
Abstract
Objective
Requests for management of menopausal symptoms and hormone replacement are increasing in the UK. Referrals to specialist clinics have to be balanced with increasing recommendations within the NHS to improve efficiency and patient care.
Study design
Retrospective evaluation of clinic records over two months at a district general (Poole Hospital) and tertiary (Guy’s Hospital) menopause service. Data on referral origin, reason for referral, interval from referral to review and outcome were collected and compared between trusts.
Main outcome measures
To evaluate and compare referrals and outcomes in a tertiary and district general menopause service and provide recommendations for improving efficiency.
Results
Most referrals are from primary care but up to 25% are from other specialties. Half of the appointments are new referrals and 95% of women attend. Of the new referrals, 50% have multiple medical comorbidities, 25% a personal or family history of cancer and 25% treatment resistance; 30% have premature ovarian insufficiency. At Guy’s Hospital, 30% are reviewed more than 18 weeks after referral, at Poole Hospital this is 6%. Treatment resistance is reported in half of the women reviewed at follow-up.
Conclusions
Menopause services review a complex patient population and the majority of referred women have more than one co-morbidity; they require time, specialist knowledge of current treatment options and a multidisciplinary approach. The main barrier to service efficiency is capacity, particularly in population dense areas; cognitive behavioural therapy and non-hormonal methods appear under-utilised in primary care, as do alternative methods of follow-up within the clinics such as telephone and patient-initiated appointments.
Introduction
The request for management of menopausal symptoms and hormone replacement therapy (HRT) is increasing in the UK. Nearly 50% of the working population are female and in line with changes in pensionable age, the rate of women older than 50 who are working continues to rise. 1 To aid workforce planning, to circumvent the potential economic implications and to improve quality of life, interventions which reduce the impact of menopausal symptoms in the workplace have had increasing exposure in the media.
Women with minor to moderate symptoms can be self-managed or reviewed in primary care but one-third of women will have severe symptoms and a quarter have considered leaving or reducing their working hours2–5 – HRT may decrease the impact of these symptoms on a woman’s daily function. If these women have complex co-morbidities they may need the involvement of a menopause specialist. The NICE menopause guideline 6 provides robust referral criteria for this specialist service which includes women in whom treatment does not improve symptoms, those with ongoing side effects from treatment, where there are contraindications to HRT, uncertainty about the most suitable treatment options and when premature ovarian insufficiency (POI) is suspected.
There are increasing recommendations within the NHS to improve efficiency and patient care within clinical services. Optimising clinic capacity by evaluating the appropriateness of referrals and offering alternative consultation methods, such as telephone- or patient-initiated follow-ups, may reduce the waiting time between referral to first treatment and between follow-up appointments, helping to achieve these recommendations.7,8
The primary aims of this project were to evaluate and compare referrals and outcomes to menopause services in a tertiary and district general hospital. The secondary aim was to provide potential recommendations for improving efficiency within the service.
Methodology
Guy’s Hospital (GH) is a tertiary NHS centre which has a fortnightly menopause clinic and a six weekly dedicated POI clinic. This service is overseen by two gynaecology consultants and a nurse consultant; they supervise six ST1-7 gynaecology trainees or GPs with a special interest in menopause care. Poole Hospital (PH) is an NHS district general hospital. It is a consultant-led service with weekly clinics; the team consists of two consultant gynaecologists, a menopause nurse specialist and an associate specialist. The lead consultants for both hospitals are experienced menopause specialists (over 20 years) with national research and policy making input.
Electronic records for all women attending menopause clinics between 1st August and 30th September 2019 were retrospectively reviewed. An ExCel spreadsheet was designed following a literature review and co-variables were given a numeric value to aid data analysis. No identifiable information was recorded and double data entry was completed.
Referral demographics such as source of referral (GP, self or hospital department) and type (new or follow-up), interval in months from referral to appointment and distance travelled from the woman’s home address were recorded.
