirmed small fibroids, a normal endometrium, a small adnexal mass which has not altered and atrophic ovaries. CA125 check arranged by the GP which was unchanged. Repeat DXA scan arranged by her GP.
Review
Gynaecology
Tibolone is used as addback with GnRH agonists to shrink fibroids prior to surgery. It is therefore reasonable to assume that it does not stimulate fibroids and is a good option for Elaine. The Thebes (Ref 2) study using both 1.25 mg and 2.5 mg doses showed significantly less bleeding than an estrogen/progestin combination. It was shown not to stimulate the endometrium but does reduce vaginal atrophy. The combined estrogenic and androgenic effect can help mood, energy and wellbeing. Twice weekly vaginal estrogen has a purely local effect, and the combination is appropriate.
Cardiovascular and metabolic
Elaine’s cardiovascular risk profile has not changed significantly, other than she is older. Despite being taken orally, tibolone is quite different to oral estrogen being antifibrinolytic, and there is no associated increase in VTE risk (this was confirmed by Vivagradova et al.3). It does not lower cholesterol as does estrogen, and there are some data that in older women with multiple risk factors there is an increase in stroke risk associated with its use. Elaine has a low risk profile such that we determined this not to apply.
Breast
Elaine’s remaining breast had been checked by examination and a mammogram will be due next year. The data with respect to breast cancer risks associated with tibolone are confusing, mainly due to low numbers. The consensus is that in all groups: in the lab, in women who have not had breast cancer and in women who have already had a diagnosis is that any effect that does exist is small. This would seem to affect growth rather than initiation. Given that she is monitored, that her dose is low, and any effect would be less than an estrogen and progestogen combination, Elaine makes an informed choice to accept this for the benefits it achieves.
Bone
The most revealing result was that of the bone density scan.
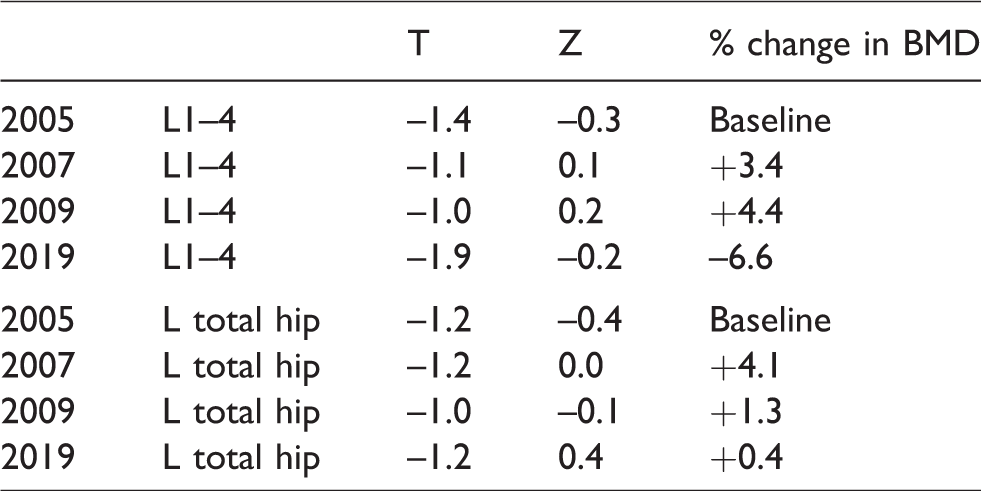
After the 2005 result, risedronate was prescribed but caused gastritis, and following an upper GI endoscopy in 2006, Elaine was told never to take bisphosphonates again. Considering that the breast cancer diagnosis was in 2011, that there were substantial spells with no HRT and that tibolone has been at below licensed dose for less than three years, I think this result is remarkable.
Normal loss would be 8–10% in the five years or so after menopause, then 1% a year thereafter. Anything less than an 18% loss is a success.
It is still important to maintain a calcium intake of approximately 1000 mg a day with adequate vitamin D and have enough weightbearing exercise as bone remodels in the lines of stress.
The studies tell us that tibolone 1.25 mg should prevent loss and it does appear to have done so.
Other
Quality of life and energy levels are very important to Elaine as she lives alone and has the bronchiectasis to contend with. She will continue with the citalopram, but this is not enough on its own and the profile of the tibolone maintains her wellbeing. Bone density assessment does not need to be repeated for another five years. Upper abdominal ultrasound no longer needs to be repeated on a regular basis, as there have been no changes over the last five years. Planned mammography at two yearly intervals seems sensible if affordable, but NHS three yearly screening can be requested if over 70. Annual monitoring of CA125 seems reasonable, and if there is no significant increase and in the absence of symptoms, I think it is entirely reasonable to increase the interval for pelvic ultrasound monitoring. Continue the current regimen. Elaine’s GP has prescribed both tibolone and estriol cream. She can be reassured that this is appropriate. Elaine has been very involved in the process and this is the product of informed decision making.
Advice for the future:
This level of analysis and integration is not easy, but with knowledge, experience and good communication, it can be achieved in half an hour. There is no way that this could happen in routine General Practice. My hope for the primary care networks is that it might be do-able to with training, the development of integrated women’s health provision and appropriate time allocation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.