Reasons for referral were coded as POI, cancer, medical co-morbidity, treatment resistance and/or symptom control. Outcome data were reviewed and coded as advice only, start HRT, change HRT preparation, increase estrogen dose, start non-hormonal treatment (such as selective serotonin reuptake inhibitors (SSRIs) or cognitive behavioural therapy (CBT)), start testosterone, organise investigations or refer to another department. Follow-up appointment was coded as discharge, face-to-face or telephone. Interval (in months) between initial review and follow-up was also recorded.
Approval for audit data collection was provided by the Trust and Lead Clinician. Caldicott Principles, Data Protection Act (1998) and the NHS Confidentiality Code (2003) guidelines were adhered to; only anonymised clinical data collected as part of routine medical records were used.
Descriptive statistics such as mean and range for continuous variables and frequency and proportions for categorical variables were used to describe the sample. To assess differences in means and proportions, p values were calculated.
Results
Referral demographics
Table 1 reports and compares the referral demographics. During the two months of data collection 176 women were booked into four clinics at GH and 149 women into 12 clinics at PH. Of the notes evaluated, there were 15% more new referrals (106 vs. 64) and 22% fewer follow-up appointments (58 vs. 78) at GH when compared to PH. Most women attended their appointments and there was no observed difference in the proportion of women who did not attend their appointment at GH (6.8%) or PH (4.6%) – all of whom were follow-ups – leaving, respectively, 164 and 142 complete data sets.
Demographics of referrals to a tertiary (Guys) and district general (Poole) menopause service.
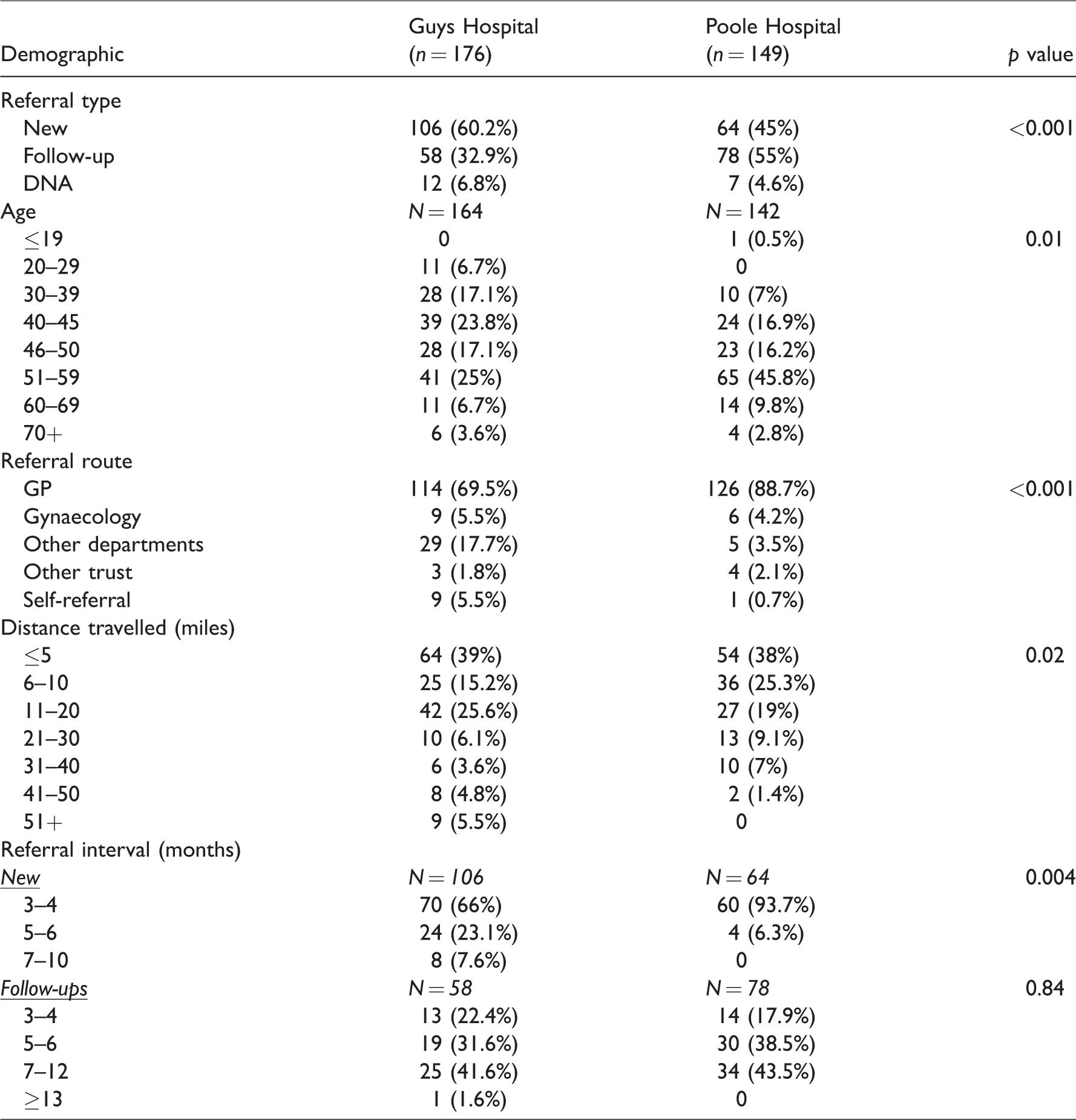
More than two thirds lived within 25 miles of both hospitals. The average age was 46 (range 60, 23–83) at GH and 51 (range 63, 16–79) at PH. There were more women with POI reviewed at GH (n = 65, 39.6%) than PH (n = 35, 24.4%); p < 0.001.
The majority of women were referred from their GP but there were more referrals from other specialties at GH (haematology, endocrinology, rheumatology, oncology, fertility and HIV medicine), which accounted for almost a fifth of the total appointments. PH saw more new patients within three months of the referral than GH (93.7 vs. 69.2%). Of the 32 women seen after 4 months at GH, 59.4% (19) were referred from another specialty.
Reason for referral
Table 2 reports the primary referral indication for new and follow-up patients; there was no observed difference between the two trusts.
New referrals:
Main referral indication for new and follow-up patients to a menopause service.

*Women presented with more than one co-morbidity
** GH and PH combined
Half of the referrals were to assess suitability for HRT in the presence of medical comorbidities; the majority, 85%, had more than one co-morbidity. At PH 85% (28) of these women had been started by their GP on low-dose HRT or an SSRI prior to review. At GH this occurred in 27.5%, the majority of the women who had not been offered alternatives prior to review were referred from other specialties.
Up to a quarter of new referrals were women with menopausal symptoms who had a personal or family history of cancer. Before clinic review, 44.8% at GH and 90% at PH had been offered non-hormonal treatments. In both trusts, 6% of the referrals were to discuss cessation advice (age 64–71); all were offered a change of HRT preparation and advice about tapering to the lowest effective dose, but none of the women were given recommendations to stop HRT. A fifth to a quarter of women reviewed were for treatment resistance; all had tried three or more preparations prior to referral. Table 3 provides examples of the complexities of these new referrals; half of whom were randomly selected from GH and half from PH.
Random selection of new referrals to a menopause service.

CBT: cognitive behavioural therapy; CVD: cardiovascular disease; aPL: anti phospholipid; HRT: hormone replacement therapy; POI: premature ovarian insufficiency; VVA: vulvovaginal atrophy.
There were more new referrals for POI to GH (n = 33, 31.1% vs. n = 14, 21.8%; p < 0.001) and there was a variety of aetiology; 26 were idiopathic, 13 iatrogenic (surgical or chemo-radiation) and 8 were for autoimmune or genetic causes.
Table 4 contains the symptoms reported in new referrals; there was no observed difference between the two hospitals. Hot flushes were reported in more than two thirds and severe cognitive impairment, insomnia, mood and/or anxiety in one-third. More than two-thirds, 70%, had three or more main symptoms. In those women who reported one symptom only, these were vasomotor, insomnia, vulvovaginal atrophy (VVA) or anxiety.
Follow-up appointments:
Symptoms reported in new and follow-up referrals at Guys and Poole Hospital Menopause Clinics.
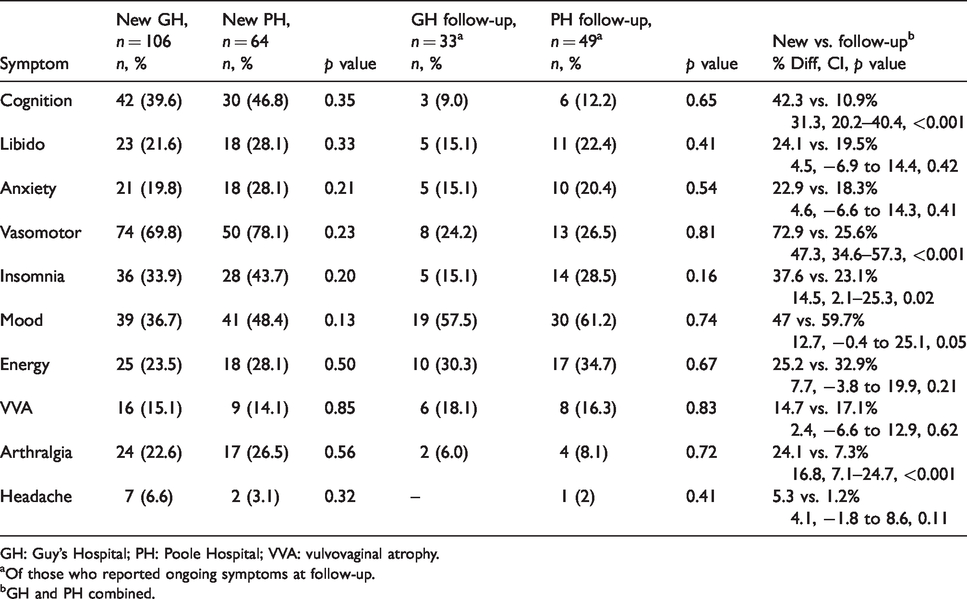
GH: Guy’s Hospital; PH: Poole Hospital; VVA: vulvovaginal atrophy.
aOf those who reported ongoing symptoms at follow-up.
bGH and PH combined.
There was no difference in the proportion of women primarily reviewed with medical co-morbidities and menopausal symptoms between new and follow-up appointments (∼50%). When compared to new appointments, follow-ups consisted of 14% more women with treatment resistance and 11% fewer women with a previous cancer diagnosis (Table 2). Three of the women were asymptomatic but had long-term follow-up in the clinic as the GP was concerned about continuing to prescribe HRT in women with a previous estrogen receptor positive cancer.
Table 4 assesses and compares symptoms reported in new and follow-up appointments; there was no observed difference between the hospitals. Follow-ups were 47% less likely to report vasomotor symptoms, 31% less likely to report cognitive effects and 14% less likely to report insomnia. They were 12% more likely to report mood as an ongoing symptom. Women with POI who had resistant symptoms accounted for half of the follow-up appointments at GH (49.2%) and more than half at PH (61.6%). The women with the most resistant symptoms at follow-up were those with a cancer history, of whom 63% had started non-hormonal treatment after the initial appointment and 54% had POI.
Clinic outcomes
Table 5 reports the management options and follow-up recommendations offered to new referrals. At both trusts a third of women were offered HRT as a new treatment and in almost a half the HRT preparation was changed to improve symptom control or reduce the risk profile. Testosterone was offered to less than 10%. Non-hormonal medications, but not CBT, were documented as being offered to 17% (18 women) at GH. At PH, 85% had already tried these options before clinic review accounting for most of the 91.5% who were not offered these.
First-line management options and follow-up recommendations offered to new referrals at Guy’s and Poole Hospitals.

CBT: cognitive behavioural therapy; DEXA: dual-energy X-ray absorptiometry; HRT: hormone replacement therapy; POI: premature ovarian insufficiency; SNRI: serotonin-norepinephrine reuptake inhibitor; SSRI: selective serotonin reuptake inhibitor.
Up to 10% of women were referred to other specialties to discuss either the safety of starting HRT, the implications of a new genetic diagnosis or potential fertility options. Up to a fifth of women were referred for investigations to assess irregular bleeding, POI aetiology, bone mineral density or to evaluate other causes of vasomotor symptoms which were not felt to be solely attributable to the menopause. Of the women who were recorded to be smokers, it was documented that GH recommended smoking cessation to 50% and at PH this was 65%.
At both trusts a fifth of women were discharged after their first appointment, almost three-quarters were offered face to face follow-up and up to 7% telephone follow-up. Two thirds were reviewed by three months and a further third by six months. Of those women whose review was delayed, capacity within the clinic was cited as the main reason in the majority. Of the women offered face–face follow-up, 19 (24.6%) at GH and 11 (22.9%) at PH could potentially have had telephone consultations such as women who were started on testosterone (with no other risk factors), women whose resistant symptoms were due to compliance or incorrect application of HRT and POI women who had appointments to discuss a normal dual-energy X-ray absorptiometry (DEXA) result or to increase their estrogen in response to a deteriorating T-score.
Discussion
Our study has shown similarities in referral indications and clinical outcomes between a specialist menopause service in a tertiary and district general hospital. Our data suggest menopause clinics are an essential specialist service as illustrated by the number of referrals (approximately 1000 per trust per annum), the complex co-morbidities of the patient population, the treatment resistance of symptoms which impact on daily function, the expertise which facilitated all women being offered individualised treatment options and the small rate of non-attenders (6%) – which indicates women value the opportunity to be reviewed by a specialist.
Half of the appointments are new referrals and although the majority are from primary care, 10–25% are from other specialties suggesting a complex patient population. NHS Guidance advises new referrals should start treatment within 18 weeks 9 ; this was achieved in 93.7% at PH and 69.3% at GH (who review 15% more new referrals). Nationally 87.5% are treated in gynaecology outpatients within 18 weeks 9 but the recent 2019 Better for Women survey of women aged 18–65 reported that 58% have poor access to local menopause services 10 and this may have a greater impact in a population dense area.
Decreased patient access to specialist services is also suggested by the distances travelled to attend appointments. In the UK, distances of 24–50 miles (equating to an hour’s drive) are reported as the maximum threshold for access to specialist services with over 25 miles from a DGH considered ‘remote’ 11 – as was observed in one third of our cohort. A low geographical accessibility may contribute to the impact on capacity observed within sparse services. 12
To improve service efficiency and patient care, the 2016 RCOG standards for gynaecological care state that robust referral pathways are needed for specialist services which manage complex gynaecological conditions. 8 Healthy women with menopausal symptoms can be managed in primary care and a survey showed 86% of GPs agree with this. 13 However, in the decade following the Million Women and Women’s Health Initiative studies,14,15 prescriptions for HRT from primary care have reduced 16 and this has been compounded by recent HRT supply shortages. 17 A 2018 survey of UK GPs reported that 44% feel under-confident in managing the menopause, 23% are not confident to prescribe HRT in healthy women and this increases to 44% in women under 45. 13 Women may seek alternative preparations or access alternative sources of information which may not be evidenced based or safe; the 2019 RCOG Better for Women survey reported 52% believe online searches are reliable sources of information. 10
Women with early menopause accounted for over 40% of the referrals – with a greater proportion reviewed at GH which has a specialist POI clinic. The NICE Menopause Guidance 6 and the BMS Vision for Menopause care 18 recommend that women with POI should be assessed by a menopause specialist. Our data supports this guidance; half of these women had concurrent co-morbidities (medical or a previous cancer diagnosis) and due to poor symptom control, treatment resistance accounted for 50% of the follow-up appointments. Women with POI benefit from the holistic care that can be provided by a centralised service such as access to fertility, genetics, counselling, DEXA scans and ongoing support for a condition which over time presents different challenges.
Our data suggests that women aged 45 and older who are referred to the menopause service are not ‘healthy’ but, like those with POI, have multiple co-morbidities in addition to complex menopausal symptoms. Of the new and follow-up appointments half had complex medical problems, 20–35% multiple treatment failure and 10–20% a personal or family history of cancer. Differentiating menopausal symptoms from other pathological aetiologies in women with multiple medical comorbidities requires expertise and the use of current evidence based medicine to accept a higher level of responsibility when treating these women.
There is evidence that centralised care in specialist centres has a positive impact on health outcomes (as long as they are geographically accessible).19,20 Our data suggests women 45 and older also benefitted from an multidisciplinary team (MDT) approach with other specialties such as endocrinology, haematology and oncology. Specialist input can promote shared decision-making which improves service provision and the quality of patient care by facilitating engagement with their own health. Extended appointments improve compliance, enable a holistic approach, optimisation of medication and can reduce the total number of reviews in women with menopausal symptoms. 21 There is evidence to suggest that extended appointments also benefit patients with psychosocial conditions22,23 – this time enables the building of rappor, the use of validated questionnaires and targeted questions which can determine the aetiological cause of mood symptoms which our data has shown to be the most resistant to treatment. In a primary care setting, time constraints, due to an ever-increasing workload and volume of patients, may hinder this.
The advantages of the service can be assessed through the outcomes. All new referrals with complex co-morbidities and symptoms which impacted on daily function were offered individualised treatment options – the majority, up to 91%, a HRT preparation and the remaining 9–17% were offered non-hormonal alternatives. At GH only a small proportion of women had been recommended alternative therapies prior to clinic review and an education day, which covers NICE recommendations and appropriate alternatives, for primary care and specialties who review these women, may improve patient symptoms and decrease referrals.
The medical complexities of the new referrals led to a high proportion being offered follow-up. Although this will have an impact upon the ability of the service to book new appointments, the importance of assessing compliance and symptom control will facilitate primary prevention of cardiovascular disease and osteoporosis in women with POI and assess the side effect profile in women with hormone responsive comorbidities.
The number of telephone follow-ups was low. An increase in this consultation method may improve the capacity for new referrals, further decrease non-attendance rates, reduce the interval from referral to assessment and the time and economic burden of women travelling long distances to appointments. The reasons which affected the decision-making to offer face to face follow-up were not recorded; these may have included patient preference, health care provider choice due to the potential complexities of the consultation or a language barrier (particularly in a multicultural city where English may not be the primary language).
Strengths of the study include double data entry, which reduced missing and erroneous data, and comparison of data between trusts was improved by similar cohort numbers. Limitations include the data collection interval – two of the clinics at each trust were reduced due to health care provider annual leave – a larger sample size may have revealed differences in some of the main referral indications. Data which evaluated the total length of follow-up (in years) for individual patients was not collected and the retrospective nature of the data collection prevented assessment of the total length of individual appointments and the cause of delay between referral and assessment (such as rebooking by the patient or the clinic).
Conclusions and recommendations
Clear criteria for referral to secondary care improves service efficiency and patient care; most of the women were referred appropriately and in line with NICE guidance. To reduce low-risk referrals, GP menopause/HRT update days would be of benefit. This may increase the management in primary care of women who are 60 or older without co-morbidities, those women who have VVA with systemic HRT and may facilitate the use of non-hormonal alternatives such as CBT and SSRIs. The RCOG ‘Better for Women’ survey reports that 50% of women struggle to access menopause care – indicating that more services are required – particularly as the number of women entering the menopause is steadily increasing per annum. Our data suggests that referrals and outcomes to a tertiary and district general experienced menopause specialist are comparable, providing evidence for units aiming to deliver a service for women who are geographically more isolated from tertiary units. A menopause service is an ideal platform for promoting primary prevention of cardiovascular disease by endorsing smoking cessation and healthy lifestyles. There was a higher proportion of delay in reviewing referrals from other specialties; to improve patient care the referral pathways for these patients should be evaluated. Offering telephone consultations or patient initiated follow-up for lower risk women and more rural communities may enhance the service and increase capacity. Further research would be of benefit in assessing patient’s views on telephone follow-ups (particularly relevant in view of the impact COVID-19 has had on elective services), the effect assessment by the service has on their working and home lives and whether women with POI prefer their long-term follow-up to be within the service or in the community.
Footnotes
Acknowledgements
The authors thank Mrs A Hillard and Mrs L Cullen for administrative assistance at Poole Hospital.
Authors' contribution
All authors conceived the manuscript. KM researched the literature, completed the data collection and analysis and wrote the first draft of the manuscript. All authors reviewed and approved the final version.
Declaration of conflicting interests
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
KM.